



Introduction
In recent years, the development of intravenous infusion technology has highlighted catheter-related complications. Among commonly used vascular access devices, peripherally inserted central catheters (PICC) and midline catheters (MC) have significant pros and cons that require thorough comparison for clinical decision-making. PICC lines, extending into the superior vena cava, are used for long-term therapies such as chemotherapy and parenteral nutrition. Reference Gifford, Hinton, Jia, Nasr, Mermis and Lahiri1 They have a lower risk of infiltration but can lead to complications such as catheter-related bloodstream infections (CRBSIs) and thrombosis. Reference Usman, Cheema, Mustafa and Iftikhar2,Reference Chen, Zhu, Wan and Qin3 MC, inserted into the upper arm and terminating before reaching the central veins, are designed for shorter-term use, typically 1–4 weeks. Reference Sebolt, Buchinger, Govindan, Zhang, O’Malley and Chopra4 They offer simpler insertion, lower cost, and reduced risk of central vein injuries. Reference Seo, Altshuler, Dubrovskaya, Nunnally, Nunn and Ello5 However, MC have a higher incidence of occlusion and phlebitis, limiting their efficacy for long-term treatments. Reference Swaminathan, Flanders, Horowitz, Zhang, O’Malley and Chopra6,Reference Sharp, Esterman, McCutcheon, Hearse and Cummings7
The choice between PICC and MC depends on factors such as therapy duration, medication type, patient vein quality, and complication risks. Reference Citla Sridhar, Abou-Ismail and Ahuja8 Although PICC requires meticulous maintenance to prevent infections, MC may offer better patient comfort but necessitates more frequent maintenance. Reference Gornik, Gerhard-Herman, Misra, Mohler and Zierler9,Reference Duijzer, de Winter, Nijkeuter, Tuinenburg and Westerink10 This meta-analysis aims to compare the safety and efficacy of PICC and MC. By synthesizing data from recent studies, we evaluate complications (such as thrombosis, CRBSIs, etc.), cost, and patient comfort. Our goal is to provide evidence-based guidance for selecting the most appropriate vascular access device, improving patient outcomes, and minimizing risks associated with intravenous therapy.
Materials and methods
This study followed the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) guidelines (Table S1) (PROSPERO ID: CRD42024570503).
Search strategy
Studies comparing PICC and MC were systematically searched in the Web of Science, EMBASE, Cochrane Library, PubMed, ScienceDirect, and Scopus databases up to June 15, 2024. The MeSH terms used were “Peripherally inserted central venous catheter” and “Midline catheter.” Additionally, eligible articles were further identified through references from retrieved literature. Detailed retrieval strategies are provided in Table S2.
Selection criteria
Inclusion criteria:
-
1) Population: Adult patients who require the insertion of PICC or MC for intravenous infusion therapy and do not have contraindications for intravenous catheter insertion
-
2) Intervention and comparison: PICC versus MC.
-
3) Outcomes: The primary endpoint is thrombosis. Secondary endpoints included other complications, cost, and satisfaction rate.
-
4) Study design: Randomized controlled trials (RCTs) or cohort studies (CTs).
-
5) Conference papers, reviews, animal experiments, and articles without original data were excluded.
Data extraction
Two independent investigators extracted the following data: study characteristics (design, period, etc.), participant characteristics (age, sex, etc.), complications (thrombosis, CRBSIs, etc.), cost, and satisfaction (satisfaction rate, dissatisfaction rate, etc.). Disagreements were resolved through re-evaluation.
Outcome assessments
Thrombosis was assessed in different locations: catheter-related, contralateral, contralateral and/or bilateral, and pulmonary embolism (PE). Additionally, thrombosis was also analyzed according to different types: catheter-related superficial thrombosis (SVT) and catheter-related deep vein thrombosis (DVT).
