



Adherence to the Mediterranean diet, which is believed to be a healthy diet, has been widely associated with good human health. In 2010, the Mediterranean diet was registered on the Representative List of the Intangible Cultural Heritage of Humanity by the United Nations Educational, Scientific and Cultural Organization, as it constitutes ‘a set of skills, knowledge, practices and traditions ranging from the landscape to the table, including the crops, harvesting, fishing, conservation, processing, preparation and, particularly, consumption of food’( 1 ).
The traditional Mediterranean diet is characterized by high consumption of fruits and nuts, vegetables, legumes and unprocessed cereals, and low consumption of meat and dairy products. Although alcohol consumption is common in the traditional Mediterranean diet, it is generally in the form of wine, in moderation and, as a rule, only during meals. Total lipid intake can be high (about or in excess of 40 % of total energy intake, as in Greece) or moderate (about 30 % of total energy intake, as in Italy); however, in all instances, the ratio of the beneficial monounsaturated to the non-beneficial saturated lipids is high, owing to the high MUFA content of olive oil, which is used liberally. Finally, because of its proximity to the ocean, moderate amounts of fish can be consumed( Reference Trichopoulou, Costacou and Bamia 2 ).
The traditional Mediterranean dietary pattern was reported by Keys and colleagues in the Seven Countries Study( Reference Keys, Arvanis and Blackburn 3 ). An important conclusion of their study, based largely on ecological evidence, was that the low saturated lipid content of the Mediterranean diet could explain the low incidence of CHD in Mediterranean countries.
One of the reasons why epidemiological studies on the Mediterranean diet have been conducted worldwide was the development of the Mediterranean diet score (MDS). The Mediterranean diet was conceptualized in the 1960s to reflect the meals that were typically eaten in the coastal areas of the Mediterranean (Southern Italy, Greece, especially in Crete, etc.)( Reference Willett, Sacks and Trichopoulou 4 ). It is essentially a frugal diet that was traditionally followed by poor rural societies( Reference Bach-Faig, Berry and Lairon 5 ). Among a variety of versions, the MDS created by Trichopoulou et al. in 1995 and updated thereafter( Reference Trichopoulou, Costacou and Bamia 2 ) is used most widely( Reference Trichopoulou, Kouris-Blazos and Wahlqvist 6 , Reference Bach, Serra-Majem and Carrasco 7 ). A gradient of adherence to the traditional Greek Mediterranean diet was constructed from nine nutritional components (fruits and nuts; vegetables; legumes; cereals; fish; olive oil; meat and poultry; dairy; wine), with values of 0 or 1 assigned to each component using the medians as cut-off values.
In a recent systematic review and meta-analysis, Grosso et al.( Reference Grosso, Marventano and Yang 8 ) reported finding an association between adherence to the Mediterranean diet and lower incidence of and mortality from CVD, including CHD, myocardial infarction and stroke. The most protective effects were associated with increased consumption of olive oil, fruits, vegetables, legumes and nuts, and moderate intake of wine (especially red wine).
However, the relationship between MDS and the incidence of IHD has yet to be elucidated in any global international comparative studies. Therefore, the purpose of the present study was to clarify the relationship between MDS and the incidence of IHD using population data from global international databases.
Methods
Variables
Incidence of IHD
The Global Burden of Disease (GBD) database is the most comprehensive source of comparable summary population health measures because of its inclusion of country-level results, uncertainty quantification and effort to maximize comparability across space, time and different health conditions( 9 ). For the purposes of the present study, we used the age-standardized incidence of IHD per 100 000 people in 2010.
Food supply
Covering all regional groupings of the FAO from 1961 to the most recent year available, the FAOSTAT database provides food and agricultural data for more than 245 countries and territories( 10 ). We examined the most recent data (since 2010) using 129 animal and vegetable food supply items after excluding the duplicates.
