



Background
There is a well-known social gradient of cardiovascular disease (CVD) risk, where individuals with low socio-economic status (SES) display the highest risk factors for CVD compared to those with high SES(Reference McNamara, Balaj and Thomson1,Reference Stringhini, Carmeli and Jokela2) . Life expectancy, even within a city, can vary by 7–8 years between affluent and less affluent neighbourhoods(Reference Vale3). Differences in health behaviour can explain some of the observed socio-economic gradients in CVD risk. Being a male college student with low SES has previously been associated with unhealthy dietary habits that increase the risk of premature CVD(Reference Martinez-Lacoba, Pardo-Garcia and Amo-Saus4). One possible mediator between low SES, health behaviour and CVD risk is health literacy. Health literacy has been defined by Berkman et al. (Reference Berkman, Davis and McCormack5) as ‘the degree to which an individual can obtain, process, understand and communicate about health-related information needed to make informed health decisions’ (p. 16). Inadequate health literacy is strongly associated with low SES, poor health status, inactivity and overweight(Reference Svendsen, Bak and Sørensen6). Health literacy has also been found to partially mediate the association between low education and health status(Reference van der Heide, Wang and Droomers7), or, with other words, high education is associated with high health literacy(Reference Michou, Panagiotakos and Lionis8). Despite this, the prevalence of inadequate health literacy was high in a highly educated Danish adult population(Reference Martinez-Lacoba, Pardo-Garcia and Amo-Saus4). In a recent International Health Literacy Population Survey (2019–2021), 33 % of 6000 Norwegians had a score at or below level 1, meaning that they lack essential key knowledge and skills necessary to take care of own health(Reference Le, Finbråten and Pettersen9). Adults with low health literacy levels are more likely to use non-scientific information sources such as television, social media, blogs or celebrity webpages than medical websites for health information(Reference Chen, Hay and Waters10). The widespread use of such non-scientific medical health information among both young(Reference Klassen, Douglass and Brennan11) and older adults(Reference Chen, Hay and Waters10) could therefore put public health at risk(Reference Naeem, Bhatti and Khan12). Nutrition literacy (NL) can be regarded as a sub-category of health literacy and involves functional skills (such as knowledge of dietary recommendations), interactive skills (the ability to communicate about nutrition and to translate nutrition knowledge into positive dietary choices), and critical NL including the ability to distinguish evidence-based nutrition information from alternative facts, among other aspects(Reference Krause, Sommerhalder and Beer-Borst13,Reference Velardo14) . Interactive NL is less developed(Reference Krause, Sommerhalder and Beer-Borst13), and thus the aim of the present study was to describe aspects of functional and critical NL among university students and employees and investigate possible associations with gender, age, body mass index (BMI), total cholesterol and field of study/work.
Method
Study design
In this cross-sectional study, we assessed demographics, two accessible CVD risk factors (BMI based on self-reported weight and height and point-of-care total cholesterol measurements) and aspects of functional and critical NL in students and employees at Oslo Metropolitan University (OsloMet), Norway. The data collection took place at two different campus locations for four consecutive days.
Study sample
The study was advertised through the university web page and social media. Subjects who were pregnant, lactating or used cholesterol-lowering medication were not permitted to participate. In total, 548 university students and employees measured total cholesterol level, and 97 % (N 534) who also responded to the questionnaire were included in the study (Table 1). Participation was voluntary, and all participants gave verbal and written informed consent to the study.
