



Introduction
Infectious intestinal disease (IID), an infection of the gastrointestinal (GI) tract that causes gastroenteritis, is estimated to affect 274 people per 1,000 population in the UK per year [Reference Tam, Viviani, Adak, Bolton, Dodds, Cowden, Evans, Gray, Hunter, Jackson and Letley1]. While most cases are mild and self-limiting, some pathogens can cause bloody diarrhoea, septicaemia, meningitis, renal failure, or death [Reference Tam, Viviani, Adak, Bolton, Dodds, Cowden, Evans, Gray, Hunter, Jackson and Letley1]. Approximately half of the people reporting IID have missed work or school due to their symptoms, and for particular pathogens, public health measures require the exclusion of individuals in certain risk groups (including children aged five and under, food-handlers, and healthcare workers) from childcare, school, or workplace settings [Reference Tam, Viviani, Adak, Bolton, Dodds, Cowden, Evans, Gray, Hunter, Jackson and Letley1, Reference Ejidokun, Hawker, Lighton, Paranthaman, Stiff and Ward2]. Consequently, the negative impact of IID extends beyond clinical presentation, potentially affecting the financial and social situations of cases and their carers. In 2018, the societal cost of foodborne illness in the UK was estimated to be over 9 billion GBP [Reference Daniel, Casadevall, Sun, Sugden and Aldin3].
Additionally, due to the self-limiting nature of most cases of IID, national surveillance captures only a fraction of cases. For every single case reported to national surveillance, there is an estimated 147 cases in the community, with approximately 15 cases presenting to the general practice (GP) [Reference Tam, Viviani, Adak, Bolton, Dodds, Cowden, Evans, Gray, Hunter, Jackson and Letley1]. However, the estimates at different levels of the surveillance pyramid [Reference Lake, Nichols, Harrison, Bentham, Sari Kovats, Grundy and Hunter4] differ widely by pathogen, for example, from 5 cases in the community for every Salmonella case reported to national surveillance to 288 cases in the community for every norovirus case reported to national surveillance [Reference Tam, Viviani, Adak, Bolton, Dodds, Cowden, Evans, Gray, Hunter, Jackson and Letley1].
Studies conducted at different levels of the surveillance pyramid have found heterogeneity in the association of socioeconomic deprivation with illness [Reference Adams, Rose, Elliot, Smith, Morbey, Loveridge, Lewis, Studdard, Violato, O’Brien, Whitehead, Taylor-Robinson, Hawker and Barr5–Reference Tam, Rodrigues, Viviani, Dodds, Evans, Hunter, Gray, Letley, Rait, Tompkins and O’Brien8]. In addition, most community or primary care level studies only examine the combined IID/gastroenteritis clinical syndrome rather than the relationship for individual IID pathogens. As the most common transmission routes (for example, person–person, foodborne, zoonotic, environmental) and sources/vehicles of infection vary by pathogen, it cannot be assumed that the relationship between infection and socioeconomic factors is the same for each pathogen. In addition, considering the differences in ascertainment at each level of the surveillance pyramid across pathogens, it is likely that the proportion of each IID pathogen included in each study differs. Analyses of datasets comprising cases linked to a microbiologically confirmed IID would therefore add considerably to the evidence base.
In this paper, we present the analysis of a large national dataset of laboratory-diagnosed IID from England. The aim of this study is to analyse the association between socioeconomic deprivation and the incidence of IID reported to national surveillance by pathogen. The objectives were to (1) compare crude incidence for each GI pathogen by index of multiple deprivation (IMD) quintile and (2) analyse the association between IMD quintile and incidence of each pathogen at the neighbourhood level (lower super output area, LSOA).
Methods
Data sources
The second generation surveillance system (SGSS) is UK Health Security Agency’s (UKHSA) primary method for collecting data on infections of clinical significance and antimicrobial resistance from laboratories across England, Northern Ireland, and Wales. Introduced in 2014, it replaced the legacy LabBase2, CoSurv, and AmSurv applications that had previously supported the reporting of laboratory surveillance data to Public Health England (PHE) and predecessor organisations. The system enables laboratories to meet their statutory obligation under the Health Protection (Notification) Regulations to report laboratory-confirmed cases of infection to UKHSA [9].
During the reporting period of this study, 127 microbiology and virology NHS and private laboratories across England reported results to SGSS. Guidance on what, when, and how they report is documented in the guide for diagnostic laboratories [9].
