



Babies born during the COVID-19 pandemic have lived in an unusual environment both prenatally and after birth. Since its outbreak in March of 2020, the pandemic has resulted in severe and prolonged health alerts and unpredictable lifestyle restrictions that have followed nonlinear trends across countries throughout the 2020–2021 2-year period. We now have sufficient evidence about the widespread and unintended consequences for individuals and societies and the overall increase in mental health symptomatology secondary to the pandemic in the general population (Guo et al., Reference Guo, De Carli, Lodder, Bakermans-Kranenburg and Riem2021; Holmes et al., Reference Holmes, O'Connor, Perry, Tracey, Wessely, Arseneault, Ballard, Christensen, Cohen Silver, Everall, Ford, John, Kabir, King, Madan, Michie, Przybylski, Shafran, Sweeney and Bullmore2020; Vindegaard & Benros, Reference Vindegaard and Benros2020). Especially for the perinatal health of mother and child, the pandemic has been severely detrimental, bringing multiple stressors to dynamic and susceptible psychobiological systems. In fact, before birth, future mothers' exposure to stressful life events, psychological distress, and/or mental health difficulties during pregnancy poses serious health risks to the fetus through psychobiological alterations that change their in-utero growth environment (Glover et al., Reference Glover, O’Donnell, O’Connor and Fisher2018). After birth, stressful experiences and postpartum mental health difficulties in new parents significantly affect parenting behaviors and, consequently, infants' early social-emotional experiences (Bernard et al., Reference Bernard, Nissim, Vaccaro, Harris and Lindhiem2018; Field, Reference Field2010; Groh et al., Reference Groh, Fearon, van IJzendoorn, Bakermans-Kranenburg and Roisman2017).
Beyond individual differences and inequalities exacerbated by the pandemic (Gur et al., Reference Gur, White, Waller, Barzilay, Moore, Kornfield, Njoroge, Duncan, Chaiyachati, Parish-Morris, Maayan, Himes, Laney, Simonette, Riis and Elovitz2020), being pregnant during the COVID-19 outbreak exposed expectant mothers to unpredictable and unexpected consequences, including additional concerns for their own and their fetus’s health, drastic changes in prenatal care and/or the need to take additional precautions, fear of infection in attending hospitals, feelings of isolation, and the sense of uncertainty in portraying the postpartum period (Tomfohr-Madsen et al., Reference Tomfohr-Madsen, Racine, Giesbrecht, Lebel and Madigan2021). In addition, the postpartum experience during the spring-summer and fall-winter of 2020 likely added additional challenges, like feelings of pandemic fatigue, new health alerts, and a prolonged erosion of the availability of support networks. In particular, access to social support has been significantly damaged by the pandemic with consequences for maternal and infant health, including a risk to maternal mental health and an impoverishment of the infant’s opportunities for learning and social exchange (Takács et al., Reference Takács, Štipl, Gartstein, Putnam and Monk2021). Indeed, it has been observed that, under stressful conditions, social support plays a protective role in child development through an indirect effect on maternal well-being (Armstrong et al., Reference Armstrong, Birnie-Lefcovitch and Ungar2005; Green et al., Reference Green, Furrer and McAllister2007). The pandemic, by disrupting the effectiveness of traditional social networks, has exposed mothers and infants to the lack of this support, which is especially valuable in contexts of greatest need (Harrison et al., Reference Harrison, Moulds and Jones2021; Patrick et al., Reference Patrick, Henkhaus, Zickafoose, Lovell, Halvorson, Loch, Letterie and Davis2020).
Overall, the COVID-19 pandemic disrupted perinatal mother-infant health by exposing mothers to several acute stressors during pregnancy and postpartum and drastically limiting the dyad’s access to social support. After 2 years of the pandemic, a significant body of evidence testifies that maternal perinatal mental health struggled as a result of the pandemic (Tomfohr-Madsen et al., Reference Tomfohr-Madsen, Racine, Giesbrecht, Lebel and Madigan2021) and is a candidate for newborn health risks secondary to the pandemic (Firestein et al., Reference Firestein, Dumitriu, Marsh and Monk2022). Ongoing global research efforts are assessing the implications of the pandemic on infant health, and results to date have highlighted the role of maternal stress in pregnancy (Iqbal et al., Reference Iqbal, Burrin, Aydin, Beardsall, Wong and Austin2021), maternal anxiety, and parental postpartum stress (Provenzi et al., Reference Provenzi, Grumi, Altieri, Bensi, Bertazzoli, Biasucci, Cavallini, Decembrino, Falcone, Freddi, Gardella, Giacchero, Giorda, Grossi, Guerini, Magnani, Martelli, Motta and Nacinovich2021). However, to achieve a relational approach to maternal and newborn health during the COVID-19 pandemic, we still need longitudinal and prospective data to understand whether and how children born to expectant mothers during the COVID-19 epidemic (March to May of 2020) are affected by pandemic-related changes and whether this impact is differentially distributed according to maternal perinatal health experiences (e.g., exposure to stressful events, psychological distress, mental health, availability of social support).
In March of 2020, we designed a prospective longitudinal study that followed pregnant Italian women through the early stages of the COVID-19 pandemic and national lockdown and their infants up to 24 months of age. In this study, we propose a comprehensive and theoretical model of perinatal mother-infant health risks related to the COVID-19 pandemic (see Figure 1).

