


Open-angle glaucoma (OAG) is one of the major chronic diseases involving the optic nerve. It is the leading cause of irreversible blindness and a recent report suggested that by 2020 the disease will affect approximately 59 million people globally( Reference Quigley and Broman 1 ). If OAG is not treated timely, severe vision loss can result from progressive optic neuropathy. Generally, OAG is characterized by progressive visual field loss and glaucomatous optic disc change with loss of retinal nerve fibre tissues( Reference Quigley 2 ). Since these processes are chronic and irreversible, medical practitioners are striving to understand the risk factors associated with the development of glaucoma.
There are two types of glaucoma: angle-closure glaucoma (ACG) and OAG. While it is known that the damage to the optic nerve due to ACG results from obstruction of the outflow of aqueous humour, with the elevation of intraocular pressure (IOP), the pathophysiology of OAG is not yet fully understood( Reference Quigley 2 ). Recent studies have described that OAG is not only an IOP-induced disease of the optic nerve, but also an age-related and neurodegenerative chronic disease( Reference McKinnon 3 , Reference Yanagi, Kawasaki and Wang 4 ). IOP-induced stress, such as elevated IOP and fluctuation of IOP, compresses the structures around the optic nerve and can lead to damage in the retina and the optic nerve by disturbing the axonal transport of trophic molecules within the nerve fibres( Reference Quigley 2 ). Emerging evidence is showing that poor ocular blood flow and neurodegenerative change also contribute to OAG pathophysiology( Reference Yanagi, Kawasaki and Wang 4 ). Poor ocular blood flow due to vascular dysfunction may cause OAG by chronic ocular ischaemia and interruption of nutrient supply to the optic nerve( Reference Flammer and Orgül 5 ). Neurodegenerative effects due to ageing, inflammation and metabolic stress have also been reported as factors contributing to glaucomatous optic neuropathy( Reference McKinnon 6 ). All these risk factors influence each other and have complex effects on the development of OAG.
Recently, vitamin D has become a major interest area of medical researchers. Vitamin D is an important secosteroid hormone that plays a role in the signalling pathways related to bone and mineral metabolism, cellular proliferation, immune modulation and the oxidative-stress system( Reference Hossein-Nezhad and Holick 7 , Reference Tarcin, Yavuz and Ozben 8 ). In general, 25-hydroxyvitamin D (25(OH)D) is accepted as the most reliable biomarker for assessing individual vitamin D status. Based on the results of serum 25(OH)D measurements in large population-based studies, it is seen that vitamin D deficiency may be associated with neurodegenerative effects on the central nervous system( Reference Balion, Griffith and Strifler 9 , Reference Van der Schaft, Koek and Dijkstra 10 ). Several biological experiments have suggested that vitamin D regulates the functions of neuroprotection in the central nervous system, including in the optic nerve( Reference Schreiner, Jande and Lawson 11 , Reference Lucas, Ponsonby and Dear 12 ). Moreover, vitamin D status can also affect chronic metabolic diseases, including diabetes, hypertension and dyslipidaemia, which are considered as the important metabolic risk factors of elevated IOP and reduced ocular blood flow( Reference Yanagi, Kawasaki and Wang 4 , Reference Oh, Lee and Park 13 ). Therefore, it can be hypothesized that vitamin D status is associated with the development of chronic optic neuropathy, i.e. OAG. However, until now, little is known concerning the epidemiological association of vitamin D status with OAG.
The present study was conducted to test the hypothesis that lower vitamin D status is associated with a greater prevalence of OAG. We investigated the relationship between the presence of OAG and serum 25(OH)D level, with adjustment for traditional potential confounders, using information from a cross-sectional, nationwide health survey. In addition, to elucidate the effects on glaucomatous changes, we examined serum 25(OH)D level in relation to IOP, which is considered to be the most important predictor of glaucoma, and vertical and horizontal cup-to-disc ratios of the optic nerve head, which reflect the structural change of the optic nerve head( Reference Quigley 2 , Reference Read and Spaeth 14 ).
Methods
Study population
The current study was based on health records collected from the Fifth Korean National Health and Nutrition Examination Survey (KNHANES V; http://knhanes.cdc.go.kr/knhanes) conducted in 2010 and 2011. The KNHANES V is a nationwide and population-based cross-sectional survey that was conducted by the Division of Chronic Disease Surveillance, Korea Centers for Disease Control and Prevention( Reference Oh, Lee and Lee 15 ). The KNHANES V consists of health records based on a health interview, a health examination and a nutritional survey. All participants for KNHANES V were randomly selected from 192 surveys in 131 locations using stratified sampling, considering population, gender, age, regional area and type of residential area. The protocol for our study was approved by the institutional review board at the Korea Centers for Disease Control and Prevention, Seoul, South Korea. All participants signed forms consenting to the use of their health information for the study.