Data from the UKHSA SGSS was extracted from 1 January 2015 to 13 December 2018 (inclusive) for Salmonella, Campylobacter, Shigella, Giardia species, and norovirus. These data include demographic characteristics for laboratory-confirmed cases of infection in England. Transmission pathways for each pathogen are included in the Supplementary Materials [Reference de Wit, Koopmans and van Duynhoven10–Reference Ajmera and Shabbir15] (Supplementary Table 1A). Certain pathogens were excluded because the SGSS data was not complete. A number of other pathogens available in the SGSS database (such as STEC) was.
Each case was assigned to a lower super output area (LSOA), which are zones representing neighbourhoods (∼1500 people) based on their residential postcode, using data available from the Office for National Statistics (ONS) [16]. There are 32,844 LSOAs in England. Socio-demographic data were obtained from the ONS and included rural/urban classification, region of England, travel abroad (Yes, No, Unsure), population by year by age (Child, if <20 years old, and Adults, if ≥20 years old) and sex (Male and Female), all at the LSOA level [16]. Area-level socioeconomic deprivation was measured through matching the individual’s LSOA of residence to the 2019 IMD [17]. The IMD is a composite measure based on seven weighted domains: income; employment; health; education; barriers to housing and services; crime; and living environment. Mean distance to a GP for each LSOA was obtained from the PHE Fingertips website [18]. Individuals who had missing age, sex, or rural/urban classification data were excluded from the multivariable logistic regression analysis.
Analysis
For the first objective, rates were calculated per 100,000 person-years by IMD quintile, using the mid-year population estimates by LSOA for 2015, 2016, 2017, and 2018. Salmonella and Shigella were disaggregated by species to reflect differing transmission pathways. 95% confidence intervals (CI) were calculated with the ‘PHEindicatormethods’ package, which used Byar’s method [Reference Breslow and Day19]. Rate ratios (RR), with 95% CI comparing the most deprived quintile with the least deprived quintile, were calculated with the ‘epitools’ package, which used the Wald test. All analyses were done in R version 4.2.1.
The second objective involved an ecological analysis using the LSOA as the unit of analysis. Univariate and multivariable ordinal logistic regression models were used, with categorised count of cases as the outcome and person-years as one of the covariates. In the former case, IMD quintile was added as a categorical variable, whereas in the latter case sex (Male and Female), age (Age groups 0–4, 5–9, 10–14, 20–59, 60–69, and ≥70), rurality/urbanicity, and distance to the GP (0–549 m, 550–1099 m, 1100–2199 m, and ≥2200 m) were also added as categorical variables, together with interaction between rurality/urbanicity and distance to the GP. The 1st IMD quintile represented the least deprived areas, while the 5th IMD quintile represented the most deprived areas. The p-values were obtained by means of the (composite) Wald test and the significance level was taken to be 5%. Table 1 shows the case categories chosen for each IID for both univariate and multivariable analysis, based on the distribution of counts for the IID in question. The proportionality of odds assumption was tested in the univariate and multivariable models using the gologit2 user-written ado program and method described in the article [Reference Williams20] for that program and executed in Stata 17.0, in which all inferential analyses were performed. In those cases where the assumption was not met, a generalised ordinal logistic regression model was fitted using the above program, where the obtained parameter estimates were then exponentiated to obtain overall odds ratios (ORs) for those parameters where the assumption appeared not to be violated, and separate ORs for each case category otherwise [Reference Janssen and Snowden14]. In all cases, their 95% CIs were obtained and the measure of association, together with these CIs, is presented for the IMD quintile in the results section.
