


Meal preparation at home is associated with diet quality among adolescents and adults, where higher frequency of preparing meals at home is associated with higher fruit, vegetable and micronutrient intakes, and with lower fat, fried food and sugar-sweetened beverage intakes(Reference Larson, Perry and Story1–Reference McLaughlin, Tarasuk and Kreiger3). As the prevalence of childhood obesity continues to rise, increased understanding of the complex relationship between food preparation behaviours and diet quality is needed. Involvement in food-related tasks could likely increase a child's perception of his/her ability to perform these behaviours(Reference Larson, Story and Eisenberg2, Reference Bandura4, Reference Hill, Casswell and Maskill5), and greater participation in preparing home meals could foster increased self-efficacy for the selection of healthier food options. Furthermore, performing food-related activities can be an important opportunity to encourage children to try and to enjoy a variety of foods. Children and adolescents involved in such activities were generally more interested in nutrition and vegetables(Reference Hill, Casswell and Maskill5) and consumed healthier diets(Reference Cabalda, Rayco-Solon and Solon6). Research on the impact of school garden programmes has shown that a hands-on approach of exposing children to a variety of fruits and vegetables is a viable strategy to encourage children to develop increased food preference and subsequently increased intake(Reference Morgan, Warren and Lubans7–Reference Somerset and Markwell9). It is possible that similar findings could be transferred to interventions teaching meal preparation skills.
Currently, the majority of reported studies describing this relationship have been conducted among adolescents and adults. Therefore, the purpose of the present analysis was to examine the association between frequency of home meal preparation and (i) fruit and vegetable preference and (ii) self-efficacy for selecting healthy foods, two factors that have been previously described to influence diet quality, in a younger population such as elementary-school children. The analysis was conducted using data collected as part of the Raising healthy Eating Active Living kids in Alberta (REAL Kids Alberta) project, a survey administered among a provincially representative population of grade 5 children in Alberta, Canada.
Experimental methods
Participants and recruitment
All elementary schools with grade 5 students in Alberta, with the exception of francophone (2 % of all schools), charter (1 %), private (7 %) and on-reserve federal schools (2 %), were included in the sampling frame. Schools were selected using a one-stage stratified random sampling design. Schools were stratified according to metropolitan (cities of Edmonton and Calgary), city (municipalities with population ≥40 000) or rural-town (municipalities with population <40 000) regions, and then randomly selected within each stratum to ensure proportional representation. Of 164 invited schools, 151 (92 %) schools agreed to participate. Schools that participated in the survey were provided with a report of the findings. In the spring of 2010, 5597 home surveys and parent consent forms were sent home, of which 3687 (66 %) were returned and 3656 (65 %) parents provided parental consent for their child to participate in the survey. Trained evaluation assistants recruited through posted job advertisements visited each school to administer student surveys. After excluding children who were absent during data collection and those who did not complete the survey, a total of 3398 (61 %) completed surveys were collected. The Health Research Ethics Board of the University of Alberta approved all study procedures.
Measures of interest
Frequency of home meal preparation
Children were asked to indicate the frequency with which they helped prepare or cook food in the home, selecting from five response options ranging from ‘never or almost never’ to ‘several times a day on most days’.
Fruit and vegetable preference
Preferences for three fruits (apples, oranges, blueberries) and nine vegetables (carrots, tomatoes, green beans, broccoli, spinach, zucchini, cabbage, squash, green peas) were rated using a 3-point scale with facial descriptors. Response options included ‘like a lot’, ‘like a bit’, ‘don't like’ and ‘don't know’. Children were instructed by evaluation assistants to select the ‘don't know’ response if they had never tried the fruit or vegetable. A fruit or vegetable preference score was calculated for each child individually. Each of the response options was assigned a score ranging from 1 to 3, with a higher score indicating a higher preference rating. Scores were totalled for fruits (range 3 to 9) and vegetables (range 9 to 27) separately and standardized to a scale of 10 to allow for comparability of results between the two food groups. All ‘don't know’ responses were excluded from the analysis.
