



Key points
-
▪ Cariprazine is a second-generation antidepressant recently approved for major depressive disorder (MDD) augmentation.
-
▪ Preclinical findings support the efficacy of cariprazine in reducing anhedonia and anxiety.
-
▪ Two studies found significant reductions in depressive symptoms following cariprazine augmentation.
Introduction
Major depressive disorder (MDD) is characterized by significant cognitive, psychosocial, and physical impairments. 1 , Reference Halaris 2 Due to the increasing prevalence of MDD, it is expected that depression will be the leading cause of global disease burden by 2030.Reference Mathers and Loncar 3 Despite the significant economic and social burden of MDD, the etiology and pathophysiology of MDD remain unclear.
The current therapeutic framework for MDD symptomatology is not predictive of response to antidepressants and other therapeutic approaches. Current depression treatment guidelines recommend antidepressants as a first-line treatment option.Reference Kennedy, Lam and McIntyre 4 However, fewer than half of MDD patients achieve full symptom remission following first-line treatment options, with cognitive difficulties, sleep problems, and low energy being the most common residual symptoms.Reference Baune, Miller and McAfoose 5 , Reference Rush 6 After failing to achieve remission with a first-line antidepressant, treatment guidelines suggest either switching to another antidepressant or adding on a second medication (ie, augmentation). Augmentation has been associated with improved outcomes compared to switching strategies after an incomplete response to an antidepressant agent.Reference Mohamed, Johnson and Chen 7 , Reference Santaguida, MacQueen, Keshavarz, Levine, Beyene and Raina 8 Second-generation atypical antipsychotics (SGAs) have been widely studied as augmenting agents added to monoamine-based antidepressants. SGAs have collectively shown to have a 1.7-fold increased likelihood of antidepressant response in addition to twofold increased chances of remission when added as an augmentation agent.Reference Caldiroli, Capuzzi and Tagliabue 9 , Reference Kato and Chang 10
Food and Drug Administration (FDA)-approved add-on treatments for MDD include aripiprazole, brexpiprazole, quetiapine XR, esketamine nasal spray, and, most recently, cariprazine. Cariprazine was approved by the FDA as an adjunctive therapy (ADT) to antidepressants for treating adult patients with MDD on December 16, 2022. Cariprazine is an SGA and has also been FDA-approved for schizophrenia and bipolar I disorder during manic and depressive episodes.
Most SGAs assert their effects through action across dopamine receptors. Cariprazine is a partial D2 and D3 receptor agonist. One of the unique features of cariprazine is the increased affinity it has for the D3 receptor. Notably, the dopamine D3 receptor has been suggested as a target for the treatment of unipolar depression.Reference Leggio, Salomone and Bucolo 11 Indeed, the expression of D3 receptors in brain regions implicated in reward pathways may subserve motivation and reward-related deficits in depression.Reference Carnicella, Drui and Boulet 12 , Reference Mansur, Subramaniapillai and Zuckerman 13 Moreover, preclinical studies using selective D3 receptor antagonists have demonstrated a significant increase in the concentration of dopamine, norepinephrine, and acetylcholine in the anterior cingulate cortex (ACC) independent of serotonergic effects.Reference Lacroix, Hows, Shah, Hagan and Heidbreder 14 , Reference Ragguett and McIntyre 15 The dysregulation of the ACC has been shown to influence mood-related changes in psychiatric disorders.Reference Strakowski, Adler and Almeida 16 The combined effects of cariprazine on the dopaminergic and reward pathways have demonstrated pro-cognitive and anti-anhedonic effects in preclinical trials.Reference Ragguett and McIntyre 15
Previous network meta-analyses and systematic reviews have found varying acceptability of cariprazine compared to other approved adjunctive atypical antipsychotics.Reference Kishimoto, Hagi, Kurokawa, Kane and Correll 17 -Reference Yan, Yang, Wang, Chen, Yin and Ma 19 While cariprazine has been FDA-approved for MDD, suggestive of a positive efficacy and safety profile, we provide an up-to-date analysis evaluating the antidepressant efficacy of cariprazine augmentation compared to other adjunctive treatments for MDD. Herein, we systematically evaluate and meta-analyze the potential antidepressant effects of cariprazine as an ADT in populations with MDD. We evaluate both continuous (ie, change in depressive symptom severity scores over time) and categorical (ie, remission and response rates) outcomes to provide a clear and clinically useful synthesis of efficacy data.
