The repercussions of obesity on health problems such as type II diabetes, CVD, hypertension and cancer are well known(1–4). Unfortunately, a growing number of children and adolescents have problems stemming from being overweight or obese(4, Reference Shields5). That is why several organizations are calling for interventions to help youngsters develop healthy nutritional and physical activity habits(1–3).
In response to this alarming situation, many schools in Europe, Canada and the USA have adopted new food policies and, consequently, replaced unhealthy products by healthy foods(6–8). Hence, adolescents are more likely to eat healthy meals by staying in school during lunch time to eat a meal prepared at home or purchased in school cafeterias, instead of frequenting fast-food restaurants. It is now well recognized that meals prepared outside the home, such as those sold in fast-food restaurants, are generally less nutritious and contain higher amounts of energy, fat and sugars than home-made meals(Reference Bowman, Gortmaker and Ebbeling9–Reference Paeratakul, Ferdinand and Champagne12).
Unfortunately, many schools are surrounded by fast-food restaurants that are very often within walking distance(13–Reference Simon, Kwan and Angelescu17). It is thus attractive for students to lunch in such places. Indeed, easy access to fast-food restaurants in areas near schools is associated with poor-quality foods consumed by adolescents and the risk of being overweight or obese(Reference Davis and Carpenter18, Reference Shepherd, Harden and Rees19). The Canadian Community Health Survey of 2004 demonstrated the extent of fast-food consumption among adolescents. It was observed that one-third of adolescents aged 14 to 18 years had consumed fast foods the day before the survey(20). A recent study ascertained that 42·5 % of students went to fast-food restaurants during lunch time at least once in the last 10 d, and 11·0 % reported that they ate in fast-food restaurants at least twice weekly(Reference Beaulieu and Godin21). These data illustrate the importance of this public health problem and confirm the need to address it.
To the best of our knowledge, no theory-based intervention has specifically focused on the problem of motivating students to remain in school for lunch instead of eating in fast-food restaurants. The present intervention programme was developed to attain this goal. More precisely, the present study examined the effectiveness of a theory-based intervention and verified the mediating effect of targeted theoretical variables on the behaviour of staying in school for lunch among high-school students.
Experimental method
Intervention description
The development of the intervention programme was guided by intervention mapping(Reference Bartholomew, Parcel and Kok22). This model combines theoretical and empirical data with the particular beliefs and context of the target population(Reference Kok, Schaalma and Ruiter23). One of the intervention mapping steps is to identify the determinants of behaviour in the target population. An extended version of the theory of planned behaviour(Reference Ajzen24, 25) served to identify these determinants. Thus, based on the observations reported by Beaulieu and Godin(Reference Beaulieu and Godin21), the target determinants of the intervention were intention, perceived social norm, perceived behavioural control, perceived self-efficacy and attitude. Specific objectives were formulated for each of these determinants, and theoretical methods and practical applications were selected. Intention was addressed indirectly through its determinants (i.e. perceived social norm, perceived behavioural control, attitude and perceived self-efficacy). For this purpose, the recommendations of Bartholomew et al.(Reference Bartholomew, Parcel and Kok22), Bandura(Reference Bandura26, Reference Bandura27) and Michie et al.(Reference Michie, Johnston and Francis28) were followed. Moreover, given that there is no evidence to support a particular type of intervention to improve nutritional behaviour(Reference Shepherd, Harden and Rees19, Reference Casey and Crumley29–Reference Flodmark, Marcus and Britton31) and many results suggest that multi-strategy interventions(Reference Shepherd, Harden and Rees19, Reference Flynn, McNeil and Maloff30–Reference Veugelers and Fitzgerald36) can be effective among adolescents, it was decided to implement a multi-component programme over a 12-week period during early 2010 (winter to spring). Considering the important role of parents in their adolescents’ food habits, some practical applications were dedicated to them. Table 1 presents the theoretical methods and practical applications associated with the target determinants.