A total of 17 476 participants were enrolled in the KNHANES V. We restricted the study population to middle-aged and elderly participants, who are generally considered at high risk of OAG( Reference Ekström 16 ). We excluded participants younger than 45 years of age (n 9607) and those not having an eye examination done (n 466). Participants with age-related macular degeneration and diabetic retinopathy (n 872) were excluded, since these diseases are the major causes of disturbance in visual field testing for the diagnosis of glaucoma( Reference Ramrattan, Wolfs and Panda-Jonas 17 ). To investigate a specific association between vitamin D and OAG, we also excluded participants without a 25(OH)D measure (n 432) and with ACG (n 5). Finally, 6094 participants were eligible for the current study (Fig. 1).
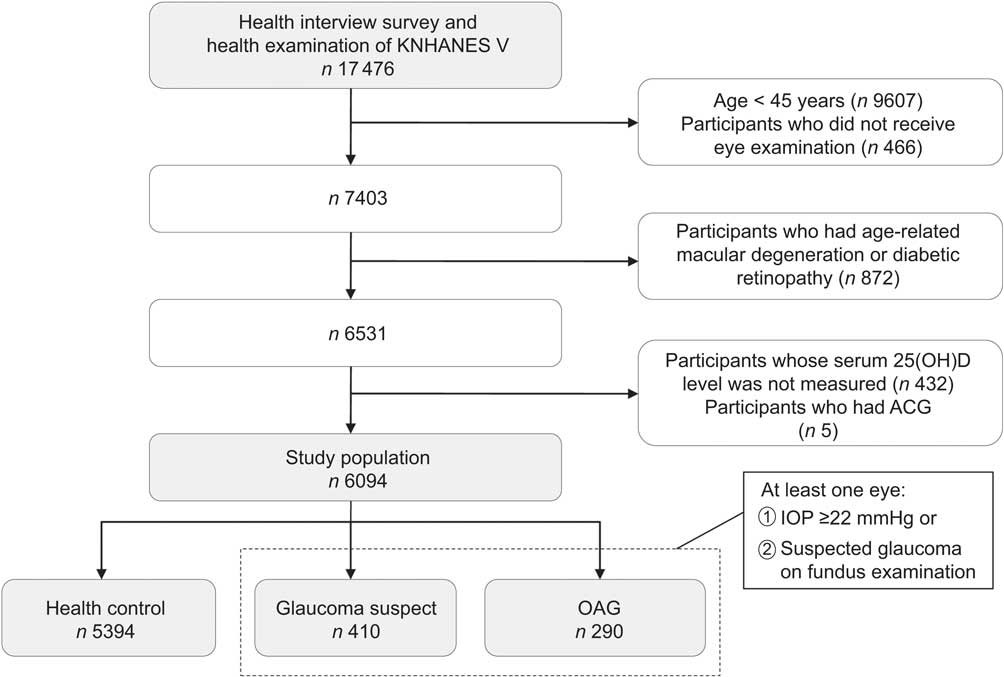
Fig. 1 Flow diagram of inclusion or exclusion of study participants from the Fifth Korean National Health and Nutrition Examination Survey (KNHANES V). OAG, open-angle glaucoma; 25(OH)D, 25-hydroxyvitamin D; ACP, angle-closure glaucoma; IOP, intraocular pressure
Ophthalmologic examination
A structured slit-lamp examination for evaluation of glaucoma status was performed. The slit-lamp examination was performed for determination of diseases in the anterior segment of the eye and measurement of the IOP and anterior chamber depth using the Van Herick method. A digital non-mydriatic fundus camera and a Nikon D-80 digital camera (Nikon Inc., Tokyo, Japan) were used to obtain the digital fundus images. Digital images were captured from all participants under physiological mydriasis. Visual field testing using Humphrey Matrix (Carl Zeiss Meditec Inc., Dublin, CA, USA) was performed if the participants had elevated IOP (≥22 mmHg) or a glaucomatous optic disc. The glaucomatous optic disc included any of the following four conditions: (i) vertical or horizontal cup-to-disc ratio ≥0·5; (ii) presence of optic disc haemorrhage; (iii) presence of retinal nerve fibre layer defect; and (iv) violation of the ISNT rule (that normal eyes show a characteristic configuration for disc rim thickness of inferior > superior > nasal > temporal). All ophthalmologic examinations were done by a trained ophthalmologist or ophthalmology resident( Reference Yoon, Mun and Kim 18 ).
