



Introduction
Eating disorders (ED) are characterized by significant disturbances in healthy eating behaviors that impact the physical, emotional, and psychosocial well-being of affected individuals (American Psychiatric Association & Association, Reference American Psychiatric Association and Association2013). Although the etiology of EDs is not fully understood, research frequently points to a multifactorial origin (Culbert et al., Reference Culbert, Racine and Klump2015). Extensive research has explored developmental, genetic, neurobiological, and psychosocial factors (Reyes-Rodríguez et al., Reference Reyes-Rodríguez, Von Holle, Ulman, Thornton, Klump, Brandt and Bulik2011), and more recently, there has been growing interest in the role of neuropsychological factors in the onset and maintenance of EDs (Smith et al., Reference Smith, Mason, Johnson, Lavender and Wonderlich2018).
In particular, executive functions (EF) – essential for purposeful and goal-directed behaviors – have been extensively studied to elucidate the neuropsychological underpinnings of EDs. A critical subdomain of EF is cognitive flexibility (CF), defined as the ability to switch between thinking about different concepts or thinking about multiple concepts simultaneously (Tchanturia et al., Reference Tchanturia, Anderluh, Morris, Rabe-Hesketh, Collier, Sanchez and Treasure2004). Poor CF has been strongly linked to anorexia nervosa (AN) and is suggested as a possible endophenotype of the disorder (Holliday et al., Reference Holliday, Tchanturia, Landau, Collier and Treasure2005). Individuals with bulimia nervosa (BN) also exhibit poor CF, as well as impairments in attention and increased impulsivity (Tchanturia et al., Reference Tchanturia, Anderluh, Morris, Rabe-Hesketh, Collier, Sanchez and Treasure2004; Wu et al., Reference Wu, Brockmeyer, Hartmann, Skunde, Herzog and Friederich2014). Recent studies have shown that executive dysfunction is present across different EDs, indicating a common underlying domain of neurocognitive deficit (Miles et al., Reference Miles, Gnatt, Phillipou and Nedeljkovic2020; Wu et al., Reference Wu, Brockmeyer, Hartmann, Skunde, Herzog and Friederich2014).
Individuals with EDs are often characterized by perfectionism, behavioral rigidity, and ritualistic behaviors related to eating, weight, and body shape (Wade et al., Reference Wade, Wilksch and Lee2012). The adaptive behavioral patterns brought about by CF are not observed in these individuals (Miles et al., Reference Miles, Gnatt, Phillipou and Nedeljkovic2020), manifesting rigid attitudes toward weight and food intake (Kingston et al., Reference Kingston, Szmukler, Andrewes, Tress and Desmond1996). Additionally, patients with AN and their unaffected relatives demonstrate an impaired executive profile characterized by inadequate set-shifting, a skill that allows individuals to flexibly shift between modes of thought (Galimberti et al., Reference Galimberti, Fadda, Cavallini, Martoni, Erzegovesi and Bellodi2013). A meta-analysis has shown that set-shifting is also particularly poor in the BN subgroup (Wu et al., Reference Wu, Brockmeyer, Hartmann, Skunde, Herzog and Friederich2014), although CF is less impaired in BN compared to AN (Zakzanis et al., Reference Zakzanis, Campbell and Polsinelli2010). Longitudinal studies have shown no significant difference in CF between those who achieved weight restoration and those in the acute phase of the illness (Miles et al., Reference Miles, Gnatt, Phillipou and Nedeljkovic2020). In contrast to studies in adults with ED, very few studies have been conducted with the adolescent population.
In some research, difficulties in emotion recognition (ER) have been frequently observed in patients with ED (Harrison et al., Reference Harrison, Sullivan, Tchanturia and Treasure2009; Kerr-Gaffney et al., Reference Kerr-Gaffney, Harrison and Tchanturia2019). Reduced ER and social and emotional factors are reported to be potential triggers at the onset of eating pathology and often play a sustaining role in ED (Fairburn et al., Reference Fairburn, Cooper and Shafran2003; Schmidt & Treasure, Reference Schmidt and Treasure2006). A study indicated that adults with AN have difficulties in recognizing negative emotions, which may play a role in maintaining the disorder (Brockmeyer et al., Reference Brockmeyer, Pellegrino, Maier, Münch, Harmer, Walther, Herzog and Friederich2019). In studies with adults, ER difficulties are evident, whereas there are only a few studies with adolescents. A recent study involving 33 adolescents with AN and using a dynamic emotion recognition task (including facial images and video clips) showed that patients with AN were able to recognize emotions as accurately as the control group but had a higher sensitivity in recognizing negative emotions, particularly disgust and sadness (Duriez et al., Reference Duriez, Guy-Rubin, Kaya Lefèvre and Gorwood2022). Studies investigating the ER functions of individuals with AN generally emphasize the difficulties they experience in the emotional and social domains (Fairburn et al., Reference Fairburn, Cooper and Shafran2003; Schmidt & Treasure, Reference Schmidt and Treasure2006). However, studies involving patients with BN and BED are limited in this regard (Tchanturia et al., Reference Tchanturia, Davies, Roberts, Harrison, Nakazato, Schmidt, Treasure and Morris2012).