Quality assessment for included studies
The quality of CTs was evaluated using the Newcastle-Ottawa Scale (NOS), including 3 items: selection, comparability, and outcome. A score of 6 or more points signifies medium to high quality. Reference Wells, Shea, O’Connell, Peterson, Welch and Losos11 The RCTs’ quality was assessed with the Jadad scale, which allocates up to 5 points for randomization, blinding, and participant inclusion, with scores of 3 or higher indicating high quality. Reference Jadad, Moore, Carroll, Jenkinson, Reynolds and Gavaghan12 The results’ quality was assessed using the GRADE approach. Reference Higgins, Altman, Gøtzsche, Jüni, Moher and Oxman13
Statistical analysis
Pooling data were analyzed using RevMan 5.3 and STATA 12.0. Continuous variables were analyzed using mean difference (MD), while dichotomous variables were assessed with pooled risk ratios (RR). Heterogeneity was assessed with the I 2 statistic and χ2 test. Significant heterogeneity (I 2 > 50% or P < .1) warranted a random-effects model; otherwise, a fixed-effects model was utilized. Funnel plots were used to assess publication bias.Reference Sterne, Sutton, Ioannidis, Terrin, Jones and Lau14 Statistical significance was indicated by P < .05.
Results
Search results
Initially, 1,502 studies were identified, and 14 studies (PICC group: 10,834 patients; MC group: 9,841 patients) were analyzed (Figure 1). Reference Swaminathan, Flanders, Horowitz, Zhang, O’Malley and Chopra6–Reference Wells, Shea, O’Connell, Peterson, Welch and Losos11,Reference Lescinskas, Trautner, Saint, Colozzi, Evertsz and Chopra18–Reference Tao, Wang, Liu, Li and Sui21 Table 1 presents the baseline characteristics. Eight studies were conducted in the United States, 4 in Europe, 2 in Australia, and 1 in China. The average catheter time for the PICC group was 30.49 days, whereas for the MC group, it was 18.24 days. All studies were rated as medium to high quality based on the NOS and Jadad scale (Tables S3 and S4). All outcomes were rated as low to very low quality by the GRADE system (Table S5).

Figure 1. Flow chart of the study selection process.
Table 1. Baseline characteristics of the included studies

Note. CT, cohort study; M/F, male/female; MC, midline catheters; PICC, peripherally inserted central catheters; RCT, randomized clinical trial.
Thrombosis
According to patients, the rate of catheter-related SVT (RR: 0.42 [0.28, 0.64]) was higher in the MC group. Catheter-related DVT, contralateral thrombosis (DVT+SVT, DVT and SVT), contralateral and/or bilateral thrombosis (DVT+SVT, DVT and SVT), and PE were similar between the 2 groups (Table 2, Figure 2).
Table 2. Comparison of PICC versus MC on thrombosis events according to patients
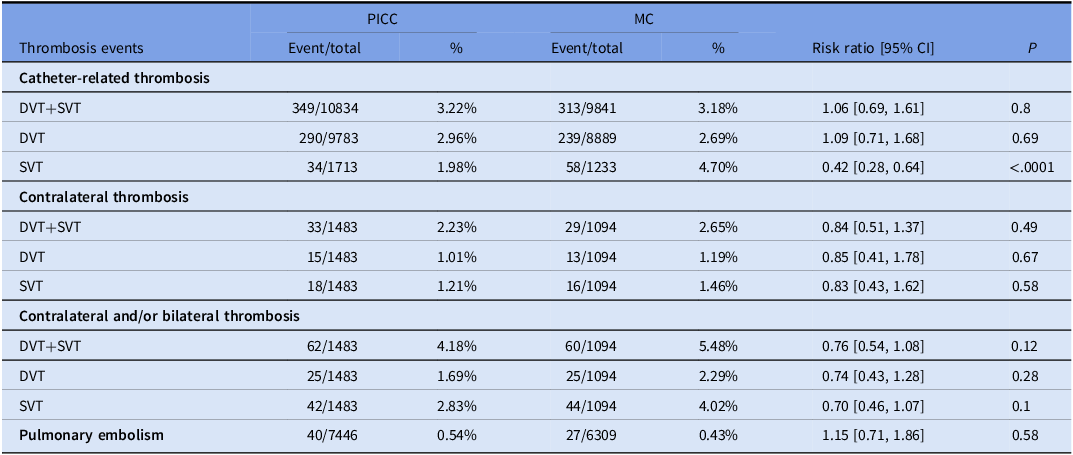
Note. CI, confidence interval; DVT, deep vein thrombosis; MC, midline catheters; PICC, peripherally inserted central catheters; RR, risk ratio; SVT, superficial vein thrombosis.