Table 1. Categories for the count of cases for each pathogen for univariate and multivariable analysis

Results
Overview of the epidemiology and microbiological data
There was a total of 314,381 cases reported to SGSS during the 4-year study period, of which 167,299 (53%) were male and 59,827 (19%) were children (Supplementary Table 1A). Distribution of cases across regions ranged from 6% (n = 17,831) in the north east of England to 18% (n = 56,331) in the south east of England. Most cases (n = 249,802, 79%) lived in urban areas, and 4% of cases (n = 12,743) reported travelling outside the UK within 7 days of onset of symptoms (Supplementary Table 1A). About two-thirds (n = 208,016) of cases were infected with Campylobacter species, 6% with Giardia (n = 18,114), 6% with Cryptosporidium (n = 18,743), 8% with norovirus (n = 26,361), 8% with non-typhoidal Salmonella (n = 26,361), 3% with Salmonella typhi/paratyphi (n = 8,690), and 3% with Shigella (n = 8,096). Of the Shigella diagnoses that were speciated (76%), 2,135 cases were infected with Shigella flexneri and 3,597 were infected with Shigella sonnei. Cryptosporidium speciation data were incomplete on SGSS and thus were excluded from subsequent analysis. The more deprived quintiles were slightly more represented in the study sample than the two least deprived quintiles, with 68,211 (22%) cases representing the most deprived quintile and 51,858 (16%) cases representing the least deprived quintile. IMD quintile classification was not conducted for 134 cases (0.04%) due to a lack of valid postcodes (Supplementary Table 2A). Six hundred and eighty-five individuals had data missing of sex variable, 567 of age variable, and 134 of rural/urban classification variable, which represented approximately 0.2% of the total cases.
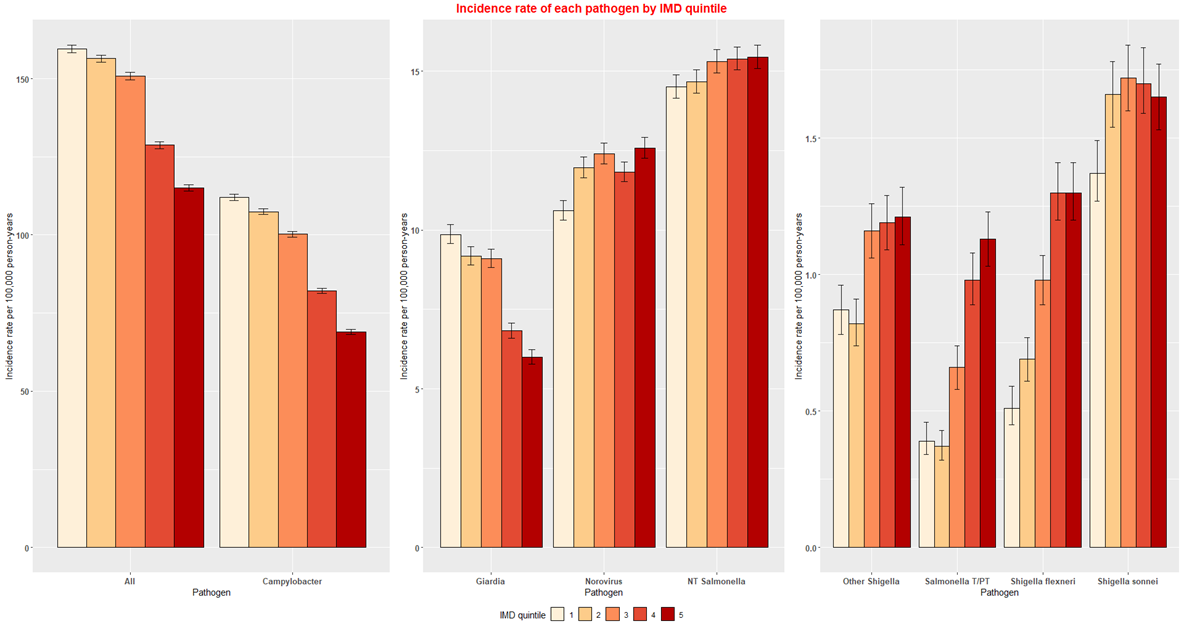
Comparison of crude incidence for each GI pathogen by IMD quintile
There was a clear trend of decreasing likelihood of (a laboratory report with) all IID pathogens with increasing deprivation, with each quintile statistically significantly lower than the preceding quintile. Comparing the lowest and highest quintiles, the rate in the most deprived quintile was 28% lower than that of the least deprived quintile (RR = 0.72; 95% CI: 0.71–0.73) (Table 2 and Supplementary Figure 1A). The incidence of Campylobacter species and Giardia decreased with increasing deprivation, with both pathogens showing a clear trend of each quintile being lower than the preceding one. The most deprived quintile had a 38% lower rate of Campylobacter (RR = 0.62; 95% CI: 0.61–0.62) and 39% lower rate of Giardia (RR = 0.61; 95% CI: 0.58–0.64) as compared to the least deprived quintile (Table 2 and Supplementary Figure 1A). Conversely, the incidence of norovirus, non-typhoidal Salmonella, S. typhi/paratyphi, S. flexneri, S. sonnei, and other Shigella increased with increasing deprivation, with all showing a generic trend across the five quintiles. The most deprived quintile had an 18% higher rate of norovirus (RR = 1.18; 95% CI: 1.14–1.23), 6% higher rate of non-typhoidal Salmonella (RR = 1.06; 95% CI: 1.03–1.10), 187% higher rate of S. typhi/paratyphi (RR = 2.87; 95% CI: 2.41–3.42), 152% higher rate of S. flexneri (RR = 2.52; 95% CI: 2.16–2.95), 20% higher rate of S. sonnei (RR = 1.20; 95% CI: 1.08–1.34), and 40% higher rate of other Shigella (RR = 1.40; 95% CI: 1.23–1.60) as compared to the least deprived quintile (Table 2 and Supplementary Figure 1A).
