


Fruit and vegetable intake has been shown to prevent the onset of a number of chronic diseases, such as CVD( Reference Hartley, Igbinedion and Holmes 1 , Reference Ness and Powles 2 ), diabetes( Reference Bazzano 3 ) and cancer( Reference Riboli and Norat 4 ), as well as other CVD risk factors( Reference Hartley, Igbinedion and Holmes 1 , Reference Rees, Dyakova and Wilson 5 ). The promotion of fruit consumption has been widely used in research interventions( Reference Pomerleau, Lock and Knai 6 ) and government-initiated school-based programmes( Reference Bere, Hilsen and Klepp 7 ) as part of a balanced healthy diet and to prevent the onset of these diseases.
The WHO recommends the consumption of 400 g of fruit and vegetables each day( 8 ). This advice has been translated into ‘5 servings per day, 7 days a week’ campaigns in many countries, which has been shown to be a better measure of intake than portion size( Reference Ashfield-Watt, Welch and Day 9 ). However, limited individual-level data exist about consumption of fruits and vegetables in Latin America.
One study of Andean adults in Peru showed that 34·5 % had low fruit intake and 33·3 % had low vegetable intake( Reference Medina-Lezama, Morey-Vargas and Zea-Diaz 10 ), where low intake was defined as consumption of fruits or fresh vegetables on less than 3 d/week. A study in Brazil noted that less than half of the participants reported adequate fruit and vegetable intake (<5 servings/d), with male gender, youth and lower educational attainment predicting inadequate intake( Reference Figueiredo, Jaime and Monteiro 11 ). Outside Latin America, various individual and environmental factors have been shown to contribute to low fruit and vegetable intake, including low socio-economic status( Reference Darmon and Drewnowski 12 ), environmental factors such as increased cost and low availability( Reference Pollard, Kirk and Cade 13 ), taste( Reference Buscher, Martin and Crocker 14 , Reference Shannon, Story and Fulkerson 15 ), improved marketing strategies of unhealthy foods, the surge of the rapid increase in fast-food culture( 8 , Reference Powell, Han and Chaloupka 16 ), and demographic factors such as younger age and male sex( Reference Figueiredo, Jaime and Monteiro 11 ).
Interventions that aim to modify healthy food intake through change in the purchasing environment, specifically those related to accessibility, provision of nutritional information at the point of purchase and price reductions, have been effective in increasing healthy food consumption( Reference Glanz and Hoelscher 17 – Reference Foster, Karpyn and Wojtanowski 19 ). Strong evidence exists for the effectiveness of certain tools based on the use of the marketing mix( 20 ), also known as the 4 P’s: product, promotion, placement and price( Reference Glanz, Bader and Iyer 21 ). This approach promotes healthy lifestyle habits through health information( Reference Mozaffarian, Afshin and Benowitz 22 , Reference Michels, Bloom and Riccardi 23 ), increased availability of healthy foods( Reference Van Kleef, Otten and van Trijp 18 , 24 , Reference Farnon 25 ) and promotions that lower the price of healthy foods( Reference French 26 – Reference Horgen and Brownell 28 ).
The promotion of foods, through adequately and strategically placed nutritional information in posters, brochures, etc., reminds the consumer of the health benefits of fruit. A statement from the American Heart Association on population approaches to improve diet recommends the use of subsidy strategies to lower prices of healthy foods as an effective intervention with strong supportive evidence( Reference Mozaffarian, Afshin and Benowitz 22 ). However, there is a scarcity of studies on interventions that change environmental and pricing factors despite the success of point-of-purchase information having been widely documented( Reference Glanz and Hoelscher 17 ). In the USA, a recent cluster randomized controlled trial of in-store marketing strategies to promote sales of healthier items in low-income, high-minority neighbourhoods showed that straightforward placement strategies can significantly enhance the sales of healthier items in several food and beverage categories, specifically milk, water and some types of frozen meals( Reference Foster, Karpyn and Wojtanowski 19 ).
The aim of the present study was to determine the effect of improving visibility, providing health information and lowering the price of fruit on fruit purchasing in a university cafeteria in Lima, Peru. We also explored the perceptions of the cafeteria’s clients about the changes in marketing strategy and their fruit purchasing preferences through focused interviews.
Experimental methods
Design
The present study was a quasi-experimental pilot study, in which individuals were exposed to three different consecutive fruit marketing strategies. This was an uncontrolled trial introduced into the cafeteria’s daily practice without randomization at the individual level. The factors that were under the control of the investigators were the marketing strategy of fruit, including fruit position in the cafeteria, information available about the health benefits of fruit and the price of the fruit.
