



Introduction
Depression is the most common psychiatric disease worldwide, with an immense cognitive, social, and economic burden (Malhi & Mann, Reference Malhi and Mann2018). Currently, approximately 280 million people are affected by depression (GBD 2019 Diseases and Injuries Collaborators, 2020), making depression the leading cause of losing years of life due to disability (Friedrich, Reference Friedrich2017; World Health, 2017). The World Health Organization ranked major depression as the third leading cause of disease worldwide and predicted that it will be the first public health concern by 2030 (World Health, 2008). Anxiety is also one of the most common mental health problems, with global estimates ranging from 3.8 to 25% across countries. Since 1990, there has been a 50% increase in the absolute number of patients with anxiety disorders (Z. Zhang et al., Reference Zhang, Wu, Zhong, Zhou, Liu, Li and Yang2021). Additionally, research around the world has reported an increase in the prevalence of anxiety and depression symptoms during the COVID-19 outbreak (COVID-19 Mental Disorders Collaborators, 2021).
During the past decades, many prominent basic and clinical studies have been carried out to elucidate the underlying causes of depression (Saveanu & Nemeroff, Reference Saveanu and Nemeroff2012). A variety of factors including genetic predisposition, cognitive dysfunctions, stressful life events, interpersonal dysfunction, biological differences, and inherited traits are implicated in developing depression and anxiety (Altemus, Sarvaiya, & Neill Epperson, Reference Altemus, Sarvaiya and Neill Epperson2014; Hammen, Reference Hammen2018; Morssinkhof et al., Reference Morssinkhof, van Wylick, Priester-Vink, van der Werf, den Heijer, van den Heuvel and Broekman2020; Penner-Goeke & Binder, Reference Penner-Goeke and Binder2019). Studies in nutritional psychiatry have suggested some evidence of the role of dietary factors in developing depression and management of depressive symptoms (Marx et al., Reference Marx, Lane, Hockey, Aslam, Berk, Walder and Jacka2021; Pano et al., Reference Pano, Martínez-Lapiscina, Sayón-Orea, Martinez-Gonzalez, Martinez and Sanchez-Villegas2021). Furthermore, some studies investigated the effect of single micronutrient supplementation such as folate (Altaf, Gonzalez, Rubino, & Nemec, Reference Altaf, Gonzalez, Rubino and Nemec2021; Jin et al., Reference Jin, Cheng, Yu, Tao, Huang and Wang2022), zinc (Yosaee et al., Reference Yosaee, Clark, Keshtkaran, Ashourpour, Keshani and Soltani2022), alpha-tocopherol (Lee et al., Reference Lee, Tariq, Lau, Tok, Tam and Ho2022), iron (Huang, Bilgrami, & Hare, Reference Huang, Bilgrami and Hare2022), and vitamin D (Parker, Brotchie, & Graham, Reference Parker, Brotchie and Graham2017) on depression management. Of note, due to its possible role in the function of the brain, vitamin D has received much attention among micronutrients (Anglin, Samaan, Walter, & McDonald, Reference Anglin, Samaan, Walter and McDonald2013).
Vitamin D is a neuroprotective hormone, representing important roles in immune system regulation, promoting cell growth and differentiation, and anti-inflammatory pathways (Holick, Reference Holick2007). It also regulates many essential genes involved in the brain function (Sultan et al., Reference Sultan, Taimuri, Basnan, Ai-Orabi, Awadallah, Almowald and Hazazi2020). Several meta-analyses of epidemiological studies have suggested a positive relationship between vitamin D deficiency and risk of developing depression (Anglin et al., Reference Anglin, Samaan, Walter and McDonald2013; Ju, Lee, & Jeong, Reference Ju, Lee and Jeong2013).
Although some review studies have presented suggestions of a beneficial effect of vitamin D supplementation on depressive symptoms (Anglin et al., Reference Anglin, Samaan, Walter and McDonald2013; Cheng, Huang, & Huang, Reference Cheng, Huang and Huang2020; Mikola et al., Reference Mikola, Marx, Lane, Hockey, Loughman, Rajapolvi and Ruusunen2023; Shaffer et al., Reference Shaffer, Edmondson, Wasson, Falzon, Homma, Ezeokoli and Davidson2014; Xie et al., Reference Xie, Huang, Lou, Fu, Ni, Hong and Ruan2022), none of these reviews have examined the potential dose-dependent effects of vitamin D supplementation on depressive symptoms to determine the optimum dose of intervention. Some of the available reviews, owing to the limited number of trials and methodological biases, were of low quality (Anglin et al., Reference Anglin, Samaan, Walter and McDonald2013; Cheng et al., Reference Cheng, Huang and Huang2020; Li et al., Reference Li, Mbuagbaw, Samaan, Falavigna, Zhang, Adachi and Thabane2014; Shaffer et al., Reference Shaffer, Edmondson, Wasson, Falzon, Homma, Ezeokoli and Davidson2014). Considering these uncertainties, we aimed to fill this gap by conducting a systematic review and dose–response meta-analysis of randomized control trials (RCTs) to determine the optimum dose and shape of the effects of vitamin D supplementation on depression and anxiety symptoms in adults regardless of their health status.
Methods
We conducted the meta-analysis per instructions outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement for Systematic Reviews of Interventions (Page et al., Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann, Mulrow and Brennan2021) and the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) Handbook (Schunemann, Reference Schunemann2008). The review protocol was registered with PROSPERO (CRD42022309640).
Data sources and searches
PubMed, Scopus, and Web of Science were systematically searched to find relevant literature up to 15 December 2022. Only English-language articles were included. Two investigators (SG and SZM) independently performed the systematic search and screened the titles and abstracts and then full-text articles to find eligible studies. Disagreements were resolved under the supervision of a third reviewer (SS-B). We also checked out the reference lists of published meta-analyses of RCTs of the effect of vitamin D supplementation. Further details about the search strategy in the databases are represented in online Supplementary Table 1.
Study selection
Inclusion and exclusion criteria were defined according to the framework of PICOS (population, intervention/exposure, comparator, outcome, and study design). Published human intervention studies were considered eligible for inclusion in the present meta-analysis if they had the following criteria: (1) RCTs, with a minimum intervention period of 4 weeks, conducted in adults aged 18 years or older, regardless of medication use and their health status; (2) evaluated the effects of vitamin D supplementation alone, regardless of type (vitamin D3, vitamin D2), method of advice (orally, injection), and dosing regimen against a control group; (3) provided a dose of vitamin D supplementation in the intervention group; and (4) provided effect estimates in the form of mean difference and its 95% confidence interval (CI) for continuous outcomes and odds ratio (OR) with its 95% CI for binary outcome, or reported sufficient information to estimate those measures. Eligible control group included usual diet, no advice, no intervention, or placebo. Trials that compared two doses of vitamin D supplementation in intervention and control arms were eligible. Except trials that used vitamin D incombinaton with calcium, others that implemented a multicomponent intervention including vitamin D in combination with another supplement (for example, omega-3) were excluded from our review.
Outcomes
Our primary outcomes were (1) the anxiety and depressive symptoms and (2) remission of depression. Moreover, our secondary outcomes included quality of life and its domains and total and serious adverse events.
Data extraction
The full texts of potentially eligible trials were examined separately by two investigators (SG and SZM). From studies considered eligible, the same two reviewers independently extracted the following characteristics from each trial: author and year of publication; population location, study design, and duration, characteristics of the population (% female, mean age ± s.d., baseline body mass index, and health status), total sample size, intervention characteristics (dose of vitamin D supplementation in the intervention group), comparison group, vitamin D deficiency (yes/no/mixed), use of antidepressant medication (yes/no/mixed), dropout, baseline depression risk, outcome measures and main results for the outcomes included.