The existing literature highlights the critical role of CF and ER in understanding ED (Fairburn et al., Reference Fairburn, Cooper and Shafran2003; Zakzanis et al., Reference Zakzanis, Campbell and Polsinelli2010). However, there is a significant gap in studies focusing on the adolescent population, where these cognitive and emotional processes are still developing (Smith et al., Reference Smith, Mason, Johnson, Lavender and Wonderlich2018). Adolescents with ED may exhibit different patterns of CF and ER compared with adults, necessitating targeted research in this age group. This study aimed to investigate CF and ER in adolescent patients with ED, exploring potential associations between these cognitive and emotional aspects. Thus, we hope to enhance our understanding of the neurocognitive mechanisms underlying ED and contribute to the development of more effective treatment approaches. We hypothesized that adolescents with ED would have lower performance in CF and ER when compared to healthy individuals. Furthermore, it was hypothesized that those with lower CF scores would also exhibit lower ER performance.
Methods and materials
Participants
This study included two main groups: an ED group and a control group. The ED group consisted of 46 adolescents ages 13–18, including 28 with Anorexia Nervosa (AN), 10 with Bulimia Nervosa (BN), and 8 with Binge Eating Disorder (BED). Among the ED group, there were 5 males (2 with AN, 1 with BN, and 2 with BED). The median age was 15.00 years (IQR: 3) for AN, 14.00 years (IQR: 2) for BN, and 14.00 years (IQR: 3) for BED. The average duration of illness was 19.2 weeks (SD = 9.2) for AN, 26.2 weeks (SD = 15.8) for BN, and 14.2 weeks (SD = 6.3) for BED.
The control group comprised 40 healthy individuals (20 females and 20 males) aged 1–18 years, with a median age of 16.00 years (IQR: 1). These individuals, who applied to our psychiatry clinic for various reasons, had no prior psychiatric history or psychiatric illness according to the psychiatric interview based on DSM-5 criteria, and had normal body weight according to percentile values of that age, were included to the study. The body mass index (BMI) was calculated by dividing a person’s weight by the square of height in centimeters. Patients with any acute or chronic illness that could impact cognitive functioning (e.g., neurological, endocrine, and immune conditions) were not included. Considering that it may have negative effects on cognitive skills, the participants with a BMI outside the expected values for the child’s age were not included in the control group.
Procedure
The structured psychiatric interview (Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version DSM-5) and neurocognitive tasks were administered to the control group and ED patients to evaluate psychiatric diagnoses. The procedure involved administering a battery of tests to evaluate CF and ER. In various studies, CF has been assessed using different neuropsychological tests (Diamond, Reference Diamond2013; Wu et al., Reference Wu, Brockmeyer, Hartmann, Skunde, Herzog and Friederich2014). These tests evaluate different aspects of CF, including set-shifting and inhibitory control, which are crucial for adaptive behavior and problem-solving. In our study, we specifically utilized the Berg Card Sorting Test (BCST) to assess set-shifting abilities and the Stroop Test to evaluate inhibitory control, aiming to capture some key aspects of CF in adolescents with ED. In addition to neuropsychological tests, we also assessed CF using the self-report Cognitive Flexibility Scale (CFS). Parents completed sociodemographic and clinical data forms. To evaluate ER, the Test of Perception of Affect via Non-Verbal Cues (TPANC) was performed on the computer. Tests were administered over two sessions on different days, each lasting 30 minutes per participant.
This study was approved by the Ankara University Faculty of Medicine Ethics Committee (İ3-202-21). This study was conducted following the Declaration of Helsinki. Detailed informed consent was obtained from all participants and their parents through written consent forms that included comprehensive information. The data supporting the findings are not publicly available because of ethical restrictions but are available on request from the corresponding author.
Measures
Sociodemographic and clinical data form
A form was created by the researchers to record sociodemographic information such as age, gender, and education, as well as clinical data including medical history.
Stroop test
This is a widely used neuropsychological test developed to assess executive functions, including attention and response inhibition (George Peabody Coll, Reference George Peabody Coll1992). It measures information processing speed, the ability to shift goals based on changing demands, and resistance to the disruptive effects of automatic processes (Williams et al., Reference Williams, Mathews and MacLeod1996). In this study, the Number Stroop version of the Stroop Test, which allows computer-based administration with the PEBL Launcher 2.1 application, was used. The test involved two conditions: congruent (where the number of items matched the number shown) and incongruent (where the number of items did not match the number shown). Participants responded by identifying the number of items and not the digit displayed. The interference effect was calculated as the time difference between responses to incongruent and congruent stimuli, with higher differences indicating greater difficulty in inhibiting automatic response tendencies (Mueller & Piper, Reference Mueller and Piper2014). In CF studies, the “interference effect” has been frequently used as a predictor of cognitive flexibility (Friedman & Miyake, Reference Friedman and Miyake2017). Therefore, we also included this measure as a CF indicator.