Finally, the participants were classified into three groups: (i) healthy control, (ii) glaucoma suspect and (iii) OAG. Participants with OAG were defined as meeting the diagnostic criteria of the International Society for Geographical and Epidemiological Ophthalmology (ISGEO)( Reference Foster, Buhrmann and Quigley 19 , Reference Chon, Qiu and Lin 20 ). The specific diagnostic criteria adopted for the Korean population were as follows( Reference Yoon, Mun and Kim 18 ): (i) the presence of frequency doubling technology (FDT) testing results, fixation error and false positive error ≤1; (ii) glaucomatous optic disc (loss of neuro-retinal rim with vertical or horizontal cup-to-disc ratio ≥0·6, or presence of optic disc haemorrhage, or presence of retinal nerve fibre layer defect, or violation of the ISNT rule); (iii) presence of an abnormal FDT testing result (at least one location of reduced sensitivity); and (iv) the presence of an open angle (peripheral anterior chamber depth >1/4 corneal thickness). Glaucoma suspects, who had structural glaucomatous change without visual field defect, were defined as having elevated IOP (≥22 mmHg) or a glaucomatous optic disc without OAG. When both eyes were eligible, one eye was randomly selected and used for the analyses.
Measurement of serum 25-hydroxyvitamin D
Fasting blood samples of individual participants were collected for measurements of serum 25(OH)D concentration. Blood samples were immediately refrigerated and transported to the Central Testing Institute in Seoul, South Korea. Blood samples were processed and analysed within 24 h after transportation. Serum 25(OH)D levels were measured using a γ counter (1470 Wizard; Perkin-Elmer Finland) with a RIA (Dia-Sorin, Stillwater, MN, USA). The inter-assay CV were 11·7 %, 10·5 %, 8·6 % and 12·5 % at 8·6, 22·7, 33·0 and 49·0 ng/ml, respectively( Reference Choi, Seo and Choi 21 ). For the present study, 25(OH)D was categorized into quintiles: ≥23·79 ng/dl (highest group, median: 27·41 ng/dl); 19·50–23·78 ng/dl (median: 21·29 ng/dl); 16·33–19·49 ng/dl (median: 17·77 ng/dl); 13·09–16·32 ng/dl (median: 14·77 ng/dl); and ≤13·08 ng/dl (lowest group, median: 11·00 ng/dl).
Assessment of covariates
Information on traditional glaucoma-related risk factors was obtained from face-to-face interviews. Each participant completed a questionnaire by providing information on age, smoking status (current smoker and non-smoker), sun exposure (≥2 h/d and <2 h/d), family history of glaucoma, migraine and cold hands. These confounding factors were identified from a previous study of a Korean population-based sample( Reference Kim, Kim and Park 22 ). Visual acuity was measured at a distance of 4 m using an international standard vision chart based on the LogMAR scale, which is an arithmetic progression with better acuity scoring a low number and worse acuity scoring a high number( Reference Hart, Chakravarthy and MacKenzie 23 ). Since impaired visual acuity is a risk factor for reduced physical function and can affect lifestyle associated with vitamin D synthesis and intake, visual acuity was recognized as a confounding factor( Reference Rubin, Roche and Prasada-Rao 24 ). It is widely recognized that metabolic status also contributes to the incidence of OAG( Reference Yanagi, Kawasaki and Wang 4 ). Therefore, we included blood pressure and several laboratory findings as confounders. Fasting blood samples were analysed in local community health centres. Measurements of serum biomarkers, including fasting glucose, total cholesterol and TAG, were taken. Blood pressure was also measured by the health professionals. To avoid collinearity between systolic and diastolic blood pressure in multivariable regression models, we selected systolic blood pressure as a covariate. When calculating the correlation matrix of all confounding variables, there was no multi-collinearity problem (all pair-wise Pearson's correlations r < 0·5).
Statistical analysis
Characteristics of the participants according to the category of glaucoma status were compared using the χ 2 test for categorized data and one-way ANOVA for continuous data. In multivariable analyses, we established three adjusted models. Model 1 was adjusted for sex, age, current smoking status, sun exposure, family history of glaucoma, migraine and cold hands. Model 2 was adjusted for variables in Model 1 plus metabolic factors which included systolic blood pressure, fasting glucose, total cholesterol and TAG. In Model 3, further adjustments were made for visual acuity and IOP. To assess the association of serum 25(OH)D level with OAG, we first used multivariable logistic regression to estimate the relevant odds ratios by 25(OH)D quintile; in this analysis we studied the two clinical outcomes: (i) OAG and (ii) glaucoma suspect or OAG. When a non-linear relationship was observed, a quadratic trend analysis was employed. In addition, we fitted generalized additive models with cubic spline regression to visualize the dose–response association between serum 25(OH)D level and OAG. The resulting spline models represented log odds ratio of OAG adjusted for variables in Model 3. We performed ANCOVA to calculate geometric means of IOP, vertical and horizontal cup-to-disc ratios according to 25(OH)D quintile, after adjusting for potential confounders. Geometric means were computed by performing the regression of the natural log-transformed values to improve approximation of a skewed distribution and taking back-transformation of the resulting log-transformed values. Multivariable linear regression models also were used to assess the association of continuous serum 25(OH)D level with IOP, vertical and horizontal cup-to-disc ratios. To test for the linear and quadratic trends across increasing categories of 25(OH)D, we treated the categories of each quintile as a simple continuous variable in a multivariable-adjusted model. We squared a centred linear trend variable of each quintile to assess quadratic trend( Reference Mukamal, Chung and Jenny 25 ). The Wald χ 2 test was used to test for interaction. We considered P < 0·05 as the indicator of statistical significance. All statistical analyses were completed using the statistical software packages IBM SPSS Statistics 18 and R software version 3·0·2 (The Comprehensive R Archive Network; http://cran.r-project.org).