Figure 1. COVID-19-related perinatal mother-infant health model. Simplified depiction of the theoretical model hypothesized. The black arrows show the direct associations between maternal and infant health variables. The green arrows show the hypothesized indirect effects of the prenatal maternal health variables and postnatal maternal COVID-19 stressful events exposure on infant’s negative affect via the mediation of maternal mental health during postpartum. The gray arrow shows the association between maternal COVID-19 pandemic-related health in pregnancy and postpartum. The orange arrow represents the moderating effect of social support on the associations between COVID-19 stressful events exposure and infant’s negative affect.
Guided by recent studies on the transgenerational consequences of adverse environmental conditions, such as natural disasters, experienced during pregnancy (King et al., Reference King, Kildea, Austin, Brunet, Cobham, Dawson, Harris, Hurrion, Laplante, McDermott, McIntyre, O’Hara, Schmitz, Stapleton, Tracy, Vaillancourt, Dancause, Kruske, Reilly and Yong Ping2015; McLean et al., Reference McLean, Cobham, Simcock, Elgbeili, Kildea and King2018), we measured distinct dimensions to quantify individual differences in the potential impact of the pandemic on maternal health. We considered significant pandemic-induced life events as an index of environmental impact and pandemic-related maternal psychological stress levels as a subjective index. We modeled the associations between these two dimensions during and after pregnancy on maternal mental health and negative affect of their infants at 6 months of age – this being a sentinel indicator for risk of developmental psychopathology (Kostyrka-Allchorne et al., Reference Kostyrka-Allchorne, Wass and Sonuga-Barke2020). We hypothesize that lower perinatal maternal mental health due to the pandemic experience is associated with higher rates of children’s negative affect. Specifically, we test the indirect effects of COVID-19-related prenatal maternal variables and postnatal maternal exposure to COVID-19 stressful events on the child’s negative affect through mediating maternal mental health during a postpartum period. Indeed, the literature describes adult mental health as sensitive to both primary and secondary environmental stressors (Lock et al., Reference Lock, Rubin, Murray, Rogers, Amlôt and Williams2012) and is thought to transmit stress to child development through multiple biological and psychological mediators (Phua et al., Reference Phua, Kee and Meaney2020). We expect that such multiple stressors in pregnancy and severe postpartum life events may damage the delicate postpartum maternal mental health, which impacts the child’s temperament through altered mother-infant exchanges, bonding, and parenting behaviors. Furthermore, opposite to the hypothesized harmful effects of exposure to COVID-19 events and psychological stress, we expect a buffering role of social support networks on the degree of negative pandemic consequences. Indeed, lack of a social network has been shown to exacerbate the effects of pandemic stress in the general population (Lebel et al., Reference Lebel, MacKinnon, Bagshawe, Tomfohr-Madsen and Giesbrecht2020) and in postpartum women (Harrison et al., Reference Harrison, Moulds and Jones2021). We expect that increased social support during the postpartum stage may limit the impact of the extraordinary, strained living conditions of the pandemic, which have tended to erase the protective function of social networks for the mother-infant dyad (Giesbrecht et al., Reference Giesbrecht, Poole, Letourneau, Campbell and Kaplan2013; Takács et al., Reference Takács, Štipl, Gartstein, Putnam and Monk2021). We hypothesized that associations between maternal and child health variables would vary according to the quality of postpartum social support, with highly supported dyads protected from the effects of maternal health on child temperament, while poorly supported dyads would be increasingly exposed to the effects of COVID-19-related perinatal maternal health on infant negative affect.
Method
Participants
Pregnant Italian women were recruited through a social media post during a defined Italian national lockdown from April 8 to May 4 of 2020. Inclusion criteria were (a) being pregnant at the time of assessment, (b) being a resident of Italy, (c) being over 18 years old, and (d) reading fluent Italian. Of the original sample of 2,502 responders (t0), 107 were excluded because they had already given birth for at least 2 weeks at the time of the first assessment; 835 did not complete the t0 assessment and/or did not leave contact information for the t1 assessment. A total of 1,560 responders agreed to be re-contacted for future phases of the study and 797 participated in the survey when contacted approximately 6 months after their expected date of delivery (t1). Of these, 139 responders did not provide complete answers to the survey, 11 were excluded because they had twins, and 4 were excluded because their pregnancies did not result in the birth of a baby (1 woman had a miscarriage and 3 voluntarily terminated the pregnancy). Therefore, a final sample size of 643 was available for all analyses in this paper (see Figure 2).

Figure 2. Study participants’ flowchart.
