



No CrossRef data available.
Article contents
Outcomes of clinical decision support for outpatient management of Clostridioides difficile infection
Published online by Cambridge University Press: 29 September 2021
Abstract
Objective:
To determine the impact of clinical decision support on guideline-concordant Clostridioides difficile infection (CDI) treatment.
Design:
Quasi-experimental study in >50 ambulatory clinics.
Setting:
Primary, specialty, and urgent-care clinics.
Patients:
Adult patients were eligible for inclusion if they were diagnosed with and treated for a first episode of symptomatic CDI at an ambulatory clinic between November 1, 2019, and November 30, 2020.
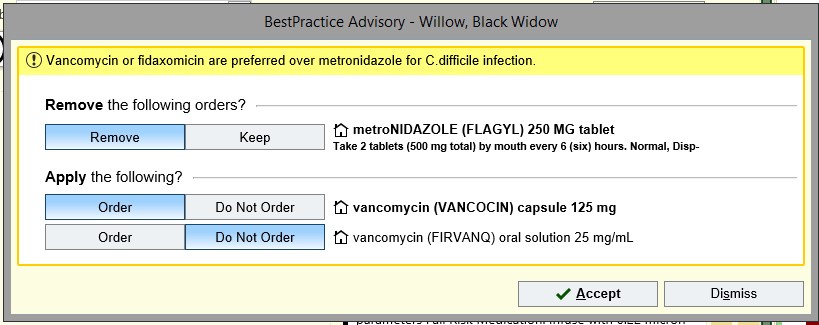
Interventions:
An outpatient best practice advisory (BPA) was implemented to notify prescribers that “vancomycin or fidaxomicin are preferred over metronidazole for C.difficile infection” when metronidazole was prescribed to a patient with CDI.
Results:
In total, 189 patients were included in the study: 92 before the BPA and 97 after the BPA. Their median age was 59 years; 31% were male; 75% were white; 30% had CDI-related comorbidities; 35% had healthcare exposure; 65% had antibiotic exposure; 44% had gastric acid suppression therapy within 90 days of CDI diagnosis. The BPA was accepted 23 of 26 times and was used to optimize the therapy of 16 patients in 6 months. Guideline-concordant therapy increased after implementation of the BPA (72% vs 91%; P = .001). Vancomycin prescribing increased and metronidazole prescribing decreased after the BPA. There was no difference in clinical response or unplanned encounter within 14 days after treatment initiation. Fewer patients after the BPA had CDI recurrence within 14–56 days of the initial episode (27% vs 7%; P < .001).
Conclusions:
Clinical decision support increased prescribing of guideline-concordant CDI therapy in the outpatient setting. A targeted BPA is an effective stewardship intervention and may be especially useful in settings with limited antimicrobial stewardship resources.
- Type
- Original Article
- Information
- Copyright
- © The Author(s), 2021. Published by Cambridge University Press on behalf of The Society for Healthcare Epidemiology of America
References
Antibiotic resistance threats in the United States, 2019. Centers for Disease Control and Prevention website. https://www.cdc.gov/drugresistance/pdf/threats-report/2019-ar-threats-report-508.pdf. Published 2019. Accessed September 10, 2021.Google Scholar
McDonald, LC, Gerding, DN, Johnson, S, et al. Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin Infect Dis 2018;66(7):e1–e48.CrossRefGoogle Scholar
Morrison, AR, Kenney, RM, Outpatient, Davis SL.
Clostridioides difficile infections: an opportunity for antimicrobial stewardship programs. Infect Control Hosp Epidemiol 2020;41:969–971.CrossRefGoogle ScholarPubMed
Drekonja, DM, Filice, GA, Greer, N, et al. Antimicrobial stewardship in outpatient settings: a systematic review. Infect Control Hosp Epidemiol 2015;36:142–152.CrossRefGoogle ScholarPubMed
Wenzler, E, Mulugeta, SG, Danziger, LH. The antimicrobial stewardship approach to combating Clostridium difficile
. Antibiotics (Basel) 2015;4:198–215.CrossRefGoogle ScholarPubMed

Wu et al. supplementary material
Wu et al. supplementary material
Image
68.5 KB