Risk of bias assessment
Version 2.0 of the Cochrane tool was used to assess the risk of bias of the eligible RCTs (Higgins et al., Reference Higgins, Altman, Gøtzsche, Jüni, Moher, Oxman and Sterne2011). Two authors (SG and SZM) independently performed risk of bias assessment. Disagreements were resolved by discussion with a third reviewer (SS-B).
Data synthesis and analysis
We considered standardized mean difference (SMD) and its 95%CI for continuous outcomes (anxiety and depressive symptoms, comorbidity index, stress, overall quality of life, bodily image, dysphoria, food avoidance, healthy worry, relationship, sexual and social reaction) and OR and risk difference (RD) for binary outcomes (depression remission, adverse events, as well as serious adverse event) to report the results. For the analyses of continuous outcomes, we first computed the mean and s.d. of changes from baseline measures for each study arm in each trial. For the studies that did not report these changes, we estimated these values using the reported means and SDs of outcomes before and after the intervention per instructions in the Cochrane Handbook (Chandler, Cumpston, Li, Page, & Welch, Reference Chandler, Cumpston, Li, Page and Welch2019). We converted trial data to s.d. if they reported standard errors rather than s.d.. (Higgins & Green, Reference Higgins and Green2008). If neither s.d. nor standard error were reported in the trials, we used the average s.d. obtained from other trials for the analyses (Furukawa, Barbui, Cipriani, Brambilla, & Watanabe, Reference Furukawa, Barbui, Cipriani, Brambilla and Watanabe2006). Second, we calculated SMD and its 95%CI for each 1000 IU/day vitamin D3 supplementation in each trial using the method introduced by Crippa and Orsini (Crippa & Orsini, Reference Crippa and Orsini2016). Trial-specific results were pooled using a random-effect model (DerSimonian & Laird, Reference DerSimonian and Laird1986). The following items were needed for this method: the dose of vitamin D3 supplementation in the intervention and control arms, the mean and its related s.d. of change in outcomes in each study arm (treatment and control groups), and the total number of participants in each group. For trials that implemented vitamin D supplementation on a weekly or monthly basis (e.g. 30 000 IU per week or 50 000 IU per month), we converted the dosing regimen to IU per day. Finally, we conducted a dose–response meta-analysis to evaluate the shape of the dose-dependent effects of vitamin D3 supplementation on depressive and anxiety symptoms outcomes (Crippa & Orsini, Reference Crippa and Orsini2016).
Then we performed pre-specified subgroup analyses based on the risk of bias (low/some concerns/high), intervention duration (⩽8, 9–24, 24–52, >52 weeks), sex (both/men/women), weight status (normal weight, obese/overweight, not reported), vitamin D deficiency (yes/no/mixed), health status, medication use (yes/no/mixed), and baseline risk of depression (low/medium/high). According to eight criteria determined by the Instrument to assess the Credibility of Effect Modification Analyses (ICEMAN), we examined the credibility of subgroup differences (Schandelmaier et al., Reference Schandelmaier, Briel, Varadhan, Schmid, Devasenapathy, Hayward and Guyatt2020). We used meta-regression analyses to compute the p-values for subgroup differences. For publication bias, we applied Egger's test (Egger, Davey Smith, Schneider, & Minder, Reference Egger, Davey Smith, Schneider and Minder1997) and Begg's test (Begg & Mazumdar, Reference Begg and Mazumdar1994) and inspected the funnel plots for asymmetry. The heterogeneity of effects among studies was quantified using the I 2 statistic and χ2 test (Pheterogeneity > 0.10) (Higgins, Savovic, Page, Elbers, & Sterne, Reference Higgins, Savovic, Page, Elbers and Sterne2019).
For the analyses of binary outcomes (adverse event, depression remission), we calculated OR, RD, and their 95%CI using the number of participants and events in the intervention and control groups. Moreover, for depression remission judgment, every study defined specific criteria for recognition. For instance, in our review, only one study considered depression remission (Marsh, Penny, & Rothschild, Reference Marsh, Penny and Rothschild2017) and defined it as when participants had Montgomery-Åsberg Depression Rating Scale (MADRS) score was 12 or less. We used STATA software version 17.0 for our analyses. A two-tailed p-value less than 0.05 was regarded as statistically significant.
Grading the evidence
The GRADE approach was applied to judge the certainty of the evidence (Guyatt et al., Reference Guyatt, Oxman, Kunz, Brozek, Alonso-Coello, Rind and Schünemann2011). According to the GRADE, evidence obtained from RCTs starts at high certainty that can be downgraded or upgraded based on pre-defined criteria. Detailed criteria that were applied for use the GRADE tool are described in online Supplementary Table 2. In order to interpretation of the magnitude of effect sizes, the estimated SMDs were interpreted as a trivial effect (0.0–0.2), a small effect (0.2–0.6), a moderate effect (0.6–1.2), a large effect (1.2–2.0), a very large effect (2.0–4.0), and an extremely large effect (⩾4.0) (Hopkins, Marshall, Batterham, & Hanin, Reference Hopkins, Marshall, Batterham and Hanin2009; Varangot-Reille, Suso-Martí, Romero-Palau, Suárez-Pastor, & Cuenca-Martínez, Reference Varangot-Reille, Suso-Martí, Romero-Palau, Suárez-Pastor and Cuenca-Martínez2022).
Results
Systematic search
The literature search yielded 2243 records, with 1 additional record identified through manual search. After excluding 607 duplicates and 1582 irrelevant records, 55 full texts were reviewed in detail for eligibility. After reviewing the full texts, 31 trials were eligible for inclusion in this dose–response meta-analysis (Alavi, Khademalhoseini, Vakili, & Assarian, Reference Alavi, Khademalhoseini, Vakili and Assarian2019; Alghamdi et al., Reference Alghamdi, Alsulami, Khoja, Alsufiani, Tayeb and Tarazi2020; Bertone-Johnson et al., Reference Bertone-Johnson, Powers, Spangler, Larson, Michael, Millen and Manson2012; Choukri, Conner, Haszard, Harper, & Houghton, Reference Choukri, Conner, Haszard, Harper and Houghton2018; de Koning et al., Reference de Koning, Lips, Penninx, Elders, Heijboer, den Heijer and van Schoor2019; Dean et al., Reference Dean, Bellgrove, Hall, Phan, Eyles, Kvaskoff and McGrath2011; Eid et al., Reference Eid, Khoja, AlGhamdi, Alsufiani, Alzeben, Alhejaili and Tarazi2019; Fazelian, Amani, Paknahad, Kheiri, & Khajehali, Reference Fazelian, Amani, Paknahad, Kheiri and Khajehali2019; Frandsen, Pareek, Hansen, & Nielsen, Reference Frandsen, Pareek, Hansen and Nielsen2014; Gaughran et al., Reference Gaughran, Stringer, Wojewodka, Landau, Smith, Gardner-Sood and McGrath2021; Ghaderi et al., Reference Ghaderi, Banafshe, Motmaen, Rasouli-Azad, Bahmani and Asemi2017, Reference Ghaderi, Rasouli-Azad, Farhadi, Mirhosseini, Motmaen, Pishyareh and Asemi2020; Hansen et al., Reference Hansen, Pareek, Hvolby, Schmedes, Toft, Dahl and Nielsen2019; Jorde & Kubiak, Reference Jorde and Kubiak2018; Jorde, Sneve, Figenschau, Svartberg, & Waterloo, Reference Jorde, Sneve, Figenschau, Svartberg and Waterloo2008; Kaviani, Nikooyeh, Zand, Yaghmaei, & Neyestani, Reference Kaviani, Nikooyeh, Zand, Yaghmaei and Neyestani2020; Khalighi Sikaroudi et al., Reference Khalighi Sikaroudi, Mokhtare, Shidfar, Janani, Faghihi Kashani, Masoodi and Shidfar2020; Krivoy et al., Reference Krivoy, Onn, Vilner, Hochman, Weizman, Paz and Weizman2017; Kusmiyati, Suryani, Herawati, & Firdausi, Reference Kusmiyati, Suryani, Herawati and Firdausi2020; Marsh et al., Reference Marsh, Penny and Rothschild2017; Okereke et al., Reference Okereke, Reynolds, Mischoulon, Chang, Vyas, Cook and Manson2020; Omidian et al., Reference Omidian, Mahmoudi, Abshirini, Eshraghian, Javanbakht, Zarei and Djalali2019; Rolf et al., Reference Rolf, Muris, Bol, Damoiseaux, Smolders and Hupperts2017; Sepehrmanesh et al., Reference Sepehrmanesh, Kolahdooz, Abedi, Mazroii, Assarian, Asemi and Esmaillzadeh2016; Sharifi, Vahedi, Nedjat, Mohamadkhani, & Hosseinzadeh Attar, Reference Sharifi, Vahedi, Nedjat, Mohamadkhani and Hosseinzadeh Attar2019; Vellekkatt, Menon, Rajappa, & Sahoo, Reference Vellekkatt, Menon, Rajappa and Sahoo2020; Vieth, Kimball, Hu, & Walfish, Reference Vieth, Kimball, Hu and Walfish2004; Wang et al., Reference Wang, Liu, Lian, Li, Liu and Li2016; L. Zhang, Wang, Zhu, & Yang, Reference Zhang, Wang, Zhu and Yang2018; Zheng et al., Reference Zheng, Tu, Cicuttini, Han, Zhu, Antony and Ding2019; Zhu et al., Reference Zhu, Zhang, Wang, Lin, Yu, Xia and Zhu2020) (online Supplementary Figure 1). The list of studies excluded through full-text evaluation with reasons is reported in online Supplementary Table 3.