Table 1 Theoretical methods and practical applications associated with determinants
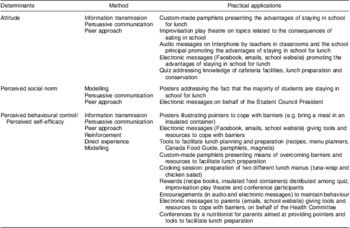
In summary, practical applications were offered: (i) in classrooms (distribution of tools, recipes and pamphlets, audio messages by teachers and school principal, cooking sessions); (ii) at lunch time (improvisation play theatre); (iii) during free time periods (electronic messages, school website, quiz); and (iv) to parents (electronic messages, conference, distribution of tools). As recommended for intervention mapping(Reference Bartholomew, Parcel and Kok22), individuals representative of the target population and stakeholders were consulted at each step of the intervention programme's development and implementation.
Study population and samples
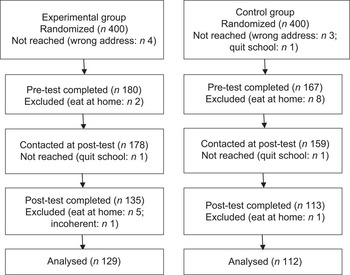
The study population comprised high-school students between the ages of 12 and 17 years. Two schools from the same school board located in the same city and sharing the same socio-economic level were invited to participate in the study. In each school, a random sample of 400 students was selected from a list of students enrolled in the main school programmes. In the experimental group, students were enrolled in general and international courses (n 400 out of 1931). In the control group, students were enrolled in general and information technology courses (n 400 out of 973). Both schools belonged to the public system and served students with a low deprivation index(37). A pre-intervention questionnaire was mailed to these 800 students. Figure 1 shows the number of participants in the experimental and control groups who completed the questionnaire pre- and post-intervention and who were included in the analysis. Response and attrition rates were respectively 45·5 % and 23·7 % in the experimental group and 42·2 % and 28·5 % in the control group.
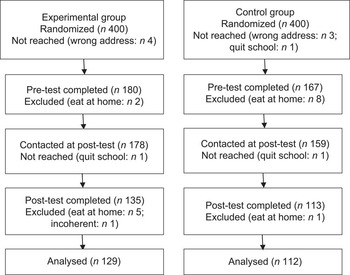
Fig. 1 Flowchart of study participation
Data collection
Experimental and control group students were invited to complete and return a self-administered questionnaire twice, the first time in September 2009 (pre-intervention) and the second time in May 2010 (post-intervention). For logistical reasons related to school organization, it was impossible to randomly sample 400 students from different levels and academic programmes during school time. Therefore, questionnaires were sent to their homes for return by mail. This data collection method also allowed parental consent to be obtained, as requested by the Research Ethics Committee. Parent and student consent forms were included in the pre-intervention package. Different strategies were adopted to encourage participation(Reference Dillman38). First, a project introduction letter was delivered to all parents of students from both schools during the summer preceding the school year. Second, gift certificates from a sports store were randomly drawn among respondents. Third, various forms of recall followed each mailing: a postcard was posted 1 week after sending the questionnaires and three audio messages in both schools were aired at 1-week intervals via the local Interphone system. Fourth, a second copy of the post-intervention questionnaire was sent to non-respondents 4 weeks after the first mailing. The study was approved by the Research Ethics Committee of Laval University (No. 2008-312/03-06-2009).
Variables measured
The questionnaire was developed in accordance with the methodology suggested by the author of the theory of planned behaviour(25) and the approach described by Godin and Kok(Reference Godin and Kok39). Questions were also formulated as per theoretician recommendations(Reference Ajzen24, Reference Ajzen40, Reference Fishbein, Triandis and Kanfer41). The questionnaire assessed sociodemographic (i.e. age, sex, school level, school programme), behavioural (i.e. number of days in the last ten school days the respondent (i) stayed in school for lunch, (ii) ate lunch prepared at home, (iii) ate lunch purchased in the school cafeteria and (iv) went to a fast-food restaurant for lunch) and psychosocial variables (i.e. intention, attitude, perceived behavioural control, perceived social norm, behavioural beliefs, self-efficacy and facilitating factors). To reduce questionnaire length, normative beliefs were not included. A 5-point Likert-type scale was utilized for most psychosocial items; the average of the sum of items of each construct was considered in the analyses. The reliability of all psychosocial variables was appropriate; internal consistency (Cronbach's α) of the baseline questionnaire varied between 0·61 and 0·94.