Experimental phases
There were three phases of this stepped intervention. Each 3-week phase was separated by a 2-week break due to holidays and other events that could affect the usual number of clients and items sold each day (Table 1). The first phase served as the baseline control phase, in which whole fresh fruit was presented in a display case at a site distant from the point of purchase (>3 m from the register) in its usual position (Fig. 1). The second phase consisted of repositioning the fruit into a covered container clearly displayed next to the point of purchase (Figs 2 and 3(a)). The cover of the container had a sign stating ‘Consuming five fruits and vegetables per day prevents many illnesses – World Health Organization’ in the local language (Spanish) that also included the price per item of fruit. Two posters (A4 size) with this message and price were also placed at the entrance of the cafeteria and on the wall next to the point of purchase. The third and final phase maintained the intervention introduced in Phase 2 but lowered the price by 33 % per item of fruit, from local price PEN 1·50 ($US 0·57) to PEN 1·00 ($US 0·38; Figs 2 and 3(b)). The research team covered the costs of buying fresh fruit during the study so that the cafeteria manager was not financially affected by the changes in price.

Fig. 1 (colour online) Fruit location in Phase 1

Fig. 2 (colour online) Fruit location near the point of purchase in Phase 2 and Phase 3
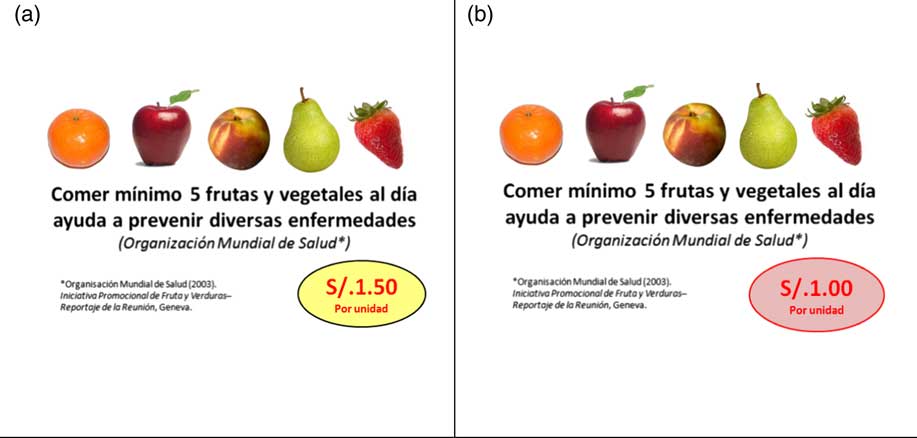
Fig. 3 (colour online) Message in the covered container and on posters in (a) Phase 2 and (b) Phase 3
Table 1 The design of the quasi-experimental study with one baseline and two intervention phases
Population and setting
The study was conducted in a university cafeteria that caters to approximately 200 students each day, the majority of whom were young adults who had graduated from high school and were enrolled full time at the university. In addition, there were approximately eighty administrative staff and faculty members, hereafter referred to as ‘non-student adults’. These data were provided by the university campus administration.
Procedures and data collection
Data collected by the salesperson through daily logs were: (i) the number of pieces of fruit sold each day; (ii) the number of full meals sold; and (iii) visible information about each fruit consumer such as the purchaser’s sex and age group (students v. non-student adults).
To avoid major variations in the flux of customers across phases, the daily hours in which fruit was sold in the cafeteria were strictly controlled. Coordination with the cafeteria manager and staff during all phases of the experiment focused on the following issues: (i) not revealing to customers that fruit consumption was being recorded for a study; (ii) complying with the hours of fruit sales; (iii) the location of the fruit; (iv) logistical issues including fruit purchase, quality assurance and freshness; (v) recording of data; and (vi) weekly data transfer to the research team. Fruit provided to the cafeteria was of optimal appearance and quality.
There was no enrolment in the study, but the cafeteria manager estimated that there were approximately 150 customers per day during the entire study, all of whom were exposed to changes in marketing strategies in Phases 2 and 3.
