



Introduction
Chronic otitis media is a chronic inflammation of the middle ear and mastoid cavity. It is a major health issue that presents as tympanic membrane perforation, recurrent otorrhoea and hearing loss. The aetiology of chronic otitis media is multifactorial: environmental, social, genetic, allergy-related, recurrent middle-ear infection, anatomical and functional factors are involved.Reference Bluestone1
The Eustachian tube has a vital role in maintaining middle-ear physiology. The major functions of the Eustachian tube are ventilation, clearance and protection of the middle ear. Eustachian tube dysfunction is an underlying cause of middle-ear diseases, for example otitis media with effusion, atelectasis and adhesive otitis media.Reference Seibert and Danner2,Reference Schilder, Bhutta, Butler, Holy, Levine and Kvaerner3 The anatomical features of the Eustachian tube are also associated with otitis media. Patients with craniofacial abnormalities and Down syndrome have a higher risk of middle-ear infections because of the shorter length and horizontal location of the Eustachian tube.Reference Verhoeff, van der Veen, Rovers, Sanders and Schilder4
Anatomical features affecting Eustachian tube functionality need to be clarified to understand the aetiopathology of chronic otitis media. Eustachian tube anatomy has been examined mostly in cadaver studies. Today, remarkable advances in computed tomography (CT) can provide better information on Eustachian tube anatomy, especially with the use of the multiplanar reconstruction technique.Reference Takasaki, Takahashi, Miyamoto, Yoshida, Yamamoto-Fukuda and Enatsu5
The Eustachian tube length, the angle of the Eustachian tube with the Reid horizontal plane, the tubotympanic angle and the Eustachian tube pretympanic diameter were measured in patients with chronic otitis media using the multiplanar reconstruction technique on temporal bone CT. To our knowledge, this is the first study to explore the effect of these four parameters on the development of chronic otitis media. Our aim was to clarify the relationship between the dimensions of the Eustachian tube and the aetiopathology of chronic otitis media.
Materials and methods
This study was approved by our institutional review board (protocol number: 28-2021) and performed according to the principles of the Helsinki Declaration. We retrospectively reviewed the data of 231 patients (124 female and 107 male) who were operated on for chronic otitis media, in a tertiary referral centre, between January 2016 and December 2021.
Patients aged 18–68 years with a diagnosis of unilateral chronic otitis media were enrolled in the study. All patients presented with tympanic membrane perforation, recurrent otorrhoea and hearing loss. The diagnosis of chronic otitis media was confirmed by otomicroscopy, pure tone audiometry and 0.5-mm thick multi-slice temporal bone CT imaging.
The diseased ears of all patients were included in group 1 and the contralateral healthy ears were included in group 2. Group 1 was separated into two subgroups: group 1A comprised ears that had chronic otitis media with cholesteatoma (n = 28) and group 1B included ears that had chronic otitis media without cholesteatoma (n = 203). The diagnosis of cholesteatoma was confirmed by intra-operative findings.
Exclusion criteria were: bilateral chronic otitis media, previous ear surgery, traumatic tympanic membrane perforations, tympanic membrane perforations without middle-ear or mastoid disease, craniofacial abnormalities, congenital ear deformities, Down syndrome, previous nasal surgery, allergic rhinitis, and malignant lesions of the paranasal sinuses and nasopharynx.
A multidetector CT system (Ingenuity Philips 128 CT Scanner, Philips Medical Systems, Cleveland, Ohio, USA) was used for imaging. The imaging parameters were as follows: slice thickness and reconstruction interval of 0.5 mm, 35 × 35 cm field of view and pitch of 1. No contrast material was used.
All the images were evaluated by two senior radiologists on an offline picture archiving and communication system. Each image was measured twice and the mean values were calculated for the statistical analysis. The multiplanar reconstruction technique was used for the reconstruction of 0.5-mm thick images. The standardisation of images was carried out for all patients by adjusting the angle of the reformatted image until the basal turns of each cochlea were viewed equally on the axial and coronal planes.