Characteristics of original articles
Characteristics of 31 trials included in the present dose–response meta-analysis are presented in online Supplementary Table 4. The included trials comprised 24 189 participants, of which, 12 091 subjects were in the control arm and 12 098 subjects were in the intervention arm. Twenty-nine trials used vitamin D3 supplement as an intervention. In one of the RCTs, vitamin D supplementation was performed in combination with calcium (Bertone-Johnson et al., Reference Bertone-Johnson, Powers, Spangler, Larson, Michael, Millen and Manson2012). In another one of the RCTs, vitamin D supplementation was combined with omega-3 supplementation (Okereke et al., Reference Okereke, Reynolds, Mischoulon, Chang, Vyas, Cook and Manson2020). The intervention duration ranged from 4 to 256.8 weeks, of which, 8 trials lasted ⩽8 weeks (Alavi et al., Reference Alavi, Khademalhoseini, Vakili and Assarian2019; Choukri et al., Reference Choukri, Conner, Haszard, Harper and Houghton2018; Dean et al., Reference Dean, Bellgrove, Hall, Phan, Eyles, Kvaskoff and McGrath2011; Kaviani et al., Reference Kaviani, Nikooyeh, Zand, Yaghmaei and Neyestani2020; Krivoy et al., Reference Krivoy, Onn, Vilner, Hochman, Weizman, Paz and Weizman2017; Kusmiyati et al., Reference Kusmiyati, Suryani, Herawati and Firdausi2020; Sepehrmanesh et al., Reference Sepehrmanesh, Kolahdooz, Abedi, Mazroii, Assarian, Asemi and Esmaillzadeh2016; Zhang et al., Reference Zhang, Wang, Zhu and Yang2018), fifteen trials lasted >8 to ⩽24 weeks (Alghamdi et al., Reference Alghamdi, Alsulami, Khoja, Alsufiani, Tayeb and Tarazi2020; Eid et al., Reference Eid, Khoja, AlGhamdi, Alsufiani, Alzeben, Alhejaili and Tarazi2019; Fazelian et al., Reference Fazelian, Amani, Paknahad, Kheiri and Khajehali2019; Frandsen et al., Reference Frandsen, Pareek, Hansen and Nielsen2014; Gaughran et al., Reference Gaughran, Stringer, Wojewodka, Landau, Smith, Gardner-Sood and McGrath2021; Ghaderi et al., Reference Ghaderi, Banafshe, Motmaen, Rasouli-Azad, Bahmani and Asemi2017, Reference Ghaderi, Rasouli-Azad, Farhadi, Mirhosseini, Motmaen, Pishyareh and Asemi2020; Hansen et al., Reference Hansen, Pareek, Hvolby, Schmedes, Toft, Dahl and Nielsen2019; Jorde & Kubiak, Reference Jorde and Kubiak2018; Khalighi Sikaroudi et al., Reference Khalighi Sikaroudi, Mokhtare, Shidfar, Janani, Faghihi Kashani, Masoodi and Shidfar2020; Marsh et al., Reference Marsh, Penny and Rothschild2017; Omidian et al., Reference Omidian, Mahmoudi, Abshirini, Eshraghian, Javanbakht, Zarei and Djalali2019; Sharifi et al., Reference Sharifi, Vahedi, Nedjat, Mohamadkhani and Hosseinzadeh Attar2019; Vellekkatt et al., Reference Vellekkatt, Menon, Rajappa and Sahoo2020; Zhu et al., Reference Zhu, Zhang, Wang, Lin, Yu, Xia and Zhu2020), five trials lasted lasted >24 to ⩽52 weeks (de Koning et al., Reference de Koning, Lips, Penninx, Elders, Heijboer, den Heijer and van Schoor2019; Jorde et al., Reference Jorde, Sneve, Figenschau, Svartberg and Waterloo2008; Rolf et al., Reference Rolf, Muris, Bol, Damoiseaux, Smolders and Hupperts2017; Vieth et al., Reference Vieth, Kimball, Hu and Walfish2004; Wang et al., Reference Wang, Liu, Lian, Li, Liu and Li2016), and three trials lasted >52 weeks (Bertone-Johnson et al., Reference Bertone-Johnson, Powers, Spangler, Larson, Michael, Millen and Manson2012; Okereke et al., Reference Okereke, Reynolds, Mischoulon, Chang, Vyas, Cook and Manson2020; Zheng et al., Reference Zheng, Tu, Cicuttini, Han, Zhu, Antony and Ding2019). Fifteen trials were conducted in patients with depression (Alavi et al., Reference Alavi, Khademalhoseini, Vakili and Assarian2019; Alghamdi et al., Reference Alghamdi, Alsulami, Khoja, Alsufiani, Tayeb and Tarazi2020; Bertone-Johnson et al., Reference Bertone-Johnson, Powers, Spangler, Larson, Michael, Millen and Manson2012; Frandsen et al., Reference Frandsen, Pareek, Hansen and Nielsen2014; Gaughran et al., Reference Gaughran, Stringer, Wojewodka, Landau, Smith, Gardner-Sood and McGrath2021; Ghaderi et al., Reference Ghaderi, Banafshe, Motmaen, Rasouli-Azad, Bahmani and Asemi2017, Reference Ghaderi, Rasouli-Azad, Farhadi, Mirhosseini, Motmaen, Pishyareh and Asemi2020; Hansen et al., Reference Hansen, Pareek, Hvolby, Schmedes, Toft, Dahl and Nielsen2019; Jorde et al., Reference Jorde, Sneve, Figenschau, Svartberg and Waterloo2008; Kaviani et al., Reference Kaviani, Nikooyeh, Zand, Yaghmaei and Neyestani2020; Omidian et al., Reference Omidian, Mahmoudi, Abshirini, Eshraghian, Javanbakht, Zarei and Djalali2019; Sepehrmanesh et al., Reference Sepehrmanesh, Kolahdooz, Abedi, Mazroii, Assarian, Asemi and Esmaillzadeh2016; Vellekkatt et al., Reference Vellekkatt, Menon, Rajappa and Sahoo2020; Wang et al., Reference Wang, Liu, Lian, Li, Liu and Li2016; Zhang et al., Reference Zhang, Wang, Zhu and Yang2018), six trials were carried out on healthy subjects (Choukri et al., Reference Choukri, Conner, Haszard, Harper and Houghton2018; de Koning et al., Reference de Koning, Lips, Penninx, Elders, Heijboer, den Heijer and van Schoor2019; Dean et al., Reference Dean, Bellgrove, Hall, Phan, Eyles, Kvaskoff and McGrath2011; Jorde & Kubiak, Reference Jorde and Kubiak2018; Kusmiyati et al., Reference Kusmiyati, Suryani, Herawati and Firdausi2020; Okereke et al., Reference Okereke, Reynolds, Mischoulon, Chang, Vyas, Cook and Manson2020), two studies were carried out on subjects with anxiety (Eid et al., Reference Eid, Khoja, AlGhamdi, Alsufiani, Alzeben, Alhejaili and Tarazi2019; Fazelian et al., Reference Fazelian, Amani, Paknahad, Kheiri and Khajehali2019), and other trials were carried out in patients with chronic diseases including schizophrenia (Krivoy et al., Reference Krivoy, Onn, Vilner, Hochman, Weizman, Paz and Weizman2017), bipolar disorder (Marsh et al., Reference Marsh, Penny and Rothschild2017), multiple sclerosis (Rolf et