The berg card sorting test (BCST)
The BCST measures cognitive processes, such as working memory, conceptualization, abstract thinking, and reasoning, including perseverative tendencies that reflect set-shifting difficulties (Karakaş & Karakaş, Reference Karakaş and Karakaş2000). In our study, it was administered using the computerized PEBL Launcher 2.1 application (Fox et al., Reference Fox, Mueller, Gray, Raber, Piper and Brucki2013; Mueller & Piper, Reference Mueller and Piper2014). Participants sorted a deck of response cards based on different stimuli without prior knowledge of sorting principles. After sorting 64 cards, the participants were expected to learn the various rules based on the feedback (correct/incorrect) given after each response. The rules change during the task, leading to perseverative errors when the individual persistently continues to respond based on the previous rule. The “perseverative error percentage” was used to assess set-shifting difficulties, which has been utilized in numerous studies (Miles et al., Reference Miles, Gnatt, Phillipou and Nedeljkovic2020). A higher percentage of perseverative errors reflects greater difficulty in set-shifting, indicating cognitive rigidity (Grant & Berg, Reference Grant and Berg1948; Miyake et al., Reference Miyake, Friedman, Emerson, Witzki, Howerter and Wager2000). Thus in our study, the perseverative error percentage on the BCST was also used as an indicator of CF.
Test of perception of affect via nonverbal cues (TPANC)
This test is designed to assess the ability to detect nonverbal cues and recognize emotions (Kılıç Tülü & Ergül, Reference Kılıç Tülü and Ergül2015). It assesses six basic emotions – fear, sadness, anger, surprise, disgust, and happiness – through various cues such as facial expressions, vocal tones, body movements, and social stories. The tool presents photos, voices, body movements, and social stories of adults and children and includes 56 questions in a computer-based format. This comprehensive approach allows for the evaluation of ER in a manner that closely mirrors real-life situations, thus providing high ecological validity.
Facial Expressions Subdomain
This subdomain consists of 24 questions featuring photos of two adults and two children expressing one of the six basic emotions. Participants identify the emotion, and the responses are recorded.
Body movements subdomain
This subdomain includes eight questions in which participants watch video clips (1–3 s each) of models expressing four emotions (happiness, sadness, anger, and fear) through body movements. Faces are not shown and participants identify emotion based on these movements.
Vocal tones subdomain
This subdomain contains 12 questions using voice recordings of two adults and two children saying a sentence. For example: “Did you taste the food?” in tones representing the six basic emotions. Participants identify the emotion based on the vocal tone.
Social stories subdomain
Thıs subdomain features 12 social stories that convey one of the six emotions. Stories are read to participants in a neutral tone, and participants identify the emotion conveyed by the story.
Each subdomain’s responses were recorded, and correct answers received 1 point, whereas incorrect answers received 0 points. TPANC total score (TPANC-TS) was used to evaluate ER in this study.
The cognitive flexibility scale (CFS)
CFS is a one-dimensional and self-reported measurement tool consisting of 12 items on a six-point Likert scale with response options ranging from 1 “strongly disagree” to 6 “strongly agree”. The internal consistency of the CFS was calculated to be 0.72, 0.73, and 0.81. Higher scores on this scale indicate a better CF level (Martin & Rubin, Reference Martin and Rubin1995). In this study, the total CFS score was used to evaluate CF in both the ED and control groups.
Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version DSM-5 (K-SADS-PL-DSM-5)
K-SADS-PL-DSM-5 is a semi-structured, diagnostic clinical interview focusing on categorical assessment of past and current psychiatric disorders in children (Kaufman et al., Reference Kaufman, Birmaher, Brent, Rao, Flynn, Moreci, Williamson and Ryan1997). According to the reliability study of the Turkish version, the consistency of diagnoses was high for ED (Ünal et al., Reference Ünal, Öktem, Çetin Çuhadaroğlu, Çengel Kültür, AKDEMİ, Foto Özdemir, Çak, Ünal, TIRAŞ and Aslan2019). In the current study, K-SADS-PL was applied to confirm ED and detect comorbidities. Disorders that could significantly affect test performance, such as psychosis and bipolar disorder, were excluded. However, given the high comorbidity of depression, generalized anxiety disorder, obsessive–compulsive disorder, and attention-deficit/hyperactivity disorder with ED, participants with these comorbidities were not excluded to ensure that the sample accurately represented the broader ED population. (Hambleton et al., Reference Hambleton, Pepin, Le, Maloney, Barakat, Boakes, Brennan, Bryant, Byrne, Caldwell, Calvert, Carroll, Castle, Caterson, Chelius, Chiem, Clarke, Conti, Crouch and Maguire2022).