Procedure
The study has a longitudinal design based on two Qualtrics hosted online surveys completed by participants during pregnancy (t0) and 6 months postpartum (t1) as depicted in Figure 1 Supplement (see Supplement material). Participants were recruited voluntarily through social media and completed the study’s online survey after explicitly agreeing to participate. For the first survey (t0) participants reported on their mental health and perceived psychological stress due to the pandemic and were asked for their consent to be re-contacted in the following months. Data were collected from April 8 to May 4 of 2020. At t0 assessment, Italians were witnessing major stressful events and strained conditions surrounding a national lockdown – which started on March 9, 2020 and lasted until June 4 – and a public health emergency. During that time frame, pandemic containment measures included an imposed national quarantine, restrictions on movement, closure of all nonessential businesses and industries, and closure of schools and universities. In addition, at that time, the number of active cases in Italy was among the highest in the world (Italian Government, 2020). For postpartum (t1) assessment, participants were emailed approximately 6 months after their date of delivery to complete our online survey about their current mental health; psychological stress due to the pandemic; a checklist of COVID-19 stressful events that occurred both prenatally and/or post-birth; perceived social support; birth outcomes (i.e., child’s sex, birth weight, age at delivery); and infant temperament. Data were collected from December 12, 2020 to May 8, 2021. In the t1 assessment, Italy was affected by the second wave of the pandemic, which led the government to introduce additional restrictions on movement and social life that were only gradually eased mid-2021. The pandemic containment measures were less strict and more heterogeneous and they mostly strained social connections as they imposed the use of protective masks outdoors and social distancing and mobility windows with curfews, but the measures did not include home confinement policies. In addition, hospitals were expanded to hold more patients than in March of 2020, and COVID-19 vaccination campaigns were so active that health alarms were perceived as less threatening.
In each survey used in this study, participants completed the questionnaires after reading a consent form and explicitly agreeing to participate. The Institutional Review Board of the University of Padova approved the first phase of the study on April 6, 2020 and the second phase of the study on October 10, 2020.
Measures
COVID-19 stressful events exposure
The survey at t1 comprised a short checklist of questions regarding direct exposure to COVID-19 major stressful events during pregnancy and/or during the first 6 months post-birth. Four significant events were selected, and items were constructed with a yes/no dichotomous answer: “Did you contract SARS-CoV-2?”; “Did any of the people who live with you contract the SARS-CoV-2?”; “Did any of your relatives contract SARS-CoV-2?”; and “Did you experience the loss of a loved one due to SARS-CoV-2?” The two different composite scores (i.e., one for the pregnancy and one for the postpartum period) were computed as the sum of the items. After computing the sum, due to the highly skewed nature of the composite scores (88.6% of participants scored 0) on the checklist referring to pregnancy exposure, we dichotomized both variables between participants who scored 0 (not exposed) and participants who scored higher than 0 (exposed).
Pandemic psychological stress
At t0 and t1, the subjective perception of psychological stress secondary to the COVID-19 pandemic was investigated through two identical set of inquiries tapping on COVID-19 pandemic health emergency impacts. Specifically, COVID-19 pandemic stress was investigated by asking participants to report how much they felt worried (1 = “Not worried at all” to 7 = “Very worried”) about four different single-item domains regarding their (1) personal health, (2) their loved ones’ health, (3) the risk that they would contract the virus, and (4) that their loved ones would. Internal consistency for the four items was good at both assessment times (t0 Cronbach’s α = 0.81; t1 Cronbach’s α = 0.79) and confirmatory factor analysis at t0 showed a solid factorial structure (see Figure 2 Supplement in Supplement materials). These four items were included in the same structural equation model in order to provide a latent score as a global index of COVID-19 pandemic psychological stress.
Maternal mental health
Prenatal (t0) and postpartum (t1) maternal mental health were assessed in terms of symptoms of depression, anxiety, and posttraumatic stress disorder (PTSD) symptoms. These three dimensions were included in the same structural equation model in order to provide a latent score as a global index of maternal mental health. Depression was assessed with the Edinburgh Postnatal Depression Scale (Cox et al., Reference Cox, Chapman, Murray and Jones1996). It is a 10-item test using a 4-point scale regarding the previous 7 days, specifically designed to explore depression risk in the postpartum period and largely validated across pregnancy. Scores are summed to provide a single index of depression (t0 Cronbach’s α = 0.85; t1 Cronbach’s α = 0.87). Anxiety was measured with the State–Trait Anxiety Inventory, State version (Spielberger, Reference Spielberger1983), a 20-item self-report questionnaire using a 4-point scale. State anxiety (t0 Cronbach’s α = 0.95; t1 Cronbach’s α = 0.95) is computed as the sum of the items and refers to the respondent’s experience at the time the questionnaire was completed (i.e., how the subject feels “now”). For PTSD symptoms, the PTSD CheckList for DSM-5 (PCL-5; Weathers et al., Reference Weathers, Litz, Keane, Palmieri, Marx and Schnurr2013) was used. The PCL-5 is a 20-item self-report measure that assesses PTSD symptoms based on DSM-5 criteria. Scores are provided on a 5-point scale based on symptom severity over the past week and summed to obtain a global score (t0 Cronbach’s α = 0.93; t1 Cronbach’s α = 0.94).
Social support
Perceived social support was investigated at t1 with the Multidimensional Scale for Perceived Social Support (Zimet et al., Reference Zimet, Powell, Farley, Werkman and Berkoff1990). Twelve items measure the perceived adequacy of social support from three sources: family members, friends, and significant others. Items are rated on a 7-point Likert-type scale ranging from “Very strongly disagree” (1) to “Very strongly agree” (7) and summed to obtain a total score of perceived social support (Cronbach’s α = 0.92).
