


Despite the wide range of techniques available for dietary assessment, ranging from questionnaires to weighed records to biological markers, no method is universally the ‘best’(Reference Barrett-Connor1) or ‘ideal’(Reference Beaton, Milner, McGuire, Feather and Little2). At best there may be ‘preferred’ methods for particular purposes(Reference McGee, Rohdas, Hankin, Yano and Tillotson3). For example, in epidemiological studies the diet history method is considered preferable; while for obtaining the average level of usual dietary intake the 24 h recall method is used, although it is known to underestimate(Reference Borrelli, Cole, DiBiase and Contaldo4). However, in situations where maternal intakes are to be examined in relation to birth outcomes, the level of accuracy required in estimating dietary intakes is considerably high. Additionally, such methods should be simple to administer and also should consider the convenience and comfort of the individual whose intake is to be assessed.
Conventional dietary assessment of an individual requires information on three aspects, i.e. correct recall of the foods consumed, their portion sizes and the nutrient contents of the foods. Several errors are introduced at each of these stages, resulting in large random deviations from the true mean. For example, random errors due to the use of food tables are reported to be in the range of 2 % to 20 %, whereas errors involved in estimating the weights (portion sizes) of foods eaten are reported to be between 20 % and 30 %. However, the more serious error may be the recall of exactly which foods are consumed in a day, which is known to range from 4 % to 400 %(Reference Bingham5). Thus obtaining accurate intake at individual level is a most difficult task and requires a high degree of skill, care and dedication on the part of the observer. Clearly, the need for modifications in conventional methods that will reduce these errors effectively is beyond doubt.
In rural communities like those in India, illiteracy in women prevents the use of food diaries or self-weighing methods commonly used in developed countries. Similarly, dietary habits and even food preparations are culture-specific and as such estimates of intake obtained by conventional methods are likely to be far from precise. It is therefore essential that community-specific considerations be incorporated to obtain objective estimates of individual intakes. In particular, objectivity in estimating the portion size and nutrient content of cooked foods needs to be attempted. In the present paper, we describe community-specific modifications to the conventional 24 h recall method for studying the dietary intake of rural pregnant women in relation to birth outcome. However, all dietary assessment methods rely more or less on information supplied by an individual and therefore independent validation is needed. We have therefore validated the modified method by comparing the estimates of intakes with those obtained from weighed records in an observer follow-up study.
Materials and methods
The current methodology was developed during the pre-recruitment phase of a prospective study planned in six villages, 40–50 km from Pune City, that aimed to examine the relationship of maternal dietary intake with birth outcome. Ethical approval was given by the KEM Hospital Ethics Committee, and permission was obtained from local village leaders. Forty-one pregnant women were selected from the study villages. We were not able to select them randomly as participation depended on their (and their families’) willingness to be followed closely from morning until late evening.
The socio-economic information collected initially showed high levels of illiteracy (31 %). The rural community comprised families (75 %) engaged in subsistence farming on either their own small landholding or other farms as labourers. Most rural women were busy with childcare, laborious domestic work and, in addition, farming work and did not have time for lengthy interviews by researchers, nor did they like the weighing or handling of food by an outsider. Thus a new approach was undertaken, with the following components.
Focus group discussions
Initially, we conducted focus group discussions (FGD) for understanding the community, even before developing the tool for the dietary survey. Discussions were focused on typical dietary patterns, staple foods, meal frequencies, foods eaten on festivals or on days of fasting, foods specifically eaten or avoided during pregnancy, and foods available outside the home. FGD thus provided insight into the nutritional knowledge and practices of the rural mothers, the typical local names of various food preparations and food taboos, especially during pregnancy. The valuable information obtained from FGD about such community specifics was useful for incorporating appropriate modifications into the conventional 24 h recall method. Additionally, the information was also found useful while interviewing the women for 24 h recall of daily intake (Fig. 1).