al., Reference Rolf, Muris, Bol, Damoiseaux, Smolders and Hupperts2017), ulcerative colitis (Sharifi et al., Reference Sharifi, Vahedi, Nedjat, Mohamadkhani and Hosseinzadeh Attar2019), and irritable bowel syndrome (Khalighi Sikaroudi et al., Reference Khalighi Sikaroudi, Mokhtare, Shidfar, Janani, Faghihi Kashani, Masoodi and Shidfar2020). Five of the 30 RCTs were carried out in individuals with normal weight (Choukri et al., Reference Choukri, Conner, Haszard, Harper and Houghton2018; Vellekkatt et al., Reference Vellekkatt, Menon, Rajappa and Sahoo2020; Wang et al., Reference Wang, Liu, Lian, Li, Liu and Li2016; Zheng et al., Reference Zheng, Tu, Cicuttini, Han, Zhu, Antony and Ding2019; Zhu et al., Reference Zhu, Zhang, Wang, Lin, Yu, Xia and Zhu2020), 15 were carried out in individuals with overweight or obesity (body mass index ⩾25 kg/m2) (Alghamdi et al., Reference Alghamdi, Alsulami, Khoja, Alsufiani, Tayeb and Tarazi2020; de Koning et al., Reference de Koning, Lips, Penninx, Elders, Heijboer, den Heijer and van Schoor2019; Fazelian et al., Reference Fazelian, Amani, Paknahad, Kheiri and Khajehali2019; Gaughran et al., Reference Gaughran, Stringer, Wojewodka, Landau, Smith, Gardner-Sood and McGrath2021; Ghaderi et al., Reference Ghaderi, Banafshe, Motmaen, Rasouli-Azad, Bahmani and Asemi2017, Reference Ghaderi, Rasouli-Azad, Farhadi, Mirhosseini, Motmaen, Pishyareh and Asemi2020; Jorde & Kubiak, Reference Jorde and Kubiak2018; Jorde et al., Reference Jorde, Sneve, Figenschau, Svartberg and Waterloo2008; Kaviani et al., Reference Kaviani, Nikooyeh, Zand, Yaghmaei and Neyestani2020; Khalighi Sikaroudi et al., Reference Khalighi Sikaroudi, Mokhtare, Shidfar, Janani, Faghihi Kashani, Masoodi and Shidfar2020; Krivoy et al., Reference Krivoy, Onn, Vilner, Hochman, Weizman, Paz and Weizman2017; Omidian et al., Reference Omidian, Mahmoudi, Abshirini, Eshraghian, Javanbakht, Zarei and Djalali2019; Sepehrmanesh et al., Reference Sepehrmanesh, Kolahdooz, Abedi, Mazroii, Assarian, Asemi and Esmaillzadeh2016; Sharifi et al., Reference Sharifi, Vahedi, Nedjat, Mohamadkhani and Hosseinzadeh Attar2019; Zheng et al., Reference Zheng, Tu, Cicuttini, Han, Zhu, Antony and Ding2019), and the remaining 11 studies did not report the participants' weight status (Alavi et al., Reference Alavi, Khademalhoseini, Vakili and Assarian2019; Bertone-Johnson et al., Reference Bertone-Johnson, Powers, Spangler, Larson, Michael, Millen and Manson2012; Dean et al., Reference Dean, Bellgrove, Hall, Phan, Eyles, Kvaskoff and McGrath2011; Eid et al., Reference Eid, Khoja, AlGhamdi, Alsufiani, Alzeben, Alhejaili and Tarazi2019; Frandsen et al., Reference Frandsen, Pareek, Hansen and Nielsen2014; Hansen et al., Reference Hansen, Pareek, Hvolby, Schmedes, Toft, Dahl and Nielsen2019; Kusmiyati et al., Reference Kusmiyati, Suryani, Herawati and Firdausi2020; Marsh et al., Reference Marsh, Penny and Rothschild2017; Okereke et al., Reference Okereke, Reynolds, Mischoulon, Chang, Vyas, Cook and Manson2020; Rolf et al., Reference Rolf, Muris, Bol, Damoiseaux, Smolders and Hupperts2017; Vieth et al., Reference Vieth, Kimball, Hu and Walfish2004). Participants in the 17 trials had vitamin D deficiency (Alavi et al., Reference Alavi, Khademalhoseini, Vakili and Assarian2019; de Koning et al., Reference de Koning, Lips, Penninx, Elders, Heijboer, den Heijer and van Schoor2019; Eid et al., Reference Eid, Khoja, AlGhamdi, Alsufiani, Alzeben, Alhejaili and Tarazi2019; Fazelian et al., Reference Fazelian, Amani, Paknahad, Kheiri and Khajehali2019; Ghaderi et al., Reference Ghaderi, Banafshe, Motmaen, Rasouli-Azad, Bahmani and Asemi2017, Reference Ghaderi, Rasouli-Azad, Farhadi, Mirhosseini, Motmaen, Pishyareh and Asemi2020; Khalighi Sikaroudi et al., Reference Khalighi Sikaroudi, Mokhtare, Shidfar, Janani, Faghihi Kashani, Masoodi and Shidfar2020; Krivoy et al., Reference Krivoy, Onn, Vilner, Hochman, Weizman, Paz and Weizman2017; Marsh et al., Reference Marsh, Penny and Rothschild2017; Omidian et al., Reference Omidian, Mahmoudi, Abshirini, Eshraghian, Javanbakht, Zarei and Djalali2019; Rolf et al., Reference Rolf, Muris, Bol, Damoiseaux, Smolders and Hupperts2017; Sepehrmanesh et al., Reference Sepehrmanesh, Kolahdooz, Abedi, Mazroii, Assarian, Asemi and Esmaillzadeh2016; Vellekkatt et al., Reference Vellekkatt, Menon, Rajappa and Sahoo2020; Wang et al., Reference Wang, Liu, Lian, Li, Liu and Li2016; Zhang et al., Reference Zhang, Wang, Zhu and Yang2018; Zheng et al., Reference Zheng, Tu, Cicuttini, Han, Zhu, Antony and Ding2019; Zhu et al., Reference Zhu, Zhang, Wang, Lin, Yu, Xia and Zhu2020), six trials were conducted in those without vitamin D deficiency (Choukri et al., Reference Choukri, Conner, Haszard, Harper and Houghton2018; Dean et al., Reference Dean, Bellgrove, Hall, Phan, Eyles, Kvaskoff and McGrath2011; Frandsen et al., Reference Frandsen, Pareek, Hansen and Nielsen2014; Jorde & Kubiak, Reference Jorde and Kubiak2018; Rolf et al., Reference Rolf, Muris, Bol, Damoiseaux, Smolders and Hupperts2017; Vieth et al., Reference Vieth, Kimball, Hu and Walfish2004), while the other eight trials were conducted in individuals with mixed vitamin D status (Alghamdi et al., Reference Alghamdi, Alsulami, Khoja, Alsufiani, Tayeb and Tarazi2020; Gaughran et al., Reference Gaughran, Stringer, Wojewodka, Landau, Smith, Gardner-Sood and McGrath2021; Hansen et al., Reference Hansen, Pareek, Hvolby, Schmedes, Toft, Dahl and Nielsen2019; Jorde et al., Reference Jorde, Sneve, Figenschau, Svartberg and Waterloo2008; Kaviani et al., Reference Kaviani, Nikooyeh, Zand, Yaghmaei and Neyestani2020; Kusmiyati et al., Reference Kusmiyati, Suryani, Herawati and Firdausi2020; Okereke et al., Reference Okereke, Reynolds, Mischoulon, Chang, Vyas, Cook and Manson2020; Sharifi et al., Reference Sharifi, Vahedi, Nedjat, Mohamadkhani and Hosseinzadeh Attar2019). Five trials