The anatomical parts of the Eustachian tube were defined as described in other studies.Reference Takasaki, Takahashi, Miyamoto, Yoshida, Yamamoto-Fukuda and Enatsu5,Reference Sadler-Kimes, Siegel and Todhunter6 The pharyngeal orifice of the Eustachian tube was defined as the point closest to the pharynx where a loop-shaped lumen appears, and the tympanic orifice of the Eustachian tube was defined as the closest point before the external auditory meatus appears on the cross-sectional image.
The length of the Eustachian tube, the angle of the Eustachian tube with the Reid horizontal plane, the tubotympanic angle and the Eustachian tube pretympanic diameter were measured using the same technique as previous studies.Reference Takasaki, Takahashi, Miyamoto, Yoshida, Yamamoto-Fukuda and Enatsu5,Reference Dinç, Damar, Uğur, Öz, Eliçora and Bişkin7–Reference Nemade, Shinde, Rangankar and Bhole9 Oblique multiplanar reconstruction images were used for measuring the length of the Eustachian tube. The tympanic and pharyngeal orifices of the Eustachian tube were observed in the same section in the coronal images, and the distance between them was measured as the length of the Eustachian tube (Figure 1). The angle of the Eustachian tube was defined as the angle between the longitudinal axis of the Eustachian tube and the Reid plane (Figure 2). The Reid plane is the horizontal plane crossing the bilateral superior wall of the external auditory meatus and the bilateral inferior orbital wall. The tubotympanic angle was defined as the angle between the line passing through the centre of the tympanic orifice of the Eustachian tube and the line passing through the centre of the bony external auditory canal (Figure 3). The pretympanic segment is the cone-shaped portion of the Eustachian tube next to the tympanic orifice. The tensor tympani muscle bulges into the lumen of the Eustachian tube and builds the roof of the pretympanic segment. The lumen of the pretympanic segment, which is located on the lateral side of the internal carotid artery and the cochlea, was clearly visible on the axial images (Figure 4).

Figure 1. The distance between the tympanic and pharyngeal orifices of the Eustachian tube was measured as the length of the Eustachian tube.

Figure 2. The angle of the Eustachian tube was defined as the angle between the longitudinal axis of the Eustachian tube and the Reid horizontal plane.

