


- SLR
systematic literature reviews
- WCRF
World Cancer Research Fund
In the UK cancer accounts for about one-quarter of all deaths, second only to CVD(1). Although survival is increasing with improved management, many cancers still carry a poor prognosis as they are less susceptible to surgical, radiotherapeutic or chemotherapeutic intervention, either because of their inherent characteristics or because they may be detected at a late stage of development.
The most common cancers are diseases of adulthood, becoming especially more common in older age. As the population ages cancer prevalence is therefore predicted to increase. Consequently, a policy of managing the burden of cancer in the population based entirely on screening for early detection and management of detected cancers is unlikely to make a marked impact at a population level except for a few types of cancer, and is also likely to be increasingly, and unsustainably, expensive.
Thus, it is important to consider the role for primary prevention in helping to reduce the clinical, personal, economic and social burden of cancer. Approximately one-third of all cancers in high-income countries such as the UK are attributed to smoking(2). Authoritative reviews have further estimated that about one-third of all cancers in such countries might be attributable to factors relating to food, nutrition and physical activity, including body fatness.
In 1997 the World Cancer Research Fund (WCRF), together with its sister organisation the American Institute for Cancer Research, published a landmark report Food, Nutrition and the Prevention of Cancer: a Global Perspective (3). This report has become the most authoritative statement on the topic and a basis for academics, researchers and policy-makers worldwide, and has been followed by a surge in research on the nutritional links with cancer.
In view of the burgeoning body of evidence, in 2001 WCRF and American Institute for Cancer Research embarked on a new report to ensure that its recommendations remained a sound basis for its own and others' activities. This report was published in November 2007(4).
Nutrition and the cancer process
Cancer develops from a clone of cells that have escaped normal regulation of growth, proliferation, differentiation and intercellular relationships. These abnormalities of function derive from disordered expression of key genes, resulting in altered cellular phenotype. The disordered gene expression may result from genetic mutation or from epigenetic factors that may silence genes that should be active or switch on genes that should be silent. Factors relating to food and nutrition may directly influence both processes.
Food components may act directly as mutagens, or conversely may interfere with the action of external mutagens either directly or by facilitating their elimination. Nutritional factors may also alter the cellular milieu by modulating hormonal axes, and so influencing growth and proliferation amongst specific cell populations. Finally, regulation of processes related to specific nutrients may directly influence the expression of key genes, for instance through abnormalities of methylation of the promoter regions of genes or of histone acetylation, which can influence DNA structure and accessibility of genes to mRNA for transcription.
While it is clear that at root cancer is a disease of gene expression, only a minority of cancers appear to be related to inherited single high-penetrance gene mutations. Consequently, a major determinant of cancer risk appears to be the interaction between genotype and environment. Amongst the earliest identified indicators of the importance of this interaction are the different patterns of cancer around the world. Low-income countries have relatively high rates of cancers of the cervix, stomach, liver and oro-pharynx (all of which are at least partly related to infections), while high-income countries are characterised by higher rates of cancers of the breast, prostate and colo-rectum (related to alterations in hormonal axes)(4). Most striking is the rapid change in cancer patterns, within one or two generations, when populations migrate. Together with the secular changes in the incidence of some cancers over only decades, this rapid change effectively excludes inherited factors as a key determinant of these patterns at a population level, although clearly they may be important in determining individual risk within populations.
The rationale for considering food, nutrition and physical activity as key environmental factors in determining cancer risk derives from a mass of epidemiological and mechanistic data, and more recently with some clinical trials as well. The second WCRF/American Institute for Cancer Research report was commissioned with an expert Panel to review this evidence, to draw conclusions and to make recommendations.