were rated as low risk of bias (Dean et al., Reference Dean, Bellgrove, Hall, Phan, Eyles, Kvaskoff and McGrath2011; Frandsen et al., Reference Frandsen, Pareek, Hansen and Nielsen2014; Gaughran et al., Reference Gaughran, Stringer, Wojewodka, Landau, Smith, Gardner-Sood and McGrath2021; Hansen et al., Reference Hansen, Pareek, Hvolby, Schmedes, Toft, Dahl and Nielsen2019; Vellekkatt et al., Reference Vellekkatt, Menon, Rajappa and Sahoo2020), twelve trials were rated to have some concerns (Choukri et al., Reference Choukri, Conner, Haszard, Harper and Houghton2018; de Koning et al., Reference de Koning, Lips, Penninx, Elders, Heijboer, den Heijer and van Schoor2019; Fazelian et al., Reference Fazelian, Amani, Paknahad, Kheiri and Khajehali2019; Ghaderi et al., Reference Ghaderi, Banafshe, Motmaen, Rasouli-Azad, Bahmani and Asemi2017, Reference Ghaderi, Rasouli-Azad, Farhadi, Mirhosseini, Motmaen, Pishyareh and Asemi2020; Jorde et al., Reference Jorde, Sneve, Figenschau, Svartberg and Waterloo2008; Krivoy et al., Reference Krivoy, Onn, Vilner, Hochman, Weizman, Paz and Weizman2017; Okereke et al., Reference Okereke, Reynolds, Mischoulon, Chang, Vyas, Cook and Manson2020; Omidian et al., Reference Omidian, Mahmoudi, Abshirini, Eshraghian, Javanbakht, Zarei and Djalali2019; Vieth et al., Reference Vieth, Kimball, Hu and Walfish2004; Wang et al., Reference Wang, Liu, Lian, Li, Liu and Li2016; L. Zhang et al., Reference Zhang, Wang, Zhu and Yang2018), and the other 14 trials were rated to have a high risk of bias (Alavi et al., Reference Alavi, Khademalhoseini, Vakili and Assarian2019; Alghamdi et al., Reference Alghamdi, Alsulami, Khoja, Alsufiani, Tayeb and Tarazi2020; Bertone-Johnson et al., Reference Bertone-Johnson, Powers, Spangler, Larson, Michael, Millen and Manson2012; Eid et al., Reference Eid, Khoja, AlGhamdi, Alsufiani, Alzeben, Alhejaili and Tarazi2019; Jorde & Kubiak, Reference Jorde and Kubiak2018; Kaviani et al., Reference Kaviani, Nikooyeh, Zand, Yaghmaei and Neyestani2020; Khalighi Sikaroudi et al., Reference Khalighi Sikaroudi, Mokhtare, Shidfar, Janani, Faghihi Kashani, Masoodi and Shidfar2020; Kusmiyati et al., Reference Kusmiyati, Suryani, Herawati and Firdausi2020; Marsh et al., Reference Marsh, Penny and Rothschild2017; Rolf et al., Reference Rolf, Muris, Bol, Damoiseaux, Smolders and Hupperts2017; Sepehrmanesh et al., Reference Sepehrmanesh, Kolahdooz, Abedi, Mazroii, Assarian, Asemi and Esmaillzadeh2016; Sharifi et al., Reference Sharifi, Vahedi, Nedjat, Mohamadkhani and Hosseinzadeh Attar2019; Zheng et al., Reference Zheng, Tu, Cicuttini, Han, Zhu, Antony and Ding2019; Zhu et al., Reference Zhu, Zhang, Wang, Lin, Yu, Xia and Zhu2020) (online Supplementary Table 5).
Primary outcomes
A total of 31 trials with 12 098 participants in the intervention group and 12 091 participants in the control group provided data on the effect of vitamin D3 supplementation on the depressive symptoms (Alavi et al., Reference Alavi, Khademalhoseini, Vakili and Assarian2019; Alghamdi et al., Reference Alghamdi, Alsulami, Khoja, Alsufiani, Tayeb and Tarazi2020; Bertone-Johnson et al., Reference Bertone-Johnson, Powers, Spangler, Larson, Michael, Millen and Manson2012; Choukri et al., Reference Choukri, Conner, Haszard, Harper and Houghton2018; de Koning et al., Reference de Koning, Lips, Penninx, Elders, Heijboer, den Heijer and van Schoor2019; Dean et al., Reference Dean, Bellgrove, Hall, Phan, Eyles, Kvaskoff and McGrath2011; Eid et al., Reference Eid, Khoja, AlGhamdi, Alsufiani, Alzeben, Alhejaili and Tarazi2019; Fazelian et al., Reference Fazelian, Amani, Paknahad, Kheiri and Khajehali2019; Frandsen et al., Reference Frandsen, Pareek, Hansen and Nielsen2014; Gaughran et al., Reference Gaughran, Stringer, Wojewodka, Landau, Smith, Gardner-Sood and McGrath2021; Ghaderi et al., Reference Ghaderi, Banafshe, Motmaen, Rasouli-Azad, Bahmani and Asemi2017, Reference Ghaderi, Rasouli-Azad, Farhadi, Mirhosseini, Motmaen, Pishyareh and Asemi2020; Hansen et al., Reference Hansen, Pareek, Hvolby, Schmedes, Toft, Dahl and Nielsen2019; Jorde & Kubiak, Reference Jorde and Kubiak2018; Jorde et al., Reference Jorde, Sneve, Figenschau, Svartberg and Waterloo2008; Kaviani et al., Reference Kaviani, Nikooyeh, Zand, Yaghmaei and Neyestani2020; Khalighi Sikaroudi et al., Reference Khalighi Sikaroudi, Mokhtare, Shidfar, Janani, Faghihi Kashani, Masoodi and Shidfar2020; Krivoy et al., Reference Krivoy, Onn, Vilner, Hochman, Weizman, Paz and Weizman2017; Kusmiyati et al., Reference Kusmiyati, Suryani, Herawati and Firdausi2020; Marsh et al., Reference Marsh, Penny and Rothschild2017; Okereke et al., Reference Okereke, Reynolds, Mischoulon, Chang, Vyas, Cook and Manson2020; Omidian et al., Reference Omidian, Mahmoudi, Abshirini, Eshraghian, Javanbakht, Zarei and Djalali2019; Rolf et al., Reference Rolf, Muris, Bol, Damoiseaux, Smolders and Hupperts2017; Sepehrmanesh et al., Reference Sepehrmanesh, Kolahdooz, Abedi, Mazroii, Assarian, Asemi and Esmaillzadeh2016; Sharifi et al., Reference Sharifi, Vahedi, Nedjat, Mohamadkhani and Hosseinzadeh Attar2019; Vellekkatt et al., Reference Vellekkatt, Menon, Rajappa and Sahoo2020; Vieth et al., Reference Vieth, Kimball, Hu and Walfish2004; Wang et al., Reference Wang, Liu, Lian, Li, Liu and Li2016; Zhang et al., Reference Zhang, Wang, Zhu and Yang2018; Zheng et al., Reference Zheng, Tu, Cicuttini, Han, Zhu, Antony and Ding2019; Zhu et al., Reference Zhu, Zhang, Wang, Lin, Yu, Xia and Zhu2020). Every 1000 IU/day vitamin D3 supplementation slightly reduced depressive symptoms (SMD: −0.32; 95% CI −0.43 to −0.22; I 2 = 98%; Pheterogeneity < 0.001, GEADE = moderate) (online Supplementary Figure 2). Of note, vitamin D supplementation resulted in a larger improvement in depressive symptoms in those with a history of depression (SMD: −0.57, 95% CI −0.69 to −0.44; n = 15 trials) (×Table 1).