Infant temperament
The very short form of the Infant Behavior Questionnaire-Revised (IBQ-R; Garstein & Rothbart, Reference Garstein and Rothbart2003) was used to assess infant temperament at 6 months old (t1). Respondents are asked to circle the frequency of specific infant reactions/behaviors exhibited in the past week on a 7-point Likert scale (“Never,” “Very rarely,” “Less than half the time,” “Half the time,” “More than half the time,” “Almost always,” and “Always”). The very short form of the IBQ-R has three broad scales computed as items’ mean scores, including effortful control, surgency, and negative affect; each contained 12 items from the IBQ-R. For purposes of this study, we used the Negative Affect scale (Cronbach’s α = 0.78).
Data analysis
After providing demographic data and descriptive analyses of the variables in the study, we tested a hypothesized model (Figure 1) of the relationships between maternal health variables across t0 and t1 and infant negative affect at t1 based on a structural equation model approach. At t0 and t1, the four items regarding participants’ worries about the COVID-19 pandemic were hypothesized to be explained by one single latent variable called Pandemic Psychological Stress, while Edinburgh Postnatal Depression Scale, State–Trait Anxiety Inventory, and PCL-5 were hypothesized to be explained by one single Maternal Mental Health latent variable. Then, we tested for the direct effects of (a) prenatal COVID-19 stressful events exposure, (b) prenatal pandemic psychological stress, (c) maternal mental health in pregnancy, (d) postpartum stressful events exposure, (e) postpartum pandemic psychological stress, and (f) maternal mental health in the postpartum period on the infant’s negative affect at 6 months of age. To test the indirect associations of prenatal and postnatal maternal health variables on each infant’s temperament, the dimensions of COVID-19 stressful events exposure, pandemic psychological stress, maternal mental health in pregnancy (t0), and COVID-19 stressful events exposure postpartum (t1) were included as independent variables (IVs); maternal mental health at t1 was inserted as a mediator and infants’ negative affect at 6 months of age was inserted as a dependent variable. Social support at 6 months postpartum (t1) was included in the model as a moderator of the associations between COVID-19 stressful events exposure, pandemic psychological stress, and maternal mental health with infant negative affect. All associations in the model were controlled for the confounding effects of gestational age at t0 (Rouse & Goodman, Reference Rouse and Goodman2014), maternal age and family socioeconomic status (e.g., family income; Hendry et al., Reference Hendry, Gibson, Davies, Gliga, McGillion and Gonzalez-Gomez2022). Regression on the infant negative affect variable also controlled for the child’s sex (Christians & Chow, Reference Christians and Chow2022).
To evaluate the goodness of fit of the model in respect to the real data, we used the following indices: the chi-square statistic, which should be nonsignificant; the comparative fit index and the Tucker-Lewis index, which should approach 0.95 to indicate optimal fit (Brown, Reference Brown2015); and the root mean squared error of approximation (RMSEA) and the standardized root mean square residual, which should approach 0.05 and 0.04, respectively, to indicate a good fit (Kline, Reference Kline2012). Nonsignificant probability values were associated with the fit of RMSEA. The mediating effects of maternal mental health at t1 were tested within the structural equation model by means of bootstrapped 95% confidence intervals (CI). Last, for the moderating effects of social support, we explored the interpretation of the significant interaction effects by performing different simple slope analyses in order to compute the target effects in case of high (M + 1 SD) and low (M – 1 SD) values of social support.
Finally, as exploratory follow-up analyses, we tested the hypothesized COVID-19-related perinatal mother-infant health model, separately examining the specific contribution of each of the maternal mental health variables (i.e., depression, anxiety, and PTSD symptoms).
In this study all analyses were performed with R software. The structural equation model was computed by means of the lavaan package (Rosseel, Reference Rosseel2012).
Results
Table 1 shows the demographic characteristics of the final sample. Characteristics of the t0 participants who did not complete the study in comparison with the final sample of this study (t1) are presented in supplemental form (see Tables S1 and S2 in Supplement materials).
Table 1. Demographic characteristics of the sample

The structural equation analysis resulted in the model presented in Figure 3. The overall fit measures indicated that the fit of the model was adequate (X2[200] = 532.091, p < .001, comparative fit index = 0.94, Tucker-Lewis index = 0.93, RMSEA = 0.05, p = .38, 90% CI [0.05, 0.06], standardized root mean square residual = 0.05). A complete description of the resulting model and the correlation matrix of the model’s variables are presented in supplemental form (see Tables S3 and S4 in Supplement materials).
