


Introduction
The accumulation of evidence, in support of the Developmental Origins of Health and Disease (DOHaD) hypothesis has reached the level where it is time to use such evidence to inform practice. Research supports the development and testing of interventions to support primary prevention of noncommunicable diseases (NCDs) via application of DOHaD principles.Reference Hanson and Gluckman 1 Evidence suggests that interventions should engage individuals during the preconceptional period,Reference Gluckman, Hanson, Seng and Bardsley 2 , Reference Itoh and Kanayama 3 pregnancy,Reference Gluckman, Hanson, Seng and Bardsley 2 , Reference Itoh and Kanayama 3 lactation,Reference Gluckman, Hanson, Seng and Bardsley 2 , Reference Itoh and Kanayama 3 childhoodReference van Deutekom, Chinapaw, Vrijkotte and Gemke 4 and adolescence.Reference Bay, Morton and Vickers 5 The possibility of educational interventions in various stages of life is suggested by Ito and Kanayama.Reference Itoh and Kanayama 3 In such interventions access to, and discussion of, scientific evidence should be facilitated. This should acknowledge the socioecological context of the group. Such processes promote transactional communication between health professionals and communities of interest.Reference Bay, Morton and Vickers 5 Such interventions are reliant on education programs that produce health professionals, including, dietitians, nurses, midwives, doctors and nutrition teachers, who have high levels of relevant health and scientific literacy.
To inform such programs, we need evidence of baseline awareness and understanding of DOHaD concepts in students entering undergraduate health training programs. However, to date, there has been little research into public, or tertiary student awareness and/or understanding of DOHaD concepts. Limited existing evidence suggests relatively low levels of awareness of DOHaD in first-time mothers,Reference Gage, Raats and Williams 6 11–14-year-old school students and their parents,Reference Bay, Mora and Sloboda 7 and 18–22-year-old female university students.Reference Endo and Oyamada 8 Thus, the purpose of this study was to assess the development of awareness and understandings of DOHaD-related terms and concepts during undergraduate courses training future health professionals. The two countries associated with this pilot study provide contrasting settings where nutritional environmental exposures in early life are causing concern with regard to future health. In New Zealand, DOHaD evidence has been identified as relevant to strategies contributing to addressing growing metabolic health issues. In this setting increasing overweight and obesity during the pre- and periconceptional and gestational periods is evident. 9 , 10 The potential for this to contribute to child, adolescent and adult obesity is driving efforts to increase knowledge and understanding of DOHaD concepts in the health professional sector. 11 , Reference Bay, Vickers, Mora, Sloboda and Morton 12 In contrast, in Japan maternal underweight during the pre- and periconceptional periods, and low birth weight are driving the need to apply DOHaD evidence to strategies to support long-term population health.Reference Gluckman, Seng, Fukuoka, Beedle and Hanson 13 , Reference Kubota, Itoh and Tasaka 14 Undergraduate health professional students of nutrition in Japan and nursing in New Zealand were chosen as study subjects, enabling examination of whether common phenomena exist with respect to the development of DOHaD concepts between the two contexts.
Method
This was a cross-sectional pilot study, conducted in April 2015 in health professional training programs in Japan and New Zealand. A standardized questionnaire was developed to assess awareness of basic DOHaD concepts related to the impact of nutritional exposures in early life on health and well-being throughout the life course. This was administered to two populations available for this pilot study, being trainee dietitians and nurses from Japan and New Zealand respectively. This offered populations from different sociocultural contexts within courses that train future health professionals who should once trained, be able to apply DOHaD concepts to their practice.
Context
Undergraduate nutrition students in Japan were engaged in a four-year course of study including compulsory papers covering core concepts of ‘Nutrition in the Life Cycle.’ DOHaD concepts were first introduced in May of Year 1 in a 90-min lecture. Throughout the rest of the program students took courses in which DOHaD concepts were integrated into lectures, with students having opportunities to complete learning activities based on these concepts. Undergraduate nursing students in New Zealand were from a 3-year course of study that utilized an integrated learning approach where development of understanding of core concepts in science, health, and practice was interwoven via application to practice. DOHaD concepts associated with maternal and child nutrition were introduced within in a compulsory nutrition paper in the third year of the course.
