


Introduction
Healthy nutrition habits play an important role in preventing chronic diseases in later stages of life(Reference Jung and Bice1). Various studies have reported the protective roles via increasing intake of fruits and vegetables (F&V: Fruits such as apples, oranges, bananas, watermelons, melons, grapes and pomegranates and Vegetables such as raw vegetables, cooked vegetables, potatoes, tomatoes, cucumbers and carrots) against chronic conditions such as cardiovascular disease, cancer and diabetes(Reference Mytton, Nnoaham and Eyles2–Reference Seyedrezazadeh, Pour moghaddam and Ansarian6). Low F&V intake is globally associated with 2·8 % of deaths, a considerable number of which are caused by cardiovascular disease, stroke and gastrointestinal cancer(7). Therefore, increasing F&V intake is a part of the public health strategies of the World Health Organization (WHO) for preventing non-communicable diseases(8). According to a study by Msambickaka, despite the benefits of F&V intake, more than 75 % of the world's population fail to consume enough F&V(Reference Msambichaka, Ezel and Abdul9). Based on the studies conducted in Iran, Zamanian pointed out that F&V intake was lower than the recommended amount (minimum of 400 g or 5 servings of F&V per day(10))(Reference Zamanian, Paksereshet and Holakouie-Naeini11). In a review study of Abdi et al. in the field of food basket and food consumption pattern of Iranians from 2000 to 2014, the results have showed that the average per capita consumption of F&V in Iran 142 and 286 g/d, respectively(Reference Abdi, AttarodiKashani and Mirmiram12), as well in Mazandaran province of Iran, according to the latest study, 70 and 49 % of people did not consume enough F&V (minimum of 2 servings F and 3 servings V), respectively(Reference Djalalinia, Saeedi Moghaddam and Sheidaei13).
Benefits of consuming F&V in people's health based on epidemiological results for daily consumption are recommended(Reference Ohtsuki, Shibata and Fukuwatari14). For example, the results of a systematic review and meta-analysis of the dose-response of F&V to the risk of cardiovascular disease, cancer and mortality have indicated that 800 g/d consumption has reduced all cases, except cancer which has been reduced by consuming 600 g/d(Reference Aune, Giovannucci and Boffetta15).
Knowledge plays a key role in changing health behaviour; therefore, it seems necessary to publicise F&V intake required to maintain ideal health(Reference Msambichaka, Ezel and Abdul9). Pengpid et al. showed that targeted interventions could increase F&V intake by identifying changeable risk factors such as low levels of education and general obesity(Reference Pengpid, Vonglokham and Kounnavong16). According to Tassitano et al., self-efficacy in behaviour change strategies was one of the main predictors of F&V intake in Brazil(Reference Tassitano, Martins and Cabral17). In addition, Wilsher et al. introduced conscience and emotional stability as very strong dimensions of F&V intake in the UK with respect to the role and importance of personality in diet and health behaviour(Reference Howard Wilsher, Houghton and Papageorgiou18). Thus, studies conducted in recent decades have focused mainly on perception of generation and maintenance of healthy behaviour(Reference Tassitano, Martins and Cabral17). The identification of mediation factors has an effective role in formulating intervention programmes(Reference Kasten, Osch and Eggers19). One of such factors is to attract social support for healthy nutrition, which can be attributed to the positive effect and encouragement of others to have healthy eating habits(Reference Adams, Figueroa and Hatsu20). Considering the fact that F&V intake can be correlated with economic and social status as well as cultural patterns in an environment(Reference Msambichaka, Ezel and Abdul9), appropriate cultural intervention is needed to target existing barriers to healthy diet and awareness of nutritional guidelines(Reference Adams, Figueroa and Hatsu20). Psychologists have developed specific models and theories to explain the determinants of people's behaviours in order to understand their behaviours and choices of people in the aspects of everyday life such as nutrition; therefore, theories and models can help program developers to identify the most effective health-promoting behavioural determinants in a particular population(Reference Hung21). For instance, Pender's health promotion model (HPM) has developed to predict health behaviour and included three groups of the effective factors health-promoting behaviour: individual experiences and characteristics, specific behavioural emotions and cognitions, and behavioural outcomes(Reference Bahmanpour, Nouri and Naderiyan22). Although individual characteristics cannot be changed, other specific variables such as Behavioural perceptions and emotions can be changed through appropriate intervention, which results will be observed in Behavioural outcome including: commitment to planning and prioritisation of priorities and demands. In other words, Behavioural outcome will be the result of people's participation in health behaviour(Reference Pender, Murdaugh and Parsons23). Also, considering that Pender's HPM has an ecological approach to change behaviour and takes into account interpersonal, interpersonal, organisational and social factors, it can be helpful in identifying the effective factors in creating and maintaining this behaviour(Reference Pender, Murdaugh and Parsons24). Therefore, as a framework for planning health interventions, this model can be applied to improve health-promoting behaviour(Reference Bahmanpour, Nouri and Naderiyan22). Adults not only consume less fruit and fewer vegetables than recommended(Reference Zamanian, Paksereshet and Holakouie-Naeini11,Reference Esteghamati, Noshad and Nazeri25) but are also exposed to at least three out of five risk factors for chronic diseases, e.g. cardiovascular disease(Reference Samavat, Hojjatzadeh and Shams26); hence, it is necessary to design and validate a model-based appropriate instrument that would be able to make strong predictions about the factors affecting F&V intake behaviour. Given the protective effect of F&V intake against a variety of medical diseases, e.g. cardiovascular disease, it has been considered a public health priority in many countries(Reference Silva, Smith-Menezes and Duarte27). Therefore, the present study aimed to validate an instrument to measure the perception of effective factors on F&V intake based on Pender's HPM among in a group of nutritionists, health education and promotion and the public sector employees, the offices of Ghaemshahr city of Mazandaran province in Iran were conducted.