Mediterranean diet score
MDS were calculated according to the most commonly used index by Trichopoulou et al.( Reference Trichopoulou, Costacou and Bamia 2 ). Items corresponding to the nine food components that comprise the MDS (vegetables; legumes; fruits and nuts; cereals; fish; olive oil; meat and meat products; dairy products; wine) were extracted. Each component was calculated as the daily supply per capita (g/d per capita). In the present study, the amount of olive oil consumed, rather than the ratio of monounsaturated to saturated lipids, was used. The amount of ethanol from wine was used as the amount of wine intake. The presumed beneficial components (vegetables, legumes, fruits and nuts, cereals, fish and olive oil) below the medians of the countries were assigned a value of 0, and 1 otherwise. By contrast, the presumed detrimental components (meat and dairy) below the medians were assigned a value of 1, and 0 otherwise. To calculate alcohol intake, we modified the MDS based on 50 g of ethanol as a standard according to median alcohol intake values. The amount of wine consumed (as ethanol) was rated as 1 for over 50 g, and 0 otherwise. Calculations were made for supply amount per 4184 kJ (1000 kcal), except for wine. Therefore, a 10-point MDS that could take a value from 0 (minimal adherence) to 9 (maximal adherence) was constructed.
Covariables
Food energy supply (kcal/d per capita) was determined based on the FAOSTAT database. Gross domestic product (GDP) per capita ($US/capita) and years of education were identified using data from the United Nations Educational, Scientific and Cultural Organization Institute for Statistics’ database( 11 ). Current smoking rates were identified using data from the GBD database( 9 ). The prevalence of obesity (BMI ≥30·0 kg/m2) was calculated based on the WHO database( 12 ). The percentage of the population over 65 years of age (ageing rate) and health expenditures ($US/capita) were identified using the World Bank database( 13 ). The most recent data available (since 2010) in all databases were used.
Statistical analysis
Analysis was conducted for the 132 countries with a population of over 1 million and no missing data. Each country was divided into two groups based on the MDS – low-score countries (≤median) and high-score countries (>median) – and then food supply amounts and socio-economic and lifestyle variables were compared between the groups using the t test. The interrelationships among these variables were assessed by single and partial correlation analyses controlled for covariables.
The effects of MDS on the incidence of IHD were evaluated using three general linear models. Model 1 was a single regression model of MDS v. the incidence of IHD; Model 2 was a multiple regression model controlled for GDP per capita; and Model 3 was a multiple regression model further controlled for socio-economic and lifestyle variables. Akaike’s information criterion was used as an estimator of the relative quality of models and the Bayesian information criterion was used as a criterion for model selection. To eliminate multiple collinearity, the variance inflation factor was calculated and variables were chosen so that the variance inflation factor of all variables was 10 or less. R version 3.3.3( 14 ) was used for all analyses and values of P<0.05 were taken to indicate statistical significance.
Results
MDS were distributed from 1 to 8 points and were not invariably high in the Mediterranean countries. MDS were generally higher in Asian and African countries, and generally lower in South American, Northern European, Eastern European and former Soviet bloc countries (Fig. 1).
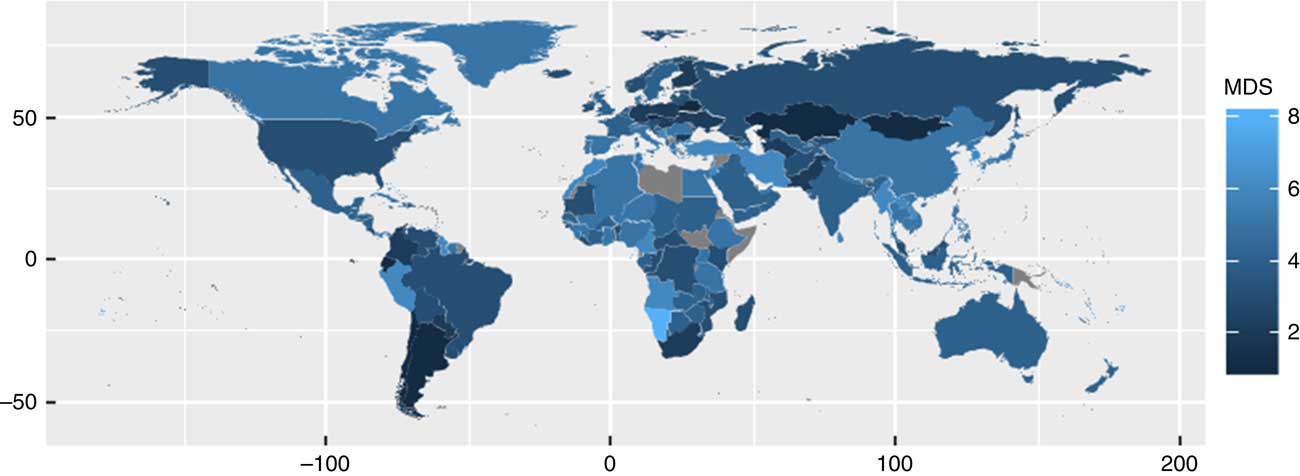
Fig. 1 Global distribution of Mediterranean diet score (MDS) by country. For the countries shown in grey, no data on food supply after 2010 were obtained
The characteristics of countries with high and low MDS are shown in Table 1. The median score was 3. The incidence of IHD was significantly lower in countries with a high than in countries with a low MDS (P=0·014). In countries with higher scores, the supplies of fruits and nuts, vegetables and legumes were significantly higher, and those of dairy products and meat were significantly lower, compared with countries with lower scores. No significant differences were seen in cereals, fish, olive oil or wine. Regarding socio-economic variables, countries with higher MDS had lower ageing rates and fewer years of education compared with countries with lower scores. Regarding lifestyle variables, countries with higher scores had lower smoking rates.