Qualitative interviews
After the end of Phase 3, twelve semi-structured interviews were conducted with students who use the cafeteria. Two investigators asked them to participate in the study after the end of classes. The sample of invited students was purposely chosen to include six males and six females, one-third of whom must have purchased fruit in the cafeteria at least once during the 9 weeks of the study. The main aim of the interviews was to obtain qualitative data regarding perceptions of the marketing strategies of fruit. Information requested included demographic questions, whether or not the student purchased fruit in the cafeteria and why, whether or not the student knew that fruit was available for sale, as well as if the student noticed the reduction in fruit price. We also explored the main reasons for not purchasing fruit. The interviews lasted approximately 20 min and were conducted by two researchers after informed consent was obtained. Potential students who refused to participate or were under 18 years of age were excluded from this qualitative phase but not from the open experiment.
Analysis
The primary outcome variables in the study were: (i) daily pieces of whole fruit purchased; (ii) daily number of full meals sold, hereafter referred to as ‘meals’, a proxy measure of the daily number of cafeteria users; and (iii) the fruit ratio, defined as the ratio between the total pieces of fruit purchased and the total number of meals sold in the same day. There were 14–15 d of observation for each phase.
Analysis of the primary outcome variables was done using the non-parametric Kruskal–Wallis test for comparing pieces of fruit sold and fruit ratio across the three phases. Pre-defined subgroup analyses were conducted by age and sex groups. A P value of <0·05 was considered statistically significant. We used the statistical software package STATA 12·0 for Windows for all statistical analyses. The qualitative interviews were reviewed by three different investigators and codification was developed according to the major themes identified, such as awareness of the marketing strategies and reasons for not purchasing fruit.
Results
Figure 4 shows daily customer counts (total meals sold) and pieces of whole fruit sold during the 12-week study period, which included a total of 44 d of study and 21 d of break.
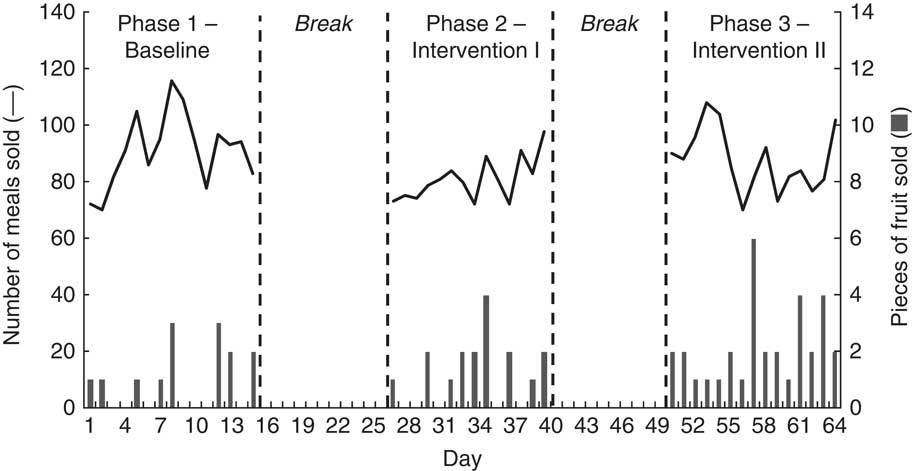
Fig. 4 Total number of meals sold daily (——) and total pieces of whole fruit sold daily (![]() ) over time during the three-phase stepped intervention on fruit purchasing in a university cafeteria, Lima, Peru
) over time during the three-phase stepped intervention on fruit purchasing in a university cafeteria, Lima, Peru
The average number of meals sold was largely stable over the study period (Table 2) with a total of 91 (sd 12·98), 80 (sd 7·75) and 87 (sd 11·18) meals sold daily in each phase, respectively. Only the total number of meals sold in Phase 1 was significantly higher than in Phase 2 (P<0·05). The minimum and maximum number of daily meals ranged from 70 to 116.
Table 2 Descriptive statistics of outcome variables in the three-phase stepped intervention on fruit purchasing in a university cafeteria, Lima, Peru
Over the duration of the three-phase study, sixty-four pieces of fruit (daily mean 1·45 (sd 1·34)) were sold. A total of fourteen pieces of fruit (daily mean 0·93 (sd 1·10)) were sold in Phase 1, seventeen pieces of fruit (daily mean 1·21 (sd 1·19)) in Phase 2 and thirty-three pieces of fruit (daily mean 2·20 (sd 1·42)) in Phase 3 (see Table 2 and Fig. 4). Fruit purchasing doubled from Phase 1 to Phase 3 (P<0·01), but there was no evidence of a difference in total fruit sold between the other phases (Table 3). When adjusting for the total number of meals sold each day, the increased fruit sold remained significant between Phases 1 and 3 (P<0·01; Table 3).