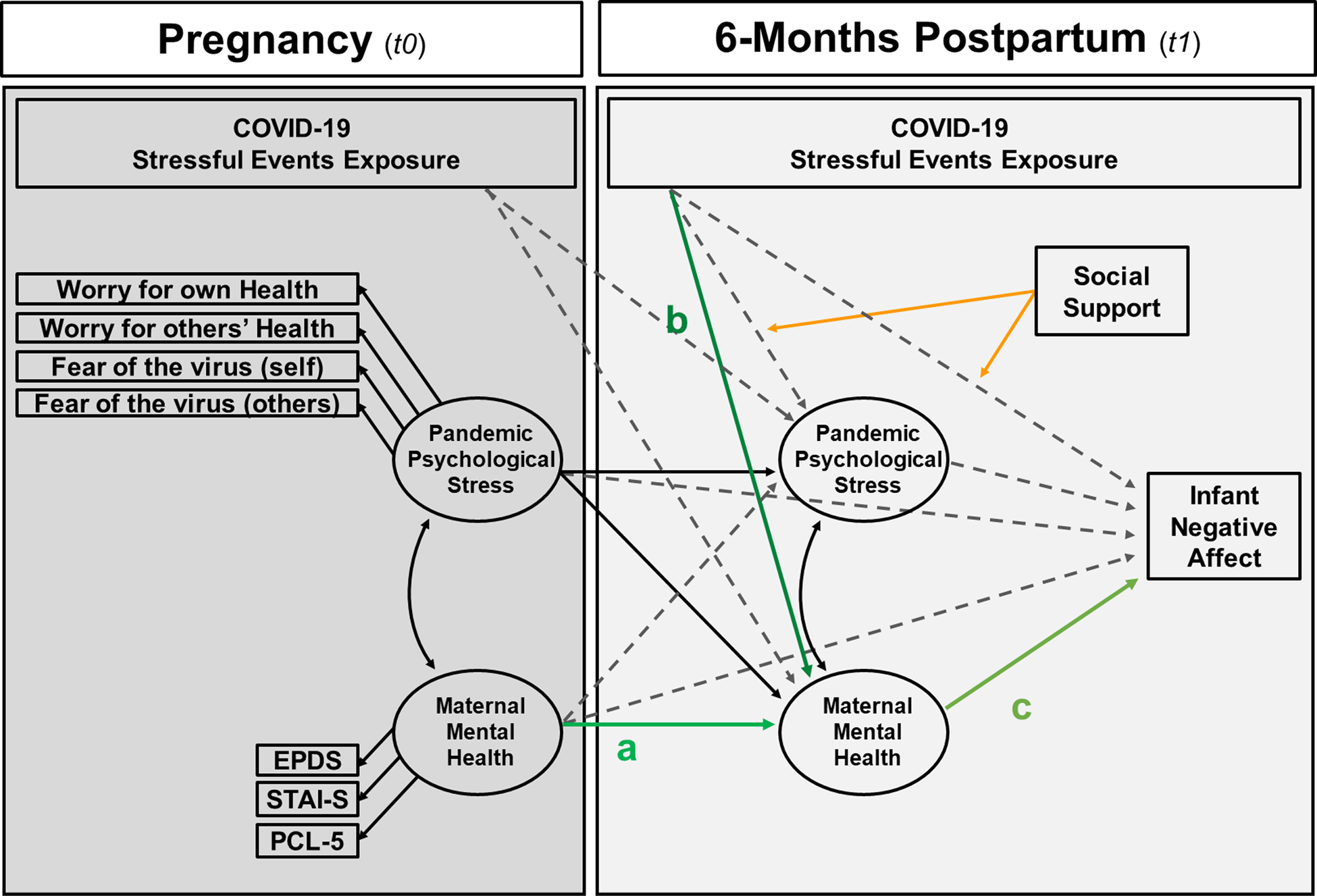
Figure 3. Results of the structural equation model. The colored (green) lines indicate the paths implicated in the mediation effects tested in the study. Specifically, a * c and b * c represent the mediation effects of maternal mental health at t1 in the associations between maternal mental health at t0 and infant negative affect as well as between COVID-19 stressful events exposure at t1 and infant negative affect. Continuous lines represent significant direct paths, dotted lines represent nonsignificant paths. The colored (orange) lines indicate the significant paths implicated in the moderation effects of social support. For sake of readability, only the observed variables that constitutes the latent variables at t0 (i.e., pandemic psychological stress and mental health) have been represented. The same variables measured at t1 are regressed on the latent variables pandemic psychological stress and mental health at t1. For the same reason of readability, the significant direct effect of social support on each mental health variable and the following nonsignificant paths have not been represented: the association between COVID-19 stressful events exposure at t0 and infant negative affect and the moderating effect of social support; the moderating effect of social support on the association between COVID-19 stressful events exposure (at t0 and t1) on mental health at t1. Each regression is controlled for the confounding effects of: gestational age at t0, maternal age and family SES (e.g., family income); regression on the infant negative affect also controlled for child’s sex.
Regarding the direct and indirect effects of t0 and t1 maternal variables on infant negative affect, only maternal mental health symptoms at t1 were directly associated with infant negative affect variance; also, it significantly and fully mediated the association between infant’s negative affect with maternal mental health at t0 (b = 1.83, SE = 0.58, z = 3.15, p = .002, bootstrapped 95% CI [0.70, 2.92]) and COVID-19 stressful events exposure at t1 (b = 0.33, SE = 0.215, z = 2.25, p = .03, bootstrapped 95% CI [0.10, 0.71]). Neither pandemic psychological stress at t0 (b = 0.26, SE = 0.15, z = 1.69, p = .09, bootstrapped 95% CI [0.00, 0.68]) nor COVID-19 stressful events exposure at t0 (b = −0.34, SE = 0.28, z = -1.20, p = .23, bootstrapped 95% CI [−1.07, 0.12]) were directly or indirectly (via maternal mental health at t1) associated with infant’s negative affect at 6 months of age. Only pandemic psychological stress at t0 was positively associated with maternal mental health at t1.
Regarding the moderation of postpartum social support on the mother-infant health associations, maternal social support at t1 significantly moderated the association between COVID-19 stressful events exposure at t1 and infant negative affect; indeed, the association between COVID-19 stressful events exposure at t1 on infant negative affect was positive and significant when mothers reported high levels of social support (b = 1.90, SE = 0.80, t[630] = 2.38, p = .02), while negative and nonsignificant associations were found when the mothers reported low levels of social support (b = −0.24, SE = 0.77, t[630] = −0.31, p = 0.76). Figure 4 depicts the simple slope analysis to interpret this interaction effect.