Table 2. Incidence rate of each pathogen by IMD quintile and RR by each pathogen comparing the most deprived quintile (5) to the least deprived quintile (1)

Analysis of the association between IMD quintile and incidence rates of each pathogen
Univariate analysis showed that higher deprivation was significantly associated with higher odds of a higher number of cases for S. sonnei, other Shigella, S. flexneri, and S. typhi/paratyphi (Table 3). A similar trend was seen for norovirus (Table 4), for which quintile 3 and quintile 5 (most deprived) had the highest odds of a higher number of cases. For non-typhoidal Salmonella, there was no clear trend with all ORs being close to 1, with the exception of the two most deprived quintiles which showed slightly higher odds of a higher number of cases (Table 4). Univariate analysis results showed that higher deprivation was significantly associated with lower odds of a higher number of cases for Giardia (Table 4) and Campylobacter (Table 5).
Table 3. Univariate logistic regression for pathogens with case categories 0, 1, ≥2

Table 4. Univariate logistic regression for pathogens with case categories 0, 1, 2, ≥3

Table 5. Univariate logistic regression for pathogens with case categories 0–5, 6–10, ≥11

Multivariable analysis results showed that higher deprivation was significantly associated with lower odds of a higher number of cases for Giardia and Campylobacter (Table 6). There was a similar trend for S. sonnei, but not all quintiles were significant. Multivariable analysis showed that higher deprivation was significantly associated with higher odds of a higher number of cases for S. flexneri, norovirus, and S. typhi/paratyphi (Table 6). For other Shigella and non-typhoidal Salmonella, there was no clear trend with all ORs being close to 1 and CI including 1 for all or most quintiles (Table 6).
Table 6. Multivariable analysis results for all pathogens

a Multivariable analysis adjusted for categorical sex, age, rurality/urbanicity, distance to the GP, and interaction between rurality/urbanicity and distance to the GP.
b *p < 0.05, **p < 0.01, ***p < 0.001.
Discussion
In this study, which used national surveillance data, we found a heterogeneous relationship between deprivation and incidence of laboratory-confirmed GI infections that varied by pathogen. Previous studies carried out in the UK and elsewhere reported an association between a high incidence of GI infections and high levels of deprivation. For example, a nationally representative analysis of 24 million calls to NHS telephone helplines for health advice in England found that there was a greater risk of GI calls from more disadvantaged areas compared to less disadvantaged areas [Reference Adams, Rose, Elliot, Smith, Morbey, Loveridge, Lewis, Studdard, Violato, O’Brien, Whitehead, Taylor-Robinson, Hawker and Barr5]. Retrospective, cross-sectional studies from different countries found a positive link (telephone-based population studies from Australia and the US) [Reference Hall, Kirk, Ashbolt, Stafford and Lalor21, Reference Herikstad, Yang, Van Gilder, Vugia, Hadler, Blake, Deneen, Shiferaw and Angulo22], no link (telephone-based population study from Canada) [Reference Majowicz, Doré, Flint, Edge, Read, Buffett, McEwen, McNab, Stacey, Sockett and Wilson23], or an inverse association (postal questionnaire from Australia) [Reference Bytzer, Howell, Leemon, Young, Jones and Talley24] between socioeconomic status and having suffered an episode of GI illness. In contrast, we reported a lower proportion of notifications of GI infection in cases living in deprived areas. However, the analysis suggests that this result reflects the high proportion of Campylobacter infections in the dataset.