Results
Characteristics of the participants by the category of glaucoma status are shown in Table 1. Our study population consisted of 5394 (88·5 %) healthy controls, 410 (6·7 %) with glaucoma suspect and 290 (4·8 %) with OAG. While some confounding variables, namely sex, age, family history of glaucoma, systolic blood pressure and visual acuity, differed significantly among the groups categorized by glaucoma status, there was no significant difference in serum 25(OH)D level. However, when the categorization was done by the quartiles of age, we observed a reverse J-shaped pattern with a slightly elevated proportion of participants with OAG in the first 25(OH)D quintile (≥23·79 ng/dl), the lowest proportion in the second quintile (19·50–23·78 ng/dl), and gradual increases for the third (16·33–19·49 ng/dl), fourth (13·09–16·32 ng/dl) and fifth quintiles (≤13·08 ng/dl; Fig. 2).
Table 1 Characteristics of individuals with healthy control, glaucoma suspect and open-angle glaucoma eyes among 6094 adult participants in the Fifth Korean National Health and Nutrition Examination Survey (KNHANES V), 2010–2011
OAG, open-angle glaucoma; SBP, systolic blood pressure; 25(OH)D, 25-hydroxyvitamin D; IOP, intraocular pressure.
*P < 0·05, **P < 0·001 v. healthy group.
†The χ 2 test or one-way ANOVA was used.
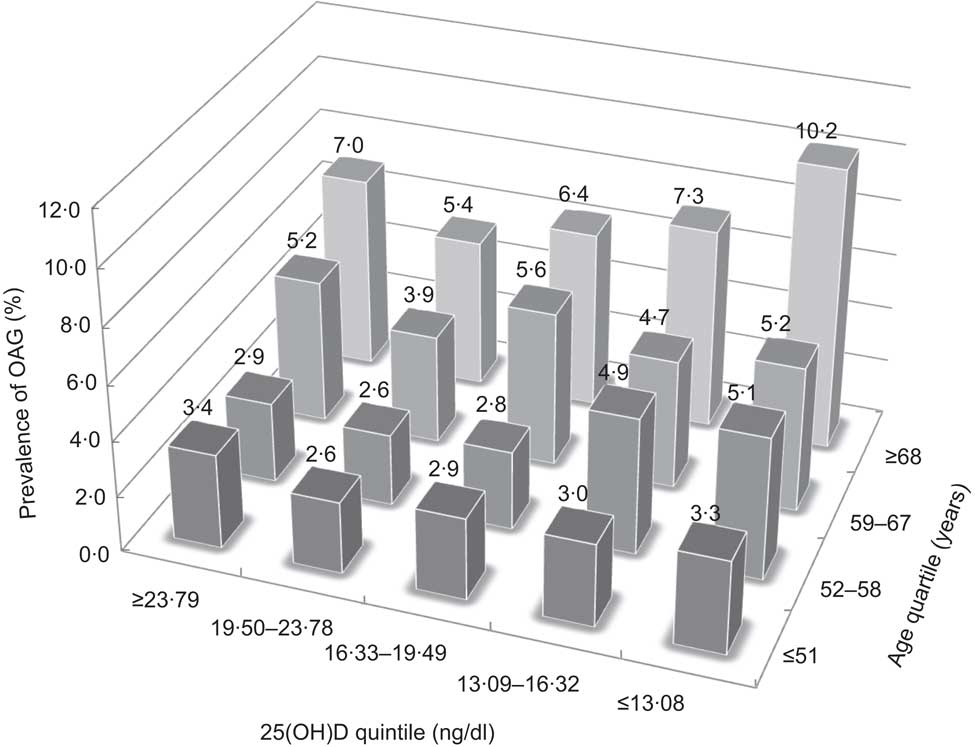
Fig. 2 Prevalence of open-angle glaucoma (OAG) calculated per quintile of serum 25-hydroxyvitamin D (25(OH)D) divided by quartile of age among 6094 adult participants in the Fifth Korean National Health and Nutrition Examination Survey (KNHANES V), 2010–2011
From the observation above, we hypothesized that there would be a quadratic relationship between serum 25(OH)D level and OAG. Table 2 shows the odds ratios of OAG and glaucoma suspect or OAG in adjusted analyses by serum 25(OH)D quintiles. The logistic regression in Model 1 showed that the association between 25(OH)D and OAG was reverse J-shaped (P for linear trend = 0·05 and P for quadratic trend <0·01). Compared with the second 25(OH)D quintile (the lowest quintile of OAG prevalence; Fig. 2), the adjusted odds ratios were 1·26, 1·31, 1·36 and 1·69 in the first, third, fourth and fifth quintiles, respectively. We observed that the fifth quintile (the lowest quintile of serum 25(OH)D level) had a significantly greater odds ratio referent to the second quintile (P < 0·01). The relationship between OAG and serum 25(OH)D level was substantially unchanged, even after adjustment for other confounders that were related to vitamin D status and risk of OAG (Model 2 and 3). After controlling for all confounding variables, odds ratios of OAG across decreasing quintiles of serum 25(OH)D level also showed a significant quadratic trend with a reverse J-shaped relationship (Model 3, P for quadratic trend = 0·02). Since the association was significant after adjustment for IOP (Model 3), these results might indicate an IOP-independent effect of serum 25(OH)D level. After stratifying the data according to sex, significance of the odds ratio trend was observed only in the male group (Model 3, P for quadratic trend = 0·01). There was no obvious trend in the female group (Model 3, P for quadratic trend = 0·39).