Methodology
Subjects
In this cross-sectional study, 11 health education and health promotion specialists in the Step of Content Validity and 495 employees of the public sector in different Steps of the study (qualitative face validity: n 10, quantitative face validity: n 30, reliability: n 30 and Construct Validity: n 425) participated (Fig. 1).

Fig. 1. Flowchart of steps of the study.
Steps of the study
The research spanned from 23 October 2018 to 23 July 2019 and in six steps: instrument development through literature review, face validity assessment, content validity assessment, reliability assessment, construct validity assessment and external validity.
Step 1 (instrument development)
In order to compile the instrument items, an extensive literature review was performed on F&V intake in Iran and abroad. Based on the appropriate items used in different instruments, a pool of questions was then prepared(Reference Gholami, Mohammadi and Pourashraf28–Reference Stables36). With the help of several health education and promotion experts, the new instrument items were finally designed in accordance with the constructs of Pender's HPM including the following factors: previous relevant behaviour, behaviour-related emotions, perceived barriers, perceived benefits, perceived self-efficacy, interpersonal influences, situational influences, commitment to action plan, immediate preferences and demand, motivational factors, and behavioural outcome. The items were then assessed on the four- and five-point Likert and Yes/No scales.
Step 2 (face validity)
Face validity was determined through qualitative and quantitative methods. First, ten people from the target group (government employees) were interviewed and asked to comment on the presence of difficult phrases, lexical ambiguity or different perceptions in each item of every construct and to express the appropriateness and coordination of items with the main purpose of each construct(Reference Polit and Beck37). After the views of the target group were collected, necessary changes were made in the items. To check face validity, the instrument was then provided again for thirty members of the target group, who were then asked to rate each item in terms of importance on the Likert scale (it does not matter at all; it does not matter; it almost matters; it matters and it matters very much) from 0 to 5. The impact scores for the importance of points 5 and 4 were then calculated separately through ‘importance × relative frequency [%] = the item impact score’. Finally, the mean impact score of each item was determined, and items with an impact score of lower than the cut-off point of 1·5 were removed from the instrument(Reference Sousa and Rojjanasrirat38).
Step 3 (content validity)
Validity analysis depends on the test content logical analysis which is examined in terms of compliance with scientific literature, the use of appropriate words, writing principles and correct position of each item. In other words, it answers the question whether the instrument content can measure the defined purpose(Reference Streiner, Norman and Cairney39). Therefore, if there is an agreement between individuals on validity, the instrument has content validity. In the present study, content validity was assessed through qualitative and quantitative methods. In the qualitative method, the instrument was sent to eighteen health education and promotion and nutrition experts for a careful review. Fourteen experts returned their written views. The quantitative method was employed to ensure the selection of the most important and correct content for the items regarding measurement of the intended objectives. Therefore, the content validity ratio (CVR) and the content validity index (CVI) were used. For this purpose, each research item was evaluated by eleven health education and promotion experts who had already announced their cooperation, based on a three-point Likert scale (1: necessary, 2: not necessary but useful and 3: not necessary). The CVR numerical value for each item was then determined through the following formula and the Lawshe table (Table 1).

Table 1. The minimum acceptable content validity ratio (CVR) based on the number of participating experts to determine validity
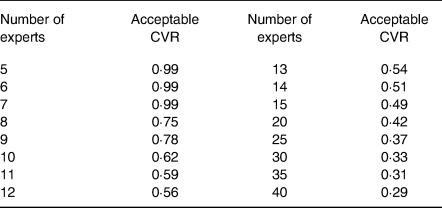
According to the number of experts and the Lawshe table, a CVR of ≥0·59 was approved. To determine the CVI, the experts evaluated each item in terms of three criteria, i.e. simplicity, relevance and clarity, on a four-point Likert scale (1: quite simple, 2: simple, 3: relatively simple, 4: not simple; 1: fully relevant, 2: relevant, 3: relatively relevant, 4: irrelevant;1: fully clear, 2: clear, 3: relatively clear, 4: unclear). The CVI was then calculated for each item considering the total number of selected options of completely agree and agree with each of the three criteria (i.e. completely relevant and relevant) according to the following formula:

In this study, a CVI score of >0·79 was considered appropriate, whereas scores between 0·70 and 0·79 were questionable. Hence, each relevant item was reviewed and corrected according to the opinions and suggestions of experts, and scores <0·70 were not accepted, while the relevant items were removed from the instrument(Reference Zhang, Liang and Chen40,Reference Rothman, Gnanaskathy and Wicks41) . After the problematic items were reviewed, corrected and deleted, the modified instrument was provided for the experts, and their CVR and CVI were recalculated.