The process for the report
Cancer is the result of a complex process of accumulation of abnormal phenotypic characteristics among a clone of cells, usually over decades. This complexity and timescale present obstacles to the study of its pathogenesis and natural history, especially during the preclinical stages. Equally, it is challenging to characterise subjects' exposure to food and nutrients, and their trajectory of growth and body composition, over the life course. In these circumstances, clinical trials cannot realistically address more than a short period of the whole pathogenetic process and are usually conducted in high-risk groups who may not be representative of the general population. Often dietary intervention is in the form of isolated supplements rather than real foods, as it is difficult to achieve or maintain differences between intervention and control groups for real dietary or physical activity interventions.
Consequently, it is difficult to identify single methodological approaches that can be seen as inherently superior. With a body of evidence comprising very different approaches, from observational epidemiology to basic science, and where the generalisability of clinical trials is limited, robust conclusions can only be drawn from a review of the totality of the relevant evidence, allowing for the advantages and disadvantages of different methods. There are accepted approaches to synthesising such evidence and inferring the likely causality of observed associations, such as that proposed in 1963 by Bradford Hill(Reference Bradford Hill5).
With a view to exploring the literature so that Bradford Hill's framework could be applied, WCRF International convened an expert Task Force to develop a standardised method for searching the literature and for analysing and displaying the evidence. This methodology Task Force met over 2 years to develop such a specification.
The feasibility, utility and reproducibility of the specification manual was tested and compared between two independent academic institutes, using endometrial cancer as a test case. As a result amendments were made to the protocol, and the final version(6) was used to conduct the series of systematic literature reviews (SLR) that formed the basis of the Panel's deliberations.
It was decided to keep the process of data collection, analysis and display separate from that of judging it. Thus, nine independent SLR centres, three in the USA, four in the UK and two in continental Europe, were commissioned to conduct SLR on the links between food, nutrition and physical activity and seventeen cancer sites. In addition, SLR were conducted on the links with weight gain and body fatness and the efficacy of nutrition and activity interventions in individuals who had already received a diagnosis of cancer. Finally, a review was conducted on authoritative national and international reports that had made recommendations for the prevention of other diseases, so that any recommendations from this report would be set in a broad public health context.
Each SLR team had to include a range of expertise, in nutrition, epidemiology, statistics, cancer biology, the specific cancer site and systematic review. Each SLR was peer reviewed at the protocol and draft final report stage. WCRF International provided a coordinator whose role was to facilitate the process and ensure consistency in application of the specification.
An expert Panel was convened, comprising twenty-one internationally-renowned scientists, with a range of expertise including nutrition, epidemiology, cancer mechanisms, clinical medicine and public health. Chaired by Professor Sir Michael Marmot, the Panel met over 5 years to discuss and judge the evidence from the SLR, to draw conclusions and to make recommendations.
Judging the evidence
Given the complex nature both of the disease process of cancer and of the characterisation of diet and physical activity over a lifetime, a simple hierarchical approach to evidence on causal links cannot rely on randomised controlled trials. Apart from the obvious inability to mask differences in dietary interventions based on real foods, in practical terms it is equally impossible to secure sufficiently large or sustained differences in lifestyle including diet between intervention groups. Where such studies are done they often use synthetic supplements of isolated nutrients, at high dose, in high-risk groups, with intermediate outcomes. Extrapolation from such studies to the general population is not therefore straightforward. However, long-term observational studies of cohorts of healthy individuals can identify hard outcomes (cancer incidence or mortality) in typical populations consuming real diets over decades. Observational studies, however, unlike randomised trials, are subject to confounding, making causal inferences less robust.
The issue of identifying important causal associations from predominantly observational data where trials are uninformative is not new. Bradford Hill in the 1960s elucidated a series of characteristics of the data that could provide a framework for consideration to help infer which associations are likely to be causal(Reference Bradford Hill7). The SLR specification required the data to be displayed in a way that facilitated the application of Bradford Hill's criteria. The evidence displayed was then judged within that framework, and the likelihood of any association being causal was graded according to how well the criteria were fulfilled.