Statistical analysis
Statistical analysis was performed using SPSS 23. The normal distribution of continuous variables was assessed using the Shapiro–Wilk test.
Comparisons between the ED and control groups
Categorical variable comparisons were performed using the chi-square test and Fisher’s exact test. For continuous variables, t-tests were used for normally distributed data to compare the means of the ED and control groups. For non-normally distributed data, the Mann–Whitney U test was used.
Comparisons among ED subgroups (AN, BN, and BED)
One-way ANOVA was used to compare the three subgroups if the data were normally distributed. Post hoc analyses for ANOVA were performed using the Tukey test for homogenous variances and the Tamhane T2 test for heterogeneous variances. For non-normally distributed data, the Kruskal–Wallis test was used. In the statistically significant results, to determine the groups contributing to the difference, post hoc analyses with the Mann–Whitney U test and Bonferroni correction to control for multiple comparisons were conducted.
Multiple comparisons and missing values
To handle multiple comparisons, Bonferroni correction was applied to adjust the significance levels, thereby reducing the risk of Type I errors. Missing values were addressed using multiple imputation methods to ensure the robustness of the statistical analysis.
Handling small group sizes
Given the small group sizes of the ED subgroups, bootstrapping techniques were employed to validate the findings. Bootstrapping is a resampling method that estimates the distribution of statistics by sampling with replacement, providing more reliable inferences from small samples.
Correlation analyses
Pearson correlation was used for normally distributed continuous variables to examine the relationships between measures. For non-normally distributed continuous variables, Spearman’s correlation was used.
P-values < .05 were considered statistically significant.
Results
The patient group consisted of 46 individuals, including 28 patients with AN (2 males, 26 females), 10 patients with BN (1 male, 9 female), and 8 with BED (2 males, 6 females). The control group comprised 20 females and 20 males. There were no statistically significant age differences between the ED and control groups. When the groups were analyzed with the Chi-square test, a significant difference was found in terms of gender distribution (p = .006). There were no significant age differences between the ED and control groups. When the groups were analyzed with the Chi-square test, a significant difference was found in terms of gender distribution (p = .006).
The distribution of ED patients in subgroups and comorbid psychiatric disorders is shown in Table 1. Despite the relatively higher prevalence of ADHD in the BED subgroup, the difference in psychiatric comorbidities between the subgroups was not statistically significant. The average duration of illness was 19.2 weeks (SD = 9.2) for the AN subgroup, 26.2 weeks (SD = 15.8) for the BN subgroup, and 14.2 weeks (SD = 6.3) for the BED subgroup. There were no statistically significant differences in illness duration by subgroup.
Table 1. Distribution of psychiatric comorbidities in ED subgroups
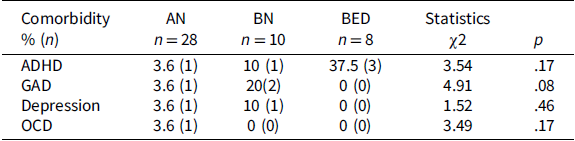
Chi Square Test. ADHD = Attention Deficit Hyperactivity Disorder, GAD = Generalized Anxiety Disorder, OCD = Obsessive–Compulsive Disorder, AN = Anorexia Nervosa, BN = Bulimia Nervosa, BED = Binge Eating Disorder, ED = Eating Disorders.
When the CFS scores were compared, the mean score of the control group (M = 53.73, SD = 9.2) was significantly higher than that of the ED patients (M = 47.81, SD = 8.6), t (84) = 3.08, p = .003, with a moderate effect size (η2 = .102). These findings indicate that the control group demonstrated better CF compared to ED patients.
Subsequently, we performed a more detailed analysis by comparing CF scores between four distinct groups: the control group, AN subgroup, BN subgroup, and BED subgroup. Significant differences in CF scores were found across these groups as shown in Table 2. To determine the specific groups contributing to these differences, pairwise comparisons were conducted using the Mann–Whitney U test, with Bonferroni correction applied to adjust for multiple comparisons (adjusted significance level set at p < .017). The results indicated significant differences between the control group and the AN subgroup (p = .006, adjusted p < .017), as well as between the control group and the BN subgroup (p = .001, adjusted p < .017). These findings suggest that the statistically significant differences in CF scores were primarily due to the disparities between the control group and the AN subgroup and between the control group and the BN subgroup. The AN and BN patients described themselves as cognitively more rigid compared to the control group.
Table 2. Comparison of cognitive flexibility scale scores and cognitive test performances between the ED subgroups and the control group

Kruskal Wallis H, AN = Anorexia Nervosa, BN = Bulimia Nervosa, BED = Binge Eating Disorder, BCST = Berg Card Sorting Test, *p < 0.05.