Table 2 Odds ratios of open-angle glaucoma and glaucoma suspect according to quintiles of serum 25-hydroxyvitamin D among 6094 adult participants in the Fifth Korean National Health and Nutrition Examination Survey (KNHANES V), 2010–2011
25(OH)D, 25-hydroxyvitamin D; OAG, open-angle glaucoma; Ref., referent category.
†Model 1 was adjusted for sex, age, current smoking status, sun exposure, family history of glaucoma, migraine and cold hands.
‡Model 2 was adjusted for variables in Model 1 plus systolic blood pressure, fasting glucose, total cholesterol and TAG.
§Model 3 was adjusted for variables in Model 2 plus visual acuity and intraocular pressure.
When the logistic regression analyses using continuous serum 25(OH)D level were conducted (Table 2), there was a significant change in adjusted odds ratio of OAG for a 1 ng/dl increase in 25(OH)D (Model 1, OR = 0·97, P = 0·02). This result indicated that the risk of OAG was associated with overall decreases in serum 25(OH)D level, although J-shaped patterns were observed in the above analyses using quintiles of 25(OH)D. To explore the overall association between serum 25(OH)D level and OAG, we used generalized additive models with cubic spline regression (Fig. 3). The smoothed curve generated from the cubic spline model, which was adjusted for variables in the fully adjusted model (Model 3), showed a decrease in odds ratio of OAG as serum 25(OH)D levels rose in the overall pattern. However, when we excluded the sparse areas with 25(OH)D values below the 5th (≤9·97 ng/dl) and above the 95th (≥30·73 ng/dl) percentiles, we found a reverse J-shaped pattern that was consistent with the quintile analyses. Consistently, there was an obvious J-shaped trend in the male group, but not in the female group.
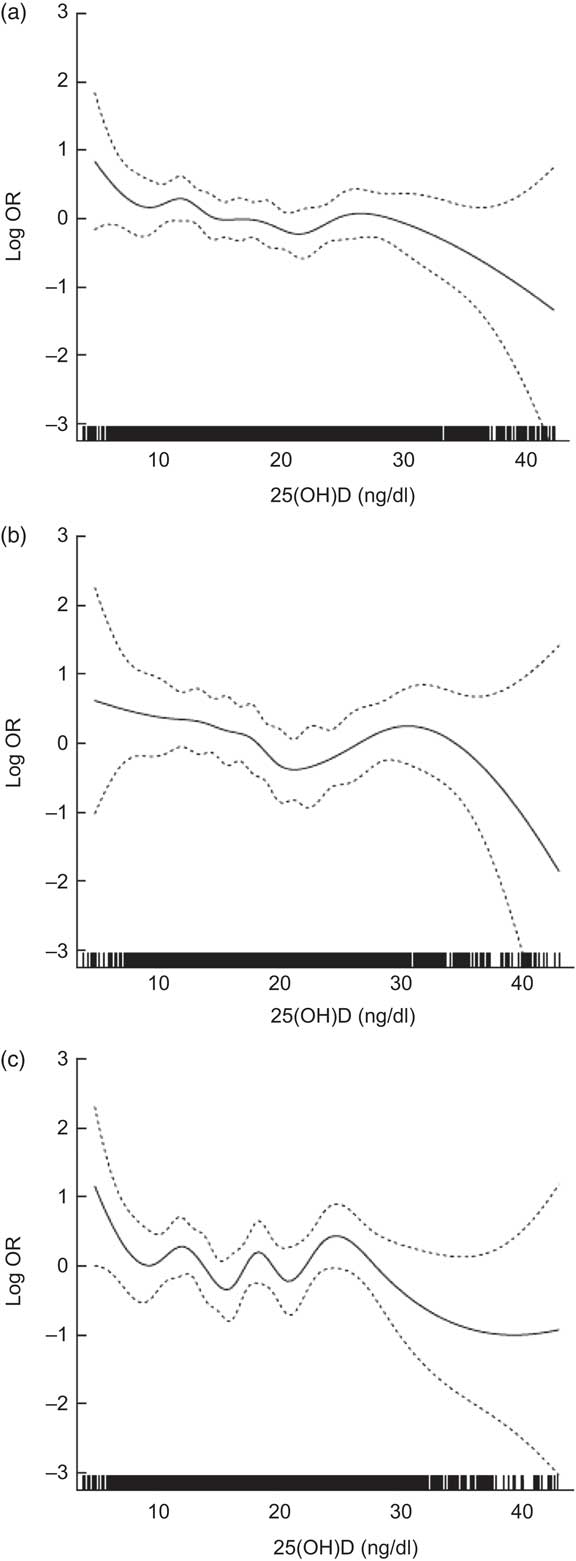
Fig. 3 Adjusted log odds ratios (–––) with 95 % confidence intervals (- - - - -) for risk of open-angle glaucoma by serum 25-hydroxyvitamin D (25(OH)D), using generalized additive models with cubic spline regression, among (a) the total, (b) the male and (c) the female participants, Fifth Korean National Health and Nutrition Examination Survey (KNHANES V), 2010–2011. The model was adjusted for sex, age, current smoking status, sun exposure, family history of glaucoma, migraine, cold hands, systolic blood pressure, fasting glucose, total cholesterol, TAG, visual acuity and intraocular pressure
However, the outcome of glaucoma suspect or OAG showed a weaker association with serum 25(OH)D level than OAG (Table 2). The odds ratios of glaucoma suspect or OAG had a marginally significant linear trend across quintiles of 25(OH)D (Model 1, P for linear trend = 0·06 and P for quadratic trend = 0·12). The analyses using continuous serum 25(OH)D level also showed a weak linear association with marginal significance (Model 1, P = 0·04).