Overall, pathogens that had common routes of transmission had similar associations with the level of deprivation. For waterborne pathogens, such as Giardia, the incidence was lower in areas of higher deprivation, even after accounting for rural/urban differences. For pathogens most frequently associated with foodborne transmission, including Campylobacter and non-typhoidal Salmonella, the incidence was also lower in areas of higher deprivation, especially in the multivariable model. For pathogens transmitted by person-to-person contact, specifically norovirus, Shigella species, and S. typhi/paratyphi, incidence was higher in more deprived neighbourhoods in the crude analysis and univariate model, although results varied in the multivariable models. This indicates that for person-to-person transmission, confounders, such as age and sex, had the biggest impact on the results. Less commonly, human host-adapted pathogens such as Shigella, may be waterborne or foodborne, particularly in individuals who travelled to developing countries [Reference Serafino Wani, Filson, Chattaway and Godbole11]. Shigella, Campylobacter, and Giardia are also associated with sexual transmission in men who have sex with men (MSM) [Reference Serafino Wani, Filson, Chattaway and Godbole11].
Our results support the hypothesis that pathogen transmission routes may have an impact on the association with IMD. A systematic review on the impact of socioeconomic status on foodborne illness in high-income countries also found an association between infection with Campylobacter and Salmonella species and higher socioeconomic status [Reference Newman, Leon, Rebolledo and Scallan25]. Another systematic review investigating the relationship between socioeconomic status and GI infections in developed countries found that among lower socioeconomic groups, the risk of infection was significantly higher from pathogens spread by person-to-person transmission, compared to foodborne pathogens [Reference Adams, Rose, Hawker, Violato, O’Brien, Barr, Howard, Whitehead, Harris and Taylor-Robinson26]. The study also found that the risk of GI infection for lower socioeconomic status (higher deprivation) was on average significantly higher among studies which analysed hospital cases, compared to studies that analysed laboratory-recorded cases [Reference Adams, Rose, Hawker, Violato, O’Brien, Barr, Howard, Whitehead, Harris and Taylor-Robinson26]. The review also highlighted that the relationship between incidence and deprivation was much stronger in children than in adults. The study by Payment (2001) also found that the proportion of GI infections caused by the different routes of exposure varied significantly across communities due to varying behavioural and socioeconomic factors [Reference Payment27].
Previous studies have highlighted overcrowded homes with fewer washing and toilet facilities per person to be associated with a higher incidence of GI infection in more deprived areas [28]. We might therefore expect GI pathogens transmitted primarily by close person-to-person contact to have a higher incidence in more deprived areas. Our analyses supported these findings, showing that a higher proportion of cases living in deprived areas reported GI infections caused by S. flexneri species, S. typhi/paratyphi, and norovirus. These three pathogen groups do not have significant animal reservoirs, and are often associated with household transmission, institutional outbreaks, and outbreaks among people living in close communities [Reference de Wit, Koopmans and van Duynhoven10, Reference Serafino Wani, Filson, Chattaway and Godbole11]. Outbreaks of S. sonnei and S. flexneri have also been detected among MSM in the UK and other developed countries [Reference Serafino Wani, Filson, Chattaway and Godbole11].
Of the zoonotic, foodborne GI pathogens that are rarely associated with person-to-person transmission, Campylobacter and non-typhoidal Salmonella were reported less frequently among cases living in deprived areas. Our results could be influenced by the fact that individuals who consume fast foods, travellers to low- and middle-income countries, as well as those who live in rural areas and have regular contact with livestock have increased risk of Campylobacter infection [Reference Bessell, Matthews, Smith-Palmer, Rotariu, Strachan, Forbes, Cowden, Reid and Innocent29]. Adams et al. [Reference Adams, Rose, Hawker, Violato, O’Brien, Whitehead, Barr and Taylor-Robinson6] also suggested that a lower risk of GI infection caused by certain foodborne pathogens in individuals living in deprived areas may be due to reduced opportunities to eat out and less frequent consumption of high-risk foods, such as unpasteurised dairy products.
Zoonotic GI pathogens may be transmitted to humans via multiple routes [Reference Dunn and Juergens12, Reference Janssen and Snowden14]. Factors such as exposure to contaminated recreational water, and international travel have been linked to a higher incidence of GI infection in less deprived individuals [Reference Janssen and Snowden14]. Moreover, individuals living in affluent rural areas are more likely to have contact with animals and the environment, and therefore their risk of infection is increased despite their higher economic status [Reference Leitch and He30].