Step 4 (reliability)
Regarding internal stability or reliability, most instruments have different scales and dimensions; therefore, it must be ensured that the subscale items are homogeneous and measure similar properties(Reference Hajizadeh and Asghari42). Therefore, the instrument was provided for thirty members of the study target group (government employees). After each item was answered on four- and five-point Likert and Yes/No scales, the internal consistency of each construct of Pender's HPM was measured through Cronbach's alpha in SPSS 22. Since the reliability of at least 70 % is desirable in scientific references, a minimum score of 70 % was also accepted as the instrument reliability(Reference Hajizadeh and Asghari42).
Step 5 (construct validity)
Factor analysis is an important method for evaluating construct validity to determine the predictability of variables(Reference Polit and Beck37); therefore, the sample size in this method should include three to fifty people per item according to Knapp and Brown(Reference Knapp and Brown43). Since a total of 118 items existed in the original research instrument, 3 people were selected for each item. Given a possible attrition rate of 20 %, 425 people were selected as the sample size. The subjects were selected through the random cluster sampling method. For this purpose, fifteen offices (about one-third of the offices) were randomly selected as clusters from the Governmental offices of Ghaemshahr, Mazandaran Province, Iran. These offices included Environment, Telecommunications, Technical and Vocational, Governor's office, Electricity, Red Crescent, Foundation, Agricultural Jihad, Civil and Personal status Registration, Document Registration, Labor and Cooperation, Sports and Youth, Roads and Urban Development, Industry and Mining and Social Security. The selected offices were located in different areas of the city with a variety of jobs and in turn differences in the amount of payment as a monthly salary. The individuals were then selected through the simple random sampling method from the designated offices. Inclusion criteria were employment in the designated offices and willingness to participate in the study after being reassured of information confidentiality. The exclusion criterion was reluctant to continue cooperation in completing the questionnaire or incomplete completion of questionnaire. There was no compulsion on participating in the study by the researcher or the heads of the offices. The participants responded to the perceived factors affecting the F&V intake behaviour questionnaire based on Pender's HPM with eleven constructs along with items of the knowledge section and socio-demographic characteristics in the self-report manner and due to the high number of instrument items, were collected after a few days (3–5 d).
Research instrument properties
The questionnaire consisted of the following components:
1. Socio-demographic characteristics included items about age, gender, education, etc.
2. Knowledge section aimed to determine the knowledge of individuals about the daily amounts and health benefits of F&V intake by choosing the correct option with a score of one. Based on the average number of correct knowledge answers, individuals were assessed with six items in score range 0–6.
3. Previous relevant behaviour intended to examine the previous relevant F&V intake behaviour and habits as well as their frequency during at least the past 1 month. This component had eight items designed on a four-point Likert scale (0: never and 3: always) in score range 0–24.
4. Perceived self-efficacy pertained to the competence of individuals to organise and perform the F&V intake behaviour as well as self-confidence in successfully performing this health behaviour. This component had eleven items designed on a five-point Likert scale (0: strongly disagree and 4: strongly agree) in score range 0–44.
5. Behaviour-related emotions pertained to abstract feelings and emotions that occurred before, during and after the F&V intake behaviour. This component had ten items designed on a five-point Likert scale (for items with a positive response, 0: never and 4: very much; and for items with a reverse negative response, 4: never and 0: very high) in score range 0–40.
6. Perceived benefits pertained to the perception of positive or reinforcing results of the F&V intake behaviour. This component had seven items designed on a five-point Likert scale (0: strongly disagree and 4: strongly agree) in score range 0–28.
7. Perceived barriers pertained to the perception of barriers, difficulties and personal costs regarding the F&V intake behaviour. This component had seventeen items designed on a five-point Likert scale (4: never and 0: very much) in score range 0–68.
8. Interpersonal influences included expectations or encouragement of other people about the F&V intake behaviour, designed in two separate sections. The first section pertained to the statements about expectations or encouragement of different people about the F&V intake behaviour, while the second section concerned the importance of people's opinion regarding the decisions made to perform the F&V intake behaviour. This component had seven items in each section designed on a five-point Likert scale (0: not at all and 4: always) in score range 0–56.
9. Situational influences pertained to perceptions about the ability of the living environment (situations, places and social events) to perform the F&V intake behaviour, designed in three separate sections. The first section consisted of four items, designed on a five-point Likert scale (0: never and 4: very much) about the effects of situations such as training classes or media on the desire to consume fruits and vegetables. Each of the second and third sections had seven items, designed on a five-point Likert scale (0: never and 4: very much) about the effects of different places and social events on the F&V intake behaviour in score range 0–72.
10. Motivational factors referred to factors (external and internal stimuli) that motivated people to perform F&V intake behaviour. This component had nine items, designed on a five-point Likert scale (0: not important at all and 4: very important) in score range 0–36.
11. Commitment to the action plan pertained to commitment to the F&V intake behaviour; this component had four items (two for fruit intake and two for vegetable intake), designed on the Yes/No and the three-point Likert scale (0: not at all and 2: very much) in score range 0–6.
