



Preventable conditions such as CVD, cancer and type 2 diabetes are the leading causes of death in Puerto Rico (PR) and have put an increasing toll on the island’s ageing population and health infrastructure(Reference Rodríguez Ayuso, Geerman and Pesante1,2) . In 2017, 17·2 % of the adult population in PR had been diagnosed with diabetes, constituting the highest observed prevalence of the disease among all US states and territories(3). Compared with the USA, PR also has a higher prevalence of risk factors such as hypertension (44·7 v. 32·3 %) and overweight and obesity (68·3 v. 66·6 %)(3). Disparate mortality from diet-related chronic diseases has also been noted for PR residents compared with Puerto Ricans residing in the mainland USA(Reference Colón-Ramos, Rodríguez-Ayuso and Gebrekristos4).
One major correlate to current chronic disease global trends has been a dietary shift from the consumption of locally grown agricultural foods towards a modernised, imported diet(Reference Popkin5,Reference Hawkes, Chopra, Friel, Labonté, Schrecker and Packer6) . In the early 20th century, as much as 90 % of PR’s 2·2 million acres were devoted to agrarian activities, bolstering the local economy and producing a vast majority of the island’s food supply(Reference Carro-Figueroa7,Reference Gould, Fain and Pares8) . Agriculture in the rural, mountainous countryside mostly composed of subsistence farming(Reference Carro-Figueroa7), and rural populations demonstrated a lower prevalence of obesity and micronutrient deficiencies as compared with their urban and upper income counterparts(Reference Fernandez9). At the time, the majority of total energy intake in PR was composed of homegrown starchy vegetables such as plantains and root crops, which were associated with lower energy intake and higher vitamin C levels than cereal grains in the typical diet(Reference Carro-Figueroa7,Reference Fernandez9,Reference Cook, Rivera and Torres Díaz10) . Although by the 1950s, imported rice, beans and codfish were increasingly consumed, 59 % of the total volume of food consumed in PR was still produced locally(Reference Carro-Figueroa7). Local production also supplied 93 % of available fresh fruits such as pineapple, avocado and oranges which – although consumed in small amounts among Puerto Rican adults – were significant sources of several vitamins and minerals(Reference Fernandez9).
In the mid- to late 20th century, governmental policies favouring industrialisation and tourism services indirectly contributed to significant declines in local food production. Today, over 85 % of the Puerto Rican food supply is imported and is increasingly composed of energy-dense cereals, animal products, fats and other processed foods(11,Reference Sinha12) . In addition to food insecurity, rural unemployment and augmented vulnerabilities to natural disasters in an imported food supply(Reference Carro-Figueroa7,Reference Gould, Fain and Pares8,Reference Gould, Wadsworth and Quiñones13) , a replacement of locally grown staple foods with imported products in island food systems may be implicated in diminished diet quality and the rise of diet-related chronic conditions(Reference Sinha12,Reference Parry14) . In island settings across the Pacific and Caribbean, reduced consumption of locally grown fresh produce such as fruit, vegetables, roots, tubers and legumes has been associated with declines in the nutritional status of these populations(Reference Sinha12,Reference Seiden, Hawley and Schulz15) . Additionally, increased reliance on imported food products has been shown to augment the availability of total energy and dietary fat, particularly from animal sources and vegetable oils(Reference Sinha12,Reference Seiden, Hawley and Schulz15) . In PR, a shift away from fresh fruit, vegetables and legumes towards energy-dense imported products may have also played a role in the ongoing nutrition and epidemiologic transitions on the island(Reference Fernandez9,Reference Sinha12) . Sugary beverages, sweets, dairy products and processed meats are currently the major contributors to total energy intake among adults in PR(Reference Mattei, Tamez and Bigornia16), a dietary reliance on processed foods that may be associated with increased health risks. For example, high intake of sweetened drinks – coupled with low intake of fruits, vegetables and fibre – has been associated with adiposity among individuals in PR(Reference Soltero and Palacios17).