Subject sampling
The study was conducted before the teaching of DOHaD-related concepts in Year 1 of the Japanese course, and following teaching of DOHaD nutrition concepts in Year 3 of the New Zealand course.
All Year 1–4 undergraduate students from the Department of Food Science and Human Nutrition, Fuji Women’s University (n=357) and Year 1–3 undergraduate students from the School of Nursing, The University of Auckland (n=252) who were present on the day of April 2015 that the questionnaire was administered were eligible to participate (Table 1). An explanation of the study was given in writing and verbally, and consent to participate was obtained. A total of 460 students, 309 (87%) Japanese and 151 (60%) New Zealand completed the paper-based questionnaire.
Table 1 Characteristics of participating undergraduate students
Questionnaire
Meetings attended by researchers from each country established the collaboration and designed the questionnaire. The questionnaire was informed by previous studies examining public awareness and/or understanding of DOHaD concepts by Bay et al.Reference Bay, Mora and Sloboda 7 , Reference Bay, Dixon, Morgan, Wall and Oyamada 15 and Gage et al.Reference Gage, Raats and Williams 6 The initial version of the questionnaire was created in English. This was translated into Japanese and piloted with a small group consisting of 10 undergraduate students. Equivalence of meaning in each language and culture was prioritized over equivalence of vocabulary in the process of translation. This meant that minor adaptations were made to accommodate local cultural differences between Japan and New Zealand. The questionnaires were reviewed by DOHaD researchers at the 2014 Annual Meeting of the Japan DOHaD society to confirm the appropriateness of the literacy level and agree on wording.
The questionnaire consisted of one ‘Yes’/‘No’ question relating to awareness of the phrases ‘Developmental Origins of Health and Disease’ or ‘First 1000 days’ and nine statements utilizing Likert attitude scales that explored awareness of life course determinants of health and well-being. We defined awareness as recognition of a concept. This may be associated with declarative knowledge, but may also be present as knowing without understanding. The Likert questions used in this study do not enable differentiation between awareness and knowledge. The response choices in Japanese were ‘Strongly Agree,’ ‘Somewhat Agree,’ ‘Don’t know,’ ‘Disagree’ and ‘Strongly Disagree,’ whereas those for the New Zealand students were ‘Agree Very Much,’ ‘Agree Moderately,’ ‘Agree Slightly,’ ‘Don’t know,’ and ‘Disagree.’ To enable comparison, responses from Japan and New Zealand were coded into four common ordinal categories being: ‘STRONGLY AGREE,’ ‘AGREE,’ ‘DON’T KNOW,’ and ‘DISAGREE.’ To achieve this, for the Japanese version ‘Somewhat Agree’ was categorized as ‘AGREE,’ ‘Disagree’ and ‘Strongly Disagree’ as ‘DISAGREE.’ For the New Zealand version ‘Agree Very Much’ was coded as ‘STRONGLY AGREE,’ while ‘Agree Moderately’ and ‘Agree Slightly’ were coded as ‘AGREE.’ In the common four opinion codes, ‘DON’T KNOW’ was taken as neither ‘AGREE’ nor ‘DISAGREE’ as performed in the paper by Al-Haqwi.Reference Al-Haqwi 16 Consequently, ‘STRONGLY AGREE,’ ‘AGREE,’ ‘DON’T KNOW’ and ‘DISAGREE’ were used in the following statistical analyses as ordinal dependent variable.