12. Immediate preferences and demand included food preferences in case of simultaneous access to fruits, vegetables and other foods. This component had eight items, designed on the Yes/No scale in score range 0–8.
13. Behavioural outcome referred to the final desired behaviour or consequence of the decision and readiness for action on F&V intake. This component had six items, designed on a 5-point Likert scale (0: not at all and 4: always) in score range 0–24. The score range in the instrument was 0–412.
To confirm the construct validity, the variables with an internal correlation were grouped through exploratory factor analysis. For this purpose, the two indicators of Kaiser-Meyer-Olkin (KMO) and Bartlett's test of sphericity were employed to evaluate data appropriateness for factor analysis. KMO is a test that checks the sample size adequacy. It varies between zero and one. The closer the resultant number to one, the more probable the sample size adequacy for factor classification is to be confirmed. The Bartlett's test of sphericity determines whether the obtained correlation matrix is significantly different from zero; in other words, it analyses the existence of correlation between the instrument items for their integration(Reference Blunch44,Reference Mucci, Rucci and Rocca45) . After the correlation matrix of variables was created, the factors were extracted through principal component analysis (PCA) with varimax rotation. Finally, the highly correlated variables were placed in a group or factor. For better results, a cut-off point of 0·40 was used for high correlation between research variables. The exploratory factor analysis was performed in SPSS 22.
Step 6 (external validity)
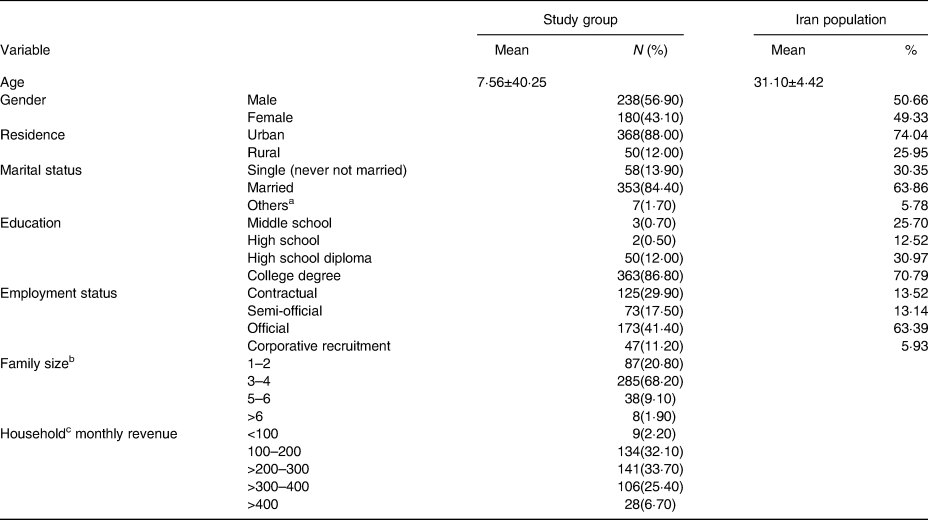
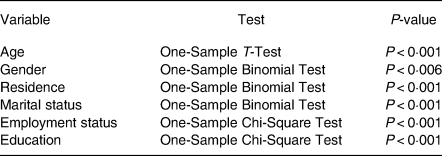
External validity is used to examine whether the results obtained from the internal validity of the instrument can be generalised to a similar group to the study group or a larger group. Because an instrument may have good internal credibility but not be generalisable to larger groups or communities(Reference Hajizadeh and Asghari46). Therefore, in the present study, the demographic characteristics of the target group with the general population characteristics of Iran (Table 3), which were extracted from the results of the latest population and housing census in the country(47) based on One-Sample T-Test, One-Sample Binomial Test and One-Sample Chi-Square Test were compared and analyzed.
Ethics
This study was approved by Isfahan University of Medical Sciences with number 398521and ethics code IR.MUI.RESEARCH.REC.1398.465. All participants in this study completed and signed the consent form before participating in the various steps of the study.
Results
Step 1 (instrument development)
A total of 112 items were designed for the primary instrument. Out of 112 items, 8 pertained to the knowledge section, 9 to the construct of previous relevant behaviour, 11 to the construct of perceived self-efficacy, 9 to the construct of behaviour-related emotions, 9 to the construct of perceived benefits, 14 to the construct of perceived barriers, 14 to the construct of interpersonal influences, 11 to the construct of situational influences, 9 to the construct of motivational factors, 4 to the construct of commitment to action plan, 8 to the construct of immediate preferences and demand and 6 to the construct of behavioural outcome.
Step 2 (face validity)
According to the face validity test results, after the results of the interview with the target group were applied to correct and revise some of the items in the qualitative section of face validity (in terms of ambiguity, simplification and higher coordination of the items), an impact score of <1·5 cut-off point was obtained by one item in the quantitative part of face validity, one item in the knowledge section, and one and two items in the constructs of previous relevant behaviour and perceived benefits, respectively; 96·42 % of the items had an acceptable average impact score and 3·57 % of items dropout of the questionnaire. The highest mean impact score pertained to three items in construct of motivational factors with a total score of 2·5; the items were (1) ‘How important is healthiness to motivate you more to eat fruits and vegetables?’ (2) ‘How important is freshness to motivate you more to eat fruits and vegetables?’ (3) ‘How important is proper price to motivate you more to eat fruits and vegetables?’ The lowest mean impact score (0·40) pertained to one item in the construct of perceived benefits, which was ‘If I eat fruits and vegetables every day, I will be accepted by others’ (Table 2).