Table 1. Background characteristics of the participants (N 534)
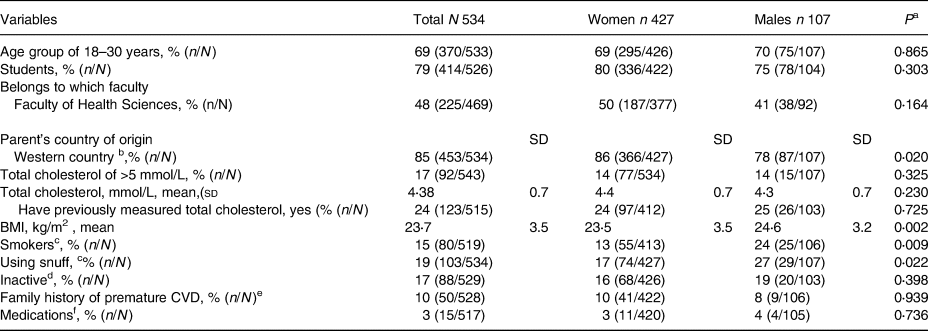
BMI, body mass index; n/N: n for the category sample and N for the total sample.
a P-value between genders using Pearson's χ 2 for categorical variables and independent sample t-test for total cholesterol and BMI.
b At least one parent born in Western countries
c Smokers/using snuff = daily + occasional.
d Inactive=rarely or <1 time per week.
e Premature CVD = ≤55 years for men or ≤65 years for women among first degree relatives.
f Blood pressure lowering, diabetes medication and/or anticoagulating agents.
Ethical approval
The study was approved by the Regional Ethical Committee of South-East with reference 2019/884 and the Norwegian Center for Research Data with reference 956205.
Questionnaire
All participants completed a questionnaire with two parts: part 1 covered questions on age, gender, body weight and height, smoking habits, physical activity level, field of study/work (all self-reported) and measured total cholesterol level (registered in the questionnaire by study personnel) in addition to other background questions that are not presented herer. All questions except the field of study/work and years of education had previously been used in a similar setting in pharmacies among 18- to 90-year-old adults(Reference Svendsen, Jacobs and Royseth15).
Part 2 coveredtwelve questions regarding NL. The questions were selected from a validated Swiss short food literacy questionnaire by Krause et al. (Reference Krause C, Beer-Borst and Sommerhalder16) (functional NL, see Table 2) and a validated Norwegian NL questionnaire by Guttersrud et al. (Reference Guttersrud, Dalane and Pettersen17) (critical NL, see Table 3). The Swiss questionnaire was translated to Norwegian by the research team, and some statements were changed to fit a Norwegian setting, whereas the questions in Norwegian remained unchanged. Six of the items that were taken from the Swiss questionnaire (NL1–NL6) focused on ‘functional NL skills’, such as the ability to obtain, process and understand basic nutrition information(Reference Krause C, Beer-Borst and Sommerhalder16), whereas six items from the Norwegian questionnaire (NL7– NL12) focused on ‘critical NL’(Reference Guttersrud, Dalane and Pettersen17). Likert scales with four or five categories were used in both the original questionnaires, but the response categories in the present study were reduced to two options: 0 ‘disagree’ and 1 ‘agree’ to reduce the respondents’ load with filling in the questionnaire.
Table 2. Responses to functional NL statements by gender
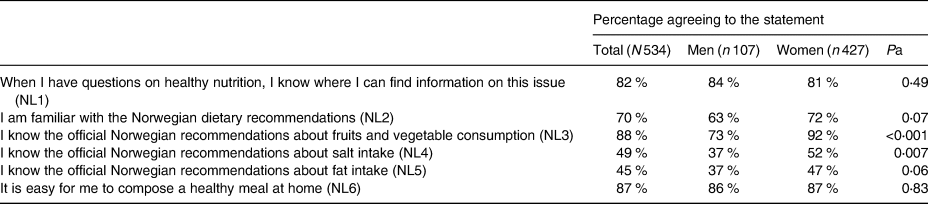
NL; nutrition literacy.