Table 1. Subgroup analyses of the effects of vitamin D3 supplement (each 1000 IU/d) on depressive symptoms
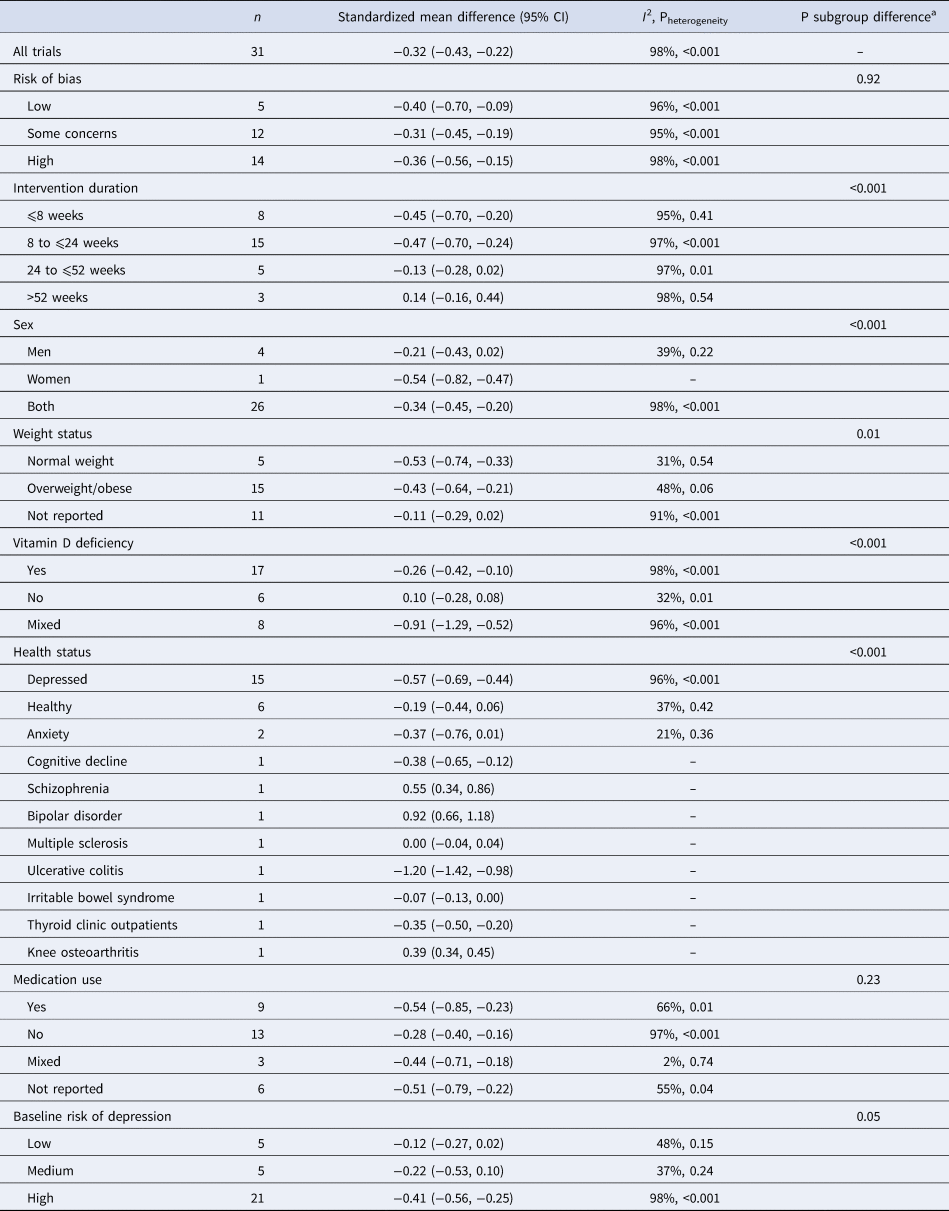
a Obtained by meta-regression analysis.
Table 1 presents the subgroup analysis of the effects of vitamin D3 supplementation (each 1000 IU/day) on depressive symptoms. There were several potential effect modifications by intervention duration, sex, weight status, vitamin D status, and health status. However, the credibility of these subgroup differences was rated low (online Supplementary Table 6). For instance, we found a stronger effect in trials with an intervention duration of ⩽8 weeks and 8 to ⩽24 weeks, and a nonsignificant effect in trials longer than 24 weeks (p group difference <0.001); however, only a few trials were available with follow-up longer than 52 weeks (Table 1). By using Egger's test (p = 0.23), Begg's test (p = 0.16), and an inspection of the funnel plot, we did not detect any evidence of publication bias (online Supplementary Figure 3).
The effects of different doses of vitamin D3 on depressive symptoms are shown in Table 2 and Fig. 1. The analysis showed that depression symptoms decreased proportionally with increase in the dosage of vitamin D3 supplementation up to 8000 IU/day (SMD8000 IU/d: −2.04; 95% CI −3.77 to −0.31), with no further change in effect estimate at higher doses (Pdose−response < 0.001, Pnonlinearity = 0.208; n = 31, Fig. 1 and Table 2).