Self-efficacy
Self-efficacy was assessed using a 4-point scale consisting of six questions, where children were asked if they were confident they could (i) eat healthy food at school, (ii) eat a healthy snack between school and dinner, (iii) eat healthy food or choose a healthy snack when with friends, (iv) eat healthy food when eating dinner with the family, (v) choose a healthy snack when alone at home and (vi) choose a healthy snack when bored or sad. Response options ranged from ‘very confident’ to ‘not at all confident’. An aggregate measure of self-efficacy was calculated based on methods previously described(Reference Spence, Blanchard and Clark10), where a score (range 1 to 4) was assigned to each response option, with a higher score indicating higher self-efficacy. Scores were then totalled across all six questions to obtain an overall self-efficacy score (range 6 to 24). Internal consistency of the scale items was high (Cronbach's α = 0·85), and a factor analysis with varimax rotation of the six items extracted one factor with loadings ≥0·70. This factor accounted for 57 % of the variance in the items. As such, the use of an aggregate measure of self-efficacy based on responses to these six questions is appropriate.
Other measures
Demographic information such as annual household income and parental education attainment was obtained from parent responses in the home survey. All survey instruments used in the present study can be found on the REAL Kids Alberta project website (www.realkidsalberta.ca).
Data analysis
All analyses were conducted with the STATA statistical software package version 11 (StataCorp, College Station, TX, USA). All analyses were weighted to represent provincial estimates of the grade 5 student population in Alberta. Random-effects regression models with children nested within schools were used to test for associations between fruit and vegetable preference, self-efficacy and frequency of helping with preparing home meals. Frequency of home meal preparation was included in the analyses as a categorical variable. Analyses were adjusted for the confounding effects of gender, household income, parent education attainment and urban, city or rural residency.
Results
Approximately half (51 %) of the surveyed children were girls, and all levels of household incomes and parental education attainment were well represented (Table 1). Approximately 30 % of children reported helping with home meal preparation at least once daily, while 12·4 % reported never helping. In general, the study children preferred fruits to vegetables (mean fruit preference score = 8·91, range 3·33 to 10; mean vegetable preference score = 6·64, range 3·33 to 10; Table 1). Fruit and vegetable preference increased with increasing frequency of helping cook food at home (Table 2). This association appeared to be more pronounced in vegetable preference compared with fruits, where helping with home meal preparations several times daily led to approximately a 10 % (or 1 point) increase in vegetable preference. On average, children had moderately high self-efficacy in selection of healthy foods (self-efficacy score = 18·54, range 6 to 24; Table 1). Self-efficacy increased with increasing frequency of helping with home meal preparation (Table 2).
Table 1 Characteristics of surveyed grade 5 children in Alberta, Canada (n 3398)Footnote *Footnote †
* Numbers presented are % unless otherwise stated.
† Results were weighted to represent provincial estimates of the grade 5 student population in Alberta.
‡ Score standardized to a 10-point scale, higher score indicates higher preference. Children were instructed to select ‘don't know’ response if they had not tried the fruit or vegetable, all ‘don't know’ responses were excluded from calculation of preference scores.
§ Score range 6 to 24, higher score indicates higher self-efficacy.
Table 2 Associations between helping with food preparation in the home and fruit and vegetable preference and self-efficacy among grade 5 children in Alberta, Canada (n 3398)
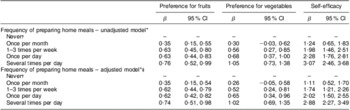
*Random-effects regression models with children nested within schools were used to test for associations.
†Reference level.
‡Analyses were adjusted for gender, annual household income, parental education attainment and geographic residency. Results were weighted to represent provincial estimates of the grade 5 student population in Alberta.
Discussion
The present study shows that involvement in home meal preparation is associated with higher self-efficacy for making healthier food choices among grade 5 children. Researchers have previously proposed that involving children in household tasks possibly builds skills and self-efficacy(Reference Rossman11). Adolescents who had higher self-efficacy tended to make healthier eating choices(Reference Gracey, Stanley and Burke12) and ate more fruits and vegetables(Reference Neumark-Sztainer, Wall and Perry13, Reference Zabinski, Daly and Norman14). Therefore, children who are involved in meal preparation activities could have increased confidence in their ability to select and consume healthier foods.