Table 1 Characteristics of countries with low and high Mediterranean diet score (MDS) in global international databases
GDP, gross domestic product.
Analysis was conducted for the 132 countries with a population of over 1 million without missing data. Each country was divided into two groups based on MDS. Food supply and socio-economic and lifestyle variables were compared between the two groups using the t test.
† The median MDS was 3. A score of 0 indicates minimum adherence and a score of 9 indicates maximum adherence.
‡ Student’s t test.
Table 2 shows the single and partial correlation coefficients controlled for covariables. The results of single correlation analysis showed that the incidence of IHD was inversely correlated with GDP, life expectancy and health expenditure. MDS were inversely correlated with ageing rate, education, obesity rate and IHD, but were not related to GDP, life expectancy, health expenditure, smoking rate or energy supply. The single correlation coefficient between MDS and the incidence of IHD was −0·245 (P<0·01).
Table 2 Single correlation coefficients of the Mediterranean diet score (MDS), IHD and eight variables (upper triangle), and partial correlation coefficients controlled for all other variables (lower triangle), in 132 countries with a population of over 1 million in global international databases

GDP, gross domestic product; Life exp., life expectancy (years); Health exp., health expenditure (1000 $US/capita).
*P<0·05, **P<0·01, ***P<0·001.
The results of partial correlation analysis controlled for covariables showed that the incidence of IHD was inversely correlated with GDP and life expectancy, and positively correlated with education, smoking rate and energy supply. MDS were inversely correlated with obesity rate and IHD. The partial correlation coefficient between MDS and the incidence of IHD was −0·209 (P<0·05).
The relationship between MDS and the incidence of IHD is shown in a bubble chart in Fig. 2, with bubble size representing the GDP per capita. The score in Japan was 5, the same as those for Italy, Spain and Greece, which were all higher than the score of 4 points in France. The single regression line between MDS and the incidence of IHD was y=−26·1x+482·9.
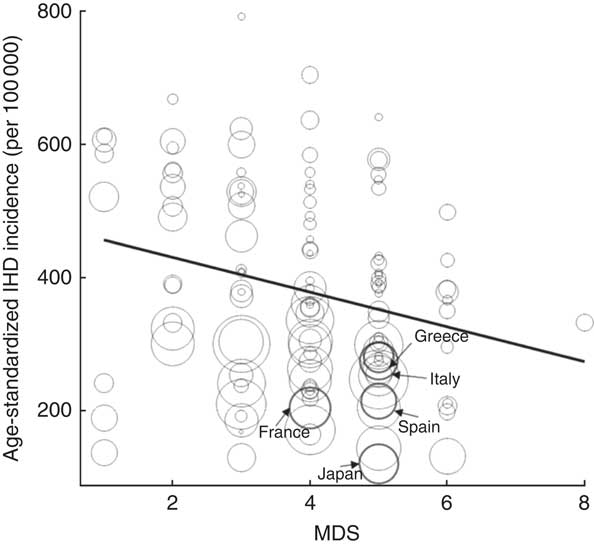
Fig. 2 Mediterranean diet score (MDS) and age-standardized incidence of IHD in the 132 countries with a population of over 1 million in global international databases. Bubble size represents the gross domestic product per capita of each country; ![]() represents the regression line (y=−26·1x+482·9)
represents the regression line (y=−26·1x+482·9)
Table 3 shows the results of the three general linear models for the incidence of IHD. In Model 1, the single regression coefficient (β) of the MDS was −26·1 (se 9·1; P<0·001). In Model 2, the partial regression coefficient controlled for GDP per capita was −28·5 (se 8·3; P<0·001). In Model 3, the partial regression coefficient of the MDS controlled for GDP, ageing rate, education, smoking rate, energy supply and obesity rate was also significant (−26·4 (se 8·6), P<0·01). In the model in which both GDP and health expenditure were included, the variance inflation factor of GDP and health expenditure was 18·2 and 16·7, respectively. Therefore, health expenditure was excluded from the covariables in Model 3. Akaike’s information criterion was lowest in Model 3 and the Bayesian information criterion was lowest in Model 2.