Statistical analyses
Descriptive statistics were used to identify frequencies. The effect of context (Japan v. New Zealand) at each of Years 1, 2 and 3 was measured using binomial or ordinal logistic regression as appropriate. Variance in frequency of yes/no responses relating to awareness of the phrases ‘Developmental Origins of Health and Disease’ or ‘First 1000 days’ was compared between contexts at Years 1, 2 and 3 using binomial logistic regression. Variance in frequencies of responses within the Likert-scale statements was assessed via ordinal logistic regression with proportional odds. Trends toward ‘Yes’ response and the higher value on the ordinal variable across undergraduate courses within each country were assessed using the Cochran-Armitage test of trend for binomial responses, and the Jonckheere-Terpstra test of trend for ordinal responses.Reference Al-Haqwi 16 – Reference Giefer, Lowe and Werlin 18
The significance threshold was 0.05. Statistical analyses were performed using Excel 2011 (Microsoft) with Statcel 4 add-on (The Publisher OMS Limited, Saitama, Japan) and EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria) and SPSS (IBM Corp, 2015).
Results
A total of 460 students, comprising 309 Japanese undergraduate nutrition students (Years 1–4) and 151 New Zealand undergraduate nursing students (Years 1–3), participated in this study. Characteristics of the participants are summarized in Table 1.
In the Japanese sample, differences in response rates were not statistically significant across Years 1–4 (P=0.595 via χ2 for independent test). In the New Zealand sample, response rates were significantly different among Years 1–3 (P<0.001 via χ2 for independent test).
Responses to questions seeking evidence of awareness of the phrases ‘Developmental Origins of Health and Disease,’ or ‘First 1000 Days’ are shown in Fig 1. ‘Yes’ response showed significant trends across undergraduate courses in the students of both contexts (P<0.001 via The Cochran-Armitage test). ‘Yes’ response was negligible in both contexts at course entry. Despite having DOHaD specific teaching in Year 1, this remained very low in the Japanese cohort in Year 2, increasing to 70% by the final year of the program. In New Zealand, there was a clear increase associated with the DOHaD specific teaching at Year 3. However, similarly to Japan, this increase only reached 60% at Year 3. Assessment via binomial logistic regression of the effect of country on response at Years 1, 2 and 3 found no significant difference in responses between both contexts (Fig. 1).
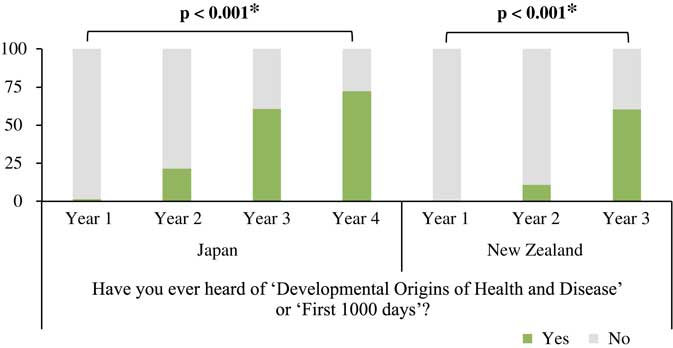
Fig. 1 Undergraduate students’ awareness of DOHaD. The Cochran-Armitage test of trend was used to assess the significance of the monotonic trend towards positive responses to this statement; p* bold significant (α=0.05). Assessment via binomial logistic regression of the effect of country on response at Years 1, 2 and 3 found no significant variation in responses.
Results of responses to statements exploring awareness of DOHaD concepts are presented in Fig 2 and Table 2. Statements (a) and (b) investigate awareness of associations between health and well-being of either parent before conception and health of the fetus. In each undergraduate year in both contexts, awareness of associations between maternal factors and fetal health was significantly higher than awareness of impacts of paternal factors (P<0.001 via Wilcoxon’s signed rank test). Progression through undergraduate courses was associated with increased awareness of maternal impacts in New Zealand. With regard to paternal factors, no significant change in awareness was observed in either context. In the final years of study (Year 4 in Japan and Year 3 in New Zealand), only two-thirds of students in each country indicated a strong agreement to this statement in relation to maternal factors (Fig. 2). Concerning awareness of associations between maternal factors and fetal health, the Japanese students reported significantly higher scores compared to the New Zealand students at Years 1 and 3, whereas there were no significant differences in that between paternal factors and fetal health (Table 2).