Figure 3. The tubotympanic angle was defined as the angle between the line passing through the centre of the tympanic orifice of the Eustachian tube and the line passing through the centre of the bony external auditory canal.
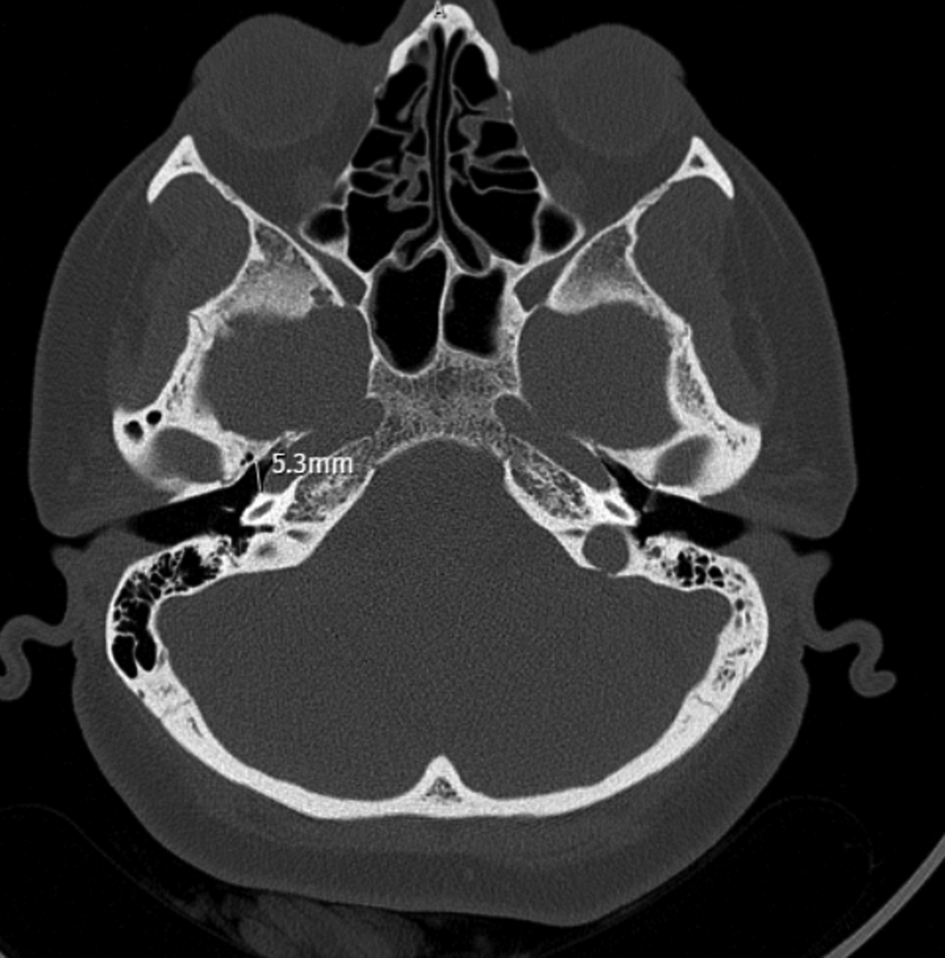
Figure 4. The pretympanic diameter of the Eustachian tube was measured on axial images.
Statistical analysis
Statistical analyses were performed using software SPSS 15.0 for Windows (SPSS, Chicago, Illinois, USA). Descriptive statistics were expressed as frequencies and percentages for categorical variables, and as mean (± standard deviation) or median (minimum–maximum) values for numerical variables. The chi-square test was used for the comparison of groups. In independent groups, the numerical variables with and without normal distribution were compared using the student's t-test and the Mann–Whitney U test, respectively. In dependent groups, a normal distribution was ensured and the numerical variables with normal distribution were compared using the paired t-test. P-values of less than 0.05 were considered statistically significant.
Results and analysis
A total of 231 patients were included in the study: 124 (53.7 per cent) were female and 107 (46.3 per cent) were male. The mean age was 34.1 ± 11.9 years, with a range of 18–68 years.
Based on middle-ear pathology, diseased ears were separated into two subgroups of chronic otitis media with cholesteatoma (group 1A, 28 ears) and chronic otitis media without cholesteatoma (group 1B, 203 ears). There were 11 female and 17 male patients in group 1A, with a mean age of 33.9 ± 10.9 years. There were 113 female and 90 male patients in group 1B, and the mean age was 34.1 ± 12.1 years. No significant difference regarding sex and age was found between these two subgroups (p = 0.103 and p = 0.933, respectively).
The length of the Eustachian tube in ears with chronic otitis media (23.3 ± 5.9 mm) was significantly shorter than that in healthy ears (24.4 ± 6.2 mm) (p < 0.001). The angle of the Eustachian tube with the Reid horizontal plane was significantly narrower in ears with chronic otitis media (21.6 ± 3.5°) versus healthy ears (23.7 ± 4.0°) (p < 0.001). The tubotympanic angle was significantly wider in ears with chronic otitis media (141.0 ± 9.2°) versus healthy ears (138.5 ± 9.8°) (p < 0.001). The Eustachian tube pretympanic diameter was significantly narrower in ears with chronic otitis media (4.21 ± 0.71 mm) versus healthy ears (4.64 ± 0.79 mm) (p < 0.001). The Eustachian tube dimensions of the diseased and healthy ears of all patients are listed in Table 1.