Methods
Literature search and study selection
Three independent reviewers (HG, DC, and SH) searched the literature for studies that evaluated the efficacy of cariprazine treatment in patients with MDD. All three reviewers conducted a search on PubMed, Google Scholar, and PsycINFO for English-language articles published between database inception and September 24, 2023, using the following Medical Subject Headings (MeSH) terms and search strings: ((cariprazine) AND (depression OR major depressive OR treatment-resistant depression OR depress*)). An additional search was performed in the reference list of identified articles by all three authors. Our systematic review reported results using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The PRISMA checklist was used to improve the reliability of included studies and comprehensively report the study methods and results.Reference Moher, Liberati, Tetzlaff and Altman 20 Following the formal search, ClinicalTrials.gov was looked at to find further published studies.
Eligibility criteria
Inclusion Criteria
Our inclusion criteria are as follows:
-
1. Confirmed diagnosis of MDD based on a standard clinical assessment or structured interview (eg, The Diagnostic and Statistical Manual of Mental Disorders (DSM)).
-
2. The intervention should be cariprazine evaluated as an adjunctive antidepressant treatment.
-
3. RCTs should include an appropriate placebo as a control.
Exclusion Criteria
Our exclusion criteria are as follows:
-
1. Unpublished data sets, case studies, conference reports, non-refereed abstracts, or observational studies.
-
2. Multiple reports from the same data set.
-
3. Absence of clinical assessment of depression and/or sample not meeting the criteria for MDD.
-
4. Treatment interventions without cariprazine.
-
5. Animal studies.
Assessment of bias
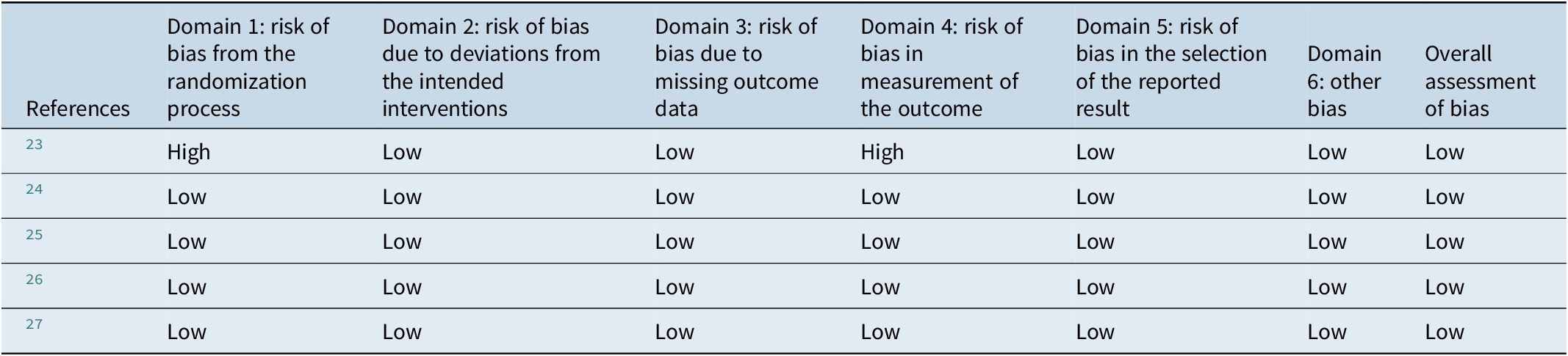
Study quality (ie, risk of bias) was assessed using the revised Cochrane risk-of-bias tool for randomized trials (RoB 2: A revised Cochrane risk-of-bias tool for randomized trials, 21). Bias was assessed in accordance with the six domains evaluating the risk of bias: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in measurement of the outcome, bias in the selection of the reported result, and bias arising from conflicts of interest.Reference Sterne, Savović and Page 22 Complete results from the Cochrane risk-of-bias guidelines are presented in Table 1.
Table 1. Cochrane Risk-of-Bias Assessment Results
Statistical analysis
A random-effects model was used to calculate the standardized mean difference (SMD) and account for the expected variability between included studies. The cutoff for significance was set at P < 0.05. The main outcome measure for the antidepressant effect across all included studies was the Montgomery–Åsberg Depression Rating Scale (MADRS) score. Therefore, the mean change in MADRS total score and standard deviation (SD) were extracted. For papers that did not report raw mean or mean difference and SD values but provided a figure of the primary outcomes, an image of the figure was taken and uploaded into PlotDigitizer, an online data extraction tool, which was subsequently used to determine the mean/mean difference and SD from the values of the plot. As the main outcome measure was the same across all included studies, results from multiple treatment groups were pooled prior to inclusion in the random-effects model. As the outcomes were continuous (ie, MADRS total scores), heterogeneity was determined using I2 values, where 25% = small, 50% = moderate, and > 75% = high heterogeneity. The least-squares mean difference (LSMD) in MADRS total scores between the cariprazine ADT and placebo groups and the overall effect size were calculated to determine the main effects of adjunct cariprazine treatment on depressive symptomatology. Risk ratios (RRs) were calculated for all eligible randomized controlled studies to determine the relative response and remission rates of cariprazine compared to placebo augmentation. The RR for all-cause dropout was also determined as a proxy for overall tolerability. Only RCTs were included in our quantitative analysis. Open-label studies were qualitatively evaluated only to reduce heterogeneity and improve the reliability of the data.