Although agriculture now constitutes <1 % of the local economy(Reference Gould, Fain and Pares8), the production and purchase of locally grown foods persist in PR. According to the United States Department of Agriculture, fruits and vegetables such as plantains, root crops and melons currently make up the majority of PR’s crop production(18). Although staples such as meat, rice and beans are mostly imported, the local agricultural market continues to supply the majority of locally consumed plantains, green bananas, squash and peppers(Reference González and Gregory19). A growing movement among consumers, local governments and the private sector has also encouraged the purchase of foods ‘Made in Puerto Rico’, emphasizing nutrition, climate resilience and the cultural heritage of farming on the island(Reference Gould, Fain and Pares8,11,Reference González and Gregory19) . The ability of vastly unused but well-suited agricultural land(Reference Gould, Wadsworth and Quiñones13) to bolster consistent and self-sufficient access to high-quality foods, conserve landscapes and environmental resources and maintain rural quality of life is also of increasing sociocultural concern(Reference González and Gregory19). The availability of locally produced fresh fruits and vegetables may therefore offer culturally relevant, nutritious and unprocessed alternatives to many imported products.
Although local foods may play a potential role in a healthful diet, only a handful of studies have examined the impact of locally produced food purchasing on food consumption patterns. One intervention study among adults in the mainland USA demonstrated mixed results, with compliance to a ‘local food’ diet resulting in reduced energy and protein intake as well as increased consumption of fruits, vegetables, dietary cholesterol and saturated fat(Reference Rose, Serrano and Hosig20). Another study using US county-level data has shown a modest association between a strong local food economy, including density of farmers’ markets, and lower prevalence of obesity and diabetes(Reference Salois21). Among a cross-sectional sample of young adults in the USA, individuals with positive attitudes towards local, sustainable food consumed more fruits, vegetables and dietary fibre as well as less added sugars, sugar-sweetened beverages and dietary fat than those who placed low importance on these practices(Reference Pelletier, Laska and Neumark-Sztainer22). In addition to nutritional health, political and sociocultural interests in food sovereignty, sustainability and local economic growth may also motivate local food purchasing in PR(Reference González and Gregory19). Although there is growing evidence pointing to the potential dietary benefits of locally grown foods, the association between intentionally purchasing local foods (IPLF) and diet quality has not been documented in PR.
To address this gap in the literature, the current study aimed to characterise the association between intentionally IPLF and diet quality among adults in PR. We hypothesised that IPLF would be associated with higher diet quality as well as higher adherence to dietary recommendations for nutrient intake in this population. By identifying specific features in the dietary patterns of adults who currently purchase local foods in PR, this research will offer important insights on the potential intersection of health and agriculture in the island food system.
Methods
Study population
Data were obtained from adults residing in PR participating in the cross-sectional study the Puerto Rico Assessment of Diet, Lifestyle, and Diseases conducted in 2015. The study design and methodology of Puerto Rico Assessment of Diet, Lifestyle, and Diseases have been described in detail elsewhere(Reference Mattei, Rodríguez-Orengo and Tamez23). Study participants were convenience sampled from patients, their companions or visitors of three primary care clinics in the San Juan metropolitan area. The three primary clinics allowed for socioeconomic representation of participants. Eligible individuals must have been living in PR at the time of the study and for at least 10 months of the previous year, aged 30–75 years and able to answer questions without assistance. All data were collected via interview-administered questionnaires by trained, bilingual research assistants using the electronic data capture tool ‘Research Electronic Data Capture’(Reference Harris, Taylor and Thielke24). The written questionnaires were in Spanish, and some questions adapted from previous research were modified using Puerto Rican vernacular. All participants provided written informed consent.
Intentionally purchasing local foods
IPLF was captured as part of a questionnaire which assessed dietary behaviours and attitudes, adapted from the Food Attitudes and Behaviors Survey of the National Cancer Institute(Reference Emanuel, McCully and Gallagher25,Reference Goodman, Blanck and Sherry26) , questions asked in the Hispanic Community Health Study/Study of Latinos(Reference Fernandez, Olendzki and Rosal27) and a validated dietary behaviours questionnaire for Latinos(Reference Tucker, Bianchi and Maras28). Participants were asked thinking about their usual habits in the past year: ‘How often do you purposely purchase foods from PR (like fruits, vegetables, meat and other products that are produced on the island rather than being imported)?’ and had the following response options: ‘rarely/never,’ ‘sometimes,’ ‘many times’ and ‘all the time.’