Table 1. Comparison of Eustachian tube dimensions in diseased and healthy ears
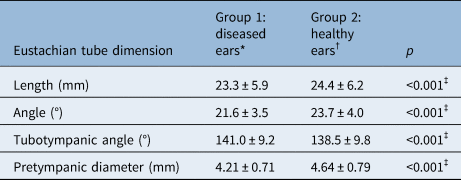
Data represent mean ± standard deviation values unless indicated otherwise. *n = 231; †n = 231. ‡Indicates statistically significant difference (p < 0.05).
When the Eustachian tube dimensions of groups 1A and 1B were compared, no significant differences were found between the two subgroups except for the tubotympanic angle, which was found to be significantly wider in ears with cholesteatoma (p = 0.028). The Eustachian tube dimensions of patients with chronic otitis media with and without cholesteatoma are listed in Table 2.
Table 2. Comparison of Eustachian tube dimensions in groups 1A and 1B
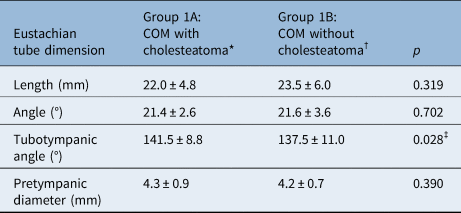
Data represent mean ± standard deviation values unless indicated otherwise. *n = 28; †n = 203. ‡Indicates statistically significant difference (p < 0.05). COM = chronic otitis media
Discussion
The aetiology of chronic otitis media is still unclear, and various theories have attempted to explain its pathogenesis. The environmental theory claims that factors such as recurrent middle-ear infections, low socioeconomic status and smoking are responsible for reduced temporal bone pneumatisation.Reference Bluestone1,Reference Verhoeff, van der Veen, Rovers, Sanders and Schilder4,Reference Bluestone, Paradise and Beery10 The genetic theory claims that temporal bone pneumatisation is genetically regulated, and poorly pneumatised ears are prone to chronic otitis media.Reference Seibert and Danner2,Reference Licameli11
Eustachian tube dysfunction is a major cause of middle-ear diseases such as otitis media with effusion (OME), atelectasis, and adhesive otitis media.Reference Seibert and Danner2,Reference Schilder, Bhutta, Butler, Holy, Levine and Kvaerner3 The anatomical features of the Eustachian tube are also associated with otitis media.Reference Verhoeff, van der Veen, Rovers, Sanders and Schilder4,Reference Licameli11 Variation in Eustachian tube dimensions may lead to poor ventilation of the temporal bone. We measured the Eustachian tube dimensions to clarify the relationship between the anatomy of the Eustachian tube and the aetiopathology of chronic otitis media.
Takasaki et al. measured the length of the Eustachian tube in healthy adults, healthy children and children with OME.Reference Takasaki, Takahashi, Miyamoto, Yoshida, Yamamoto-Fukuda and Enatsu5 The lengths of the Eustachian tube (mean ± standard deviation), for the right and left sides respectively, were 42.5 ± 2.8 mm and 42.9 ± 2.9 mm in adults, 37.5 ± 3.3 mm and 38.0 ± 3.2 mm in healthy children, and 37.2 ± 3.0 mm and 37.6 ± 3.2 mm in children with OME. The Eustachian tube was significantly longer in adults, but no significant difference in length was found between healthy children and children with OME. Hashimoto et al. evaluated the length of the bony segment of the Eustachian tube in 20 patients with middle-ear cholesteatoma and found no significant relationship.Reference Hashimoto, Yanagihara, Hyodo and Sakagami12 Dinç et al. measured the length of the Eustachian tube in 125 patients with chronic otitis media, tympanosclerosis, cholesteatoma and retraction pockets.Reference Dinç, Damar, Uğur, Öz, Eliçora and Bişkin7 The Eustachian tube length was: 39.3 ± 2.5 mm in normal ears, 37.9 ± 2.1 mm in patients with chronic otitis media, 38.5 (37.6–44.0) mm in those with tympanosclerosis, 41.5 (34.3–43.8) mm in patients with retraction pockets and 38.9 ± 2.2 mm in those with cholesteatoma. The Eustachian tube was found to be shorter in ears with chronic otitis media versus those with tympanosclerosis, in ears with chronic otitis media versus normal ears, and in ears with cholesteatoma versus those with retraction pockets. Gulustan et al. measured the length of the bony Eustachian tube segment in patients with cholesteatoma, and found a significant relationship between chronic otitis media with cholesteatoma and Eustachian tube length.Reference Gulustan, Gunes, Yildiz, Yazici, Abakay and Inci13 In our study, the length of the Eustachian tube in ears with chronic otitis media (23.3 ± 5.9 mm) was significantly shorter than that in healthy ears (24.4 ± 6.2 mm). This finding leads to the hypothesis that a shorter Eustachian tube causes nasopharyngeal reflux into the middle ear and provokes inflammatory conditions; therefore, the length of the Eustachian tube may be an important factor in the aetiopathology of chronic otitis media.