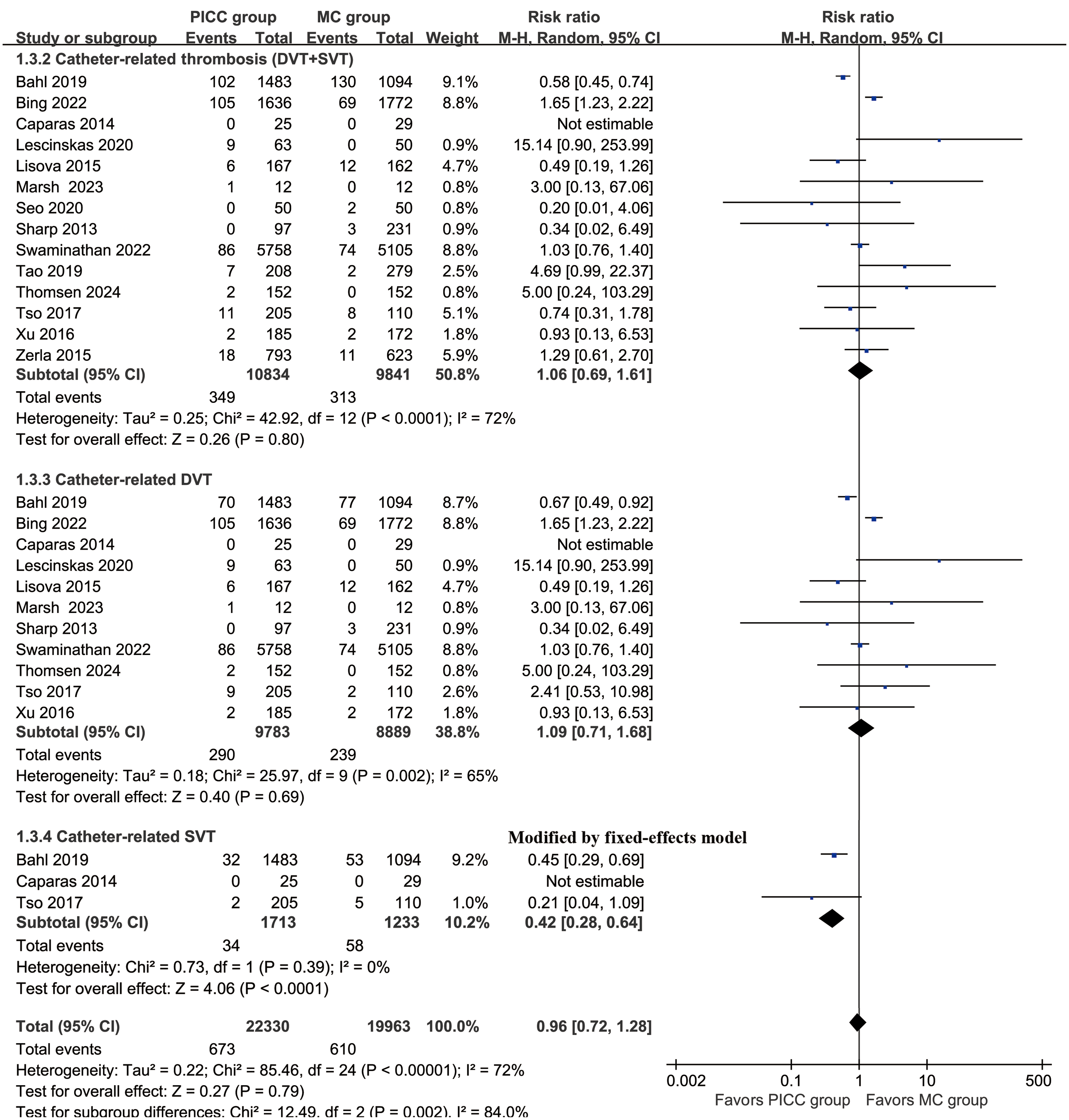
Figure 2. Forest plots of catheter-related thrombosis (DVT+SVT), catheter-related DVT, and catheter-related SVT associated with PICC versus MC. DVT, deep vein thrombosis; SVT, superficial vein thrombosis; PICC, peripherally inserted central catheters; MC, midline catheters.