Results
Search results
Following the removal of duplicates, our database search returned 236 unique articles. An additional five articles were found through a manual search of the references. Subsequently, 241 titles and abstracts were independently reviewed for eligibility. The full text of 18 articles was screened for eligibility.
Following a full-text review, 13 articles were excluded for not meeting the outlined inclusion criteria and primary study outcomes. The reasons for exclusion are as follows: 11 articles were excluded for not having MDD as the primary diagnosis in the participant group, one article was excluded for the wrong treatment (ie, cariprazine was not an ADT), and one article was excluded for the incorrect study design (ie, a case study). A complete summary of search results is presented in accordance with the PRISMA guidelines (Figure 1).
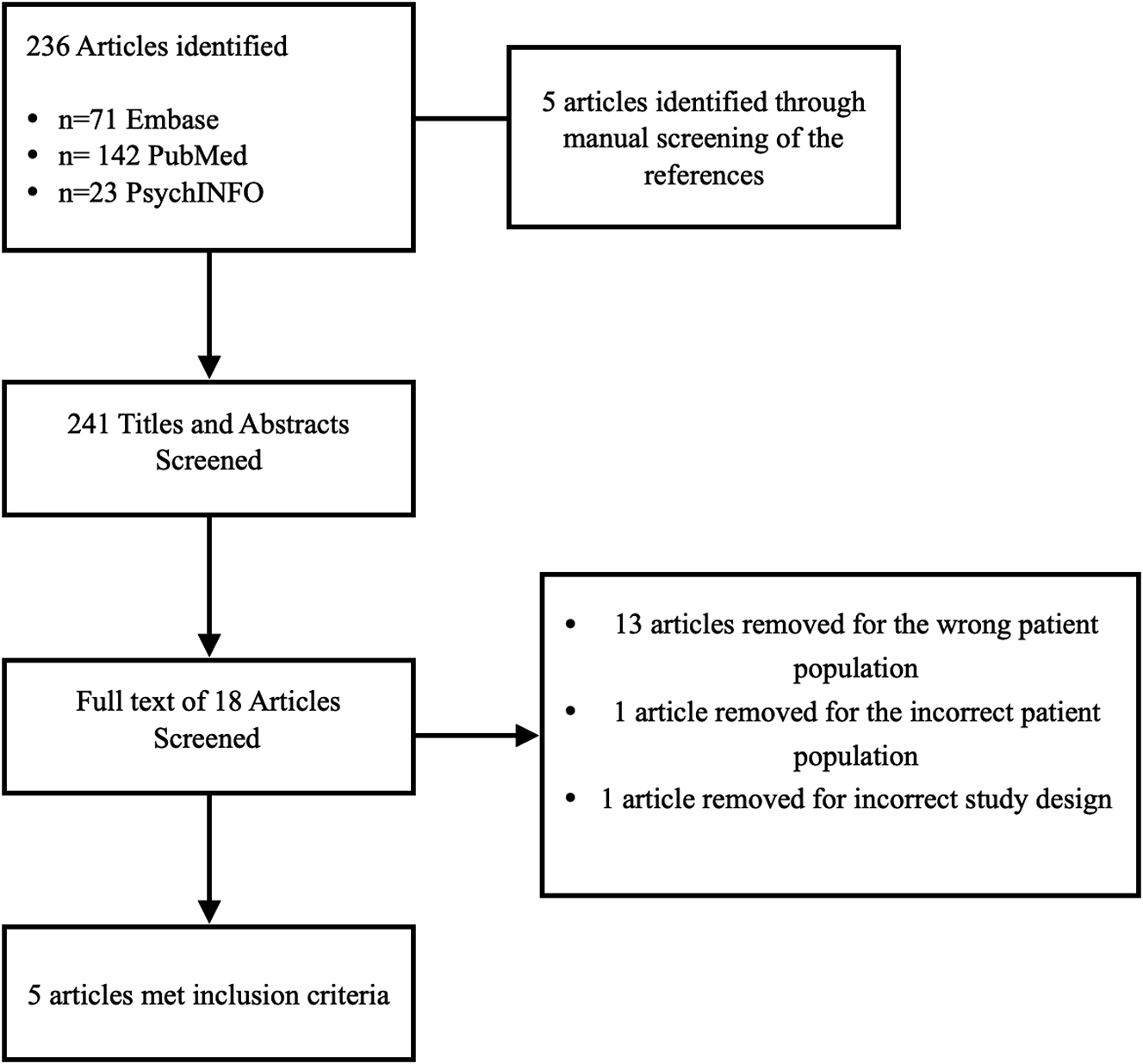
Figure 1. Preferred reporting items for systematic reviews and meta-analysis (PRISMA) study selection flow diagram.