Described in 1962 by the World Federation of Radiology, the Reid horizontal plane has been used to calculate the angle of the Eustachian tube with the Reid horizontal plane,Reference Nemade, Shinde, Rangankar and Bhole9 which is the angle between the longitudinal axis of the Eustachian tube and the Reid plane. Habesoglu et al. evaluated 25 paediatric patients with chronic otitis media, and found no significant relationship between the angle of the Eustachian tube with the Reid horizontal plane and chronic otitis media.Reference Habesoglu, Habesoglu, Bolukbasi, Naiboglu, Eriman and Karaman14 However, in several studies, the angle of the Eustachian tube with the Reid horizontal plane was detected to be significantly narrower in chronic otitis media versus normal ears.Reference Dinç, Damar, Uğur, Öz, Eliçora and Bişkin7,Reference Nemade, Shinde, Rangankar and Bhole9,Reference Aksoy, Sayin, Yazici, Kayhan, Karahasanoglu and Hocaoglu15 Dinç et al. measured the angle of the Eustachian tube with the Reid horizontal plane to be 23.6 ± 2.4° in normal ears and 22.9 ± 2.8° in diseased ears.Reference Dinç, Damar, Uğur, Öz, Eliçora and Bişkin7 Nemade et al. found this angle to be 27.56 ± 3.62° in healthy ears and 25.41 ± 2.57° in diseased ears,Reference Nemade, Shinde, Rangankar and Bhole9 and Aksoy et al. measured it to be 28.84 ± 3.97° in healthy ears and 26.85 ± 4.04° in diseased ears.Reference Aksoy, Sayin, Yazici, Kayhan, Karahasanoglu and Hocaoglu15 Our findings are concordant with these studies, with measurements of this angle of 23.7 ± 4.0° in healthy ears and 21.6 ± 3.5° in ears with chronic otitis media. We therefore suggest that a more horizontal Eustachian tube may contribute to the pathogenesis of chronic otitis media by hampering the clearance of middle-ear secretions.
The tubotympanic angle is the angle between the line passing through the centre of the tympanic orifice of the Eustachian tube and the line passing through the centre of the bony external auditory canal. A few studies have investigated the role of the tubotympanic angle in patients with chronic otitis media. Aksoy et al. measured this angle in 70 patients who had chronic otitis media with cholesteatoma, 70 who had chronic otitis media without cholesteatoma and 70 healthy controls.Reference Aksoy, Sayin, Yazici, Kayhan, Karahasanoglu and Hocaoglu15 The angles were measured as 145.17 ± 6.36°, 144.58 ± 6.72° and 147.1 ± 6.38°, respectively. Aksoy et al. found no significant difference in tubotympanic angle values,Reference Aksoy, Sayin, Yazici, Kayhan, Karahasanoglu and Hocaoglu15 but other studies have detected a wider tubotympanic angle in patients with chronic otitis media.Reference Nemade, Shinde, Rangankar and Bhole9,Reference Vivek, Menon, Sandya and Polson16 Nemade et al. found tubotympanic angle values of 148.12 ± 3.43° in diseased ears and 145.14 ± 4.34° in healthy ears.Reference Nemade, Shinde, Rangankar and Bhole9 Vivek et al. measured the tubotympanic angle to be 146.17 ± 6.11° in a case group and 143.17 ± 6.01° in the control group.Reference Vivek, Menon, Sandya and Polson16 We also found that the tubotympanic angle was significantly wider in ears with chronic otitis media (141.0 ± 9.2° in diseased ears and 138.5 ± 9.8° in healthy ears). A wider tubotympanic angle may increase the transfer of upper respiratory tract pathogens to the middle ear, and hence increase susceptibility to middle-ear infections.