Before any evidence was presented, the Panel agreed a set of minimum criteria for each grade. The grades were: convincing; probable; limited; substantial effect on risk unlikely. The limited category was further divided into where it was suggestive of a causal relation and where no conclusion could be drawn. In addition, to provide flexibility, certain characteristics of the evidence could be used to upgrade or downgrade conclusions.
Once conclusions were reached, they were presented graphically in the form of a matrix. Matrices were presented for each cancer, with all identified exposures categorised according to the grade of conclusion as to the likely causality of the association. In addition, matrices were presented for each main group of exposures, with the specific exposure–cancer links categorised according to their likely causality (although excluding the large category of limited–no conclusion).
Once agreed, these conclusions provided the basis for making recommendations. Recommendations were based only on conclusions for which the likely causality was judged probable or convincing.
Making recommendations
Recommendations were developed by the Panel with the aim of being as far as possible applicable throughout the world. Where evidence was specific to particular local circumstances this fact was stated. In addition, all recommendations were considered within the context of the review of authoritative expert reports on other diseases, to ensure that they were conducive generally to public health and not restricted to cancer prevention.
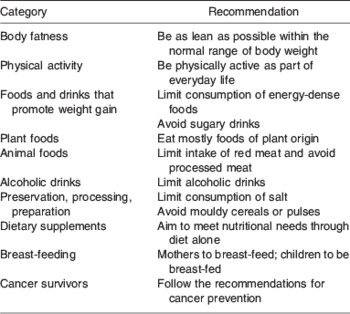
The Panel made ten recommendations. Each recommendation has a title to identify the broad category of food, nutrition or physical activity addressed. This title is followed by a brief headline to provide a sense of the essence of the recommendation, but without detail or quantification. Each recommendation then has a public health goal or goals, directed to policy-makers or health professionals with the aim of facilitating policies or programmes and quantified to aid target setting and monitoring of progress. This public health goal is followed by personal recommendations as a basis for the population (as communities, families or individuals) to make decisions about their own diet and lifestyle, also quantified where possible.
Each of these recommendations is accompanied by explanatory footnotes, which should be considered an integral part of the recommendation.
The headline recommendations are shown in Table 1.
Table 1. Headline recommendations of the expert Panel convened to discuss and judge the evidence from the systematic literature reviews, to draw conclusions and to make recommendations
Looking to the future
The conclusions and recommendations of the Panel set out in the report form a robust basis for further research and for public and professional education programmes. WCRF is preparing materials and other resources that begin this process.
However, scientific evidence is continually accumulating, and each new study needs to be considered in the context of the existing evidence. Thus, WCRF has commissioned a group from Imperial College, London, UK to combine the existing databases produced by the cancer-site SLR, and to update them as new information accrues. This process is overseen by a panel of independent experts, and will be accompanied by periodic reports of updated conclusions and of the implications for the recommendations.
Furthermore, while food, nutrition and physical activity are proximate causes of patterns of cancer, and of other chronic diseases, it is clear that patterns of food consumption and of activity are themselves determined by powerful social, cultural, political and economic factors. A further report to be published in November 2008 will address the evidence for determinants of such patterns and for what might be effective in influencing them. This report, Policy and Action for Cancer Prevention: Food, Nutrition, and Physical Activity – a Global Perspective, will explore the evidence in a similarly rigorous way and make further recommendations for policies and actions to politicians, policy-makers, health professionals and others.
Conclusions
The 2007 WCRF/American Institute for Cancer Research Report Food, Nutrition, Physical Activity, and the Prevention of Cancer: a Global Perspective was produced by an independent Panel, based on systematic reviews conducted by independent academic institutions and conducted transparently according to the most rigorous procedures. It represents the most authoritative review of the topic ever produced and is the most robust current basis for research, education and policy.
Acknowledgements
I have no conflict of interest. I act as a paid consultant to WCRF International, and was project director for the WCRF/ACIR 2007 Report.