Dietary measures
Self-reported usual dietary intake in the past 12 months was captured by trained interviewers using a semi-quantitative FFQ adapted from the National Cancer Institute-Block FFQ by including culturally relevant foods and portion sizes that were major contributors to energy and nutrient intake for this population(Reference Tucker, Bianchi and Maras28). This instrument has been previously adapted and validated for a Puerto Rican population living on the island(Reference Tucker, Bianchi and Maras28,Reference Palacios, Trak and Betancourt29) . Participants with energy intakes <2510·4 kJ (<600 kcal) or >20083·2 kJ (>4800 kcal) and/or two or more sections of the questionnaire left blank were excluded from the analysis. The electronically captured data from the FFQ were linked to the Minnesota Nutrient Data System (version 5.0_35) for food and nutrient analyses. Values reported in this analysis correspond only to nutrients derived from dietary intake and do not include supplement use.
Diet quality was assessed using the Alternate Healthy Eating Index 2010 (AHEI), a validated measure predictive of chronic disease risk(Reference Chiuve, Fung and Rimm30). Among a sample of Puerto Rican adults living in the USA, higher AHEI has been found to be associated lower waist circumference, blood pressure and blood glucose as well as higher serum HDL-cholesterol at 2 years(Reference Mattei, Sotres-Alvarez and Daviglus31). The AHEI is composed of eleven components including vegetables without potatoes (servings/d), fruit without juices (servings/d), whole grains (g/d), sugar-sweetened beverages and fruit juice (servings/d), nuts and legumes (servings/d), red/processed meat (servings/d), trans fat (% of energy), long-chain (n-3) fats (EPA + DHA, mg/d), PUFA (% of energy), Na (mg/d) and alcohol (drinks/d). Participants were scored for each AHEI components from 0 (least healthy) to 10 (healthiest) as continuous; intermediate levels were prorated based on pre-selected cut-offs of recommended intake. The component scores were then added for a total AHEI score ranging from 0 (lowest diet quality) to 110 (highest diet quality).
Dietary reference intakes were assessed to determine nutritional status and defined using proposed guidelines from the National Academy of Sciences for selected main nutrients in the diet that are deemed important for health maintenance and disease prevention(32), including vitamins D, B12 and B6 folate, Ca, Mg, Fe, K and Na. Meeting dietary recommendations for these nutrients was defined as reported intake within the dietary reference intakes age- and sex-specific cut-offs. The percent meeting dietary recommendations in the study sample was determined using estimated average requirement (EAR, or the value estimated to meet the requirement of half the healthy individuals in the population), except for K and Na for which there is no EAR and adequate intakes (AI, or the value based on observed or experimentally determined approximations of nutrient intake by a group of healthy people) were estimated instead.
Covariate assessment
Information on covariates was collected as part of a questionnaire assessing demographic and socioeconomic characteristics, medical history, lifestyle behaviours and psychosocial measures. Age, sex, ethnicity, educational attainment, income, rural residency and use of the Supplemental Nutritional Assistance Program were self-reported. Participants were also asked to report their history of smoking, which was classified as current, former or never smoker. Physical activity was assessed using a modified Paffenbarger questionnaire of the Harvard Alumni Activity Survey(Reference Paffenbarger, Wing and Hyde33), previously used in a Puerto Rican cohort(Reference Tucker, Mattei and Noel34) and with scores defined as: <30 sedentary physical activity, 30 to <40 light activity and ≥40 moderate/vigorous activity. Nutritional awareness was probed by asking participants how often they sought and used nutritional/health information.
Statistical analysis
Statistical analysis included participants who completed the FFQ and responded to the question on IPLF (n 243 out of 248). Sociodemographic and behavioural characteristics were similar for Puerto Rico Assessment of Diet, Lifestyle, and Diseases participants who did and did not have complete, valid FFQ data(Reference Mattei, Tamez and Bigornia16). Only 12 % of participants reported ‘rarely/never’ IPLF, and thus to improve statistical power, the two lowest frequencies of IPLF (i.e. ‘rarely/never’ and ‘sometimes’) were combined as one category (hereafter referred to as ‘seldom’) and used as the reference group for all analyses. For clarity, the ‘many times’ response will be referred to as ‘often’ IPLF, and the ‘all the time’ response will be referred to as ‘always’ IPLF. Means (sd) or percentages of all covariates were calculated, and differences across categories of IPLF were detected using a t test for continuous variables or χ 2 test for categorical variables.