The diameter of the Eustachian tube varies throughout its length. The pharyngeal, mid, pre-isthmus, isthmus, post-isthmus and pretympanic segments make up the six topographic parts of the Eustachian tube. Although the pretympanic segment is the widest part of the Eustachian tube, it is greatly affected by middle-ear inflammation.Reference Nemade, Shinde, Rangankar and Bhole9 In the cadaver study of Sadé and Luntz, the temporal bones of 71 infants were examined.Reference Sadé and Luntz17 Forty-six of these infants had no middle-ear inflammation, while 25 had either acute or secretory otitis media. The mean luminal cross-sectional area of the pretympanium was significantly narrower in the diseased ears (4.14 ± 1.77, vs 5.33 ± 1.88 mm2 in healthy ears, p = 0.03). A few studies have measured the pretympanic diameter in patients with chronic otitis media. Vivek et al.Reference Vivek, Menon, Sandya and Polson16 and Nemade et al.Reference Nemade, Shinde, Rangankar and Bhole9 found that the pretympanic diameter of the Eustachian tube was significantly reduced in ears with chronic otitis media. Vivek et al. measured the Eustachian tube pretympanic diameter to be 2.979 mm in diseased ears and 3.410 mm in healthy ears.Reference Vivek, Menon, Sandya and Polson16 Nemade et al. measured this diameter to be 5.37 ± 2.10 mm in diseased ears and 6.47 ± 2.40 mm in healthy ears. They also evaluated the Eustachian tube patency in ears with chronic otitis media, and found that the pretympanic diameter was significantly narrower in patients with a blocked Eustachian tube.Reference Nemade, Shinde, Rangankar and Bhole9 According to our findings, the Eustachian tube pretympanic diameter was significantly narrower in ears with chronic otitis media compared to healthy ears (4.21 ± 0.71 mm in diseased ears vs 4.64 ± 0.79 mm in healthy ears). These findings suggest two possibilities: chronic Eustachian tube dysfunction might inhibit the growth of the Eustachian tube or a genetically narrow Eustachian tube might lead to chronic otitis media.
We compared the Eustachian tube dimensions of patients in groups 1A and 1B to clarify the effect of Eustachian tube dimensions on the development of cholesteatoma. No significant difference was found between the two subgroups except in the tubotympanic angle measurements. The tubotympanic angle was found to be significantly wider in ears with cholesteatoma, which is similar to the findings of Vivek et al.Reference Vivek, Menon, Sandya and Polson16 In the study by Aksoy et al., the angle of the Eustachian tube with the Reid horizontal plane was found to be significantly narrower in ears with chronic otitis media with cholesteatoma when compared to healthy ears and ears with chronic otitis media without cholesteatoma.Reference Aksoy, Sayin, Yazici, Kayhan, Karahasanoglu and Hocaoglu15 However, we could not demonstrate a significant difference between the angle of the Eustachian tube with the Reid horizontal plane in ears having chronic otitis media with cholesteatoma and without cholesteatoma. Although we found that the dimensions of the Eustachian tube are important in the aetiology of chronic otitis media, we could not detect a significant relationship between Eustachian tube dimensions and progression to cholesteatoma, except for the tubotympanic angle.