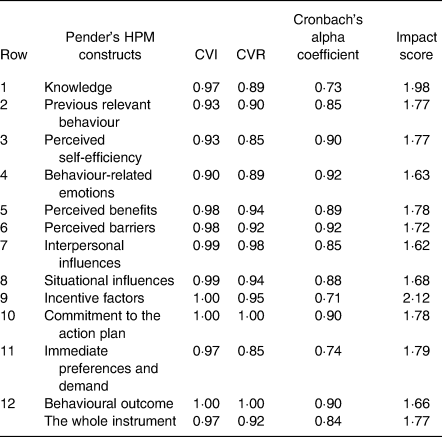
Table 2. The mean content validity ratio (CVR), content validity index (CVI), impact score and Cronbach's alpha coefficient of Pender's HPM constructs
Step 3 (content validity)
All opinions and corrective views of experts in the qualitative section of content validity were applied to the items. In the quantitative section, CVR and CVI showed that one item in the knowledge section, one item in the construct of previous relevant behaviour, two items in the construct of perceived benefits and one item in the construct of perceived barriers had CVR scores of <0·59. In addition, one item in the knowledge section and one item in the construct of perceived benefits had CVI scores of <0·70; therefore, these items were removed from the instrument. Moreover, one item in the construct of previous relevant behaviour and one item in the construct of behaviour-related emotions had CVI scores within the 0·70–0·79 range. Thus, these items were revised (Table 2). The mean CVR for all instrument items was 0·92. The highest mean CVR (1·00) pertained to the constructs of behavioural outcome and the commitment to the action plan, while the lowest (0·85) to the constructs of perceived self-efficiency and immediate preferences and demand (Table 3). The mean CVI for all instrument items was 0·97. The highest mean CVI (1·00) pertained to the constructs of motivational factors, behavioural outcome and commitment to the action plan and the lowest (0·93) to the constructs of previous relevant behaviour and perceived self-efficacy (Table 2). At the end of this step, 6·25 % of items dropout of the questionnaire.
Table 3. Demographic characteristics
a For example, divorced, widow, living apart from spouse.
b People.
c US$.
Step 4 (internal consistency)
Cronbach's alpha coefficient was applied to measure reliability. The results indicated that the reliability coefficient of the knowledge section was <0·70, which was unacceptable. Accordingly, an item efficient in reducing the reliability coefficient was removed, and Cronbach's alpha coefficient reached an acceptable level. Cronbach's alpha coefficient was acceptable for other constructs. The highest Cronbach's alpha coefficient (0·92) pertained to the constructs of behaviour-related emotions and perceived barriers, while the lowest (0·71) was related to the construct of motivational factors. Cronbach's alpha coefficient of the whole instrument was 0·84 (Table 2).
Step 5 (construct validity)
Analysis of Exploratory factor was performed on collected data from 418 questionnaires of the target group (government employees). The data of seven questionnaires were excluded due to incompleteness. The mean age of participants was 40·25 ± 7·56 years within the 26–60 range; other demographic characteristics are listed in Table 3.
A KMO index of 0·85 was considered for the sample size adequacy. It showed that the sample size was suitable for exploratory factor analysis. The Bartlett's test of sphericity was significant (P < 0·001, χ 2 = 87 985/874·87, df = 6903), showing a sufficient correlation between variables. According to the results of PCA with varimax rotation and minimum eigen value (Minimum one), 104 items were identified in the form of 15 factors extracted through exploratory factor analysis (Fig. 2). The perceived self-efficacy factor, accounting for 6·65 % of the model variance, was the strongest predictor and motivational factors (2), accounting for 2·43 % of the model variance, was the weakest predictor in the model. The factor loads of the items ranged from 0·40 to 0·83, and the cumulative variance for the whole model was 61·17 %. After factor analysis, reliability was calculated through the Cronbach's alpha coefficient for each factor. The factors behaviour-related emotions and perceived benefits had the highest Cronbach's reliability coefficient (0·96), while the factor behavioural outcome had the lowest Cronbach's reliability coefficient (0·72). The reliability coefficient for all factors was 0·96 (Table 4). At the end of this step, 11·86 % of items dropout of the questionnaire.