Dietary intake of energy and nutrients as well as the percent of participants meeting dietary recommendations was determined, and differences by category of IPLF were detected using t-test for continuous variables or χ 2 test for categorical variables. Means (sd) for all nutrients (except for percentages from total energy intake of carbohydrates, protein, fat and alcohol) were log-transformed due to skewed distributions and were adjusted for age, sex and total energy intake using the residuals method.
Multivariate generalised linear models (GLM) were fitted to determine the adjusted means of AHEI scores and its components by IPLF categories. A partially adjusted model was estimated controlling for age, sex, ethnicity, educational attainment, income, rural residency and use of Supplemental Nutritional Assistance Program food assistance. A fully adjusted model further adjusted for behavioural factors – namely, physical activity, smoking status, nutritional awareness, as well as total energy intake (kcal/d). Covariate adjustment was carried out based on established findings in the literature. For example, food consumption among Puerto Rican adults has been associated with various behavioural and sociodemographic factors, including age, sex, education, income, smoking status and physical activity(Reference Colon-Ramos and Perez-Cardona35,Reference Colon-Ramos, Perez-Cardona and Monge-Rojas36) . Rural residency was controlled for due to a higher density of agricultural food production in rural areas in PR(Reference Gould, Wadsworth and Quiñones13). Additionally, because use of Supplemental Nutritional Assistance Program food assistance may affect food purchasing behaviours(Reference Condon, Drilea and Jowers37), this covariate was also controlled for. Finally, nutritional awareness was included in the model because seeking out nutritional/health information has been associated with attitudes towards local foods and diet quality(Reference Pelletier, Laska and Neumark-Sztainer22). A supplemental analysis was conducted to identify the top five food contributors by mean proportion of total energy intake to the components of the AHEI with statistically significant differences across IPLF categories.
Statistical significance was defined a priori at an α of 0·05. All analyses were performed using SAS software version 9.4 (SAS Institute Inc.).
Results
Most participants were female (68·9 %), Puerto Rican (79·4 %) had attained college or higher education (62·4%) and had a total household income <$10 000 (56·9 %) (Table 1). Seldom IPLF was reported by nearly a third (33·9 %) of participants, 33·5 % reported often and 30·6 % reported always IPLF. There was no significant difference in covariate distributions across IPLF groups, except for age, such that, on average, participants who often and always IPLF were older than those who seldom did so.
Table 1 Sociodemographic and behavioural characteristics by frequency of intentionally purchasing local food among adults living in Puerto Rico*

GED, General Education Diploma; SNAP, Supplemental Nutritional Assistance Program.
* Shown as mean values and standard deviations or percent, as assessed from a subset of a cross-sectional convenience sample of 380 adults aged 30–75 years recruited in 2015 from primary care clinics in the San Juan, Puerto Rico metropolitan area who completed a culturally adapted FFQ.
† Defined as how often the participant purposely purchased foods from Puerto Rico (like fruits, vegetables, meat and other products that are produced on the island rather than being imported). Analyses were carried out on participants with non-missing responses (n 243); eighty-four participants responded ‘rarely/never’ or ‘sometimes’ (combined for the reference group and referred to as ‘seldom’); eighty-three responded ‘many times’ (referred to as ‘often’) and seventy-six responded ‘all the time’ (referred to as ‘always’).
‡ Sedentary physical activity defined as a score <30, light activity as 30 to <40 and moderate/vigorous activity as ≥40, as captured using a modified Paffenbarger questionnaire.
§ Defined as how often the participant seeks out and uses health/nutritional information obtained by any means (television/magazine/Internet).
|| Defined as any member of the household currently receiving benefits from SNAP.
¶ Statistical significance for differences between categories of intentionally purchasing local foods determined by two-sided t test or χ 2 test.