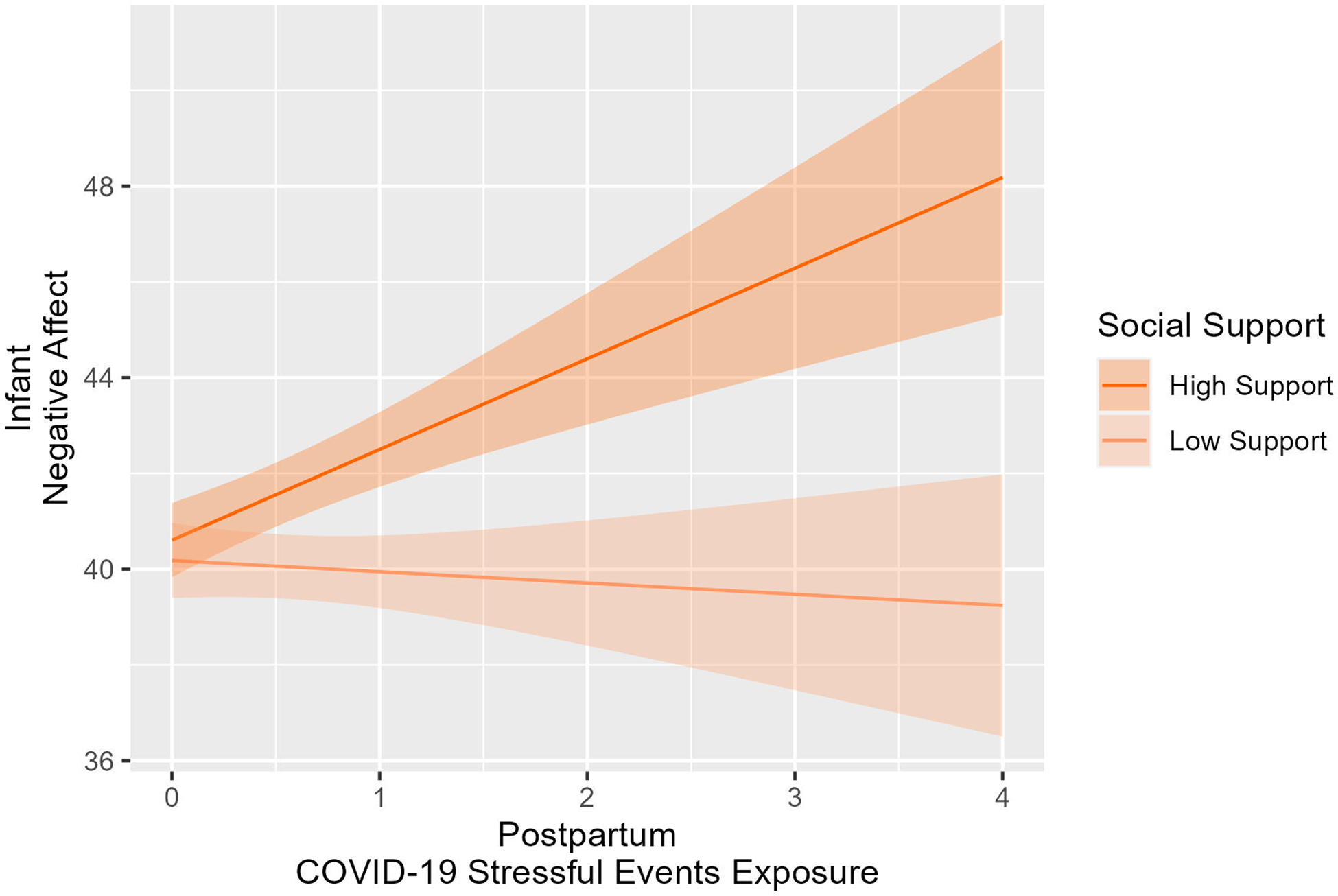
Figure 4. The association between COVID-19 stressful events exposure in postpartum and infants’ negative affect at 6 months moderated by social support.
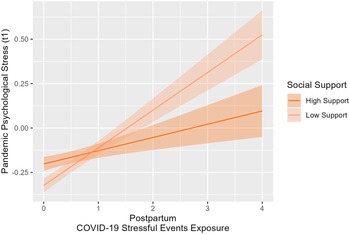
Also, social support significantly moderated the association between COVID-19 stressful events exposure at t1 and pandemic psychological stress at t1: High COVID-19 stressful events exposure was associated with high psychological stress when mothers reported low levels of social support (b = 0.21, SE = 0.04, t[630] = 4.70, p < .001), while when the mothers reported high levels of social support the association was not significant (b = 0.07, SE = 0.04, t[630] = −1.85, p = .07). Figure 5 shows the simple slope analysis used to interpret this interaction effect.

Figure 5. The association between COVID-19 stressful events exposure in postpartum and the pandemic psychological stress at 6 months moderated by social support.
In addition to the direct, mediated, and moderated paths of the model, pandemic psychological stress at t1 was negatively predicted by family socioeconomic status versus positively by the gestational age at the t0 assessment.