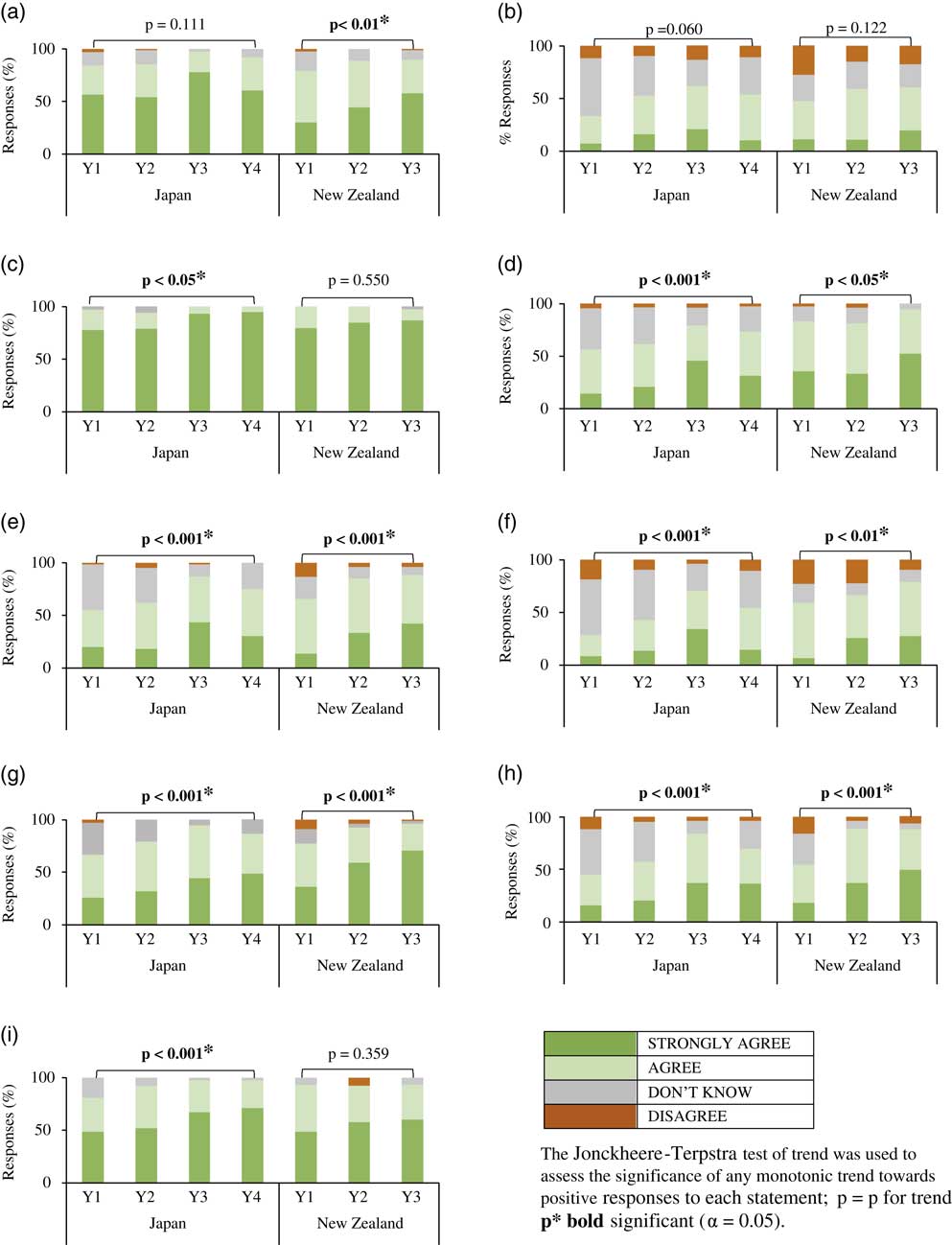
Fig. 2 Undergraduate students’ awareness of life course determinants of health and well-being. (a) A woman’s general health and well-being before conception affects the health of the fetus during pregnancy. (b) A father’s general health and well-being before conception affects the health of the fetus during pregnancy. (c) A woman’s nutrition during pregnancy affects the health of the fetus during pregnancy. (d) A woman’s nutrition during pregnancy affects the health of the child in the first 2 years of life. (e) A woman’s nutrition during pregnancy affects the health of the child throughout childhood. (f) A woman’s nutrition during pregnancy affects the health of the child throughout adulthood. (g) A child’s nutrition during the first 2 years of life affects the health of the child throughout childhood. (h) A child’s nutrition during the first 2 years of life affects the health of the child throughout adulthood. (i) An individual’s diet affects their risk for developing noncommunicable diseases such as cancer, heart disease, type 2 diabetes, etc.