Compared with participants who reported seldom IPLF, those who always IPLF had a significantly higher percentage of total energy coming from carbohydrates (54·8 v. 52·1 %; P = 0·018) as well as higher intake of dietary fibre (27·6 v. 21·3 g/d; P < 0·0001), vegetable protein (29·2 v. 25·3 g/d; P = 0·0003), n-3 fatty acids (1·9 v. 1·6 g/d; P = 0·008), folate (495 v. 418 μg/d; P = 0·0003), Mg (341 v. 295 mg/d; P < 0·0001), Fe (16·0 v. 14·8 mg/d; P = 0·036) and K (3719 v. 3104 mg/d; P < 0·0001) (Table 2). Participants in the always IPLF category also had significantly lower starch:fibre ratio (4·2 v. 5·2; P < 0·0001) and lower intake of animal protein (46·5 v. 53·2 g/d; P = 0·012), SFA (21·4 v. 24·0 g/d; P = 0·006), trans fatty acids (2·4 v. 3·1 g/d; P < 0·0001) and cholesterol (309 v. 399 g/d; P = 0·008) than their seldom IPLF counterparts. Finally, compared with those who seldom IPLF, a larger proportion of adults in the study sample who always IPLF met dietary recommendations for vitamin D (1·2 v. 7·9 %, P = 0·038), Mg (71·1 v. 52·4 %; P = 0·016) and K (14·5 v. 1·2 %; P = 0·001). No significant differences were noted between participants who often and seldom IPLF, except for a higher consumption of dietary fibre among individuals who often IPLF (online Supplementary Table S1).
Table 2 Mean intake of energy and nutrients, and percent meeting dietary recommendation, by those who seldom and always intentionally purchase local foods among adults in Puerto Rico
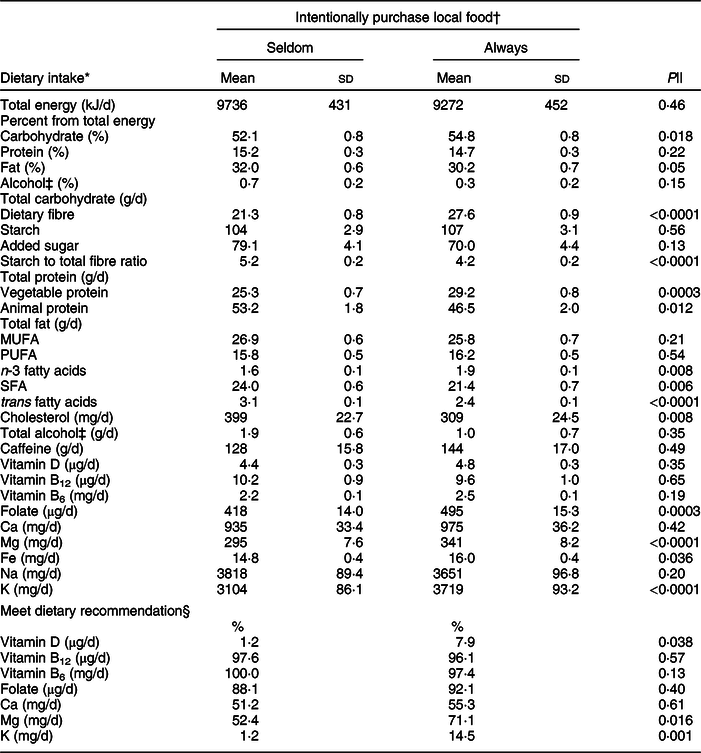
* Dietary intake values correspond to dietary intake only (without supplements use) in g/d unless indicated otherwise. Mean values and standard deviations for all nutrients (except for total energy intake and percentages from total energy intake of carbohydrates, protein, fat and alcohol) were log-transformed due to skewed distributions and were adjusted for age, sex and energy intake using the residuals method.
† Defined as how often the participant purposely purchased foods from Puerto Rico (like fruits, vegetables, meat and other products that are produced on the island rather than being imported). Analyses were carried out on participants with non-missing responses (n 243); eighty-four participants responded ‘rarely/never’ or ‘sometimes’ (combined for the reference group and referred to as ‘seldom’), eighty-three responded ‘many times’ (referred to as ‘often’) and seventy-six responded ‘all the time’ (referred to as ‘always’).
‡ Alcohol intake is restricted to only those who reported consuming alcoholic beverages (n 234).
§ Shown as percent meeting the estimated average requirement (EAR, or the value estimated to meet the requirement of half the healthy individuals in the group), except for K and Na for which there is no EAR and adequate intakes (AI, or the value based on observed or experimentally determined approximations of nutrient intake by a group of healthy people) were estimated instead. Corresponds to dietary intake only (without supplements use) adjusted for energy intake using the residuals method.
|| Statistical significance for differences between categories of intentionally purchasing local foods determined using two-sided t test or χ 2 test.