Statistically significant differences in Stroop interference scores were observed as shown in Table 2. Results showed that the BED subgroup had significantly higher Stroop interference scores than the control group (U = 1.108, p = .006, Bonferroni-adjusted p < .008), indicating greater difficulties with inhibitory control in the BED subgroup. In contrast, no significant differences in Stroop interference were found between the control group and AN subgroup (U = 378.0, p = .024, Bonferroni-adjusted p > .008) or the BN subgroup (U = 145.0, p = .186, adjusted p > .008). Additionally, BCST perseverative error percentages showed no significant differences between ED subgroups and the control group (H (3) = 4.173, p = .243).
When comparing the ED and control groups based on TPANC-TS and its subdomains, the Mann–Whitney U test revealed statistically significant differences with small-to-moderate effect sizes between the ED and control groups in the “tone of voice” and “social stories” subdomains, with the ED group presenting higher scores as shown in Table 3. The higher scores indicated a better understanding of subdomains.
Table 3. Comparison of the TPANC subdomain scores of the ED and control groups
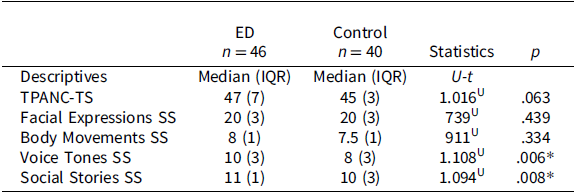
TS = Total Score, SS = Subdomain Scores. U = Mann–Whitney U, t = Student t-test, ED = Eating Disorders. * pp < 0.05.
For a more detailed analysis, ER performances were compared between the AN, BN, BED subgroups and the control group across TPANC subdomains. The results indicated no significant differences in most subdomains. However, the Mann–Whitney U test revealed that the AN subgroup had significantly higher scores than the control group in the “tone of voice” subdomain, with a large effect size (U = 181.500, p < .001, r = .345). Similarly, the AN subgroup scored higher in the “social stories” subdomain compared to the control group, with a large effect size (U = 231.000, p < .001, r = .520). These findings suggest that individuals in the AN subgroup may have a superior understanding of tone of voice and social stories compared to controls.
Initially, the ED and control groups were compared in terms of emotion expression, and significant differences were found between the ED and control groups for the expression of disgust and fear (Table 4). The ED group showed better recognition of disgusted expressions compared to the control group (r = .25), as well as for fearful expressions (r = .23), as shown in Table 4.
Table 4. Emotion expression scores for ED and control groups
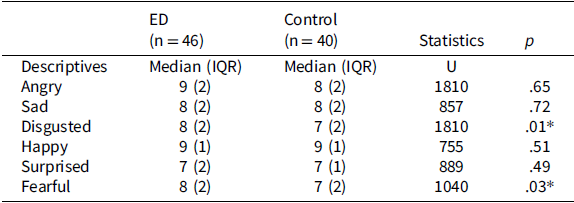
ED = Eating Disorders U = Mann–Whitney U. *p < 0.05.
To determine the source of these differences, pairwise comparisons were conducted using the Mann–Whitney U test. The pairwise comparisons revealed that the AN subgroup exhibited significantly better recognition of expression of disgust compared to the controls (U = 293.500, p = .007, adjusted p-value = .008), with a moderate effect size (r = .47). Similarly, for expressions of fear, the AN subgroup again showed significantly better recognition compared to the control group (U = 257.00, p = .002, adjusted p-value = .008), with a moderate effect size (r = .54). In contrast, no significant differences in ER performance were found between the BN subgroup, BED subgroup, and control group.
Relationship between cognitive flexibility and emotion recognition
The evaluation of the relationship between TPANC-TS scores and CF predictors (Stroop interference, BCST perseveration percentage, and CFS scores) is shown in Table 5. A significant negative correlation was found between BCST Perseveration Percentage and TPANC-TS in the ED group. This suggests a medium-to-large effect size, indicating that higher perseverative percentage rates indicative of cognitive rigidity are associated with lower ER scores. However, no significant relationships were found between Stroop Interference, CFS scores, and TPANC-TS.
Table 5. Relationship between cognitive flexibility and emotion recognition in ED and control groups
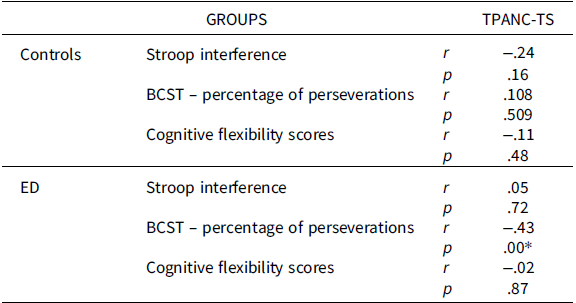
ED = Eating Disorders, TPANC-TS = Test of Perception of Affect via Non-Verbal Cues Total Score, Spearman Correlation Analysis, *p < 0.05.