Table 3 Partial regression coefficients of Mediterranean diet score (MDS) and covariables in three general linear models for the incidence of IHD in 132 countries with a population of over 1 million in global international databases
GDP, gross domestic product; AIC, Akaike’s information criterion; BIC, Bayesian information criterion.
**P<0·01, ***P<0·001.
Discussion
Using population data from global international databases, the present study provides the first evidence of a significant relationship between the Mediterranean diet and the incidence of IHD. This association remained after controlling for socio-economic and lifestyle variables.
The Mediterranean diet, which is regarded as one of the world’s healthiest, has been followed and protected by residents of Mediterranean countries for a long time. Numerous studies have been conducted on the Mediterranean diet, including that by Trichopoulou et al.( Reference Trichopoulou, Costacou and Bamia 2 ).
The health benefits of the Mediterranean diet have been widely researched in the past, particularly in terms of the incidence of CVD( Reference Estruch, Ros and Salas-Salvado 15 – Reference Martinez-Gonzalez and Bes-Rastrollo 18 ) and the prevention of type 2 diabetes( Reference Martinez-Gonzalez, de la Fuente-Arrillaga and Nunez-Cordoba 19 , Reference Salas-Salvado, Bullo and Estruch 20 ) and metabolic syndrome( Reference Kastorini, Milionis and Esposito 21 ). The European Prospective Investigation into Cancer and Nutrition (EPIC) study has also reported some benefits of the Mediterranean diet against the occurrence of cancer. Evidence of the potential protection provided by the Mediterranean diet seems stronger for gastric, colorectal and breast cancers, especially when alcohol is excluded from the definition( Reference Couto, Boffetta and Lagiou 22 , Reference Buckland, Travier and Cottet 23 ). In addition, many systematic reviews and meta-analyses have reported the beneficial effects of the Mediterranean diet, and the reliability of these results is considered high( Reference Sofi, Abbate and Gensini 24 , Reference Daniele, Noce and Vidiri 25 ). However, we could not find any studies that analysed a large number of countries simultaneously using the same scoring method. According to the results of the present study, MDS are high in countries in Asia as well as those in the Mediterranean region.
According to the GDB database, the annual global incidence of IHD in 2010 was estimated to be 379·7 per 100 000 persons( 9 ). From this value and the results of the present study, the incidence of IHD is expected to decrease by 7·1 % for every 1-point increase in MDS. This suggests the importance of maintaining a healthy diet based on meals rich in fish, vegetables, fruits and cereals.
Scientific evidence has shown that the adoption of the Mediterranean diet is a protective factor against the onset of various types of CVD, cancer, ageing and obesity. As shown by the EPIC study, the Mediterranean diet is most effective for the prevention of several chronic diseases, including cancer. The anti-tumour effects of the Mediterranean diet owe mostly to the combination of antioxidants, fibre and polyunsaturated fats. This dietary pattern is therefore essential as a preventive measure against all-cause mortality( Reference Menotti, Kromhout and Puddu 26 , Reference Martínez-González and Sánchez-Villegas 27 ).
In the present study, the intakes of wine, olive oil and grains were not necessarily high in the countries with high MDS. The reason for this may be because of differences in eating habits by region( Reference Davis, Bryan and Hodgson 28 ). For example, wine and olive oil are consumed on a daily basis in a limited number of countries; in traditional dishes in Asian countries, these foods are rarely used.