a P-value between genders using Pearson's χ 2. Questions NL1–NL6 were adapted to the Norwegian setting from Krause et al. (Reference Krause C, Beer-Borst and Sommerhalder16)
Table 3. Responses to critical NL statements by gender
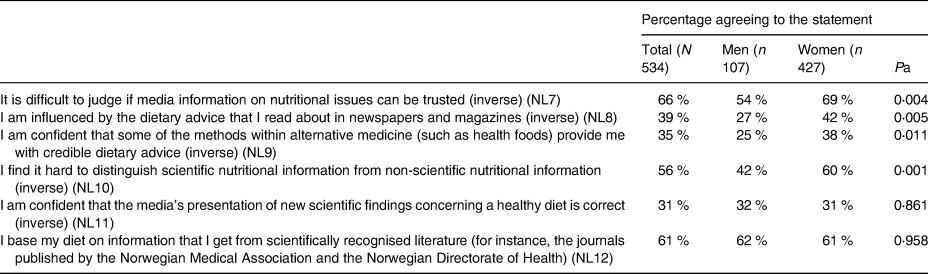
NL; nutrition literacy.
a P-value between genders using Pearson's χ 2. Questions NL7–NL12 were obtained from Guttersrud et al. (Reference Guttersrud, Dalane and Pettersen17) Inverse means that ‘agreeing’ indicates lower NLs.
Total cholesterol measurement
We assessed total cholesterol levels in students and employees, as this is an important CVD risk factor that, at the same time, is easy and cheap to measure(Reference Svendsen, Jacobs and Royseth15,Reference Catapano, Graham and De Backer18) . Total cholesterol was measured using finger-prick samples and the device Accutrend Plus (Roche Diagnostics) by trained study personnel. The measurement device captures total cholesterol levels in the range of 3⋅88–7⋅76 mmol/l. Values below 3⋅88 mmol/l were shown and reported as ‘low’ to the subjects and registered as 3⋅9 mmol/l, whereas values above 7⋅76 mmol/l were shown and reported as ‘high’ and registered as 7⋅8 mmol/l. After the measurements, all subjects received information on the impact of lifestyle on cholesterol levels verbally and, if they wanted more information, they received a brochure with healthy lifestyle advice. Subjects with total cholesterol of 7 mmol/l or higher were also advised to measure their total cholesterol level again during their next visit at their general practitioner.
Statistics
Background data and functional and critical NL were presented stratified on gender and as means and standard deviations or % and n/N, and gender differences were tested using the χ 2 test or the independent sample t-test.
The six functional NL questions (NL1–NL6, see Table 2) were found to have an adequate internal consistency, where the Kuder–Richardson 20 Test (KR20) (which is equivalent to Cronbach's α but for dichotomous variables) showed a KR20 reliability coefficient of 0⋅711. Thus, these questions were summarised into a functional NL scale. The critical NL questions, on the other hand, had a low KR20 reliability coefficient (0⋅445) and could therefore not be summarised to a score, and the items were examined separately in descriptive analysis.
For the functional NL scale, each affirmative answer to the statements (see Table 2 for statements) was given one point. The scale was thus from 0 to 6, where 6 was regarded as having the highest functional NL. The bivariate association between potential predictors and the functional NL scale was assessed using Spearman's correlation. Variables with a significance level of P ≤ 0⋅1 were included in an ordinal regression model to assess factors predicting functional NL. Data were analysed using SPSS Statistics 26 and STATA SE version 16.1.
Results
Background characteristics
Of the total sample of 534 students and employees, most (80 %) of the samples were female students in the age group of 18–30 years. Mean total cholesterol level and BMI were within the normal range in both men and women, but there were a higher proportion of men (27 %) than women (17 %) who used snuff and/or smoked (24 v. 13 %) (Table 1).
Functional NL skills (NL1–NL6)
Of the total population, 82 % agreed to the statement that they knew where to find information on healthy nutrition issues (NL1). Furthermore, 70 % reported that they were familiar with the Norwegian dietary recommendations (NL2). Among specific food or nutrient recommendations, the majority (88 %) agreed that they were familiar with the recommendation about fruit and vegetable consumption (NL3), whereas the recommendation for salt intake (NL4) and fat intake (NL5) was less known (49 and 45 %, respectively). There was a higher proportion of women than men that reported to be familiar with all the specific nutrient recommendations (Table 2).