To examine whether the significant differences in gender distribution between the groups influenced the results, the CF and ER performances of the control group were compared between males and females. As shown in Table 6, independent sample t-test results indicated no significant difference between participants in all measured domains: TPANC-TS, Stroop intervention, BCST – percentage of perseveration, and CFS.
Table 6. Comparison of cognitive flexibility and emotion recognition between females and males in control and ED groups
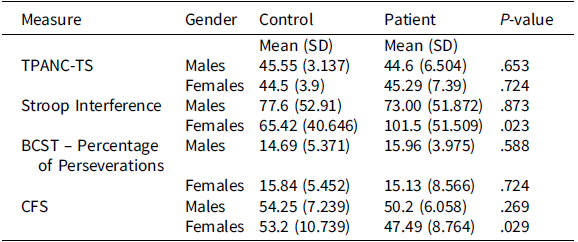
SD = Standard Deviation, ED = Eating Disorders, p < 0.05. Student t-test, TPANC-TS= Test of Perception of Affect via Non-Verbal Cues Total Score, Stroop Interference = Stroop Interference Score, BCST – Percentage of Perseverations = Berg Card Sorting Test Perseveration Percentage, CFS = Cognitive Flexibility Scale.
Discussion
This study used CFS scores, Stroop interference effect, and BCST perseveration percentage as predictors of CF, whereas TPANC-TS data were analyzed to assess ER. Compared to the controls, the ED group perceived themselves as more cognitively rigid, as indicated by self-report via the CFS. The significantly higher CFS scores (indicating better CF) in controls partially supported the primary hypothesis of a significant difference in CF between the ED group and the control group. However, contrary to our expectations, no significant differences were observed in the perseverative error percentages on the BCST or total scores on the TPANC between the two main groups.
In addition to the generally lower CFS scores among patients with ED, comparisons between each subgroup and the control groups revealed significant differences between those with AN and BN compared to the controls. However, despite the lower scores observed in BED patients, the difference between the BED and the control groups was not statistically significant. BED patients, on the other hand, demonstrated significant challenges in inhibitory control, as evidenced by their Stroop Test performance.
Comparison of age, gender, and presence of comorbidities in ED and control groups
In the current study, similar age ranges and disease severity of the ED patients may have minimized the potential confounding effects. The participants in the ED group were predominantly female, whereas the control group had equal numbers of females and males. This distribution is consistent with the literature, indicating a higher ED prevalence among females (Hoek & van Hoeken, Reference Hoek and van Hoeken2003).
Comorbidity rates in the BED subgroup were relatively higher compared to the AN and BN subgroups, but the difference was not found to be significant. In addition, although some patients had subclinical levels of anxiety and depression, the frequency of comorbid depression and anxiety diagnoses was lower than that reported in the ED literature (Golden & Attia, Reference Golden and Attia2011), possibly because the study was conducted during the initial diagnosis period.
Evaluation of CFS scores, BCST, and stroop tests
Our study suggests that individuals with ED perceive themselves as more cognitively rigid, as partially indicated by self-reported measures. Specifically, the BED subgroup demonstrated significant difficulties with inhibitory control, as highlighted in Stroop test results. This difficulty may reflect the neurocognitive characteristics underlying binge-eating behaviors, as inhibition control issues are often linked to impulsive tendencies (Barkley, Reference Barkley1997). A longitudinal study reported that AN patients rated themselves as more rigid, however, this was not reflected in objective neuropsychological measures (van Noort et al., Reference van Noort, Lohmar, Pfeiffer, Lehmkuhl, Winter and Kappel2018). Although ED patients generally presented lower scores on CFS, this perception-cognitively more rigid- did not translate into objective differences in set-shifting abilities as measured by the BCST. The discrepancy between self-reported and neurocognitive assessments aligns with the weak correlation frequently observed between these measures; some argue that self-report scales offer broader, ecologically valid insights into cognitive rigidity by capturing daily life experiences that objective tests may overlook (Calderoni et al., Reference Calderoni, Muratori, Leggero, Narzisi, Apicella, Balottin, Carigi, Maestro, Fabbro and Urgesi2013; Halmi et al., Reference Halmi, Sunday, Strober, Kaplan, Woodside, Fichter, Treasure, Berrettini and Kaye2000; Lounes et al., Reference Lounes, Khan and Tchanturia2011). In addition, neurocognitive test results in adult patients with ED may differ from those in adolescents, particularly in the early stages of the disorder. This suggestion challenges the endophenotype hypothesis, which suggests that cognitive inflexibility arises during the pre-disease period (Tenconi et al., Reference Tenconi, Santonastaso, Degortes, Bosello, Titton, Mapelli and Favaro2010). Conducting longitudinal studies that evaluate patients with neuropsychological tests from the time of diagnosis could offer valuable insights into this area.