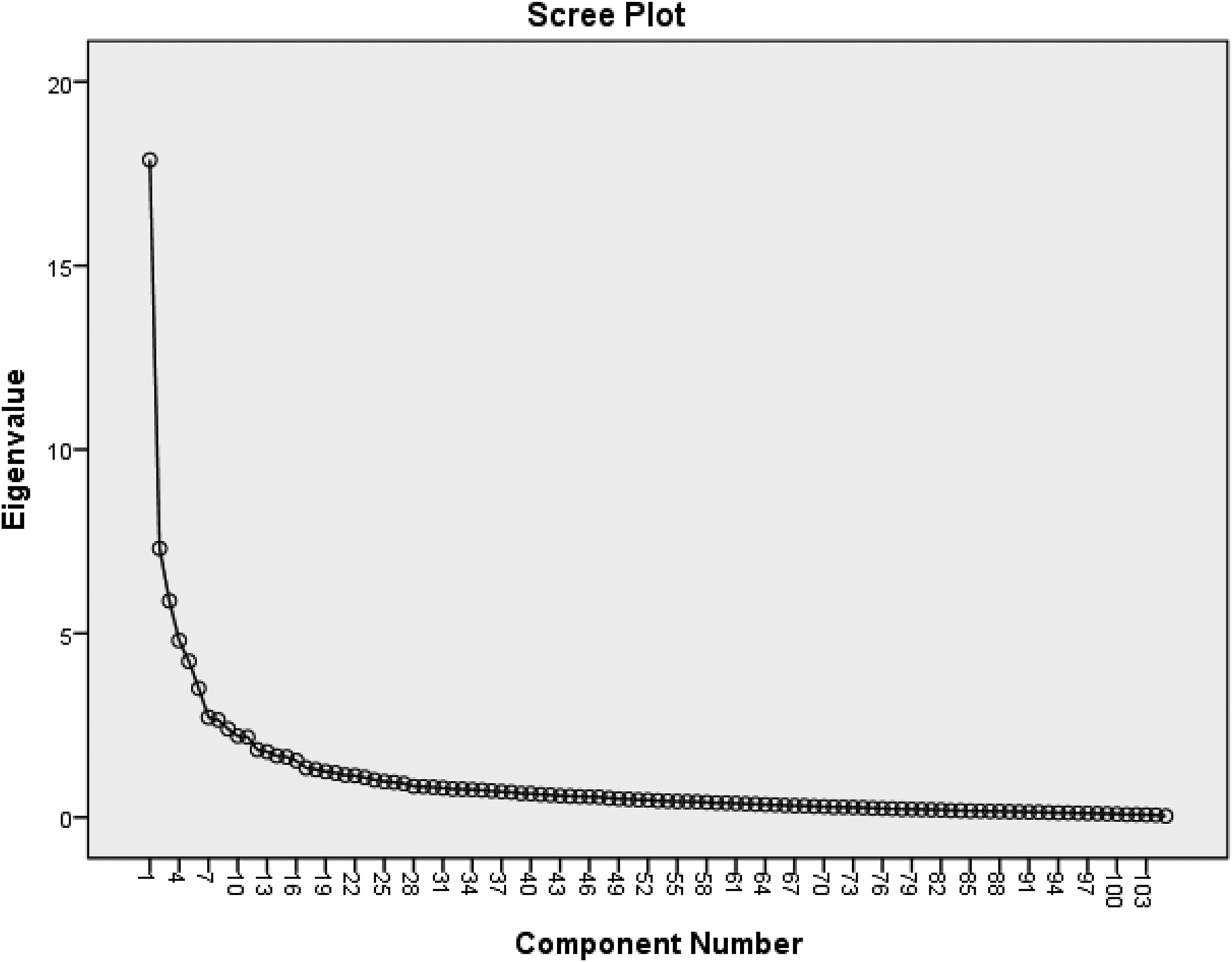
Fig. 2. Pebble chart for image of the eigen value in each of the extracted items.
Table 4. Factor loads extracted from exploratory factor analysis with varimax rotation

Step 6 (external validity)
There was no significant relationship between the demographic characteristics of the target group (government employees) and the general population of Iran (P < 0·001; Table 5).
Table 5. Investigating the relationship between the characteristics of the studied sample (government employees) and the general population of Iran
Discussion
One of the evaluated models in recognising behaviours and creating new behaviours is Pender's HPM(Reference Pepper48). According to this model, people commit to behaviours that the perceived benefits and self-efficacy of that behaviour are high and the perceived barriers are low(Reference Abbaszadeh, AlizadehEghdam and BadriGargari49). Strategies related to interpersonal and situational influences are also two important factors in behaviour change in Pender's HPM(Reference Bennie, Pedisic and Suni50). Interpersonal influencing factors include recognising the behaviours, beliefs or attitudes of others(Reference Khodaveisi, Omidi and Farokhi51). Family, peers, authorities and health-care providers are important interpersonal resources that can increase or decrease commitment to action(Reference Abbaszadeh, AlizadehEghdam and BadriGargari49). Interpersonal influences have indirect effect in addition to direct effect. Indirect effect is through social pressure or persuasion to commit to a plan of action(Reference Yang, Luo and Chiang52). Situational influence is an approach that not only assesses individual perceptions and cognition of each situation and context but also how to behave as a facilitator or barrier to behaviour and includes perceptions of existing options, wants and needs, and environmental characteristics(Reference Hsiao, Chien and Wu53). Which can be effective through an environment saturated with stimuli to perform the behaviours, such as a logo that represents the salient feature of a health behaviours(Reference Yang, Luo and Chiang52). Therefore, people should relate to and recognise health behaviours and direct them to their interpersonal interactions in order to act more in the direction of behavioural intention and to adapt themselves more to the cognitive symptoms related to the behaviour in question(Reference Zhang, Hu and Xing54). In this way, F&V intake as a health behaviour as well is influenced by a series of psychological, social and structural factors leading to certain beliefs and choices(Reference Zhang, Liang and Chen40). Considering people make food choices about 220 times a day(Reference Aida, Heather and Monique55), targeting individual, interpersonal and environmental factors to increase fruit and vegetable intake should be a priority for public health interventions(Reference Ziaei, Shahi and Dastgiri56). On the other hand, the value of educational programmes also depends on their effectiveness based on the appropriate utilisation of theories and models(Reference Pepper48). In this regard, the present study aimed to determine the validity and reliability of an instrument to assess the perceived F&V intake behaviour based on Pender's HPM. The initial instrument was developed with 112 items, which eventually increased to 118 items (before step 5: Construct Validity) because, according to experts and participants, some common items of the F&V intake behaviour with a higher importance for accurate response were divided into two separate items. The final instrument had acceptable content validity (CVR and CVI) and reliability scores. The mean impact score of all items was acceptable except for four items that were unable to gain the minimum acceptable mean impact score. This can be attributed to using qualitative methods in formal validity and applying the results on items before performing a quantitative step, something which could minimise difficulty, inconsistency or ambiguity in words and phrases of each item. This indicates that effective and timely determination of face validity and content validity, both qualitatively and quantitatively, can affect formulating and reviewing of the items and can hence have a valuable effect on the instrument design. The highest mean impact score pertained to the construct of motivational factors, which was added as a new construct to Pender's HPM. According to this construct, there are certain factors in the form of internal or external stimuli that can strongly motivating person to develop the desired health behaviour despite the existing barriers. Therefore, the construct of motivational factors had a special importance from the perspective of the study target group. CVR, CVI and reliability results indicated an optimal validity and reliability of the research instrument. Tajfard et al. conducted a similar study on nutritional behaviour of women based on Pender's HPM(Reference Tajfard, Vahedian Shahroudi and Esmaili57). The comparison of the results of that study with those of this one showed that the present study had a higher mean CVR in the constructs of previous relevant behaviour, perceived self-efficacy, interpersonal influences and behavioural outcome, a lower mean CVR in the construct of situational influences, and