Bivariate analysis showed a positive correlation (P < 0⋅02) between the functional NL score and being female, above 30 years, being an employee (v. a student), studying or working at the Faculty of Health Sciences, being from a Western country, having a cholesterol level above 5 mmol/l, being a non-smoker and being physically active at least three to four times per week (data not shown). Having a BMI above 25 kg/m2 was however not associated with the functional NL score (and therefore not included in the ordinal regression model).
When controlling for the other variables in an ordinal regression model, being a student or employee at the Faculty of Health Sciences was associated with a higher likelihood of having a higher functional NL score (OR 1⋅50, 95 % CI 1⋅06, 2⋅11). Whereas males (OR 0⋅64, 95 % CI 0⋅42, 0⋅99), those 30 years of age and below (OR 0⋅39, 95 % CI 0⋅23, 0⋅65) and those being physically active less than three times per week (OR 0⋅05 95 % CI 0⋅35, 0⋅71) had significantly lower odds ratios for having a higher category of functional NL (Table 4).
Table 4. Factors associated with functional NL score (N 534)a
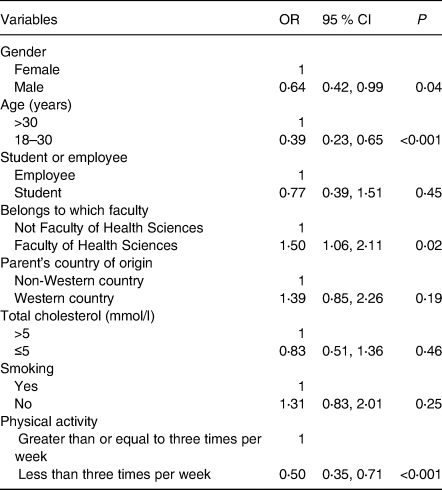
a Adjusted odds ratios (OR) were derived from ordinal regression analysis in which each OR was adjusted for all other factors listed. An OR greater than 1 indicates that subjects with the characteristics have a higher likelihood of having a higher category of functional NL score.
Critical NL skills (NL7–NL12)
As shown in Table 3, as many as 66 % of university students and employees agreed that they found it difficult to judge if information on nutritional issues from the media could be trusted (NL7), with a higher proportion among women (69 %) than men (54 %). Similarly, considerably more women (60 %) than men (42 %) found it hard to distinguish between scientific and non-scientific information about diet (NL10). With no gender difference, 31 % were confident that the ‘media's presentation of new scientific findings concerning a healthy diet is correct’ (NL11), whereas significantly more women (42 %) than men (27 %) agreed that they ‘let themselves be influenced by the dietary advice that they read about in newspapers’ (NL8). In total, 61 % stated that they ‘base their diet on information that they get from scientifically recognized literature including the national dietary recommendations’ (NL12). Nevertheless, a significant proportion of women (38 %) compared to men (25 %) agreed that alternative medicine could also provide credible dietary advice (NL9) (Table 3).
Straified into age groups, there was a larger proportion of ‘older' 31- to 70-year-old men (41 %) who stated that they were influenced by diet advice in the newspapers compared to those aged ≤30 years (younger) (21 %) (P 0⋅040). Concurrently, there was a lower proportion of older women (52 %) than younger women (63 %) who found it hard to distinguish between scientific and non-scientific nutrition information (P 0⋅022). No other differences in age groups were reported.
Discussion
Most of the students and employees at a Norwegian university reported that they knew where to find information on nutrition issues and that they were familiar with the national dietary guidelines, indicating adequate functional NL skills. There seemed to be a lower proportion of men than women, agreeing that they were familiar with specific dietary recommendations, and being male mas associated with lower odds of having a high functional NL score. On the other hand, more women than men stated that (1) they were influenced by advice from the media and (2) they found it hard to distinguish between scientific and non-scientific nutrition information (critical NL).