In line with previous research, our findings suggest that while neurocognitive tests provide objective data, self-reported measures capture a broader spectrum of CF deficits as experienced in daily contexts (Dahlgren et al., Reference Dahlgren, Hage, Wonderlich and Stedal2019). Interventions aimed at enhancing CF have shown effectiveness in reducing symptoms of depression in AN patients, highlighting the potential benefits of such interventions for this group (Tchanturia et al., Reference Tchanturia, Lloyd and Lang2013). Our results underscore the need for a dual-focused approach in ED treatment, one that addresses both subtype-specific characteristics – such as impaired inhibitory control in BED, likely reflecting their uncontrollable binge-eating behaviors and requiring a different approach than that for restrictive eating patterns – and shared cognitive mechanisms across EDs. Future research involving a larger, more balanced sample of ED patients, particularly in BED and BN subgroups, is warranted to confirm these findings. Additionally, the relatively small size of our BED subgroup and its higher prevalence of comorbid ADHD may have influenced inhibitory control outcomes, as ADHD is known to exacerbate difficulties in inhibitory responses (Barkley, Reference Barkley1997).
The lack of significant differences in BCST perseverative error percentages between the patient and control groups requires further interpretation. The BCST assesses set-shifting ability, which is the capacity to switch between different tasks or mental sets (Berg, Reference Berg1948; Grant & Berg, Reference Grant and Berg1948). Perseverative errors occur when a previous rule is persistently used, disregarding feedback that indicates it is incorrect. The nonsignificant results on BCST perseverative error percentages suggest that while patients with ED exhibit deficits in inhibitory control as shown by the Stroop test, their ability to shift between tasks or mental sets is similar to that of the control group. This finding implies that the CF aspect of executive functioning, as measured by set-shifting tasks, may not be as affected in ED patients as inhibitory control. Alternatively, the BCST may not be as sensitive to detecting certain types of cognitive deficits in ED patients as the Stroop Test.
Our study found that patients with BED struggled more with response inhibition than controls and other ED subgroups. Limited literature compares BED with other EDs, often emphasizing obese individuals (Danner et al., Reference Danner, Ouwehand, van Haastert, Hornsveld and de Ridder2012). Our findings suggest that compromised inhibitory control in the BED subgroup may be related to excessive eating behavior consequences similar to those in obese individuals (Dohle et al., Reference Dohle, Diel and Hofmann2018).
Nonetheless, our results should be interpreted cautiously, considering the gender imbalance between the control and the patient groups, with significantly higher rates of females in the ED group. Although the balanced gender distribution in the control group may be notable in terms of reflecting the population sample, the significant difference between the control and ED groups may have influenced our findings. The literature indicates that females generally perform better in ER tasks because of biological and social factors, whereas males may exhibit different patterns of CF (Gur et al., Reference Gur, Richard, Calkins, Chiavacci, Hansen, Bilker, Loughead, Connolly, Qiu, Mentch, Abou-Sleiman, Hakonarson and Gur2012; Thompson & Voyer, Reference Thompson and Voyer2014). To understand the effect of this condition, females and males were compared across the groups and no differences were found in CF skills. This may suggest that disease rather than gender is more influential. Nonetheless, the distribution of males in ED subgroups is a point to be considered and may have reduced the reliability of the findings.
Evaluation of ER findings
The study revealed no significant differences in total TPANC scores between the groups. In contrast to previous studies utilizing static paradigms and reporting impaired ER in ED patients, our study employed the more ecologically valid TPANC, which assessed ER through facial expressions, movements, voices, and social stories (Guala, Reference Guala2012; Janssens et al., Reference Janssens, Lataster, Simons, Oorschot, Lardinois, van Os and Myin-Germeys2012). This ecologically enhanced approach could account for the variation in outcomes and better reflect real-life ER within these populations.
While most ER studies in AN have focused on adults, the available research involving adolescents aligned with our findings, indicating the absence of ER deficits in the ED group (Laghi et al., Reference Laghi, Pompili, Zanna, Castiglioni, Criscuolo, Chianello, Baumgartner and Baiocco2015; Mendlewicz et al., Reference Mendlewicz, Linkowski, Bazelmans and Philippot2005; Nalbant et al., Reference Nalbant, Kalaycı, Akdemir, Akgül and Kanbur2019). In our study, an intriguing observation emerged, in which the AN subgroup exhibited superior emotional understanding in the vocal tone and social story sections compared with the controls. Utilizing the International Affective Picture System for facial ER, a separate assessment revealed that the AN restrictive subgroup displayed reduced recognition of happiness compared with both the BN subgroup and controls, which was attributed to higher depression scores in the AN restrictive subgroup. This led to the reconsideration of a fundamental ER deficit in patients with ED (Connan & Stanley, Reference Connan and Stanley2003). Notably, our ED group showed enhanced ER, which was possibly attributed to lower depression comorbidity. Gender imbalance in the groups may have influenced the results. Research has indicated that girls tend to outperform boys in ER skills (Oldershaw et al., Reference Oldershaw, Lavender, Sallis, Stahl and Schmidt2015; Russell et al., Reference Russell, Schmidt, Doherty, Young and Tchanturia2009; Westwood et al., Reference Westwood, Kerr-Gaffney, Stahl and Tchanturia2017), which might have contributed to the higher-than-expected performance in the ED group with a higher proportion of girls.