Travel outside the UK, especially to countries where specific GI pathogens are endemic, may increase the risk of infection. In the UK, 95% of S. typhi/paratyphi cases have a history of travel to an endemic area, and the remaining cases are acquired through contact with an infected traveller [Reference Ejidokun, Hawker, Lighton, Paranthaman, Stiff and Ward2]. Adams et al. [Reference Adams, Rose, Hawker, Violato, O’Brien, Whitehead, Barr and Taylor-Robinson6] suggested that individuals in deprived areas may be less likely to travel abroad, and this risk factor may therefore impact more on individuals from affluent areas. However, as with foodborne exposures, the assumption that travellers are from the least deprived areas is confounded by the frequency of travel by individuals living in high-deprivation areas to high-risk countries to visit family and friends [Reference Ejidokun, Hawker, Lighton, Paranthaman, Stiff and Ward2].
The strength of the study was the use of nationally representative laboratory data, which is the most comprehensive source of clinical data on individual GI pathogens for England, which allowed the analysis of specific pathogens and their associated transmission routes. However, the use of national surveillance data results in a dataset that over-represents pathogens such as Campylobacter and under-represents the true burden of norovirus infection in the community, which limits generalisability at the level of the community. The data from the second study of infectious intestinal disease in the community (IID2 Study) from 2008 to 2009 [Reference Tam, Viviani, Adak, Bolton, Dodds, Cowden, Evans, Gray, Hunter, Jackson and Letley1] estimated that for every case of Salmonella captured by national surveillance, there were 1.4 GP consultations and approximately 5 community cases; and for cases of campylobacteriosis, there were 1.3 GP consultations and 9.3 community cases. For every case of norovirus reported to national surveillance, there were 2.3 GP consultations and 288 community cases [Reference Tam, Viviani, Adak, Bolton, Dodds, Cowden, Evans, Gray, Hunter, Jackson and Letley1]. Patients reporting IID are only routinely tested for norovirus if they are children less than 5 years of age, adults over 60 years, food-handlers, or immunocompromised patients [Reference Tam, Viviani, Adak, Bolton, Dodds, Cowden, Evans, Gray, Hunter, Jackson and Letley1]. For every national surveillance case of Giardia, there were 1.5 GP consultations and approximately 14 community cases [Reference Tam, Viviani, Adak, Bolton, Dodds, Cowden, Evans, Gray, Hunter, Jackson and Letley1]. Faecal samples are not routinely tested for Giardia as criteria for testing often include a history of travel [Reference Dunn and Juergens12]. Ethnicity may interact with deprivation in that ethnic groups with ties to countries where Giardia is endemic may be more likely to travel, and therefore be tested for Giardia, than other ethnic groups.
Testing patterns by geography and deprivation status were not investigated in this study as the dataset contained only positive, infected cases. Consequently, the data may reflect testing bias and differences in access to health services. A systematic review [Reference Willems, De Maesschalck, Deveugele, Derese and De Maeseneer31] also showed that patients from lower social classes faced less participatory consultations, which reduced information sharing. Previous studies in the UK also showed lower reporting rates for GI infections among more deprived individuals [Reference Olowokure, Hawker, Weinberg, Gill and Sufi32]. Additionally, laboratory cases generally reflect the most clinically severe cases, and while socioeconomic deprivation is associated with more severe illness, pathogens such as norovirus usually cause short-lived symptoms [Reference Tam, Viviani, Adak, Bolton, Dodds, Cowden, Evans, Gray, Hunter, Jackson and Letley1]. Consequently, the association of lab-reported incidence of norovirus with socioeconomic deprivation found in this study may be more likely to reflect the incidence of outbreak-associated norovirus or those in targeted groups. Other potential confounders, such as ethnicity and travel patterns, were not included in the analysis. For example, there are known ethnic differences in the risk of Campylobacter infection in the UK [Reference Gillespie, O’Brien, Penman, Tompkins, Cowden and Humphrey13, Reference Manaseki, Hawker and Ali33]. Finally, as this was an ecological analysis, conclusions cannot be drawn regarding individual risk factors and how they can be targeted to reduce inequalities among deprived groups.