Functional NL
As many as 70 % of university students and employees reported to be familiar with the national dietary guidelines, mirroring what has been found in national surveys by the Norwegian Health Directorate(19). The population overall seemed to be more familiar with the recommendations for fruits and vegetables than for the recommendations for intake of salt and fat, which is supported by Worsley et al. (Reference Worsley, Wang and Byrne20). Nonetheless, the 30 % that disagreed, and were not familiar with the national dietary recommendations, could imply that even among university students and employees, there is a group that seemed to be resistant to the mass of nutrient and diet communication(Reference Worsley, Wang and Byrne20). This warrants further studies to describe other characteristics with these students and employees. In the present study, we did not evaluate food literacy, which includes skills, such as to what degree can you apply the information for instance in regard to preparing food and ability to pick the healthy foods in the store(Reference Krause, Sommerhalder and Beer-Borst13). Hence, although 70 % of the samples agree that they are familiar with the dietary recommendations, it cannot be translated to percent agreeing to follow the dietary guidelines. From a public health perspective, it is also challenging that many consumers choose less healthy eating options without being aware that it is in fact the less healthy option(Reference van Buul, Bolman and Brouns21).
We found that being female, having a higher age, studying or working at the Faculty of Health Sciences, and being more physically active were significant predictors of higher levels of functional NL in our sample of university students and employees. Supporting our findings, an Australian study found that higher age, female gender and university education were among the major predictors of higher nutrition knowledge score(Reference Worsley, Wang and Byrne20). However, high education does not automatically imply high nutrition or health literacy; a population study among Danes found that despite being a relatively highly educated group of individuals, the prevalence of inadequate health literacy was high(Reference Svendsen, Bak and Sørensen6). In our study, being overweight, having a higher total cholesterol level and being a smoker did not seem to impact the functional nutrition knowledge score. In comparison, overweight but not smoking was associated with low health literacy in the Danish adults(Reference Svendsen, Bak and Sørensen6). These diverging findings could partly be due to our population being healthier than in the Danish study: in both students and employees, BMI and total cholesterol level were on average within the recommended levels. The prevalence of smokers and those who used snuff were also in line with the general Norwegian population as reported by Statistics Norway(22).
Critical NL
We also assessed aspects of critical NL, which implies that one is able to judge nutrition information, and to critically reflect on the factors that influence dietary behaviour for the individual and the society(Reference Krause, Sommerhalder and Beer-Borst13). We found that 82 % agreed that they knew where to find information about healthy nutrition. In comparison, a considerable proportion (37 %) found it challenging to find health-promoting information, which is in line with the results in a recent report on health literacy level in a representative sample of the Norwegian population(Reference Le, Finbråten and Pettersen9). Furthermore, about 30 % of both men and women reported that they were ‘confident that the media's presentation of new scientific findings concerning a healthy diet is correct’, which could be worrying considering the other finding that 56 % of the same population of highly educated women and men had problems in distinguishing between scientific and non-scientific nutrition information. Supporting this result, a large proportion of the previously mentioned comparable Norwegian population found it challenging to assess whether they could trust information from the mass media about diseases (55 %) and health risks (49 %)(Reference Le, Finbråten and Pettersen9).
We observed several gender differences in the assessment of critical NL. First, there was a significantly higher frequency of women (60 %) than men (42 %) who found it hard to distinguish between scientific and non-scientific information about diet. Next, more women than men responded that they were influenced by dietary advice presented in the media (42 v. 27 %, respectively) and found alternative medicine advice to be credible (38 v. 25 %, respectively). Since only 20 % of the study samples were men, these observed gender differences warrant further studies. The newly published report on the Norwegian population's health literacy level(Reference Le, Finbråten and Pettersen9) showed that only 20 % reached a high level of general health literacy (covering aspects such as find, understand, assess and use health-related information). Furthermore, that women and those with an education above upper secondary level had slightly better skills(Reference Le, Finbråten and Pettersen9)An assessment of the population's NL level still remains to be elucidated in Norway.