Table 2 Comparison of the distribution of responses in Years 1, 2, and 3, based on country

NCDs, noncommunicable diseases.
A cumulative odds ordinal logistic regression with proportional odds was run for each undergraduate year to determine the effect of country (Japan compared with New Zealand) on the belief that the response to each question was ‘STRONGLY AGREE’. *P bold significant (α=0.05).
Statements (c)–(f) investigated awareness of associations between maternal nutritional exposures during pregnancy and health of the offspring through to adulthood. Awareness of associations between nutritional exposures during pregnancy and fetal health was demonstrated by almost 80% of Year 1 students in both contexts. This increases significantly in Japan during the undergraduate program, but not in New Zealand. Progression through undergraduate years was associated with significant increases in awareness of associations between maternal nutritional exposures during pregnancy and offspring health beyond pregnancy in both contexts. However, less than 50% of students in their final year of study selected ‘STRONGLY AGREE’ in response to statements in relation to infant, child and adult health (Fig. 2). When comparisons between the two contexts (Japan and New Zealand) were made at each of Years 1–3, there were no significant differences with regard to awareness of associations between maternal nutritional exposures during pregnancy and fetal health, and between maternal nutritional exposures during pregnancy and adult health. However, awareness of associations between maternal nutritional exposures during pregnancy and infant health were significantly lower in Year 1 and Year 3 students in Japan than those in New Zealand. Similarly, awareness of associations between maternal nutritional exposures during pregnancy and child health were significantly lower in Year 2 students in Japan compared with those in New Zealand (Table 2).
Statements (g) and (h) investigated awareness of associations between nutritional exposures during infancy and health through to adulthood. Participation in undergraduate study in both contexts was associated with significant increases in awareness of these associations across all undergraduate years. However, as with the effects of maternal nutritional exposures, levels of awareness of impacts of nutritional exposures in infancy on adult health were lowest. Less than 50% of students in their final year of study selected ‘STRONGLY AGREE’ in response to these statements (Fig. 2). Concerning awareness of associations between nutritional exposures during infancy and health throughout childhood, the Japanese students in Year 2 and Year 3, but not Year 1, selected responses that were significantly lower in value compared with the New Zealand students. Regarding awareness of associations between nutritional exposures during infancy and health throughout adulthood, the Japanese students in Year 2, but not Year 1 and Year 3, selected significantly lower values compared with those of New Zealand (Table 2).
Statement (i) investigated general awareness of associations between nutrition and NCD risk, demonstrating that, on course entry in both contexts, this was a commonly held viewpoint. While a significant increase in the proportion of students selecting ‘STRONGLY AGREE’ in response to this statement was observed in Japan, this was not the case in New Zealand. In the final year of undergraduate study in both contexts, less than 75% of students studying to become health professionals selected ‘STRONGLY AGREE’ in response to this statement (Fig. 2). There were no significant differences in general awareness of associations between nutrition and NCD risk between students in New Zealand and Japan (Table 2).