The aetiological factors affecting chronic otitis media, such as allergic, environmental, social and genetic factors, are likely to affect both ears. The reason why some patients have unilateral chronic otitis media remains controversial. According to our findings, the dimensions of the Eustachian tube may be responsible for this phenomenon. We reviewed the literature for interaural differences in the Eustachian tube measurements of healthy subjects. Takasaki et al. measured the length of the Eustachian tube and the angle of the Eustachian tube with the Reid horizontal plane, and detected no significant difference between the left and right ears of healthy adults, healthy children and children with OME.Reference Takasaki, Takahashi, Miyamoto, Yoshida, Yamamoto-Fukuda and Enatsu5 El-Anwar et al. measured the length of the bony and cartilaginous parts of the Eustachian tube, the total length of the Eustachian tube, the width and height of the Eustachian tube tympanic orifice, the tubotympanic angle, and the angle of the Eustachian tube with the Reid horizontal plane in 100 healthy subjects.Reference El-Anwar, Eldib, Nofal and Khazbak18 They found no significant difference in the measurements for left and right ears except for the length of the bony segment of the Eustachian tube, which was significantly longer on the left side. In a recent study by Janzen-Senn et al., several parameters, such as the length of the bony and cartilaginous parts of the Eustachian tube, the total length of the Eustachian tube, and the angles of the bony and cartilaginous parts of the Eustachian tube with the horizontal and sagittal planes, were measured in 143 healthy subjects.Reference Janzen-Senn, Schuon, Tavassol, Lenarz and Paasche19 Significant interaural differences in the length of the bony part of the Eustachian tube and in the angle of the cartilaginous part of the Eustachian tube to the horizontal plane were found. The bony part of the Eustachian tube was longer, and the angle between the cartilaginous part of the Eustachian tube and the horizontal plane was smaller, on the right side. The authors reported that these differences might have been coincidental, and due to the resolution of images or the lower fossa cranii media on the right side.
• Eustachian tube anatomical features have an important role in the aetiology of otitis media with effusion, atelectasis and adhesive otitis media
• Patients with craniofacial abnormalities and Down syndrome have a higher risk of middle-ear infections associated with the shorter length and horizontal location of the Eustachian tube
• Advances in computed tomography, such as multiplanar reconstruction, provide better information on Eustachian tube anatomy
• The Eustachian tube was shorter, narrower and located more horizontally in ears with chronic otitis media
• No relationship between Eustachian tube dimensions and cholesteatoma development was detected
There are several limitations to our study. Firstly, given the retrospective design of the study, we did not assess Eustachian tube function. Although we excluded patients prone to Eustachian tube dysfunction (e.g. craniofacial abnormalities, allergic rhinitis), an objective evaluation regarding the functionality of the Eustachian tube was not performed. Further studies assessing both the anatomy and function of the Eustachian tube are needed. Secondly, our study did not rule out the effect of chronic Eustachian tube dysfunction on the development of the Eustachian tube. Childhood-onset chronic otitis media might have led to limited growth of the Eustachian tube. The evaluation of Eustachian tube dimensions in childhood-onset and late-onset chronic otitis media might provide better understanding of the relationship between chronic otitis media and Eustachian tube anatomy.
The measurement of Eustachian tube dimensions using the multiplanar reconstruction technique on temporal bone CT is a non-invasive, reliable and easy technique, with no need for extra radiation. Comprehension of the Eustachian tube anatomy pre-operatively may be helpful in achieving better surgical results. Modification of the surgical approach might be considered when bony narrowing of the pretympanic segment is detected. Post-operative hypoventilation may be prevented by using cartilage graft, and balloon tuboplasty may be added to the surgical procedure in cases of severe narrowing.
Conclusion
This study demonstrates that Eustachian tube length, the angle of the Eustachian tube with the Reid horizontal plane, the tubotympanic angle and the Eustachian tube pretympanic diameter are closely related to chronic otitis media aetiopathology, but are not related to cholesteatoma development, except for the tubotympanic angle. Measurement of the Eustachian tube dimensions on temporal bone CT scan images is a simple technique that can be used in clinical practice.
Competing interests
None declared.