Table 2. The effects of vitamin D3 on depressive symptoms from the nonlinear dose–response meta-analysis (standardized mean difference and 95% confidence interval)

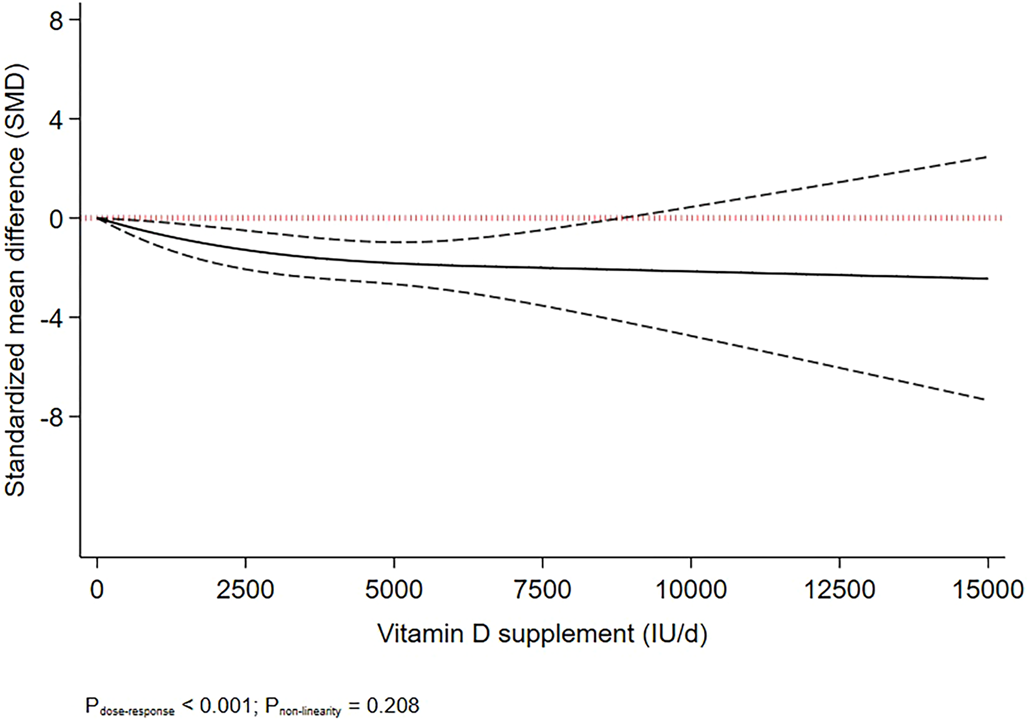
Figure 1. Dose-dependent effect of vitamin D supplement on depressive symptoms. Solid lines represent standardised mean difference and dashed lines represent 95% CI.
One study reported the effect of vitamin D3 supplementation on the odds of depression remission (Marsh et al., Reference Marsh, Penny and Rothschild2017). Vitamin D3 supplementation had no significant effect on depression remission (online Supplementary Figure 4 and Table 3).
A total of seven trials with 332 individuals in the intervention group and 309 individuals in the control group provided data on the effect of vitamin D3 supplementation on the severity of anxiety (Choukri et al., Reference Choukri, Conner, Haszard, Harper and Houghton2018; Dean et al., Reference Dean, Bellgrove, Hall, Phan, Eyles, Kvaskoff and McGrath2011; Fazelian et al., Reference Fazelian, Amani, Paknahad, Kheiri and Khajehali2019; Ghaderi et al., Reference Ghaderi, Banafshe, Motmaen, Rasouli-Azad, Bahmani and Asemi2017, Reference Ghaderi, Rasouli-Azad, Farhadi, Mirhosseini, Motmaen, Pishyareh and Asemi2020; Khalighi Sikaroudi et al., Reference Khalighi Sikaroudi, Mokhtare, Shidfar, Janani, Faghihi Kashani, Masoodi and Shidfar2020; Zhu et al., Reference Zhu, Zhang, Wang, Lin, Yu, Xia and Zhu2020). Our analysis showed that every 1000 IU/day of vitamin D3 did not significantly reduce the severity of anxiety (online Supplementary Figure 6 and Table 3).
Secondary outcomes
The effect of vitamin D3 supplementation on secondary outcomes is demonstrated in online Supplementary Figure (7–20) and Table (3).<TE: Please check this is supplementary table citation or actual table ciation?. Opening bracket missing here.> Vitamin D3 supplementation had no effects on secondary outcomes including adverse events and different aspects of quality of life.
Grading of the evidence
The GRADE evidence rating for primary and secondary outcomes is presented in online Supplementary Table 8. The certainty of the evidence was rated moderate for the effects of vitamin D3 supplementation on depressive symptoms due to a downgrade for inconsistency and an upgrade for the dose–response gradient. The certainty of evidence was rated very low to low for other outcomes (×Table 3). Of note, the effects of vitamin D3 supplementation on depressive symptoms surpassed the threshold set as large effect size (SMD: −1.2 to −2) in the nonlinear dose–response meta-analysis, suggesting that supplementation with vitamin D3 at a dose of 8000 IU/day could lead to a large improvement in depressive symptoms.
Table 3. The effect of vitamin D3 supplementation (per 1000 IU/day) on primary and secondary outcomes

Discussion
To our knowledge, this is the first meta-analysis to investigate the dose-dependent effect of vitamin D supplementation on depression and anxiety symptoms in adults. Our results presented evidence of moderate certainty of the beneficial effects of vitamin D supplementation on depressive symptoms in adults. We did not find any significant effects of vitamin D supplementation on depression remission and anxiety symptoms. Vitamin D3 supplementation had no effects on quality of life.
Evidence from population-based epidemiological studies is consistent with the hypothesis that low serum vitamin D concentration is associated with a higher risk of depression (Anglin et al., Reference Anglin, Samaan, Walter and McDonald2013; Ju et al., Reference Ju, Lee and Jeong2013). Furthermore, our findings are consistent with existing evidence presented by meta-analysis of RCTs about the effects of vitamin D supplementation on depressive symptoms. A recent meta-analysis of 11 trials indicated that vitamin D3 supplementation improved the Beck Depression Inventory score in patients with psychiatric disorders (Jamilian et al., Reference Jamilian, Amirani, Milajerdi, Kolahdooz, Mirzaei, Zaroudi and Asemi2019). The results of another recent meta-analysis including 29 trials with 4504 participants indicated that the use of vitamin D3 may be beneficial to decrease the incidence of depression and improvement of depression symptoms (Xie et al., Reference Xie, Huang, Lou, Fu, Ni, Hong and Ruan2022). Moreover, another meta-analysis of four trials with 948 participants showed that vitamin D3 supplementation positively impacted depression rating in patients with major depression (Vellekkatt & Menon, Reference Vellekkatt and Menon2019). However, there is some conflicting evidence, suggesting that oral administration of vitamin D3 did not have a significant effect on the reduction of post-intervention depression score (Lázaro Tomé et al., Reference Lázaro Tomé, Reig Cebriá, González-Teruel, Carbonell-Asíns, Cañete Nicolás and Hernández-Viadel2021).
Although the beneficial effects of vitamin D supplementation on depressive symptoms have been ascertained in previous research, the optimum dose of supplementation for reducing depressive symptoms has not been determined in previous studies. Our primary findings indicated that every 1000 IU/day of vitamin D3 supplementation significantly reduced depressive symptoms. We found that depressive symptoms decreased proportionally with the increase of the dosage of intervention up to 8000 IU/day. We found the greatest impact at 8000 IU/day, and that higher doses had no added values for treatment of depressive symptoms.
Our subgroup analyses indicated a stronger effect on depressive symptoms in women than in men. This is consistent with the literature, which suggests that the relationship between vitamin D3 deficiency and depression risk was stronger in women than in men (Harse et al., Reference Harse, Zhu, Bucks, Hunter, Lim, Cooke and Murray2021; Landel, Annweiler, Millet, Morello, & Féron, Reference Landel, Annweiler, Millet, Morello and Féron2016; Lerchbaum, Reference Lerchbaum2014). There are physiological interactions between the effects of vitamin D and estrogen. Vitamin D deficiency may lead to lower estrogen levels, which can cause depression. This can make women more vulnerable to the effects of vitamin D deficiency (Harse et al., Reference Harse, Zhu, Bucks, Hunter, Lim, Cooke and Murray2021; Landel et al., Reference Landel, Annweiler, Millet, Morello and Féron2016; Lerchbaum, Reference Lerchbaum2014). However, there was only one trial in women, and the credibility of subgroup difference was rated low. Therefore, the potential sex difference in the effect of vitamin D3 supplementation on depressive symptoms should be interpreted with caution.