In another study comparing adult AN patients with controls, the correlation between extended illness duration, lower BMI, and impaired ER was attributed to brain adaptations in response to hunger and irregular eating patterns (Brockmeyer et al., Reference Brockmeyer, Pellegrino, Maier, Münch, Harmer, Walther, Herzog and Friederich2019). Considering the short disease duration of AN patients (approximately 19 weeks) and the incomplete neurobiological development, these cross-sectional results should be followed up on at later ages. Although adolescents with AN did not exhibit ER difficulties in our study, their social and relational difficulties documented in the literature (Oldershaw et al., Reference Oldershaw, Lavender, Sallis, Stahl and Schmidt2015; Russell et al., Reference Russell, Schmidt, Doherty, Young and Tchanturia2009; Westwood et al., Reference Westwood, Kerr-Gaffney, Stahl and Tchanturia2017) warrant investigation of factors related to ER deficits in larger samples.
Patients with AN accurately recognized emotions similar to controls but were more sensitive to negative emotions, particularly disgust and sadness. This may indicate heightened negative emotional sensitivity, particularly in sensory-associated emotions (Duriez et al., Reference Duriez, Kaya Lefèvre, Di Lodovico, Viltart and Gorwood2021). The one study exploring disgust sensitivity in AN yielded mixed results (Aharoni & Hertz, Reference Aharoni and Hertz2012). Higher dorsolateral prefrontal cortex activation in response to negative emotions was reported in AN patients (Seidel et al., Reference Seidel, King, Ritschel, Boehm, Geisler, Bernardoni, Beck, Pauligk, Biemann, Strobel, Goschke, Walter, Roessner and Ehrlich2018). Investigating whether the recognition of negative stimuli corresponds to heightened cortical activity and self-control may be beneficial.
Evaluation of the relationship between CF and ER
Contrary to our hypothesis, there was no correlation between CF predictors (CFS, Stroop interference, BCST perseveration percentage) and ER (TPANC-TS), except for a negative correlation between perseveration percentages and ER. Several studies have indicated that enhanced emotional understanding is linked to various cognitive abilities, especially executive functions ((Arcelus et al., Reference Arcelus, Haslam, Farrow and Meyer2013; Cardi et al., Reference Cardi, Di Matteo, Gilbert and Treasure2014). However, the majority of the studies were conducted with adult patients. A previous study suggested that children with better inhibitory control have higher ER performance and that they should improve their inhibition capacity to understand the emotions of others (Fabio et al., Reference Fabio, Esposito, Carrozza, Pino and Caprì2020). In this sense, the fact that this relationship was not shown with the Stroop Test and CFS scores in our study seems to contradict previous findings. The imbalanced distribution of males and females in the groups may have influenced the results. However, to the best of our knowledge, this is the first study to examine the relationship between CF and ER in adolescents with ED. Further studies are warranted to highlight the association between different domains of executive functions, including CF, set-shifting, and inhibitory control.
Conclusions
Adolescents with AN and BN perceive themselves as more cognitively rigid based on self-reported measures, although no significant differences were observed in set-shifting abilities. However, the BED subgroup displayed specific impairments in inhibitory control, aligning with the impulsive tendencies associated with this subgroup. Although adolescents with AN demonstrated a heightened sensitivity in recognizing certain negative emotions, our study did not identify any significant ER deficits in ED patients compared to controls. These findings underscore the need for a dual approach in ED treatment that addresses both subtype-specific characteristics and shared cognitive mechanisms. Future studies with larger, more homogeneously distributed samples across gender and ED subgroups would be beneficial to confirm these findings and to further examine the effects of ED on cognitive and emotional functioning in greater detail.
Limitations
The main limitations of this study include its cross-sectional design, imbalanced gender distribution among the groups, and small sample size, which restrict our findings to correlational conclusions rather than causal inferences. The research was conducted at a single center; hence, multicenter longitudinal studies are warranted to provide insights into the progression of CF and inhibitory control over time in ED. Additionally, the limited sample size impacted subgroup analyses, with uneven representation across the BN and BED subgroups, potentially affecting the generalizability of these findings to the broader population. While gender distribution in the control group was balanced, the predominance of female participants in the ED group is a limitation, although it may reflect the typical gender distribution observed in ED populations. To address the potential impact of gender distribution on our results, additional analyses were conducted, and no significant gender-related differences were observed. Thus, our findings should be interpreted cautiously, and these limitations taken into account.
Acknowledgments
We would like to thank Amber Rochette, Ph.D., and the Research and Editing Consulting Program of the International Neuropsychological Society for editorial assistance.
Funding statement
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Competing interests
None to declare.







 Open access
Open access