In the questionnaire, a first screening question identified students who usually returned home for lunch; these students were asked to complete only the sociodemographic items and were excluded from the analysis. The same questionnaire was used at each time measurement in both schools. However, for the experimental school, a few questions were added in the post-intervention questionnaire to verify the degree of exposure to intervention activities.
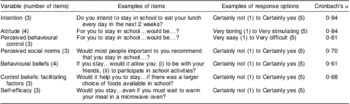
Two dependent variables were operationalized with the following question: ‘On how many days did you stay in school for lunch in the last 10 school days?’ (intra-class coefficient = 0·71). One of the dependent variables was the number of days out of ten that students remained in school for lunch. The second dependent variable was expressed as a proportion, i.e. the proportion of students who stayed in school for lunch every day (i.e. all 10 d). Table 2 presents the numbers of items that served to assess each psychosocial variable, examples of questions and response options as well as Cronbach α values.
Table 2 Number of items, examples of questions and response options, and Cronbach α values for the theoretical constructs (n 337)
Data analysis
Descriptive analysis of the sociodemographic variables was undertaken to first verify sample representativeness. ANOVA and the χ 2 test verified the equivalence of the experimental and control samples and the potential differences between study completers and drop-outs for baseline sociodemographic, behavioural and psychosocial variables. Given the negative skewness of the distribution of the first dependent variable (i.e. number of days), Poisson regression was applied, with the GENMOD procedure controlling for covariates (age and past behaviour). With regard to the second dependent variable (i.e. proportion of students), log-binomial regression with GENMOD compared the proportion of students who stayed in school every day (i.e. all 10 d) with those who did not stay every day (i.e. 9 d or less), also controlling for age and past behaviour. The moderating effects of sex, age and school programme were tested in the latter analysis by means of interaction terms between treatment and each of these variables. Analysis was performed only on participants who completed both pre- and post-tests. Finally, intention-to-treat analysis was conducted and included drop-outs, who were attributed baseline data on the dependent variable (last observation carried forward).
To verify if the intervention positively changed the target psychosocial variables, analysis of covariance was performed controlling for past behaviour, baseline values of the study variables and sociodemographic covariates associated with the study variables. Moreover, mediation analysis ascertained if the effect of the intervention (X) on the outcome (Y; i.e. the mean number of days that students stayed in school for lunch) was mediated by changes in the targeted psychosocial variables (M). A bootstrapping procedure (5000 bootstrap samples) was applied(Reference Preacher and Hayes42–Reference Preacher, Rucker and Hayes45) controlling for key covariates (age, past behaviour, means of psychosocial variables at baseline) according to the SAS macro procedure proposed by Preacher and Hayes(46). The given a, b, c and c′ paths represent respectively the unstandardized regression coefficients of the effect of the intervention on the mediator (a), the direct effect of the mediator on the outcome (b), the total effect of the intervention on the outcomes (c) and the direct effect of the intervention on the outcome (c′). Mediation was considered significant if the bias-corrected and accelerated (BCa) 95 % confidence interval did not span zero(Reference Preacher and Hayes42, Reference MacKinnon43). All analyses were undertaken with the SAS statistical software package version 9·2 (SAS Institute, Cary, NC, USA).
Results
Samples
The two randomized samples of 400 students did not differ in gender, school level and programme type from their respective reference populations. This observation also applied to respondents (experimental school, n 178; control school, n 159) with the exception of school programme type in the control school; students from the information technology programme were over-represented in comparison to the reference population (49·1 % v. 40·6 %; χ 2 = 5·53, P = 0·018). Students in the experimental and control groups who completed the baseline questionnaire did not differ in terms of gender and school level from non-respondents. However, a higher percentage of student non-respondents were registered in the general programme compared with other programmes (experimental: 58·6 % v. 41·4 %; χ 2 = 12·96, P = 0·0003; control: 63·9 % v. 36·1 %; χ 2 = 6·64, P = 0·01).