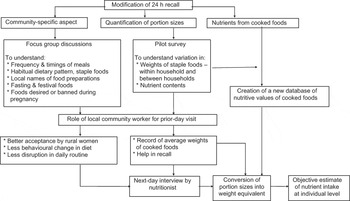
Fig. 1 Flow chart showing the various steps in modifying the conventional 24 h recall method
Pilot study
In addition to FGD, a pilot investigation was undertaken on thirty pregnant women to understand the variations in portion sizes as well as nutrient contents of staple foods consumed by mothers in the study area. We recorded the actual weights of major food items such as roties (wheat/bajra/sorghum bread), rice and dhal/vegetables in each house. It was observed that women were remarkably consistent in making roties of similar size, as the weight of roties within a household varied negligibly (CV = 3 %). However, there was a large between-household variation (CV = 22 %) in the weight of roties. Furthermore, in the case of cooked items like rice (CV = 28·5 %), dhal (CV = 33·6 %) and vegetables (CV = 39·9 %), the variation was even larger. Unlike roties, within-household variations in preparations of vegetables (dry or with gravy) also existed and, as such, an average weight (of three servings) for each food item was necessary for each household. Therefore, although the rural diet appeared outwardly monotonous, large between- and within-household variations in the serving size of staple foods were prevalent.
In the pilot study, about eighty food samples were analysed in the laboratory for their energy and protein content to examine between- and within-household variations in the nutrient content of major foods. Despite the fact that samples were taken from different households, the variation in energy content (per 100 g) in roties from household to household was relatively small (CV = 5–10 %). This small exercise revealed a need for a database on nutrient contents of commonly consumed food items at village level because a database on the nutritive values of Indian foods (cooked) was not available. Use of such a database would reduce errors due to the use of different food tables in estimating nutrient intakes (Fig. 1).
Role of community workers
Local village girls, educated up to the 10th standard (above age 16 years), were appointed as community workers (CW). This was necessary because local girls were more acceptable to the rural women and thus helped in overcoming their reluctance for weighing and handling of food by outsiders. They were trained to use food scales for recording the average weights of roties and food servings. For recording such weights, they visited the women before each meal on the day prior to that scheduled for the 24 h recall. On the following day, the woman was interviewed by one of four nutritionists, using a 24 h recall questionnaire, to record portion sizes of roties and servings of rice, dhal and vegetables, in chronological order from morning until dinner time. Weights recorded by the CW were then applied to these portion sizes to quantify intakes of each food item. This prior-day visit of CW helped in converting portion sizes into their weight equivalents and also helped the recall of the mothers on the following day.
Creation of food tables
The existing databases available for nutritive values pertain to only raw foods(Reference Gopalan, Rama Sastri and Balasubramanian6) and were used to estimate the nutrient content of raw foods consumed (such as milk and fruit). In order to create a database of nutrient contents for cooked foods, we collected from each village ten to twenty-five samples of major food items such as roties, rice and dhal, and at least three samples for vegetable preparations. For this purpose, CW were trained to collect representative samples from each household for laboratory analysis.
A laboratory oven was installed in a central village research centre and food samples were dried at 100°C for 12 h, weighed, dried for a further 4–6 h and then re-weighed to ensure that all moisture had been removed. The dried samples were packed individually in air-tight bottles and transported to Pune for laboratory analysis. Protein was estimated by the micro Kjeldhal method using the 1030 Kjeltec autoanalyser system. Fat was estimated using the Soxhlet method in which food samples were subjected to continuous extraction in diethyl ether for 18 h(Reference Raghuramulu, Madhavan and Kalyanasundaram7). Carbohydrates were estimated by subtraction. Analysis of 1227 food samples was done to obtain a database of macronutrient values for 288 distinct food items commonly consumed in this rural community. This database was useful for estimating daily intakes of energy, protein, carbohydrate and fat. It helped to avoid errors involved due to use of food tables and was a useful addition for obtaining precise estimates of maternal intakes.