As compared with those who seldom IPLF, mean AHEI scores were 3·6 (P = 0·038) points higher among those often IPLF and 9·3 (P < 0·0001) points higher among those always IPLF, after adjusting for relevant covariates (Table 3). These associations remained statistically significant from the unadjusted to the partially adjusted and fully adjusted models. AHEI component scores were analysed to determine specific associations of IPLF. Compared with those who seldom IPLF, participants who always IPLF had significantly higher fully adjusted mean AHEI component scores for vegetables (7·1 v. 5·1; P < 0·0001), fruits (3·6 v. 2·0; P = 0·0002), whole grains (6·7 v. 5·5; P = 0·039), nuts and legumes (6·7 v. 5·6; P = 0·034), trans fat (7·3 v. 6·5; P = 0·0003) and long-chain (n-3) fats (7·6 v. 6·7; P = 0·002) (Table 4). Participants who reported often IPLF also had higher scores for each of these six AHEI components; however, differences were only significant for vegetables (6·6 v. 5·1; P = 0·0004) and n-3 fats (7·2 v. 6·7; P = 0·048) scores. As a supplemental analysis, we ranked the top five foods contributing to total energy intake for these six AHEI components by IPLF category. The top five foods ranking exclusively among participants who responded often or always, but not seldom, IPLF included romaine lettuce, winter squash, apples, hummus, white beans, canola oil and salad dressing (online Supplementary Table S2). These participants also tended to have a higher contribution to total energy from sweet potatoes, avocados and old-fashioned oatmeal, but lower from french fries. On the other hand, cassava, turnip, microwaved popcorn and mayonnaise were ranked exclusively among those who responded seldom IPLF.
Table 3 Adjusted means of the alternate health eating index-2010 by frequency of intentionally purchasing local food among adults living in Puerto Rico

* Defined as how often the participant purposely purchased foods from Puerto Rico (like fruits, vegetables, meat and other products that are produced on the island rather than being imported). Analyses were carried out on participants with non-missing responses (n 243); eighty-four participants responded ‘rarely/never’ or ‘sometimes’ (combined for the reference group and referred to as ‘seldom’), eighty-three responded ‘many times’ (referred to as ‘often’) and seventy-six responded ‘all the time’ (referred to as ‘always’).
† Adjusted for sociodemographic covariates: age, sex, ethnicity, level of education, total household income, rural residency and use of Supplemental Nutritional Assistance Program (SNAP) food assistance.
‡ Adjusted for all sociodemographic covariates in model 1 as well as behavioural covariates: physical activity, smoking status, nutritional awareness and total energy intake (kcal/d, to convert kcal to kJ multiply it by 4·184).
§ Statistical significance for differences between means determined by two-sided t test.
Table 4 Adjusted means of component scores* of the alternate health eating index-2010 by frequency of intentionally purchasing local foods among adults living in Puerto Rico

* Component scores range from 0 to 10, with higher scores denoting healthier intake.
† Defined as how often the participant purposely purchased foods from Puerto Rico (like fruits, vegetables, meat and other products that are produced on the island rather than being imported). Analyses were carried out on participants with non-missing responses (n 243); eighty-four participants responded ‘rarely/never’ or ‘sometimes’ (combined for the reference group and referred to as ‘seldom’), eighty-three responded ‘many times’ (referred to as ‘often’) and seventy-six responded ‘all the time’ (referred to as ‘always’).
‡ Adjusted for age, sex, ethnicity, level of education, total household income, rural residency, use of Supplemental Nutritional Assistance Program food assistance, physical activity, smoking status, nutritional awareness and total energy intake (kcal/d, to convert kcal to kJ multiply it by 4·184).
§ Statistical significance for differences between means determined by two-sided t test.