Table 3 enumerates the characteristics of respondents and differences between the two groups at pre-test. Several differences were noted. In particular, compared with respondents from the experimental group, a higher proportion of those from the control group were boys, were older, stayed less often in school for lunch, reported going more often to fast-food restaurants and had a less positive predisposition towards the target behaviour. Differences were also observed between drop-outs and participants included in the analysis. Compared with participants included in the analysis, a higher proportion of drop-outs were enrolled in the general programme (55·2 % v. 41·5 %; χ 2 = 5·21, P = 0·02), were slightly older (14·70 (sd 1·45) years v. 14·02 (sd 1·48) years; t = −3·82, P = 0·0002), reported eating lunch in school less frequently (9·07 (sd 1·77) d v. 9·52 (sd 0·97) d; t = 2·34, P = 0·02) and perceived fewer advantages of eating in school (3·87 (sd 0·86) v. 4·07 (sd 0·71); t = 2·07, P = 0·04).
Table 3 Baseline characteristics of respondents and differences between the experimental and control groups at pre-intervention: high-school students aged 12 to 17 years, central Canada, September 2009
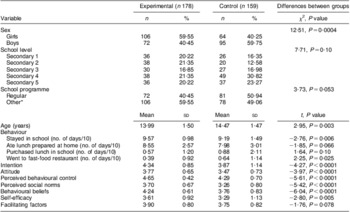
*Other programme: experimental = international education; control = information technology.
Intervention effect on behaviour
Table 4 presents descriptive statistics on the different behavioural patterns adopted by students in the lunch period. The proportion of experimental group students who went to fast-food restaurants at least once during the last ten school days before the intervention was 24·0 % compared with 17·2 % after the intervention; proportions in the control group were 32·7 % and 31·5 %, respectively. Poisson regression analysis controlling for age and past behaviour showed that the intervention had a significant effect on the mean number of days that students stayed in school for lunch (relative risk (RR) = 1·55; 95 % CI 1·06, 2·27; P = 0·024; Fig. 2). Similar results were obtained with intention-to-treat analysis (RR = 1·53; 95 % CI 1·13, 2·09; P = 0·006). No moderating effects of sex, school programme and school level were apparent.
Table 4 Number of days out of last ten school days that high-school students aged 12 to 17 years adopted different behaviours during lunch time, pre- and post-intervention, according to school; central Canada, September 2009 (pre) and May 2010 (post)

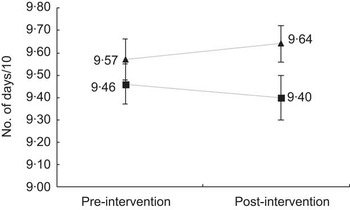
Fig. 2 Number of days out of last ten school days that high-school students aged 12 to 17 years stayed in school for lunch, pre- and post-intervention, according to school (—▴—, experimental, n 129; —▪—, control, n 112); central Canada, September 2009 (pre) and May 2010 (post). Values are means with their standard errors represented by vertical bars
Log-binomial regression analysis compared students who stayed in school every day over a 10 d period with those who stayed 9 d or less, also controlling for age and past behaviour. Again, a significant intervention effect was seen (RR = 1·21; 95 % CI 1·04, 1·40; P = 0·014; Fig. 3). Similar results were obtained with intention-to-treat analysis (RR = 1·18; 95 % CI 1·05, 1·33; P = 0·005). The goodness-of-fit test demonstrated good fit of the model with no significant results (χ 2 = 22·79, P = 0·29). No moderating effects of sex, school programme and school level were observed.

Fig. 3 Comparison of the proportions of high-school students aged 12 to 17 years who stayed in school for lunch every day during the last ten school days, pre- ( $$$$) and post-intervention (
$$$$) and post-intervention ( $$$$), according to school (experimental, n 129; control, n 112); central Canada, September 2009 (pre) and May 2010 (post)
$$$$), according to school (experimental, n 129; control, n 112); central Canada, September 2009 (pre) and May 2010 (post)
Mediating analyses of theoretical variables
Table 5 reports the changes in psychosocial variable means (i.e. intention, perceived behavioural control, perceived social norms, attitude, behavioural beliefs, self-efficacy and facilitating factors) between pre- and post-intervention. Controlling for the covariates sex, past behaviour and baseline self-efficacy, analysis of covariance disclosed a significant difference between the experimental and control schools for self-efficacy only (F(1, 241) = 3·92, P = 0·0489). Self-efficacy remained stable in the experimental group compared with a slight decline in the control group. Finally, bootstrapping mediation analysis revealed a significant mediating effect of self-efficacy on the mean number of days that students stayed in school for lunch (path a: 0·23, P = 0·049; path b: 0·34, P < 0·000001; path c: 0·12, P = 0·27; path c′: 0·05, P = 0·64; BCa point estimate = 0·079; 95 % CI 0·0059, 0·1958). No other variable had a significant indirect mediating effect.