According to catheter days, the rate of catheter-related thrombosis (DVT+SVT) (RR: 0.41 [0.18, 0.95]) was higher in the MC group. Catheter-related DVT and PE were similar between the 2 groups (Table 3).
Table 3. Complications assessment according to catheter days
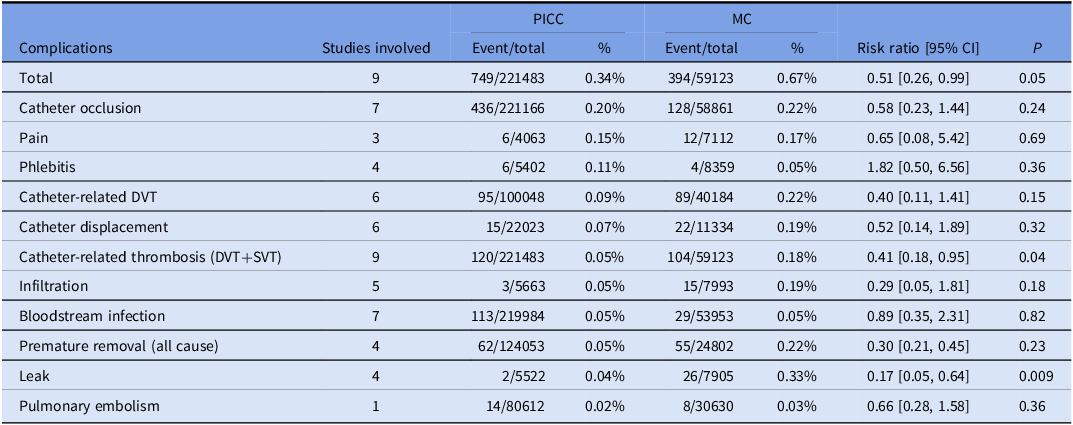
Note. CI, confidence interval; DVT, deep vein thrombosis; MC, midline catheters; PICC, peripherally inserted central catheters; RR, risk ratio; SVT, superficial vein thrombosis.
Complications assessment according to patients
More infiltrations (RR: 0.27 [0.12, 0.62]) and leaks (RR: 0.16 [0.05, 0.53]) were found in the MC group. Meanwhile, more CRBSIs (RR: 1.95 [1.15, 3.32]) were found in the PICC group (Figure 3). The rates of total complications, catheter occlusions, premature removals (all causes), catheter displacements, phlebitis, and pain were similar between the 2 groups (Table 4, Figures S1 and S2).

Figure 3. Forest plots of catheter-related bloodstream infection associated with PICC versus MC. PICC, peripherally inserted central catheters; MC, midline catheters.
Table 4. Complications assessment according to patients

Note. CI, confidence interval; DVT, deep vein thrombosis; MC, midline catheters; PICC, peripherally inserted central catheters; RR, risk ratio; SVT, superficial vein thrombosis.
Complications assessment according to catheter days
According to catheter days, more total complications (RR: 0.51 [0.26, 0.99]) and leaks (RR: 0.17 [0.05, 0.64]) were found in the MC group. The rates of catheter occlusions, pain, phlebitis, catheter displacements, infiltrations, CRBSIs, and premature removals were similar between the 2 groups (Table 3).