Finally, the separate exploratory follow-up analyses performed to test the COVID-19-related perinatal mother-infant health model using each single mental health index (i.e., anxiety, depression, PTSD symptoms) produced overall consistent results regarding direct, mediated, and moderated paths with slight differences depending on which index was considered. Specifically, both the depression-only and the anxiety only models produced very similar findings to the original model (with the mental health latent variable) with the addition of a significant direct association between both prenatal depression and prenatal anxiety on infants' negative affect. The posttraumatic stress-only model again produced very similar results with the addition of a significant association between posttraumatic stress at t0 and pandemic psychological stress at t1. It also showed a lack of association between COVID-19 stressful events exposure at t1 and the PTSD score at t1. Detailed figures and fit indexes for the three models are presented in Figure 3 Supplement in Supplement materials.
Discussion
The prenatal and postnatal growth epochs are critical periods for infant and child development to the extent that adverse, traumatic, and stressful experiences during these periods produce programming effects on brain, development, and psychopathological risk (Monk et al., Reference Monk, Spicer and Champagne2012, Reference Monk, Lugo-Candelas and Trumpff2019). In this study, we longitudinally modeled relationships between several stressors describing maternal experiences of pandemic COVID-19 in Italy during pregnancy and a postpartum period and temperamental negative affect in offspring at 6 months of age. Specifically, we observed how the association between maternal health and infant temperament in a perinatal period characterized by extraordinary environmental conditions takes into account the degree of maternal exposure to COVID-19 life events and/or pandemic-related psychological stress.
The results of the presented model support the hypothesis of a perinatal maternal-infant health risk related to COVID-19; in fact, we show that in a cohort of pregnant women largely not directly affected by a COVID-19 infection, postpartum maternal mental health is a significant perinatal pathway for the transmission of pandemic-related maternal health to the child’s temperament and thus potentially also to the risk of developmental psychopathology. Negative affect in the infant is a sentinel for subsequent psychopathology pathways and a node in the intergenerational transmission of mental health problems; its early assessment, monitoring, and protection is a key goal for infant mental health and psychopathology (Gartstein & Skinner, Reference Gartstein and Skinner2018; Sacchi et al., Reference Sacchi, De Carli, Vieno, Piallini, Zoia and Simonelli2018). In mother-infant dyads where mothers were exposed to the peak of the pandemic in pregnancy, maternal mental health at 6 months postpartum conveys the effect of maternal mental health in pregnancy and postpartum stressful events on the child’s negative affect. Moreover, although it does not mediate the effect on child outcome, postpartum maternal mental health was also longitudinally associated with the psychological stress of the prenatal pandemic period, potentially highlighting the lasting costs to maternal health of pandemic-imposed changes in the perinatal period. Taken together, these processes could reflect a cascade of underlying mechanisms involving epigenetic, inflammatory, and/or endocrine pathways in which stress-based alterations in maternal biology and social functioning – partially induced by the pandemic – could transit to the fetus and newborn by altering the prenatal environment (Glover, Reference Glover2011; Van den Bergh et al., Reference Van den Bergh, van den Heuvel, Lahti, Braeken, de Rooij, Entringer, Hoyer, Roseboom, Räikkönen, King and Schwab2017) and putting parenting behaviors at risk in a very sensitive time window (Huizink et al., Reference Huizink, Menting, De Moor, Verhage, Kunseler, Schuengel and Oosterman2017; Stein et al., Reference Stein, Pearson, Goodman, Rapa, Rahman, McCallum, Howard and Pariante2014).
We also observed the decisive role of perceived social support for pandemic mother-infant dyads. Social support is an established protective factor as it can function as a buffer to the negative impact of environmental risk factors on mothers and children (Bedaso et al., Reference Bedaso, Adams, Peng and Sibbritt2021; Sacchi et al., Reference Sacchi, Miscioscia, Visentin and Simonelli2021; Takács et al., Reference Takács, Štipl, Gartstein, Putnam and Monk2021). Our results demonstrate that social support can moderate the effects of exposure to COVID-19 stressful events on both pandemic psychological stress and child temperament, albeit with different and at first glance counterintuitive results. On the one hand, consistent with the hypotheses and in line with the evidence of the moderating effect of social support on COVID-19-related stress in pregnant women (Khoury et al., Reference Khoury, Atkinson, Bennett, Jack and Gonzalez2021; Meaney et al., Reference Meaney, Leitao, Olander, Pope and Matvienko-Sikar2021), lack of postpartum social support appears to intensify the negative effect of exposure to COVID-19 events on maternal psychological stress. On the other hand, when examining infants' negative affect, infants of mothers reporting high social support scores seem to be more susceptible to the negative effect of COVID-19 stressful events on their negative affect. This unexpected result on the seemingly aggravating effect of social support might suggest that infants of mothers with a more supportive social network might be particularly exposed to the COVID-19 burden that prevented help from important figures such as grandparents (Riem et al., Reference Riem, Lodder, Guo, Vrielink-Verpaalen, van IJzendoorn, Bakermans-Kranenburg and De Carli2021) during the first few months after birth. In other words, high perceived social support – by means of readjusting the ways of maintaining continuity in supportive relationships – might have reduced the perceived psychological stress due to the pandemic. Conversely, precisely those families with high perceived social support might have suffered more from an unexpected lack of concrete and in-person availability during the pandemic due to imposed isolation and related restrictions with possible consequences on the care burden and thus on the child’s temperament. This might have particularly impacted those families where new mothers reported stressful events consequent to the COVID-19 pandemic. Qualitative investigations on the impact of the COVID-19 pandemic have consistently highlighted the lack of peer and intergenerational support as a primary source of difficulty in the perinatal period (Atmuri et al., Reference Atmuri, Sarkar, Obudu and Kumar2022; Chivers et al., Reference Chivers, Garad, Boyle, Skouteris, Teede and Harrison2020; Kumari et al., Reference Kumari, Ranjan, Sharma, Sahu, Bharti, Zangmo and Bhatla2021). Certainly, more in-depth research is needed to explore the specificity of the COVID-19 pandemic on child adaptation with the result that we might need to rethink current models of child social development.