an equal mean CVR in the construct of commitment to the action plan. In addition, the present study had a higher mean CVI score in the constructs of perceived barriers, perceived benefits, interpersonal influences, situational influences and behavioural outcome, a lower mean CVI score in the constructs of perceived self-efficacy and behaviour-related emotions, and an equal mean CVI score in the construct of previous relevant behaviour. Regarding the instrument reliability, the present study had a higher Cronbach's alpha coefficient in the constructs of situational influences and behavioural outcome, a lower Cronbach's alpha coefficient in the constructs of previous relevant behaviour, perceived self-efficacy and perceived benefits, and an equal Cronbach's alpha coefficient in the construct of behaviour-related emotions. Eating habits are of special importance in the F&V intake(Reference Toft, Jakobsen and Aadahl58). Gholami et al. also showed that eating habits had the greatest impact on F&V intake(Reference Granner34). In the present study, the reliability coefficient of this construct was 0·85, which was optimal; however, it was lower than that of the Gholami (0·90) and Kasten (0·95) studies(Reference Kasten, Osch and Eggers19,Reference Gholami, Mohammadi and Pourashraf28) . Other models and theories have also been applied to develop instruments regarding the predictors of F&V intake such as the theory of planned behaviour and the stages of change model. For instance, Babazadeh et al. (Reference Babazadeh, Taghdisi and Sedgifard59) and Narimani et al. (Reference Narimani, Farmanbar and Mozaffari60) developed their instruments based on the theory of planned behaviour and the stages of change model with reliability coefficients of 0·82 and 0·87, respectively. Therefore, considering the reliability coefficient in the present study (0·84), it can be stated that the reliability scores of instruments in these studies developed through three different theories or models were approximately equal. In a study by Jung et al. on F&V intake, the constructs of the instrument developed based on the theory of planned behaviour had a Cronbach's alpha coefficient of 80–94(Reference Jung and Bice1). To determine the construct validity, the KMO index indicated the appropriateness of the sample size for exploratory factor analysis. In order to achieve better results in the present study, a cut-off point of 0·40 was used as a criterion for high correlation between items. The results demonstrated that the majority of items (88·13) had a high correlation and hence remained in the study, while 11·86 % of the items had a less correlation than the cut-off point and hence were removed. Extracted factors including: Factor 1 ‘perceived self-efficacy’ with 11 items, Factor 2 ‘perceived barriers’ with 15 items, Factor 3 ‘situational influences’ (1) with 10 items, Factor 4 ‘interpersonal influences’ (1) with 7 items, Factor 5 ‘motivational factors’ (1) with 7 items, Factor 6 ‘interpersonal influences’ (2) with 7 items, Factor 7 ‘behaviour-related emotions’ with 7 items, Factor 8 ‘perceived benefits’ with 7 items, Factor 9 ‘previous relevant behaviour’ with 8 items, Factor 10 ‘commitment to action plan’ with 4 items, Factor 11 ‘immediate preferences and demand’ with 6 items, Factor 12 ‘situational influences’ (2) with 4 items, Factor 13 ‘knowledge’ with 5 items, Factor 14 ‘behavioural outcome’ with 4 items and Factor 15 ‘motivational factors’ with 2 items. After exploratory factor analysis, some factors, including situational influences 1 and 2, interpersonal influences 1 and 2, and motivational factors 1 and 2, which had a common concept based on the main constructs of Pender's HPM, were combined. A total of twelve main factors were achieved. Optimal reliability of the factors, separately and in total, can be attributed to the formation and correct extraction of factors. At the same time, since these factors could contribute to 61·17 % of the total variance of the model, they have strong predictive effects on the model, e.g. referring to the extraction factor 4 and 6 as interpersonal influences 1 and 2, which could make up a total of 8·64 % of the total variance of the model, can indicate the predictive power of this construct in the present study in understanding consumer behaviour. F&V were in line with the results of a study by Delshad et al. In Tehran, Iran, which showed that government employees who had more interpersonal influence were more likely to engage in the health behaviour studied (stretching exercise)(Reference Delshad, Tavafian and Kazemnejad61). Accordingly, the results of Guadagnin et al. can be mentioned in relation to the importance of the construct validation for development of an accurate instrument. In the present study, 44 % of the main items about nutritional knowledge had low construct validity; therefore, they were not useful for evaluating the concepts of nutritional knowledge. This highlights the importance of construct validity(Reference Guadagnin, Nakano and Dutra62). Motivational factors were also analysed in the present study as a developmental construct in Pender's HPM. The results showed that this construct not only was accepted in face validity, content validity and reliability but also played a role in confirming the construct validity