Table 5 Mean scores for psychosocial variables among high-school students aged 12 to 17 years, pre- and post-intervention, according to school; central Canada, September 2009 (pre) and May 2010 (post)
*P ≤ 0·049.
Discussion
The present study was undertaken to measure the effect of an intervention programme aimed to encourage high-school students to stay in school for lunch instead of eating in fast-food restaurants. The results showed the usefulness of our intervention in enhancing the mean number of days that students stayed in school as well as the proportion of students who stayed in school every day to eat either a lunch prepared at home or a meal purchased in the school cafeteria. The study ascertained that self-efficacy was the only theoretical variable mediating this effect. Finally, only self-efficacy appeared to be influenced by the intervention, mainly because of a decline in control group values.
Programme development, implementation and evaluation were achieved in reference to the framework of intervention mapping(Reference Bartholomew, Parcel and Kok22). This model has already demonstrated its utility in guiding efficient health promotion interventions(Reference Bartholomew, Parcel and Kok22, Reference Côté, Godin and Gagné47–Reference Van Empelen, Kok and Schaalma49) and, more specifically, nutritional interventions among adults(Reference Guillaumie, Godin and Manderscheid50) and youngsters(Reference Hoelscher, Evans and Parcel51–Reference Reinaerts, De Nooijer and De Vries53). Within this framework, it is also recommended to use theories to plan interventions for the modification of target behaviours(Reference Kok, Schaalma and Ruiter23, Reference Godin54–Reference Webb, Joseph and Yardley59). In the context of the present study, the intervention was developed in reference to the theory of planned behaviour.
Although the mean number of days students stayed in school for lunch was already high before the intervention, a closer look at the results revealed that during the 10 d observation period, one student out of four in the experimental school and one student out of three in the control school went to fast-food restaurants for lunch at least once instead of eating a meal in school. Other studies(Reference Beaulieu and Godin21, 60) have reported similar or even more discouraging statistics, highlighting the importance of addressing the problem of fast-food consumption by adolescents.
In the present work, the mediating role of perceived self-efficacy highlights the importance of working on this variable to facilitate adoption of the target behaviour. Perceived self-efficacy refers to the individual's belief in his/her capacity to organize and execute an action. It determines if a behaviour will be initiated, the amount of effort made for its adoption and maintenance in the face of obstacles and difficult experiences(Reference Bandura61, 62). In the present study, the main intervention effect seemed to maintain the self-efficacy level in the experimental group, whereas it declined slightly in the control group. Many programme components were based on Bandura's recommendations for improving self-efficacy, such as direct experience and vicarious observation (e.g. cooking sessions), as well as social persuasion (e.g. posters, custom-made pamphlets, electronic and audio messages). Thus, the theoretical methods and practical applications for changing perceived self-efficacy listed in Table 1 appear to be effective in this setting and in the target group, as confirmed by some insight from the process evaluation (data not reported).
Nevertheless, the role of self-efficacy as a mediator of intervention effectiveness in changing health-related behaviour appears to be inconsistent. In fact, two important reviews of dietary behaviour change interventions among youngsters did not identify a mediating role of self-efficacy(Reference Cerin, Barnett and Baranowski63, Reference van Stralen, Yildirim and te Velde64). Similarly, Guillaumie et al.(Reference Guillaumie, Godin and Manderscheid50) did not observe a mediating effect of this variable on fruit and vegetable consumption among adults. However, self-efficacy was a mediator of the intervention effect promoting physical activity(Reference van Stralen, Yildirim and te Velde64) and smoking cessation among adolescents(Reference Bricker, Liu and Comstock65). More research is required to determine the precise role of self-efficacy in interventions aimed at improving nutritional behaviours as well as to identify specific means and approaches to empirically enhance self-efficacy. Clarification of the process involved could help to develop more appropriate interventions. Indeed, programmes could be enriched by the recognition of important components, and their cost could be reduced by removing those that are ineffective(Reference Cerin and MacKinnon66).