The results of such an analysis could be expected to vary depending on the scoring method. For example, our research results have issues, such as including both red and white wine. For more detailed and accurate analyses, it may be necessary to develop a new scoring method focusing on ‘groups of foods susceptible to food culture’. If food intake is replaced with nutrient intake, it may be possible to adjust food differences in accordance with differences in food culture and to propose dietary contents to be ingested for each area of the world. Some recent papers have weighted the Mediterranean diet on a nutrient basis( Reference de Lorgeril, Salen and Martin 29 , Reference Kafatos, Verhagen and Moschandreas 30 ) or created nutrient scores( Reference Buckland, González and Agudo 31 – Reference Guallar-Castillon, Rodriguez-Artalejo and Tormo 33 ). Furthermore, a variety of MDS, such as the alternative and relative MDS( Reference Fung, Rexrode and Mantzoros 34 ) and Mediterranean Adequacy Index( Reference Fidanza and Fidanza 35 ), have been developed; however, evidence of the validity of these scores remains insufficient.
In the present study, we used the score created by Trichopoulou et al.( Reference Trichopoulou, Costacou and Bamia 2 ). We initially included fruits in the score, but fruit consumption is associated with higher socio-economic status, which, in turn, is associated with a comparatively higher consumption of meat( Reference Dubowitz, Heron and Bird 36 ); this could pose some problems regarding the inclusion of fruits as a variable in the score calculation. Therefore, we conducted an additional analysis excluding fruits. However, no relationship was found between MDS and the incidence of IHD in the correlation or regression analyses. This seems to indicate that fruits play an important role in preventing IHD. Additionally, a previous study reported that higher consumption of fruits is associated with a lower risk of all-cause mortality, particularly cardiovascular mortality( Reference Dubowitz, Heron and Bird 36 ). Consequently, we used Trichopoulou’s score, including fruits as a variable.
To calculate alcohol intake, we modified the MDS based on 50 g of ethanol as a standard based on median alcohol intake values. There are ongoing discussions about the effect of ethanol intake, but considering past research about the cardiovascular protective effects of ethanol, ethanol intake was used in the score calculations( Reference Chiva-Blanch, Arranz and Lamuela-Raventos 38 , Reference Roerecke and Rehm 39 ).
We also performed a sensitivity analysis on the impact of MDS on IHD. In the analysis, the annual incidence rate per 100 000 cases of IHD was estimated to be 457·5 at the lowest MDS value and 272·9 at the highest (full adjustment model). The sensitivity analysis between each food group and MDS showed that legumes had the greatest influence on MDS, followed by meat, dairy products, fish, fruits, vegetables and cereals. Olive oil and wine were found to have only a slight influence, likely owing to the fact, from a global point of view, that intake of olive oil and wine is extremely low for most countries.
The present study has several limitations. First, the results consist of country data, not personal data, and it was not possible to analyse by sex or age group. Second, MDS were not calculated based on the actual consumption of foods. The amount of waste at home was considered, but because the disposal rate did not differ greatly depending on the food, the effects of the difference between supply and consumption amounts per 4184 kJ (1000 kcal) would be not large. Physical activity is an important factor in relation to the incidence of IHD. However, it is virtually impossible to conduct accurate and objective dietary surveys simultaneously around the entire world. In the present study, we used objective data obtained from almost all the countries in the world for the analysis; however, we could not obtain data on physical activity. We obtained inactivity data from the WHO database( 40 ). Although these data, which were obtained from citizens in 108 countries, were incomplete, the association between MDS and the incidence of IHD in the regression model controlled for inactivity, in addition to GDP, ageing rate, years of education, smoking and obesity, was still significant (β=−20·3 (se 9·2); P<0·05).
Several studies have investigated the relationship between the Mediterranean diet and the incidence of IHD by summarizing data from cohort studies in several countries and regions; however, no global-scale studies have been conducted. Similar to previous studies, the results of the present study using population data from global international databases suggest that the Mediterranean diet may be effective for the prevention of IHD. In fact, following the Mediterranean diet may have greater preventive effects on IHD than other lifestyle variables such as smoking, obesity and exercise.
Acknowledgements
Financial support: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. Conflict of interest: The authors have no conflicts of interest to disclose. Authorship: A.S., T.I., K.M., F.K. and H.S. formulated the research question. A.S. and H.S. designed the study. A.S. carried out the study. A.S., F.K. and H.S. analysed the data. A.S. and H.S. wrote the article. Ethics of human subject participation: Not applicable.