Table 3 Results of the Kruskal–Wallis tests comparing each pair of phases in the three-phase stepped intervention on fruit purchasing in a university cafeteria, Lima, Peru
Females purchased more fruit overall. Of the fruit purchased in Phase 1, 100 % was purchased by females (Fig. 5). However, by Phase 3, females only purchased 67 % of the total fruit (P<0·01) because males increased their purchase of fruit significantly after the introduction of improved visibility, health information and price reduction strategies: specifically, males purchased no fruit in Phase 1, but purchased eleven pieces of fruit in Phase 3 (P<0·01).
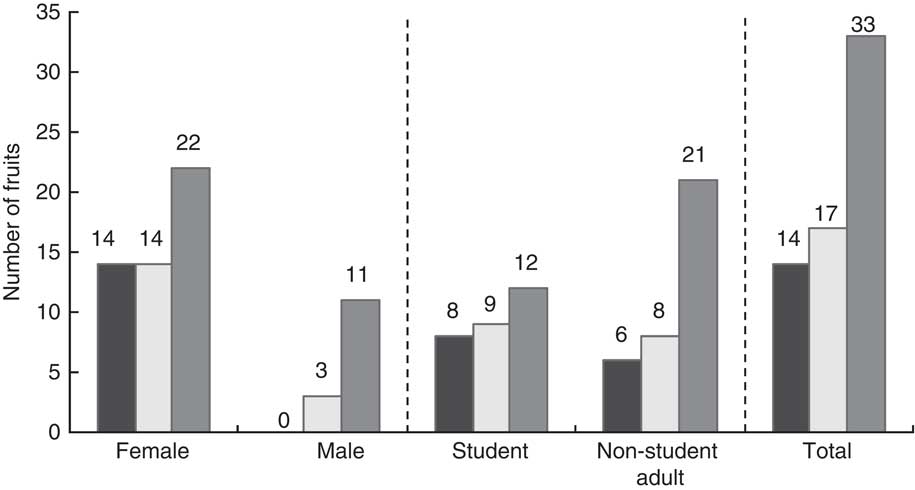
Fig. 5 Total fruit purchased overall, by sex and by age group in each experimental phase (![]() , Phase 1;
, Phase 1; ![]() , Phase 2;
, Phase 2; ![]() , Phase 3) during the three-phase stepped intervention on fruit purchasing in a university cafeteria, Lima, Peru
, Phase 3) during the three-phase stepped intervention on fruit purchasing in a university cafeteria, Lima, Peru
Non-student adults increased their fruit purchasing when exposed to each of the different experimental phases (P<0·05 for Phase 1 to 2, for Phase 2 to 3 and for Phase 1 to 3), but this increase was not observed among students. Between Phases 1 and 3, non-student adult females doubled their fruit purchasing, while non-student adult men tripled their purchasing. However, male students were the group with the lowest fruit consumption: only two male students purchased fruit during the study, both in Phase 3. Female students maintained a constant level of purchasing throughout the study (eight, nine and ten pieces of fruit in Phases 1, 2 and 3, respectively).
Of the twelve students interviewed, only one did not notice that fruit was available for sale in the cafeteria. Of the eleven students who noticed the fruit visibility experiment, nearly half noticed that the fruit price had changed in Phase 3, and two in twelve students identified price as a barrier to purchase. One of the most common reasons for not purchasing fruit in the cafeteria was a marked preference to use extra cash to buy cookies, pastry items and other unhealthy snack foods. Other reasons included preferences for unavailable fruit types, preferences regarding the way in which fruit was displayed and prepared, suspicions regarding the freshness of the fruit provided in the cafeteria, and bringing fruit from home to eat.
Discussion
Main findings
The present quasi-experimental study demonstrated that fruit purchasing increased with a simple intervention: improving visibility with fruit position near the point of purchase, adding information on health and price near the point of purchase, and reducing the price. Our results found that this combined strategy doubled fruit purchasing among cafeteria users compared with a baseline period without the intervention. In the study, females purchased more fruit overall, although men were more sensitive to the changes in marketing strategy, increasing their purchasing dramatically between each phase. Students did not respond to changes in marketing strategies, reflecting the challenges in promoting fruit purchasing among young adults.
The study also found low baseline levels of fruit sales in the cafeteria in general. This result should not be interpreted as an indication of low fruit consumption among the cafeteria users, because we did not explore their detailed patterns of fruit intake. However, in another Peruvian setting, there is evidence from a population-based survey that at least one-third of the adult population in an urban city consumed fruits on less than 3 d/week( Reference Medina-Lezama, Morey-Vargas and Zea-Diaz 10 ). In this larger context, more ambitious strategies are needed to promote fruit consumption in Peru.