Frequency of participation in home meal preparation was also associated with higher preference for fruits and vegetables in the present study. Food selection can be influenced by a variety of factors, of which food preference is most often shown to be associated with food intake(Reference Glanz, Basil and Maibach15–Reference Rollins, Loken and Birch17). Children and adolescents who ate meals more frequently with their families tended to have healthier dietary patterns(Reference Gillman, Rifas-Shiman and Frazier18, Reference Larson, Neumark-Sztainer and Hannan19). Meal preparation, like family mealtimes, could provide the opportunity for family interaction where eating patterns and food preferences are modelled and developed. Currently, children do not consume the recommended amounts of fruits and vegetables(Reference Krebs-Smith, Guenther and Subar20, Reference Storey, Forbes and Fraser21). As such, strategies to increase fruit and vegetable preference, and subsequently intake, should be explored. Nutrition education and programmes encouraging children to participate in meal preparation activities could be a viable approach.
Fruit and vegetable preference and self-efficacy could be potential mediators in the complex relationship between involvement in meal preparation and the consumption of a healthier diet. Both of these factors were previously shown to be linked to higher diet quality in children and adolescents(Reference Gracey, Stanley and Burke12–Reference Zabinski, Daly and Norman14, Reference Rasmussen, Krolner and Klepp16, Reference Rollins, Loken and Birch17) and were observed in the present study to be associated with a higher frequency of involvement in home meal preparation. The mechanism behind the association of participation in food-related activities and dietary outcomes is currently not well described. For instance, increased involvement in home meal preparation may lead to increased appreciation for fruits and vegetables, and subsequently to increased intake. Higher involvement in home meal preparation may also lead to increased self-efficacy for selecting healthier foods. Conversely, it is also possible that children with higher fruit and vegetable preference and self-efficacy are also healthier eaters who would be more interested in food-related activities such as meal preparation. As temporal causality cannot be inferred from cross-sectional surveys, an intervention study design such as evaluation of a school-based programme will be appropriate to investigate the directionality of this association.
The present study was conducted among a large provincially representative sample and its response rate can be considered high for school-based research. Limitations of the study include the use of self-reported information. It should also be taken into account when interpreting the results of the present analysis that the survey questions do not indicate if children were preparing home meals from scratch or if they were using ready-made foods. The use of convenience foods is increasingly common with the current demand for foods that require a minimum of time and effort to prepare(Reference Alexy, Sichert-Hellert and Rode22). As use of convenience foods was negatively associated with diet quality(Reference Alexy, Libuda and Mersmann23, Reference Pryer and Rogers24), this is a point that warrants further clarification in future studies. Furthermore, involvement in home meal preparation could be indicative of the frequency of eating meals at home, where children with higher involvement are from families where more meals are prepared and consumed at home. As eating meals at home has been associated with healthier diets(Reference Bowman, Gortmaker and Ebbeling25–Reference Veugelers, Fitzgerald and Johnston28), it is thus possible that these children are likely to have better diet behaviours than their peers.
Conclusions
A higher degree of involvement in food-related activity may be instrumental in the development and maintenance of healthy eating behaviours in children. Encouraging the development of food preparation skills could be a viable approach in health promotion programmes, where a hands-on approach can be seen as a way to enhance the effectiveness of nutrition education. Teaching children how to prepare simple, cost-effective and healthful meals can help in the development of a life skill that could be maintained through adulthood.
Acknowledgements
This research was funded through a contract with Alberta Health and Wellness and through a Canada Research Chair in Population Health and an Alberta Heritage Foundation for Medical Research Health Scholarship to P.J.V. All interpretations and opinions in the present study are those of the authors. The authors declare no conflict of interest. All authors participated in the planning of the analysis and writing of the present article; analysis was done by Y.L.C. The authors would like to thank all students, parents and schools for participating in the study. They would also like to thank all evaluation assistants and health promotion coordinators for the collection and processing of data, and Megan Purcell and Connie Lu for leading the data collection, management and validation.