In addition, we examined the interaction between serum 25(OH)D and predictive factors of OAG. The adjusted geometric means of IOP and vertical and horizontal cup-to-disc ratios of the optic nerve head are shown in Table 3. The trends of the predictive factors were linear rather than quadratic across the quintiles of 25(OH)D. The multivariable linear regression models measured the associations of serum 25(OH)D level with these factors. Serum 25(OH)D levels were inversely and consistently related with vertical (P = 0·03) and horizontal (P = 0·01) cup-to-disc ratios even after full adjustment. This finding suggests that the structural change of the optic nerve, an important factor for detection of glaucoma, may be affected by 25(OH)D levels. We also observed a significant inverse relationship between IOP and serum 25(OH)D levels (P < 0·001).
Table 3 Adjusted geometric means of predictive factors of open-angle glaucoma across quintiles of serum 25-hydroxyvitamin D among 6094 adult participants in the Fifth Korean National Health and Nutrition Examination Survey (KNHANES V), 2010–2011
25(OH)D, 25-hydroxyvitamin D; IOP, intraocular pressure.
†Model 1 was adjusted for sex, age, current smoking status, sun exposure, family history of glaucoma, migraine and cold hands.
‡Model 2 was adjusted for variables in Model 1 plus systolic blood pressure, fasting glucose, total cholesterol and TAG.
§Model 3 was adjusted for variables in Model 2 plus visual acuity and IOP.
Discussion
To our knowledge, the present study is the first to demonstrate an association between vitamin D status and risk of OAG in a human population sample. The nature of this relationship was a J-shaped increase of OAG at lower vitamin D status. In the study population, taken from KNHANES V, the cross-sectional findings indicate that the lowest quintile of serum 25(OH)D level had a significantly increased odds ratio of OAG, but not glaucoma suspect or OAG, suggesting that vitamin D deficiency may be significantly linked to clinical optic nerve dysfunction of OAG patients, rather than simply structural glaucomatous change of glaucoma suspects. Unexpectedly, there was an insignificantly increased risk of OAG in the highest quintile of serum 25(OH) level, and it contributed to a statistically significant quadratic association. In addition, we found that IOP, vertical and horizontal cup-to-disc ratios had a significant relationship to serum 25(OH)D level. These results support the study's hypothesis that low vitamin D status is associated with an increased risk of OAG. Since the analyses were adjusted for a wide range of confounders including visual acuity, sun exposure and metabolic factors, vitamin D deficiency should be considered as an independent risk factor for OAG. Low vitamin D status might render additional hazardous effect on the optic nerve because patients with OAG already have impaired vision that might reduce daily activities and deteriorate vitamin D status. Therefore, it is possible to describe that patients with OAG might be in a vicious cycle of visual impairment and low vitamin D status (Fig. 4).