In the present study we adopted a multi-component programme that included many behavioural change methods and practical applications targeting specific behavioural determinants. This approach appears to be successful in encouraging students to stay in school for lunch and is in agreement with the observation of Webb et al.(Reference Webb, Joseph and Yardley59) that interventions incorporating more behaviour change techniques have a higher probability of being effective. The behavioural change methods applied in the present programme were selected mainly from those suggested by health and clinical psychologists with expertise in developing and implementing behaviour change interventions(Reference Bandura26–Reference Michie, Johnston and Francis28, Reference Bartholomew, Parcel and Kok67).
Notwithstanding the positive results reported above, the overall effect remains modest. The lack of intervention efficacy in positively changing most targeted theoretical variables could reflect a ‘ceiling effect’, since the targeted cognitions were already relatively high at baseline. In addition to the ceiling effect, season was a factor that could have limited the impact of our intervention. Indeed, the arrival of warmer days in spring could have impacted the results. At that time of the year, students are tempted to leave the school yard to eat in fast-food restaurants, as observed in a previous study(Reference Beaulieu and Godin21). Moreover, as reported during process evaluation, students and parents are usually more motivated to prepare lunch at the beginning than at the end of the school year. It is also possible that our intervention acted on other unknown cognitions that were not measured or targeted, such as social climate during the study period. Nevertheless, the intervention maintained the self-efficacy level in the experimental group compared with a slight decrease observed in the control group.
Some study limitations must be addressed. First, the response rate was lower than 50 %, and differences between completers and drop-outs at baseline might have introduced a bias in the findings since it is likely that more students interested in the behaviour may have agreed to participate and complete the whole study. The results could have been different if less motivated students had participated in larger numbers. However, intention-to-treat analysis confirmed the main observations and provided some confidence in the study results. Second, only two schools were involved in the present evaluative study. Caution must be exercised before generalizing the findings. Additional investigations are required before a more definite conclusion can be reached. Third, the results were obtained after relatively short-term follow-up. It is necessary to verify if the gains achieved with this intervention can be sustained over a longer time period. Fourth, intervention implementation was not optimal. For example, the list of parents’ email addresses was not complete; 30 % of email addresses were missing. Consequently, many parents did not receive the four electronic messages sent. Also, since students’ email addresses were not available, only those who joined the Facebook student group (51 % of respondents) saw the four electronic messages. Nevertheless, parents and students who were not reached may have had access to educational message content if they consulted the school website. Fifth, given budget limitations, not all students participated in the cooking sessions offered; only 11 % of respondents had the opportunity to participate in these sessions. Finally, sample size was not optimal to test all aspects of the study.
Conclusions
To the best of our knowledge, the present study is the first to evaluate an intervention aimed at increasing the number of students staying in school for lunch. Our theory-based intervention was effective in reaching its goal, demonstrating that it is feasible to implement interventions addressing the problem, and should contribute towards improving the eating habits of high-school students. These results should also help to generate evidence-based data to guide government authorities, school leaders and health professionals in developing and executing appropriate interventions among young people and their families to promote the adoption of better nutritional habits.
Acknowledgements
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. D.B. was supported by grants from the ‘Ministère de l’Éducation, du Loisir et du Sport du Québec’, Laval University and the Heart and Stroke Foundation of Canada. G.G. is holder of the Canada Research Chair on Behaviour and Health funded by the Canadian Institutes of Health Research. The authors declare that they have no competing interests. D.B. contributed to questionnaire development; data collection, treatment, analysis and interpretation; development and implementation of the intervention; and manuscript editing. G.G. contributed to questionnaire development; data analysis and interpretation; critical review of intervention material; and manuscript editing. The authors thank Roseline Drolet, France St-Onge and members of Health Action Committee of Rochebelle High School for their numerous collaborations in the performance of this project. They also thank Léo-Daniel Lambert for data analysis, Lydi-Anne Vézina-Im and Andréa Bilodeau for their help in the intervention implementation and manuscript revision.