Discussion
As far as we are aware, this is the first study that has attempted to determine levels of awareness of DOHaD concepts in undergraduate students on entry to, and during health professional training programs in which DOHaD concepts are taught. In general, the results in both contexts showed similar low levels of awareness on entry to the programs. This finding is comparable with data reported from surveys examining awareness of DOHaD concepts in first-time mothers in five European countries,Reference Gage, Raats and Williams 6 11–14-year-old school students/their parents in New Zealand,Reference Bay, Mora and Sloboda 7 and 18–22-year-old female Japanese university students.Reference Endo and Oyamada 8 Therefore, it is probable that low levels of awareness and understanding of DOHaD concepts are common in adult populations around the world.
Health professionals should be able to demonstrate high levels of understanding of DOHaD principles and their potential for application in practice. This may support the potential for interventions to promote primary NCD risk reduction and the transgenerational opportunities for improved health offered by application of DOHaD concepts in practice to succeed. This requires the provision of education for aspiring health professionals in which DOHaD concepts are integrated across learning programs and identified as being relevant to practice. Our present study demonstrated that year of undergraduate health professional training was positively associated with increasing awareness of DOHaD concepts, suggesting an increasing exposure within the courses. Nonetheless, despite such increasing percentage of students in their final year responding ‘STRONGLY AGREE’ to most statements, levels of awareness of paternal impacts before conception remained extremely low, and strong awareness of the ongoing impact of nutritional exposures in pregnancy to later-life health remained below 50%. These results indicate that present education is insufficient in both contexts.
Reductionist thinking with respect to NCD cause and effect is common in many societies. The low levels of awareness of life course determinants of health and well-being expressed by the students in our survey represents a frame of reference aligned to reductionist thinking that will have developed as a result of exposure to ideas expressed within family, community, education and society over time. Frames of reference are deeply held views based on assumptions, conceptions, and expectations involving values, beliefs and concepts.Reference Dirkx, Mezirow and Cranton 19 While DOHaD evidence challenges these frames of reference, to shift them to the point where DOHaD evidence is integrated into thinking and action is a significant challenge that the DOHaD community need to embrace.
The need for integration of concepts underpinning the DOHaD hypothesis in undergraduate health training has been argued for by Gluckman, Beedle and Hanson. In their publication of Principles of Evolutionary Medicine, they propose that learning programs that promote knowledge of the integral role of developmental and evolutionary history in understanding health and disease should be included in undergraduate health professional education.Reference Gluckman, Beedle, Buklijas, Low and Hanson 20 Nesse et al. argue that in order for such education to be effective programs must promote the development of contextual understanding of content from across relevant science disciplines as well as evolutionary and developmental biology.Reference Nesse, Bergstrom and Ellison 21 This highlights the need for understanding to develop over time, and be applied in the setting of professional health training programs.
The results presented in this paper suggest that the introduction of DOHaD-related content in the programs associated with this study is not presently representative of the vision presented by Nesse et al.Reference Nesse, Bergstrom and Ellison 21 While we do see a change in awareness of basic concepts in the progression across the courses measured in this study, the evidence points toward this being inadequate in its current form. This suggests that the current practice in terms of integration of DOHaD-related concept development in the undergraduate programs represented in this study is a good starting point. However, greater development of integration of concepts underpinning the DOHaD hypothesis must occur if these courses are to result in students graduating with capabilities (knowledge, attitudes, skills and values) that are required to apply principles associated with the DOHaD hypothesis in practice, and communicate this frame of reference effectively within the communities in which they are working.
Limitations
The present study has several limitations. First, it only assessed awareness, rather than awareness and understanding. Typical of surveys designed to be undertaken in a very short time frame (therefore increasing likely response rates), the survey did not engage participants in questions that could uncover why they select specific responses. This can be addressed by increasing the time requested of participants and adding in open-ended questions that ask participants to explain why they selected a particular response. These data can then be coded to establish theme patterns from which typical and atypical indications of understanding can be elucidated. Alternatively, focus groups with a subset of participants can produce a similar result if they are repeated until saturation of ideas expressed has been established.