Our study showed that incidence rates can potentially vary across deprivation quintiles, depending on the pathogen and its transmission route, based on laboratory data. Our results were consistent in showing that infections most strongly associated with areas of increasing deprivation were those transmitted by person–person contact, and that those transmitted by zoonotic contamination of the environment were least likely to be associated with areas of deprivation. The development, introduction, and mobilisation of safe and effective vaccines against GI pathogens which transmit from person to person and target risk groups, such as children, should be a priority for prevention. As evidenced by the paediatric rotavirus immunisation, GI vaccine introductions can help to reduce socioeconomic inequalities in disease burden (both health and socioeconomic) [Reference Hungerford, Vivancos, Read, Iturriza-Gόmara, French and Cunliffe34]. Vaccination against S. typhi is recommended for travellers to endemic areas such as parts of Asia (such as India, Pakistan, and Bangladesh) to prevent the infection [Reference Sulieman35]. There are currently no licensed vaccines for noroviruses, Giardia, Campylobacter, and Shigella, although several candidates are under development [Reference Debbink, Lindesmith and Baric36–Reference Böhles, Böhles, Busch, Busch, Hensel and Hensel40].
Further research could investigate the relationship between the type of symptomatic healthcare presentation and the number of total laboratory samples from primary care/hospitals and deprivation. Primary care and hospitals have access to total faecal samples, including negative samples, which are not reported to SGSS. Self-reporting of GI symptoms and stool sample testing, for example through a website app, could allow us to understand testing patterns for GI by socio-demographic and spatial measures [Reference Davies, Iturriza-Gómara, Glennon-Alty, Elliot, Vivancos, Alvarez Nishio, Cunliffe and Hungerford41]. It would also be interesting to investigate whether ethnicity has an impact on the incidence rates as suggested by other studies [Reference Gillespie, O’Brien, Penman, Tompkins, Cowden and Humphrey13, Reference Manaseki, Hawker and Ali33].
The findings of this study suggest that at the level of national laboratory surveillance, the incidence of pathogens that are most strongly associated with increasing deprivation are those transmitted by person–person spread and least strongly associated are those transmitted by zoonotic contamination of the environment. Previous studies have shown an increased risk of IID in more deprived regions, particularly in children, at community, primary care, and hospital levels [Reference Adams, Rose, Hawker, Violato, O’Brien, Whitehead, Barr and Taylor-Robinson6]. We therefore suggest that the most effective solution for the reduction of IID inequalities is prioritising the reduction of person-to-person infections’ spread, especially in children.
Abbreviations
- CI
-
confidence interval
- GI
-
gastrointestinal
- GP
-
general practice
- IID
-
infectious intestinal disease
- IMD
-
index of multiple deprivation
- LRT
-
likelihood ratio test
- LSOA
-
lower super output area
- MSM
-
men who have sex with men
- ONS
-
Office for National Statistics
- OR
-
odds ratio
- PHE
-
Public Health England
- RR
-
rate ratio
- SGSS
-
second generation surveillance system
- UKHSA
-
United Kingdom Health Security Agency
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0950268823000869.
Data availability statement
The data that support the findings of this study are available from UKHSA, but restrictions apply to the availability of these data, which were used under licence for the current study, and so are not publicly available. Aggregated data are, however, available from the authors upon reasonable request and with the permission of UKHSA.
Acknowledgements
The authors acknowledge the contributions of Theme 1 (People and Places) NIHR Health Protection Research Unit in Gastrointestinal Infections members.
Author contribution
L.B. and J.H. conceptualised and designed the study. L.B. and C.J. were responsible for supervision. M.B. and S.B. were responsible for investigation, validation, and formal analysis. A.-M.O. was responsible for data curation. M.B. and S.B. were responsible for writing the original draft. J.H. was responsible for funding acquisition. N.Q.V. provided statistical support. M.B., S.B., C.J., D.H., J.H., and L.B. edited the manuscript. All authors read and approved the final manuscript.
Funding statement
This study is funded by the National Institute for Health and Care Research (NIHR) Health Protection Research Unit in Gastrointestinal Infections, a partnership between the UK Health Security Agency, the University of Liverpool, and the University of Warwick. The views expressed are those of the author(s) and not necessarily those of the NIHR, the UK Health Security Agency, or the Department of Health and Social Care.
Competing interest
The authors declare that they have no competing interests.
Ethical standard
The UKHSA has approval to handle data obtained through laboratory surveillance under Regulation 3 of the Health Service (Control of Patient Information) Regulations 2002. Informed patient consent was not required as UKHSA has the authority to handle patient data for public health monitoring and infection control under Section 251 of the UK National Health Service Act 2006.










 Open access
Open access