Cost and satisfaction assessment
In the assessment of satisfaction, a higher rate of dissatisfaction (RR: 4.77 [2.33, 9.77]) was reported in the PICC group. The rate of satisfaction and needing improvements was similar between the 2 groups (Figure S3). Meanwhile, the costs (MD: 63.00 [61.59, 64.41] dollars) were also higher in the PICC group (Figure S4).
Sensitivity analysis
Sensitivity analyses for total complications, catheter-related thrombosis (DVT+SVT), and catheter-related DVT were performed, demonstrating that excluding any individual study did not affect the results’ reliability (Figure S5).
Publication bias
The analysis of total complications, catheter-related thrombosis (DVT+SVT), CRBSIs, and catheter displacement revealed no evidence of publication bias (Figure S6).
Discussion
The debate over the optimal choice between PICC and MC for intravenous therapy in oncology and critical care is ongoing. Both catheter types play essential roles in patient management, yet their associated complications and overall effectiveness require detailed evaluation to inform clinical decision-making. This study aims to address the controversy by systematically comparing the safety profiles of PICC and MC, focusing on complications, cost, and patient satisfaction. Our findings suggest that PICC generally have fewer complications (catheter-related thrombosis [DVT+SVT], catheter-related SVT, infiltrations, and leaks) but are associated with higher costs and greater patient dissatisfaction compared to MC.
Thrombosis is a primary concern with the use of vascular access devices. Our study showed that the rate of catheter-related thrombosis (DVT+SVT) was higher in the MC group, especially when evaluated per catheter days. These results are consistent with previous studies that reported a higher risk of thrombosis with MC, likely due to their shorter length and positioning in peripheral veins, which may predispose patients to venous irritation and subsequent clot formation. Reference Tripathi, Kumar and Kaushik26 In contrast, PICCs extend into larger central veins, potentially providing better hemodilution of infused substances and a reduced risk of thrombosis. Reference Lago, Tiozzo, Boccuzzo, Allegro and Zacchello27 The longer duration of PICC placement, averaging 30.49 days compared to 18.24 days for midlines, may also contribute to the higher rate of thrombosis observed in the PICC group. The prolonged catheter placement may cause mechanical irritation to the vessel wall, leading to endothelial damage and promoting thrombus formation. Reference Siddiqui, Coughlin, Koenen, Al-Yaman, Bestgen and Regueiro28 Additionally, the extended exposure time allows for a greater accumulation of fibrin and other clotting factors around the catheter, which could increase the likelihood of developing DVT. Reference Liu, He, Zeng, Yue, Wei and Zeng29 Moreover, the presence of the catheter over a longer period increases the risk of CRBSIs, which are known to contribute to a hypercoagulable state and further elevate the risk of thrombosis. Reference Sánchez Cánovas, García Torralba, Blaya Boluda, Sánchez Saura, Puche Palao and Sánchez Fuentes30 However, it is important to note that PICCs are not without thrombotic complications, necessitating vigilant monitoring and management to mitigate these risks. Reference Zochios, Umar, Simpson and Jones31
Beyond thrombosis, other complications associated with these catheters are also critical. Our analysis revealed that MC had higher incidences of infiltrations and leaks, complications that can significantly affect patient comfort and safety. Reference Sharp, Esterman, McCutcheon, Hearse and Cummings7 Conversely, PICCs were more frequently associated with CRBSIs, severe complications that require prompt medical intervention. Reference Mai, Cui, Wang, Tan, Xian and Pai32 This discrepancy suggests that although MC may be preferable in scenarios where reducing the risk of CRBSIs is paramount, PICCs might be more suitable for longer-term use where infiltration and leakage are primary concerns. Reference Seo, Altshuler, Dubrovskaya, Nunnally, Nunn and Ello5 Notably, the lower rates of catheter occlusion and phlebitis in PICCs suggest a more favorable profile for long-term use in stable patients. Reference Meto, Cabout, Rosay, Espinasse, Lot and Hajjam33
Cost and patient satisfaction are crucial factors influencing the choice of vascular access devices. Our study found that PICCs incur higher costs due to their more complex insertion and maintenance protocols, contributing to higher dissatisfaction rates reported among patients. Reference Chen, Yue, Liao and Li34 The dissatisfaction associated with PICCs may be attributed to the frequent need for maintenance and the discomfort linked to long-term central venous access. On the other hand, MCs, despite their lower costs, often lead to higher complication rates, potentially increasing overall healthcare costs due to the additional treatments required to manage these complications. Reference Lee, Ryu, Hong, Cho, Hong and Bae35 Balancing these factors is vital to optimizing patient outcomes and healthcare resource utilization. Additionally, the patient satisfaction aspect sheds light on the holistic patient care approach. The higher dissatisfaction rates in PICC users could be a result of the invasive nature of the procedure and the associated discomfort over extended periods. Reference Buchanan, Burt, Moureau, Murray and Nizum36 In contrast, MCs, being less invasive, tend to offer better patient comfort despite their higher complication rates. This dichotomy suggests a nuanced approach to catheter selection where patient preferences and clinical indications must be harmonized.