Validation of the modified 24 h recall method
The modified 24 h recall method thus developed was validated against a ‘reference’ method. In the ‘reference’ method women were followed from early morning until dinner time by a nutritionist and all foods eaten by the woman were weighed using Ishida scales (5 g LC). A sample of each food item consumed (25 % of identical portions of food by weight) was collected in an air-tight plastic container, making composite samples for each women. Thus, for each woman, the foods eaten up until lunch time were pooled together in one composite and foods eaten thereafter until dinner time were pooled to form a second composite sample. These samples were analysed in the laboratory using the methods described above.
On the same day, CW recorded the average weight of roties as well as servings of each food item prepared in the household as part of her routine work. The women were interviewed the next day, by a different nutritionist, for recording the consumption in terms of servings using the modified 24 h recall method. This was helpful to validate the data recorded by CW.
Statistical methods
Mean intakes estimated by modified 24 h recall were compared with those from the reference method using paired t tests. Association between the two was examined with the help of correlation coefficients and regression analysis. Bland–Altman plots(Reference Bland and Altman8) were examined to assess systematic or differential bias in the two methods. We compared intakes in our study with the dietary allowances recommended by the Indian Council of Medical Research(9) and calculated the sensitivity and specificity of the test method for identifying inadequate dietary intakes.
Results
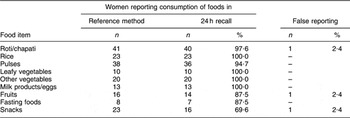
In estimating the daily intake of individuals, it is essential in the first instance to know correctly the foods consumed in a day. This depends on the accuracy of the 24 h recall of the individual. We therefore examined, for each women, the foods listed in the 24 h recall and the corresponding information recorded by an observer for the reference method (Table 1). This comparison was done for major food groups. It was observed that over 95 % of the women were able to recall correctly the staple food items they consumed, such as roti, rice and vegetables. However, for foods like snacks, foods consumed on fasting days and fruits, which are not items of the daily meal, recall accuracy was in the range of 65 % to 85 %. One cannot deny that there could be error due to false reporting of items which are not actually consumed. Although such errors are beyond our control, they were of negligible order (one case out of forty-one).
Table 1 Recall of various food items by respondents in comparison with the reference method: pregnant rural Indian women (n 41), pre-recruitment phase of the Pune Maternal Nutrition Study
Second, comparison for portion sizes was done by comparing the actual weights of consumed foods (reference method) with the estimates obtained using average weights recorded by the CW (modified 24 h recall method), as shown in Table 2. It can be observed that the difference was not significant for any food item. This shows that the average weights of food items recorded by CW on the day prior to the interview were able to estimate adequately the weights of portion sizes of foods recorded in the 24 h recall.
Table 2 Weight of various food items obtained by the two methods: pregnant rural Indian women (n 41), pre-recruitment phase of the Pune Maternal Nutrition Study
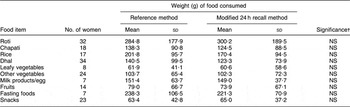
†Difference between the two methods tested using the paired t test.
Finally, the total daily intake estimated by the reference method and the modified 24 h recall method were compared for major macronutrients (Table 3). It can be noted that mean energy and protein intakes were lower compared with the reference method by only 2–6 % while fat intakes were almost the same. None of the differences were statistically significant when compared by the paired t test. Correlation coefficients between the estimates of daily intakes obtained by the two methods were significant, showing a high degree of association. These findings suggest that modifications incorporated in the 24 h recall substantially improved the accuracy of the estimates of maternal intakes.
Table 3 Comparison of nutrient intakes by the two methods: pregnant rural Indian women (n 41), pre-recruitment phase of the Pune Maternal Nutrition Study

Correlation was significant: **P < 0·01.
†Difference between the two methods tested using the paired t test.