Other studies in the field
There is a scarcity of studies with interventions utilizing promotional strategies that incorporate both changes in environmental factors and pricing to promote healthy food consumption in cafeterias. Being an important day-to-day environmental interaction prone to the introduction of healthy, or unhealthy, food patterns, these deserve to be studied. Two studies, one developed by Jeffery et al.( Reference Jeffery, French and Raether 29 ) in a university cafeteria and another by French( Reference French 26 ) in two high-school cafeterias, found that reducing the price of fruit by 50 % increased the purchasing of fruit between three- and fourfold. Those studies included a final phase which consisted of a return to baseline conditions, showing that fruit purchase then reverted to its original lower level. Our study was more conservative in price reduction (33 %) compared with the previous studies and the finding was also more moderate, with only a twofold increase in purchasing. Our study population was similar to that of French’s study( Reference French 26 ), given that employees and young students were the main users of the cafeterias.
The effectiveness of monetary subsidies in promoting healthy food consumption was demonstrated in a review of twenty studies from developed countries (USA, Canada, Europe, New Zealand and South Africa)( Reference Hartley, Igbinedion and Holmes 1 ). Our study suggests that monetary subsidy in the form of a discount in the price of fruit is a valid strategy in a Latin American middle-income setting. However, our study population, in a university, is in a better economic situation than the majority of the Peruvian population. Also, the intervention did not have a uniform effect on students and non-student adults, nor on men and women.
Other studies have explored the positive effect of financial incentives on healthy food purchasing, but these are not comparable to our study because they implemented the intervention using vending machines or in grocery stores and they promoted different types of healthy food items, such as low-fat snacks( Reference Hartley, Igbinedion and Holmes 1 ).
Our study explored not only the price effect, but the effect of providing a health message with better visibility of fruit near the point of purchase as well. Interventions using point-of-purchase promotion have demonstrated success as marketing strategy( Reference Buscher, Martin and Crocker 14 , Reference Glanz and Hoelscher 17 ). In contrast, the use of health messages shows inconclusive results in terms of effectiveness( Reference Horgen and Brownell 28 , Reference Anderson, Bybee and Brown 30 , Reference Epstein, Jankowiak and Nederkoorn 31 ). In the unsuccessful interventions with university students, one potential explanation is that nutrition labelling is less eye-catching and does not advertise as well the taste, cost, convenience and energy value of fruit compared with unhealthy options( Reference Buscher, Martin and Crocker 14 , Reference Horgen and Brownell 28 ).
Our results support the argument that interventions to make healthier foods more economically attractive may be more effective than nutrition or health messages alone( Reference Horgen and Brownell 28 ).
The low fruit consumption among the young adult population, and their poor response to the intervention, guided the decision to focus our qualitative study on the student group. We identified variables that were important in this subgroup, including fruit preference, fruit preparation and non-fruit snacks with less nutritional value. Awareness of the nutritional value of fruit over other sweet snacks was identified; however, the less nutritional snacks were frequently cited as a more popular choice, potentially explaining the poor response to the health promotion message of fruit. Failure of the cost reduction strategy to impact this group was harder to explain. One participant explained that the price of fruit would have to be the same as that at the local market for her to consider buying fruit at the cafeteria.
Our qualitative study identified a range of factors that contribute to the low fruit purchasing among students at the university cafeteria, as well as factors that may explain the resistance to these interventions. However, most of these students live with their parents and the easy access to fruit in the family home may help explain this difference. Further study could help determine actual fruit intake in this age group. The challenge for policy makers attempting to increase fruit intake in this group is to design an intervention that overcomes these barriers.
Limitations of the study
In the present study we were not able to differentiate the isolated effects of placement, promotion or price. Yet, this trade-off in the design was made to align our interventions to real scenarios, in which a package of progressive changes is implemented as per established marketing strategies around product, promotion, placement and price.
The study was limited in that only pre–post comparisons were conducted. Thus, results may have been influenced by temporal changes, such as a process of desensitization to fruit sales. In order to tackle this problem, we designed the study taking into account variables that may have threatened its validity. To diminish these weaknesses, we implemented the experiment during weeks with few or no days of holiday or conferences inside the university campus that may have altered the number of customers in the cafeteria. We also registered the number of meals sold each day to control for any other relevant changes that might have introduced higher volumes of meals sold in the cafeteria. Our results did not show any major fluctuations in total sales across phases.