The limitations of this meta-analysis should be considered when interpreting the results. First, the included studies vary in design, population characteristics, and clinical settings, introducing heterogeneity into the analysis. Second, the quality of evidence, as assessed by the GRADE approach, was generally low to very low, reflecting potential biases and limitations in the primary studies. Thirdly, none of the included studies specified whether thrombosis and other adverse events occurred during or after catheter placement, making it challenging to analyze the causes of these complications. Additionally, the reliance on published data may result in publication bias, as studies with negative results are less often published. Future research should include high-quality RCTs with standardized outcome measures to provide more robust evidence. Despite these limitations, our findings contribute valuable insights into the comparative safety profiles of PICC and MC. The higher thrombosis rates observed with MC highlight the need for careful consideration of patient-specific factors when selecting a vascular access device. For instance, patients with a higher risk of thrombotic events may benefit more from PICC, despite their higher costs and maintenance requirements. Conversely, in settings where the risk of infection is a primary concern, and short-term access is sufficient, MC might be the preferred choice.
Conclusion
PICC appears to be a safer method of intravenous catheterization for adult patients, with fewer complications compared to MC. However, the higher cost and patient dissatisfaction associated with PICC require careful consideration. Clinicians should tailor catheter selection to individual patient needs, balancing the risk of complications with cost and patient comfort to optimize care outcomes. Future research should focus on high-quality RCTs to further clarify the comparative safety and efficacy of these vascular access devices.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/ice.2024.190.
Data availability statement
Data is provided within the manuscript or supplementary information files.
Acknowledgments
The authors thank Professor Wenxiong Zhang, MD (The second affiliated hospital of Nanchang University) for his statistical advice.
Author contribution
Juan Qiu had full access to all the data in the manuscript and took responsibility for the integrity of the data and the accuracy of the data analysis. All authors read and approved the final manuscript.
Concept and design: Jianyun Wen, Shuping Xiong, Ziwei Tu, Ping Lin, Yeqin Yuan, Wenhong Fu, and Juan Qiu.
Acquisition, analysis, or interpretation of data: Jianyun Wen, Shuping Xiong, Ziwei Tu, Ping Lin, Yeqin Yuan, Wenhong Fu, and Juan Qiu.
Statistical analysis: Jianyun Wen, Shuping Xiong, Ziwei Tu, and Ping Lin.
Drafting of the manuscript: Jianyun Wen, Shuping Xiong, Ziwei Tu, and Juan Qiu.
Critical revision of the manuscript for important intellectual content: Jianyun Wen, Shuping Xiong, Ziwei Tu, and Juan Qiu.
Supervision: Jianyun Wen, and Juan Qiu.
Financial support
This study was supported by the Scientific and Technological Projects of Jiangxi Provincial Health Commission (grant number: SKJP220228121). Role of the Funding: The funding had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Competing interests
None.
Ethics standard
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study, formal consent is not required.