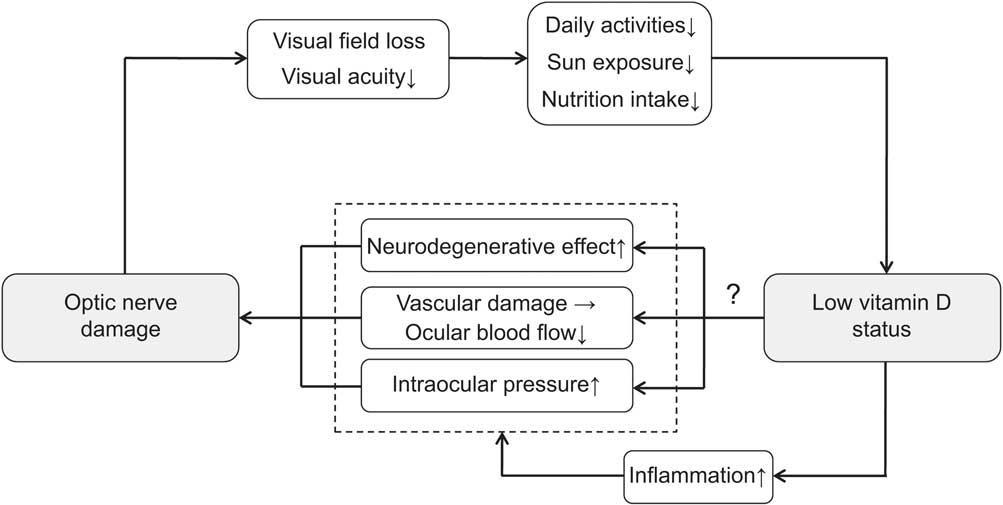
Fig. 4 Diagram for the possible relationship between optic nerve damage and reduced vitamin D status
The association between vitamin D status and OAG is not fully understood. Previous studies have mostly focused on the relationship between vitamin D and IOP( Reference Krefting, Jorde and Christoffersen 26 ). Although some animal studies suggest that vitamin D may be associated with IOP, the results of human studies have been equivocal( Reference Kutuzova, Gabelt and Kiland 27 ). In a randomized controlled trial, there was no reduction in IOP in human subjects with high-dose vitamin D supplement( Reference Krefting, Jorde and Christoffersen 26 ). However, this result might be limited by the small sample size consisting of only eighty-seven healthy participants and a 6-month short-term follow-up. Our findings showed that IOP was associated with serum 25(OH)D level in a population-based approach including participants with OAG and glaucoma suspect, as well as healthy controls. Therefore, further work is required to confirm whether vitamin D status affects the development of OAG through IOP. In addition, a previous epidemiological study reported that the risk of OAG due to exfoliation syndrome increased in northern-latitude populations, suggesting reduced vitamin D metabolism could be one of mechanisms explaining the link between latitude and exfoliation syndrome( Reference Wiggs 28 ). However, these data are insufficient to support our findings because the prevalence of exfoliation syndrome is very low in Asian countries including South Korea( Reference Chen, Chen and Zhang 29 ).
Recently, OAG is seen as a complex and multifactorial disease that may be influenced by not only IOP, but also the systemic conditions. Since effects of low serum 25(OH)D level on the risk of OAG seem to be significant in the adjusted models, vitamin D may have an IOP-independent protective effect on OAG. The potential mechanisms underlying this association are still not fully understood, but may be mediated by the several protective roles of vitamin D, either directly (by activation of the vitamin D receptor) or indirectly (by regulation of calcium homeostasis)( Reference Yang, Ma and Zhang 30 , Reference DeLuca, Kimball and Kolasinski 31 ). First, vitamin D may affect immunomodulation in the pathogenesis of OAG( Reference McKinnon 3 ). Recent researches have shown that imbalance of the immune system is a major contributor to neurodegenerative injuries on the optic nerve axons and ganglion cell bodies. Since it has been well established that vitamin D has marked effects on regulating immune cell functions, this effect may play a key role in the protection of the optic nerve. Second, vitamin D also regulates important neurotrophic factors in the central nervous system and the plasticity process in neural networks. The researches using animal models have found that vitamin D has the neurotrophic property associated with the synthesis of neurotrophic growth factors and neurotransmitter metabolism( Reference Balion, Griffith and Strifler 9 , Reference Van der Schaft, Koek and Dijkstra 10 ). It is possible that this effect may help in the regeneration of the optic nerve after injury. Third, vitamin D regulates oxidative stress on neurons by activation of calcium channels( Reference DeLuca, Kimball and Kolasinski 31 ). A previous study suggests that the oxidative stress-induced amyloid β-peptide deposition could involve the optic nerve in OAG( Reference McKinnon 6 ). In support of this view, evidence accumulating over two decades has shown that vitamin D is closely associated with a number of neurodegenerative or psychiatric diseases such as Alzheimer's disease, Parkinson's disease, depression and schizophrenia( Reference DeLuca, Kimball and Kolasinski 31 ). Several researches have shown that these diseases could affect the development of OAG; therefore, we have expected that OAG shares the biological mechanisms of vitamin D.