Our study did not include a return to baseline scenario after the experimental phases; therefore, we could not analyse if the positive effect of fruit purchasing was sustained over time or not. However, we know from previous studies that after price reduction is suppressed, fruit sales return to their original level( Reference French 26 , Reference Jeffery, French and Raether 29 ), confirming that the increase in fruit purchases is strongly related to the introduction of a financial incentive, and this may be true for the health message and point-of-purchase interventions, too.
Ideally, electronic records could have informed us if there was any substitution effect when fruit purchases increased, such as a reduction in overall purchasing of unhealthy foods. However, we were not able to capture this in our study as the cafeteria did not have an electronic system. The substitution effect is an important indicator that merits attention when designing future studies. Ni Mhurchu et al. ( Reference Ni Mhurchu, Vandevijvere and Waterlander 32 ) provide an example of a monitoring framework to use when designing future studies.
Finally, our study was implemented in a cafeteria of a university located in a population of middle-to-high socio-economic level with higher educational attainment. This population is not representative of the entire population of a developing country like Peru; yet the experiment conducted was worth exploring in this setting as it enabled a favourable assessment of the effects of changes in fruit’s visibility and price reduction across sex and age groups.
Strengths of the study and further research
The present study is the first one in Peru and probably one of the first in Latin America to explore how quick, low-cost, simple interventions using combined marketing tools such as promotional messages, product placement and changes in price of healthy items can make a big difference in consumer purchasing and subsequent health behaviours. According to Epstein et al.( Reference Epstein, Jankowiak and Nederkoorn 31 ), this kind of experimental research is still in an early stage. Therefore, more of these approaches are needed, especially in developing countries.
The fact that our experiment was conducted under pragmatic day-to-day circumstances, and not under laboratory conditions, provides us with an element of external validity, as Epstein et al.( Reference Epstein, Jankowiak and Nederkoorn 31 ) point out, while being aware of its limitations in generalizability. Students and staff from the university campus face a real situation in which any cafeteria customer can shop at convenience stores outside the university, and can choose from among healthy and unhealthy food items, such as snacks (chips, candy, crackers), beverages (water, soft drinks, juice), desserts, etc.
Other strengths of our study include: (i) the recording of two pieces of basic personal information, sex and a proxy of age; (ii) an affordable price of fruit (less than $US 0·50) that removed disincentives related to cost; and (iii) the use of a health message near the point of purchase based on the ‘5-a-day’ recommendation by the WHO, which has also been promoted by Glanz and Hoelscher( Reference Glanz and Hoelscher 17 ).
Multi-site studies in real-world scenarios are needed to provide more information on the external validity of the results.
Conclusion
The current pilot study suggests that promoting fruit through a combination of product placement close to the point of purchase, added health information and lower price has a large positive effect on fruit purchasing, especially among non-student adults and males in a university cafeteria. Students were more resistant to behavioural change than non-student adults to the interventions that promoted fruit purchasing.
Acknowledgements
Acknowledgements: The authors’ special appreciation and thanks go to Ana María Flores, Giuliana Vargas and Stephany Curipaco, among other members of the cafeteria’s staff, for providing valuable support with authorization, sales data registration and logistics. Francisco Diez Canseco, Antonio Bernabé and Germán Málaga contributed with relevant suggestions. Financial support: M.K.C., J.J.M. and the CRONICAS Center of Excellence in Chronic Diseases at Universidad Peruana Cayetano Heredia were funded by the National Heart, Lung, and Blood Institute (NHLBI), National Institutes of Health (NIH), US Department of Health and Human Services (contract number HHSN268200900033C). C.P.B. was supported by the NIH and Fogarty International Center through the International Clinical Research Fellows Program at Vanderbilt University (grant number R24 TW007988). The funders had no role in the design, analysis or writing of this article. Conflict of interest: None. Authorship: M.K.C., T.D.P. and J.J.M. conceived and designed the experiments; M.K.C. and T.D.P. performed the experiments; M.K.C. and C.P.B. analysed the data; M.K.C., T.D.P. and C.P.B. wrote the manuscript; all authors gave final approval of the version submitted for publication. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects/patients were approved by the Hospital Nacional Cayetano Heredia, in Lima, Peru. For the intervention, we did not seek the consent of individuals because no identifying individual data were collected (only age group and sex) and the authors felt there was negligible risk involved for the participants; furthermore, knowledge of the experiment would have been in conflict with the study design, which uses a before–after comparison instead of a control group. Verbal informed consent was obtained from all participants in the qualitative study.