Discussion
The results of this analysis demonstrate that adults in PR who intentionally purchase local food products generally had healthier dietary intake than those who seldom do so. The association between local food purchasing behaviour and diet quality was strongest among individuals who always purchase locally, and intermediate results were observed among those who often purchase locally. The diet of adults in PR who intentionally purchase local food was higher in fruits, vegetables, whole grains and nuts and legumes; consisted of a healthier fat profile and better met nutritional recommendations. Previous research has similarly suggested that individuals motivated to purchase locally grown produce may experience improved dietary intake and health status(Reference Vasquez, Sherwood and Larson38). These findings also align with previous ecological evidence linking a nutrition transition towards modernised, imported diets to declines in diet quality(Reference Popkin5,Reference Hawkes, Chopra, Friel, Labonté, Schrecker and Packer6) . Although disease-related dietary shifts have been documented in PR and similar island settings(Reference Fernandez9,Reference Sinha12,Reference Parry14,Reference Seiden, Hawley and Schulz15) , the ability of local food production to support a healthy diet had been largely unexplored. Overall, these findings support the need for further longitudinal and interventional research to confirm that local food purchasing behaviour plays a role in nutrition and disease prevention, particularly in regions transitioning away from the production and consumption of local foods.
A markedly higher consumption of vegetables and fruits, including squash, sweet potatoes, avocado, and beans, among individuals who purchase locally likely reflects locally available agricultural products in PR(18). Individuals who always purchase locally were more likely to meet dietary recommendations for Mg and K, minerals found in fruits and vegetables commonly consumed in the Puerto Rican diet(Reference Lopez39). Many of these locally produced foods are also high in fibre(Reference Slavin40) and are good sources of folate (e.g. bananas, citrus fruits)(Reference Subar, Block and James41) and Fe (e.g. beans)(Reference Block, Dresser and Hartman42), which may explain higher intake of these nutrients among those who always purchase locally. Additionally, high local food purchasing behaviour was associated with lower saturated fat, trans fat and cholesterol as well as higher omega-3 fat intake. This healthier fat profile may be due, in part, to a replacement of animal protein containing high levels of unhealthy fats(Reference Valsta, Tapanainen and Mannisto43), with legumes and other plant-based proteins. Higher consumption of plant-based foods among individuals who purchase locally may also translate to long-term health benefits, as a dietary shift from animal to plant-based protein has been associated with lower mortality risk(Reference Song, Fung and Hu44). Taken together, these results suggest that adults in PR are obtaining important nutritional benefits from the consumption of local agricultural products and a more minimally processed plant-based diet.
The benefits of local food purchasing behaviour may extend to agricultural development, food security and environmental sustainability in PR. Amplifying food autonomy in a climate-vulnerable food system is of cultural and sociopolitical interest, with many small farmers on the island increasingly relying on backyard agriculture, fishing and agroecology for self-reliant sustenance and informal economic productivity(Reference Garriga-López45). Recent calls for climate-sensitive global food systems also encourage the adoption of a plant-based diet, with an emphasis on increasing vegetables, fruit, legumes, whole grains and nuts as well as decreasing red meat and other animal products in the diet(Reference Willett, Rockström and Loken46). The results of our study suggest that local food production may play a role in meeting these goals. For example, increased cultivation of beans, a nutritious and frequently consumed staple in Puerto Rican cuisine(Reference Mattei and Campos47), as a plant-based protein may decrease environmental costs associated with red meat and dairy production on the island(18,Reference Eshel, Shepon and Makov48,Reference Frank, Havlík and Stehfest49) . Local agricultural systems may also decrease dependence on imported products, supporting rural economies(Reference Gould, Fain and Pares8) and providing fresher, more nutrient-rich foods than stored, frozen or canned varieties(Reference Rickman, Barrett and Bruhn50). With 42 % of the island’s land mass currently suitable for farming and recent upticks in organic and hydroponic vertical production, local food systems may play a renewed role in increasing healthy food availability through climate-adaptive farming practices(Reference Gould, Wadsworth and Quiñones13,18) .
Notably, the intake of unhealthy foods and nutrients – such as sugar-sweetened beverages, red/processed meat and Na – among those who always purchase locally did not differ from those who seldom purchased local foods. These findings reflect a generally high consumption of processed foods in PR, contributing to overall poor diet quality and nutritional status on the island(Reference Mattei, Tamez and Bigornia16,Reference Colon-Ramos, Perez-Cardona and Monge-Rojas36) . Despite a small local foods sector, the Puerto Rican food supply is still overwhelmingly composed of imported products, many of which are highly processed and relatively inexpensive when compared with locally produced fresh foods(Reference Carro-Figueroa7,11) . Therefore, although the promotion of local foods in PR may have benefits for healthy food consumption, other efforts may be necessary to reduce the consumption of unhealthy foods in the population.