Our subgroup analyses also highlighted a significant subgroup difference by intervention duration, where trials with an intervention duration of ⩽8 weeks and 8 to ⩽24 weeks indicated a stronger effect than those with 24 to ⩽52 weeks. Of note, an increasing effect was seen among trials with an intervention duration of >52 weeks. Regarding the length of the intervention, ‘8 weeks’ was identified as the window of time that may start the vitamin D response, whether in the prevention or therapy of depression (Xie et al., Reference Xie, Huang, Lou, Fu, Ni, Hong and Ruan2022). The decline in the efficacy of vitamin D supplementation in reducing depressive symptoms can be explained by attrition bias, lower compliance, and higher dropout in trials with longer intervention durations.
There are several possible physiological mechanisms to explain why vitamin D3 supplementation is effective in treating depression. These mechanisms include its impacts on cellular signaling, neurotropic and immunomodulatory processes, serotonin synthesis, expression of mitochondrial proteins, increasing the expression of vitamin D3 receptors in important brain regions, and decreasing levels of C-reactive protein, as an inflammatory marker linked to depression (Geng et al., Reference Geng, Shaikh, Han, Chen, Guo and Jiang2019). Moreover, oxidative stress can be a contributing factor to depression. Vitamin D has important antioxidant properties and thus, may have therapeutic effects against depressive symptoms (Penckofer et al., Reference Penckofer, Ridosh, Adams, Grzesiak, Woo, Byrn and Halaris2022; Thurfah, Christine, Bagaskhara, Alfian, & Puspitasari, Reference Thurfah, Christine, Bagaskhara, Alfian and Puspitasari2022; Vellekkatt & Menon, Reference Vellekkatt and Menon2019). Vitamin D may also affect the serotonin system and maintain circadian rhythms, which are linked to depression (Casseb, Kaster, & Rodrigues, Reference Casseb, Kaster and Rodrigues2019; Ceolin, Mano, Hames, Antunes, & Moreira, Reference Ceolin, Mano, Hames, Antunes and Moreira2021).
Additionally, the possible benefits of vitamin D on physical health in the long term were as follows: Vitamin D supplementation has been shown to have long-lasting benefits such as reducing the risk of falls and fractures, as demonstrated in the ViDA trial (Khaw et al., Reference Khaw, Stewart, Waayer, Lawes, Toop, Camargo and Scragg2017). It has also been found to lower central blood pressure among vitamin D deficient participants (Sluyter et al., Reference Sluyter, Camargo, Stewart, Waayer, Lawes, Toop and Wassertheurer2017) and lower the risk of overall mortality (Chowdhury et al., Reference Chowdhury, Kunutsor, Vitezova, Oliver-Williams, Chowdhury, Kiefte-de-Jong and Hoshen2014).
Despite the aforementioned findings, we could not find a significant association between vitamin D3 supplementation and depression remission. Furthermore, we could not observe a significant relationship between vitamin D3 supplementation and the severity of anxiety. Nevertheless, some previous studies demonstrated that vitamin D supplementation was effective in alleviating anxiety symptoms (Borges-Vieira & Cardoso, Reference Borges-Vieira and Cardoso2023; Eid et al., Reference Eid, Khoja, AlGhamdi, Alsufiani, Alzeben, Alhejaili and Tarazi2019; Zaromytidou et al., Reference Zaromytidou, Koufakis, Dimakopoulos, Drivakou, Konstantinidou, Rakitzi and Kotsa2022). These controversies may be attributed to the low number of trials available in this field, design of the studies, initial serum 25(OH)D concentrations of the participants, dose and type of vitamin D supplement (D2 v. D3), intervention duration, method of supplementation and age of the target group.
There were several strengths to our study. Our study updated earlier findings by including more recent RCTs in this field (Alavi et al., Reference Alavi, Khademalhoseini, Vakili and Assarian2019; Alghamdi et al., Reference Alghamdi, Alsulami, Khoja, Alsufiani, Tayeb and Tarazi2020; de Koning et al., Reference de Koning, Lips, Penninx, Elders, Heijboer, den Heijer and van Schoor2019; Eid et al., Reference Eid, Khoja, AlGhamdi, Alsufiani, Alzeben, Alhejaili and Tarazi2019; Fazelian et al., Reference Fazelian, Amani, Paknahad, Kheiri and Khajehali2019; Gaughran et al., Reference Gaughran, Stringer, Wojewodka, Landau, Smith, Gardner-Sood and McGrath2021; Ghaderi et al., Reference Ghaderi, Rasouli-Azad, Farhadi, Mirhosseini, Motmaen, Pishyareh and Asemi2020; Hansen et al., Reference Hansen, Pareek, Hvolby, Schmedes, Toft, Dahl and Nielsen2019; Kaviani et al., Reference Kaviani, Nikooyeh, Zand, Yaghmaei and Neyestani2020; Kusmiyati et al., Reference Kusmiyati, Suryani, Herawati and Firdausi2020; Omidian et al., Reference Omidian, Mahmoudi, Abshirini, Eshraghian, Javanbakht, Zarei and Djalali2019; Sharifi et al., Reference Sharifi, Vahedi, Nedjat, Mohamadkhani and Hosseinzadeh Attar2019; Vellekkatt et al., Reference Vellekkatt, Menon, Rajappa and Sahoo2020; Zheng et al., Reference Zheng, Tu, Cicuttini, Han, Zhu, Antony and Ding2019; Zhu et al., Reference Zhu, Zhang, Wang, Lin, Yu, Xia and Zhu2020). Additionally, to the best of our knowledge, this is the first meta-analysis that investigated the dose-dependent effects of vitamin D3 supplementation on depression and anxiety symptoms in adults. We also applied the GRADE approach to rate the certainty of evidence. The Cochrane risk of bias tool (Version 2.0) was utilized to assess the methodological quality of included RCTs. Lastly, Pre-specified subgroup analyses were conducted based on various study characteristics, including risk of bias, intervention duration, sex, weight status, vitamin D deficiency, health status, medication use, and baseline risk of depression. This comprehensive approach enabled the exploration of potential effect modifiers.
However, there were also some limitations in the present meta-analysis. First, other factors may act as a moderator in the association between vitamin D supplementation and depressive symptoms. Although we did several subgroup analyses by participants and study characteristics, several unknown variables can affect the results. Second, we had limited evidence about the effects of vitamin D supplementation on depression remission and severity of anxiety. In addition, a subgroup analysis by intervention duration suggested that vitamin D supplementation was no longer effective in reducing depressive symptoms at follow-up longer than 52 weeks. Also, we included adults regardless of their depression, anxiety, and health status. Finally, despite efforts to identify all relevant studies, publication bias may have influenced the findings, as studies with statistically significant results are more likely to be published. Therefore, more trials are needed to test the long-term efficacy of vitamin D supplementation on depressive symptoms, as well as on depression remission and anxiety symptoms.
Conclusion
Our dose–response meta-analysis of randomized trials demonstrated that vitamin D supplementation may result in a large improvement in depressive symptoms at follow-up shorter than 24 weeks. The greatest impact was seen at 8000 IU/day, and higher doses had no added value in reducing depressive symptoms. Vitamin D supplementation had no effects on depression remission and anxiety symptoms. More trials with high quality are needed to test the long-term efficacy of vitamin D supplementation, considering baseline vitamin D levels of individuals, on depressive symptoms, as well as on depression remission and anxiety symptoms.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0033291724001697.
Data availability statement
The data sets generated or analyzed during the current study are not publicly available but are available from the corresponding author at reasonable request.
Acknowledgements
None.
Author contributions
SS-B designed the research process. SG and SZM searched the databases and extracted the data and necessary information. AJ performed statistical analyses. SG wrote the manuscript. AJ and SS-B critically revised the manuscript. All authors confirmed the final manuscript for submission. SS-B is the guarantor.
Funding statement
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
None.







 Open access
Open access