Another possible explanation for the association of lower vitamin D status with OAG may lie in the mechanism of impaired ocular blood flow. Several studies have shown the influence of vitamin D on peripheral or micro-vessel circulation( Reference Yang, Ma and Zhang 30 ). These studies have revealed that vitamin D regulates the rennin–angiotensin system and improves endothelial cell-dependent vessel vasodilatation. In one animal-based study, it is discussed that suppression of the rennin–angiotensin system can decrease the risk of OAG by improving ocular blood flow( Reference Shah, Sharma and Mehta 32 ). An anti-inflammatory effect of vitamin D also inhibits endothelial dysfunction from metabolic damage or oxidative stress( Reference Yang, Ma and Zhang 30 ). Furthermore, vitamin D status might reflect chronic non-specific illness that could affect systemic circulation( Reference Pittas, Chung and Trikalinos 33 ). These researches have shown that improving vitamin D status may have a beneficial effect on the vascular dysregulation leading to local vasospasm( Reference Flammer and Orgül 5 , Reference Pittas, Chung and Trikalinos 33 ).
Despite expectations that a linear trend would appear, we actually found a reverse J-shaped relationship between serum 25(OH)D level and OAG. It is feasible that the relationship identified in the present study could reflect exposure to UV light, because there is a theoretical basis for assuming that long-term exposure to UV not only increases vitamin D synthesis but also directly induces oxidative damage to the anterior chamber of the eye, finally leading to OAG( Reference Izzotti, Saccà and Longobardi 34 ). Therefore, it is possible that highly elevated vitamin D levels could be associated with OAG due to excessive exposure to UV. Another possible explanation is that there may be a subgroup of the population who is genetically resistant to vitamin D( Reference McGrath, Eyles and Pedersen 35 ). These individuals could have relatively elevated levels of serum 25(OH)D, but may be accompanied by relative vitamin D deficiency.
We also observed the unexpected finding that there was no obvious trend between vitamin D and OAG in females. The disturbed trend among females is most likely explained by menstrual status or hormone replacement therapy. In general, females have an independent risk factor for OAG due to lower levels of oestrogen and progesterone after menopause, while males may not( Reference Pasquale, Loomis and Weinreb 36 ). Furthermore, recent works have revealed that sexual hormonal status could lead to nutrition deficiency and various chronic diseases, which may be linked to low vitamin D status and development of OAG( Reference Lim, Kung and Sompongse 37 , Reference Battaglia, Mancini and Regnani 38 ).
The strength of present study is that it is based on a large population sample size so it minimizes selection bias. An additional strength is the characterization of demographic, biochemical and ophthalmologic covariates to reveal an independent association between serum 25(OH)D level and OAG. The study has several limitations. First, the findings reported herein are cross-sectional and observational. Although OAG is usually considered irreversible and the study population is nationwide and randomly sampled, the study's cross-sectional nature precludes the determination of a direct association between vitamin D and OAG. We expect that a longitudinal and interventional study design will draw a definitive conclusion about the association between vitamin D status and OAG. Second, the ISGEO criteria for OAG diagnosis did not consider the progression of disease and comprehensive ophthalmologic examination. Although use of the ISGEO criteria is a preferred method in a cross-sectional epidemiological study, clinical diagnosis of OAG may not perfectly match the ISGEO criteria( Reference Foster, Buhrmann and Quigley 19 , Reference Chon, Qiu and Lin 20 ). Third, this is an Asia-specific study performed at the level of a single country. Generally, the incidence and progression of glaucoma are influenced by ethnic differences and genetic backgrounds. Thus, it is uncertain whether the results will be equally applicable to other demographic groups.
Conclusion
There was a reverse J-shaped association between vitamin D status and the risk of OAG, with significantly elevated risk at lower vitamin D levels. This epidemiological finding, which is not previously reported, suggests that vitamin D deficiency should be considered as a potential risk factor for the development of OAG. In order to confirm the protective effect on OAG, larger, more comprehensive studies of vitamin D supplementation are needed.
Acknowledgements
Sources of funding: The authors have no support or funding to report. Conflicts of interest: The authors declare that they have no conflict of interest. Ethical approval: The study protocol was approved by the institutional review board at the Korea Centers for Disease Control and Prevention (IRB No: 2010-02CON-21-C, 2011-02CON-06-C). Authors’ contributions: T.K.Y. performed the statistical analysis and drafted the manuscript. E.O. collected the data and analysed the experimental results. S.H. collected the data and provided feedback on the paper. T.K.Y. and E.O. contributed equally to this work.