Some limitations of our study should be mentioned. Convenience sampling in the metropolitan area of PR may limit generalisability, as participants had high levels of education; additionally, those with complete FFQ data were more likely to be employed which may induce selection bias(Reference Mattei, Tamez and Bigornia16). As a subjectively assessed measure, misclassification of IPLF frequency – albeit non-differential – may also be possible. Additionally, no direct relationship between purchasing intentions and actual food purchases can be made, and future work is needed to determine the origin of each food item in the dietary measure. Because of the cross-sectional design of the study, directionality of associations cannot be established. It may be possible, for example, that previous healthful dietary intake may encourage individuals to purchase local food due to perceptions of higher quality and/or motivation to support the local food economy(Reference Pelletier, Laska and Neumark-Sztainer22). This limitation, however, was partially addressed by controlling for participants’ nutritional awareness, which may be related to both dietary intake and food purchases. Similarly, we adjusted for other social and behavioural factors that may be associated with the likelihood of purchasing local products and diet quality, including age, gender, income, education and food assistance(Reference Colon-Ramos and Perez-Cardona35–Reference Vasquez, Sherwood and Larson38). However, it is possible that our statistical models did not adjust for all potential complex social, behavioural and economic confounding factors. Finally, a limited sample size may have impeded our ability to detect other important associations; however, based on the consistency and strength of current findings, a larger sample size and further adjustments may only help confirm the association between IPLF and diet quality.
The promotion of high-quality staple foods has already been identified as an important step in combatting chronic disease risk, particularly in areas with ongoing nutrition and epidemiologic transitions(Reference Mattei, Malik and Wedick51). Although this report is exploratory in nature, it supports the potential utility of local food purchasing in attaining this goal, highlighting important intersections between nutritional health and local food economies in these settings. In PR and similar food systems, policies that bolster local food production may simultaneously promote a healthier and more sustainable plant-based diet. Given recent calls for health- and climate-informed global food policies(Reference Willett, Rockström and Loken46,Reference Popkin52,Reference Frison, Smith and Johns53) , future research should investigate the ability of local food purchasing behaviour to strengthen the nutritional benefits and environmental sustainability of local food systems across a range of cultural, political and socioeconomic contexts. Local food purchasing in PR may serve as an important nexus for nutrition and agriculture that can serve as a model for more healthful food systems around the world.
Acknowledgements
Acknowledgements: The Puerto Rico Assessment of Diet, Lifestyle, and Diseases study thanks to the contribution from all our interviewers, the staff at the partner clinics and the participants. Financial support: The study was funded by private anonymous donations to Harvard TH Chan School of Public Health, a Dry Bean Health Research Program Incentive Award from the Northarvest Bean Growers Association and institutional funds from FDI Clinical Research. Further funding assistance was obtained from the NIH-National Heart Lung and Blood Institute grant number R01-HL143792 and NIH-National Institute on Minority Health and Health Disparities grant number R21-MD013650. AM was funded by the NIH National Research Service Award (NRSA) Training Grant in Academic Nutrition (grant number T32 DK 007703). MT was funded by the National Council of Science and Technology (CONACyT, Mexico), and JM was supported by a Mentored Career Development Award to Promote Faculty Diversity in Biomedical Research from the NHLBI (grant number K01-HL120951). The Northarvest Bean Growers Association, CONACyT, NHLBI, NIMHD and NRSA had no role in the design, analysis or writing of this article. Conflict of interest: None. Authorship: A.M. conceptualised the research question, conducted data analysis and interpretation and wrote the manuscript. M.T. and J.F.R.-O. contributed to data acquisition, validation and interpretation. J.M. was principal investigator on the study and conceptualised the study, supervised conduct and management of the study and data quality control, conducted interpretation of the results and contributed to the manuscript. All authors listed have reviewed and approved the final version of the manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving research study participants were approved by the Institutional Review Board at Harvard T.H. Chan School of Public Health, University of Massachusetts-Lowell, Northeastern University and Ponce Health Sciences University. Written informed consent was obtained from all participants.
Supplementary material
For supplementary materials accompanying this paper visit https://doi.org/10.1017/S1368980020003134