Although the above analysis indicated concordance between the two estimates obtained by the two methods, it was not known whether any systematic bias existed. Therefore Bland–Altman plots (Fig. 2) were obtained for energy, protein and fat. These revealed that differences in the two methods were random and did not exhibit any systematic bias. In particular, the modified method was capable of classifying individuals correctly into the same third of the intake distribution obtained by the standard method, thus showing good association between the two methods (P = 0·03 for energy, P = 0·005 for protein and P = 0·03 for fat, χ 2 test).
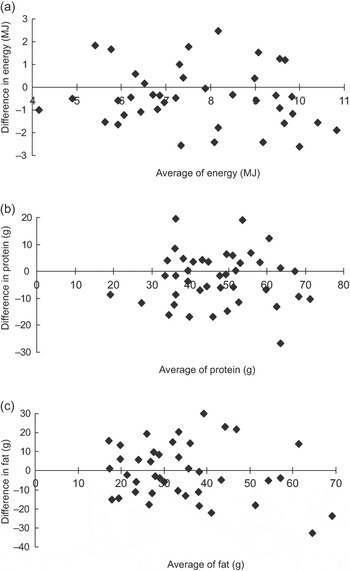
Fig. 2 Bland–Altman plots comparing the reference method and the modified 24 h recall method for: (a) energy (r = −0·0987); (b) protein (r = −0·0254); and (c) fat (r = −0·1473)
For the assessment of a method as a whole, it is advisable not to depend on the correlation coefficient alone, but to calculate some kind of misclassification matrix for all categories of intake(Reference Bellach10). Maternal intakes were therefore examined by the adequacy (or otherwise) of nutrients and data analysed to examine the sensitivity and specificity of the modified method (Table 4). It can be observed that the modified method was sensitive (85 %) to identify energy as well as protein inadequacy in maternal intakes. It also showed reasonably good specificity (82 % for energy and 63 % for protein) and indicated a lower risk of classifying wrongly the maternal intakes as inadequate when they are actually adequate by the standard method. Thus the modified method was found satisfactory even in these aspects.
Table 4 Sensitivity and specificity of the modified method with regard to adequacy of energy and protein intakes: pregnant rural Indian women (n 41), pre-recruitment phase of the Pune Maternal Nutrition Study
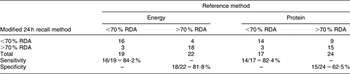
RDA, recommended dietary allowance.
Discussion
Dietary assessment is an inherent part of most nutrition investigations and as such is of concern for every nutritionist. Despite a wide range of techniques available for the assessment of dietary intake, associations of diet with health are often observed to be weak. In particular, despite overwhelming evidence for a relationship between maternal weight changes and birth weight, it is still to be shown that these associations followed from diet(Reference Susser11). One of the ways for improvement is to make the existing techniques more sensitive to community specifics, as there is a large variation from community to community with respect to staple foods, their preparations and dietary habits. Unlike Western communities, mothers from poor communities in rural India are often illiterate, not able to maintain their own food records, busy working on farms making less time available for interviews, rarely consume market foods and have strong food taboos especially in pregnancy – all of these facts need consideration in developing appropriate techniques for assessment of maternal intakes. In the present paper, we describe modifications incorporating such community specifics into the conventional 24 h recall method and the validation of the same.
Initial FGD were extremely useful for devising the questionnaire for the 24 h recall. Our results showed that a prior-day visit by a CW contributed considerably in reducing errors in several ways. It was helpful in overcoming the reluctance of the rural mothers, for getting average weights for food items cooked on that day, and provided help for the actual 24 h recall. In maintaining a food diary there is always a risk that the subject will alter his normal diet, while in the interview method it is easier for the subject to make an incorrect statement about his food habits(Reference Bingham12).