Overall, maternal mental health (MMM) after birth is a key variable for mother-infant perinatal health in the COVID-19 era. MMM was significantly depleted by the impacts of the pandemic, such as decreased availability of social support and exposure to major stressful events. MMM appeared to absorb several features of prenatal stress, such as mental health symptoms and psychological stress due to the pandemic, and MMM appeared to channel some of these exposures into plausible risks for offspring developmental psychopathology as indicated by the effects of MMM on infants’ negative affect. The study again suggests that maternal psychological health assessment in pregnancy and postpartum periods could help in protecting the perinatal health of both mother and infant. Mental health monitoring and support, along with the promotion of social support during this period can function as an effective shield from various sources of risk (e.g., stressful life events, psychological distress, anxiety, depression, and isolation or poor connectedness) that could impact the mother-infant dyad. In addition, the study highlights the role of various stressors, such as COVID-19 exposure and psychological stress, MMM, and lack of social support, in offspring developmental trajectories during the pandemic from the womb to 6 months old.
Finally, the study provides an ecological framework for observing the interconnectedness of stressors placed at multiple levels of maternal experience during the perinatal period. It both provides a live measurement of several indices of health while the stressor is active and investigates maternal and neonatal health in an unpredictable and changing socioeconomic health scenario characterized by alarms, isolation, lack of family support, and limited socialization opportunities for newborns.
The longitudinal research design used in this study was a timely investigation at the peak of a pandemic, and it ensures robust data. However, for a correct interpretation of the results, some limitations must be acknowledged. First, although the ample size and wide regional and socioeconomic distribution of the sample largely supports generalizability of the results, the self-selection of participants should not be overlooked. Also, a voluntary web-based recruitment caused by extraordinary home confinement conditions during April of 2020 resulted in the exclusion of participants unwilling and/or unable to access the internet. In addition, the unusual conditions of the pandemic, which only allowed online surveying at the time of the first assessment, limited the choice of more extensive and detailed assessments. Indeed, the model would have benefited from a comprehensive, longitudinal assessment of social supports in pregnancy. In addition, the absence of standardized measures available for assessing the impact of the COVID-19 pandemic, both in terms of exposure and distress, forced an ad hoc assessment study design that limits comparison possibilities with other studies. Finally, although a gold-standard measure of child temperament was adopted and the maternal mood-state proved to be an unbiased assessment of child functioning (cf. Olino et al., Reference Olino, Michelini, Mennies, Kotov and Klein2021), findings on the infant’s negative affect should be interpreted with the understanding that parental accounts of child development carry a potential for risk of overestimation, as the mother and child constitute a single psychobiological system that shares both genetic and environmental susceptibilities. Mother and child influence one another in subtle ways.
Conclusion
Infants born during the 2020 COVID-19 pandemic showed temperamental negative affect associated with maternal perinatal health factors as described by maternal psychological pandemic stress levels, exposure to COVID-19 stressful events, and mental health. The study found significant associations between COVID-19 with perinatal risks for maternal and infant health outcomes in dyads exposed to COVID-19 stressors during pregnancy, especially in settings of high pandemic psychological stress and poor social support or direct exposure to COVID-19 stressful events in a 6-month postpartum period.
The COVID-19 pandemic has highlighted how perinatal health policies and clinical services might need to apply relational health frameworks that consider the mother-infant dyad as a developing unit (cf. Firestein et al., Reference Firestein, Dumitriu, Marsh and Monk2022). There is a consequent need to extend pregnancy related medical care throughout the first postpartum year in order to both effectively protect maternal mental health and contain and reduce the transmission of pandemic-related stress to newborns.
Finally, as the COVID-19 pandemic continues and continues to contribute to unstable social, economic, and health conditions it is critical that scientific research anticipates that beyond the inequalities already produced or exacerbated by the current crisis, additional risks are coming and affecting the next generation in complex and layered ways. The effects may stem from early difficulties in maternal and child health quality along the perinatal period (Provenzi & Grumi, Reference Provenzi and Grumi2021; Wade et al., Reference Wade, Prime and Browne2020).
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954579423000093
Acknowledgments
We acknowledge the valuable contributions of all the pregnant women who lent themselves to this research, sharing their emotional well-being during the difficult time of the pandemic. We would like to thank Annachiara Gianbattista, Francesca Sartor, and Arianna Vola for their support in data collection and Luisa Bertoldo, Michela Meni, and Gaia Rota for helping us reach out to pregnant women during the pandemic.
Funding statement
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflicts of interest
None.







 Open access
Open access