Strengths and limitations
The major strength of our study was that we were able to include a considerable proportion of students and employees during one week of recruitment. This was probably due to the low threshold for participation on different university campus locations and the inclusion of total cholesterol measurements. Although we attempted to include students and employees from several fields of study, the majority of the final sample belonged to the Faculty of Health Sciences. Furthermore, 80 % were females, and mean total cholesterol levels and BMI were within the normal range, indicating that we included a health-conscious sample.
There are some limitations with the NL questions (part 2 of the questionnaire). First, the questionnaire concerning NL has not been validated but was rather combined by selected questions from two validated questionnaires(Reference Krause C, Beer-Borst and Sommerhalder16,Reference Guttersrud, Dalane and Pettersen17) . Secondly, the critical NL questions could be directly used since the questionnaire was in Norwegian(Reference Guttersrud, Dalane and Pettersen17), but the functional NL questions selected from a questionnaire by Krause et al. (Reference Krause C, Beer-Borst and Sommerhalder16) had to be translated. The latter questions(Reference Krause C, Beer-Borst and Sommerhalder16) were not back-translated after having been translated to Norwegian. Furthermore, in the present study there were only two response categories (agree or disagree), whereas the original questionnaires had five response categories. Hence, there might have been nuances that we did not capture. These are limitations that should be taken into account when interpreting the results. Furthermore, for future studies, a tool covering all three NL domains should be developed and validated in Norway, preferable using Rasch modelling(Reference Guttersrud, Dalane and Pettersen17).
Conclusion
We found that university students and employees appeared to have a relatively high functional NL knowledge (e.g. of dietary guidelines and where to find nutrition information) and that predictors of a higher functional NL score were being female, having higher age, being physically active and affiliated with health sciences. Whereas the main challenge, particularly among women, seemed to be in the critical NL domain such as difficulties in distinguishing between scientific and non-scientific information about diet, despite that 50% of the sample was affiliated with health sciences. The present study therefore calls for a thorough assessment of functional and critical NL levels among university students and employees. If our present results are verified, actions to increase critical NL levels to avoid misinformation among university students and employees should be taken.
Acknowledgments
We thank Ellen Raael for contributing to the data collection. We also thank students and employees at OsloMet for participating in the study.
V.F., A.S., K.S., V.H.T.H. and M.C.W.M. were responsible for data collection. K.S., L.E.T., V.F., A.S., M.C.W.M. and V.H.T.H. had the responsibility for analysing and interpreting the data. K.S. wrote the manuscript draft in collaboration with V.H.T.H. and L.E.T. All authors gave critical comments to the interpretation of the results and to the manuscript, and all authors have read and approved the final version of the manuscript.
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects/patients were approved by the Regional Ethical Committee of South-East with reference 2019/884 and the Norwegian Center for Research Data with reference 956205. Written informed consent was obtained from all subjects/patients.
The study material needed for the total cholesterol measurements was covered by OsloMet, whereas the National Advisory Unit on Familial Hypercholesterolemia contributed with the healthy lifestyle brochures.
L.E.T., V.F., A.S. and I.N. declare no conflict of interest. K.S. has received honoraria from Sanofi and Amgen for lectures. K.R. reports personal fees from Akcea, Amgen, Mills DA, Norwegian Directorate of Health, Sanofi, Sunnovion and Novartis. M.P.B. reports personal fees from Amgen and Sanofi. K.B.H. reports grants and/or personal fees from Tine SA, Mills DA, Olympic Seafood, Amgen, Sanofi. M.C.W.M. is involved in projects with research grants from industrial partners and has received research funds from Mills AS. V.H.T.H. collaborates with and/or has received research grants from Mills AS, Mesterbakeren, Det Glutenfrie Verksted and Norwegian Celiac Disease Association. None of these findings are related to the content of this manuscript.





 Open access
Open access