Validation in different settings(Reference Borrelli, Cole, DiBiase and Contaldo4, Reference Chanpagne, Boudreau, Wozniak and Howat13–Reference Bull, Wheeler and Gatenby15) has been confined to weighed records only and has not taken into consideration the nutrient content of foods consumed. Creation of a database on the nutrient content of commonly consumed foods in the rural community therefore was an additional feature of our approach which reduced the errors due to the use of food tables. Further, the use of food tables needs the weights of raw ingredients as well as the final cooked weight of each food preparation for computing conversion factors to estimate the individual’s intake of raw ingredients. This was not feasible in rural conditions and, as laboratory estimations are more precise than those obtained by food tables, the modified method suggested here offered objectivity in the final estimates of daily intake of an individual. It is worthwhile to mention that the modified method was not compared with the conventional 24 h recall method, which is known to have errors, but was compared only with the ‘reference’ method, i.e. weighing method, which ensured the superiority of the modified method in obtaining objective estimates of daily intake in field studies.
Validity describes the degree to which a dietary method measures what it purports to measure(Reference Gibson16), and no one measure alone can determine the validity of a method. The best approach is to look at several such measures for confirmation of results(Reference Bellach10). We used several checks in validating our approach. First, the mean energy and protein intakes (7615 kJ (1820 kcal) and 45·3 g, respectively) obtained by the modified method compared well with those obtained by the reference method (7795 kJ (1863 kcal) and 48·6 g, respectively). Second, correlation analysis showed high values of correlation coefficients, indicating good association between the modified method and the reference method, and also ensured that the relative ranking of maternal intakes was similar by the two methods. Additionally, Bland–Altman plots of estimates by the two methods ensured the absence of systematic bias. Third, our results showed that the method developed had high sensitivity and specificity with regard to identifying inadequate maternal intakes. This observation in fact ensures that objective assessment of maternal intakes is possible in free-living populations.
The method was used to estimate the dietary intakes of rural pregnant mothers in the main study. It was observed(Reference Rao, Yajnik, Kanade, Fall, Margetts, Jackson, Shier, Joshi, Rege and Lubree17) that energy and protein intakes of the rural mothers were low in early (7·4 (sd 2·1) MJ and 45·4 (sd 14·1) g, respectively) as well as late gestation (7·0 (sd 2·0) MJ and 43·5 (sd 13·5) g, respectively). However, they were comparable to the observations from other Indian studies(Reference Rawtani and Varma18, Reference Vijayalaxmi and Lakshmi19). The 24 h recall is known to underestimate the individual’s intake(Reference Borrelli, Cole, DiBiase and Contaldo4). Estimate of under-reporting using the cut-off of 1·2 × BMR(Reference Goldberg, Black, Jebb, Cole, Murgatroyd, Coward and Prentice20) was 23 % when BMR was estimated from the FAO/WHO/United Nations University equation(21). It has been shown(Reference Piers and Shetty22) that the measured BMR of even well-nourished Indian women is lower than that predicted by this equation. For the rural undernourished mothers (average body weight 42·0 kg) in the present study, actual BMR would be lower still. Therefore the above percentage cannot solely be attributed to under-reporting and may indicate genuinely low intakes in these rural Indian women.
Our study underscores that simple modifications to conventional methods backed by understanding of community specifics and nutritional peculiarities are of immense importance in obtaining objective estimates of daily intakes of individuals in free-living populations. The approach would be adaptable in other communities in India and in other developing countries where illiteracy in women is a major obstacle to using food diaries or self-weighing methods commonly employed in developed countries.
Acknowledgements
We acknowledge the help of the Director, Agharkar Research Institute, for providing the necessary facilities to carry out this research work. Thanks are also due to field staff for collecting the data. We declare that there is no conflict of interest. S.R. was responsible for conceptualizing and writing the manuscript; A.N.K. was responsible for data collection and data analysis; S.R.J. was responsible for the nutrient estimation of food samples; C.S.Y. was one of the Principal Investigators of the collaborative study. Financial support for the study was given by the Wellcome Trust, London, UK and the Medical Research Council, UK.