as two separate factors called motivational factors 1 and 2, contributing to 6·63 % of the total variance in the model. Therefore, it can be used along with other constructs of the model in future studies. Considering that one of the applications of exploratory factor analysis is to check the convergent validity of the items classified in each factor, so in the present study, the correlation coefficient of all extracted factor items was higher than the desired level of 0·4, which showed good internal consistency at the level of items of these factors(Reference Rubio, Berg-Weger and Tebb63). The results of external validity in the present study showed that the demographic characteristics of the study group are not homogeneous with the general population of Iran, thus the results of the present study cannot be generalised to the population of Iran, various reasons can explain this. First, the researcher selected a special study group (government employees) from the general population of Ghaemshahr to study, which usually includes a specific age group (24–55 years) and a large percentage of these people have a university degree and Also, due to being employed in offices, most of these people live in urban areas. Second, the study sample was selected from a city located in the north of Iran. The purpose of Instrument Validation was to use in this group and finally in the population of the city staff in future studies, so it is somewhat predictable that the capability. It does not have generalisation to the general population and especially to a larger society such as the population of Iran, which included different age groups and, in turn, the level of education, marital status and various employment status that were related to age groups. according to the latest study. In Mazandaran province of Iran, that people did not consume enough F&V(Reference Djalalinia, Saeedi Moghaddam and Sheidaei13), therefore effective and comprehensive interventions need to be planned and considered to improve that behaviour in that group. Because of the complexity of this behaviour, any intervention for changing F&V consumption should be planned and implemented based on understanding of determinants at both the environment and individual levels at first step. Hence, understanding the mediators that facilitate our target group in improving their F&V intake behaviour first step require a valid and reliable instrument. Thus, the present study aimed at design a reliable and valid instrument to measure determinants of F&V intake behaviour as the first step of a multi-phase intervention programme. Of course, after measuring the determinants of behaviour using designed instrument, F&V intake assessment using F&V frequency instrument before and after of effective interventions will be measured. In this time, we do not want to assess any relation between scores in the instrument and intakes of F&V.
Participation of a large number of government employees and diversity of the designated offices were considered the strengths of the present study. The offices were located in different geographical locations of the city, paid different salaries and differed in terms of extent and performance; therefore, their employees were characterised by a wide range of working conditions. The large number of the instrument items was one of the research limitations. This could reduce the accuracy of responses. In addition, since the employees were only available at working hours, they hardly accepted to participate in the study or completed the questionnaire on time.
Conclusion
In order to implement effective interventions for promoting health behaviour, it is necessary to identify the effective factors. This requires the use of appropriate, complete and accurate tools. As a result, time, accuracy and scientific principles for development and standardisation of instrument can guarantee the effectiveness of researchers’ attempts at promoting and enhancing the health of society. The research instrument can be used as a suitable instrument in future studies because it was developed in cooperation with health education experts and the target group (governmental employees) observing the scientific principles and gained desirable formal validity, content validity and reliability, and an acceptable construct validity through exploratory factor analysis.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/jns.2021.90.
Acknowledgements
This study was derived from a dissertation submitted in partial fulfilment of requirements for a PhD degree in health education and promotion with the approval number 398521 and ethics code IR.MUI.RESEARCH.REC.1398.465 in Isfahan University of Medical Sciences. The researcher would like to thank all the professors and participants including the experts of the Health Education and Promotion Group and government employees who helped implement this project.
All authors participated in the design of the study, in addition, F. K. H. was specifically involved in data collection and J. Y. was involved in data analysis. All authors participated in the preparation, interpretation and correction of the manuscript.
This project was financially supported by Esfahan University of Medical Sciences.
The authors declare that they have no conflict of interests.










 Open access
Open access