While assessment of courses in New Zealand and Japan has provided insight to identify the validity of the survey in different contexts, issues associated with contextual translation of the survey tool arose, which reduced the reliability of inter-context comparisons. As discussed in the methods, these pertain to the differences in interpretation of the Likert scale. This arose as a consequence of the modification of the original questionnaire for use in Japan and will be addressed in any future use of the tool. In this paper, we rearranged the response choices into common four categories to enable comparison between the two contexts. This appears not to have affected their equivalence, and thus the conclusions reached. That is, the overall the trend for strength of response to increase across time was evident in both groups.
The two universities of which students were sampled in this study may not be representative of the two counties. Furthermore, the undergraduate students belong to two differing health professional programs (nursing and nutrition). While both professions are engaged in care that requires understanding of the role of nutrition across the life course on health and well-being, there may be differences in emphasis. This study was not designed to enable a general comparison of understanding of DOHaD concepts between students in the two countries. Rather, it was assessing the potential of the tool to assess the development of awareness and understandings of DOHaD-related terms and concepts during undergraduate courses training future health professionals. We think that it is meaningful that similar results were obtained between the two very different contexts.
Assessment of the impact of socioecological context on development of awareness and understanding of DOHaD evidence and its potential for application in health care would be more usefully undertaken if assessment could occur with students in equivalent courses in different settings.
The fact that a close analysis of the way in which DOHaD was incorporated in each of the program curriculum was not undertaken maybe considered a further limitation. Therefore, the relationship between changes in understanding of DOHaD concepts and curriculum content during health professional education remains to be clarified.
The study could be enhanced significantly by following a cohort of students through an undergraduate program. With the addition of focus groups and access to academic assessment results from within the cohort, this could uncover the extent to which particular aspects of learning programs supported development of understanding of DOHaD concepts to the point where these were integrated into interpretation of health-related inquiry, and eventually practice. Attention to behavior change (personal and professional) could also be a useful addition to future studies investigating the impact of inclusion of DOHaD concepts in health professional training programs.
Conclusion
This study has indicated that the use of a standardized questionnaire enabled assessment of awareness of DOHaD concepts in undergraduate students in two different contexts. Findings demonstrated low entry level of awareness of DOHaD-related terms and concepts in undergraduate Japanese nutrition and New Zealand nursing students. Year of undergraduate training was positively associated with increasing awareness of DOHaD concepts, suggesting an increasing exposure to DOHaD concepts within the courses. Nonetheless, despite the increasing percentage of students in their final year responding ‘STRONGLY AGREE’ to most statements, levels of awareness of paternal impacts prior to conception remained extremely low, and strong awareness of the ongoing impact of nutritional exposures in pregnancy to later-life health remained below 50%. This indicates that in the contexts examined in this study, significant scope exists for educators to construct learning programs that facilitate development of understanding of associations between early-life exposures and later-life health and well-being is required.
Financial Support
This work was supported by grants-in-aid for Scientific Research (C) from the Ministry of Education, Culture, Sports, Science, and Technology, Japan (Grant Number JP23617021) and from a University of Auckland, School of Nursing FRDF Research Seeding Grant and a Liggins Institute FRDF grant (3706937).
Conflicts of Interest
None.
Ethical Standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national guidelines on human experimentation (Ethical Guidelines for Medical and Health Research Involving Human Subjects established by the Ministry of Education, Culture, Sports, Science and Technology and the Ministry of Health, Labour and Welfare, Japan) and with the Helsinki Declaration of 1975, as revised in 2008, and has been approved by the institutional committees (Fuji Women’s University Human Participants Ethics Committee, Ref. 2014-11; The University of Auckland Human Participants Ethics Committee, Ref. 013093).
Acknowledgments
The authors wish to acknowledge participating students and teachers for their time and investment in this study.





 Open access
Open access