Study characteristics
In all included studies, participants received cariprazine treatment through a titrated dose increase. Four studies were randomized, double-blind, placebo-controlled trials.Reference Durgam, Earley and Guo 24 -Reference Sachs, Yeung, Rekeda, Khan, Adams and Fava 27 One study was an open-label trial design with no placebo comparator group or an active comparator groupReference Vieta, Earley and Burgess 23 (Table 2).
Table 2. Characteristics of Included Studies
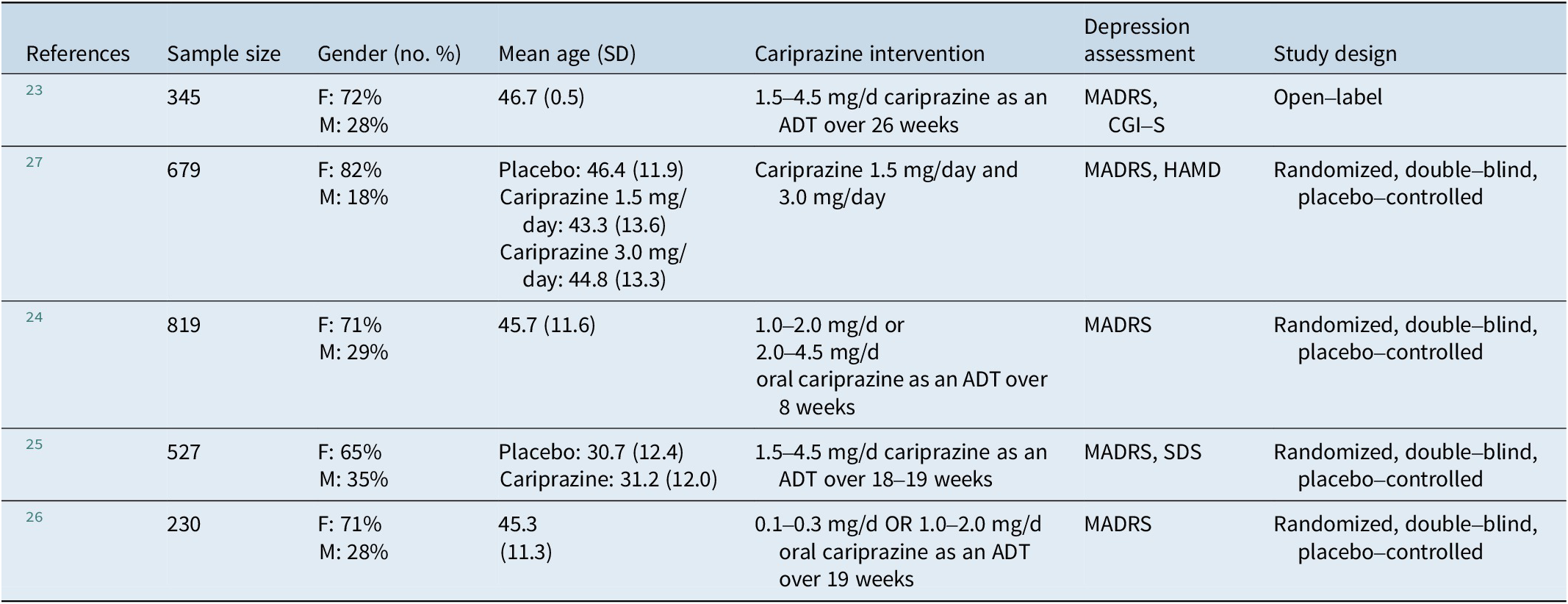
Abbreviations: ADT, adjunctive therapy; CGI-S, Clinical Global Impressions-Severity; F, female; HAMD, Hamilton Depression Rating Scale; M, male; MADRS, Montgomery–Åsberg Depression Rating Scale; SD, standard deviation; SDS, Sheehan Disability Scale.
Earley et al.Reference Earley, Guo, Németh, Harsányi and Thase 25 included an 8-week open-label ADT phase and an 8-week randomized double-blind phase. During the open-label phase, participants (n = 807) were prescribed a commercially available ADT (eg, vilazodone). The ADT was chosen by the study investigators insofar as it was not a treatment and the participants were previously non-responders.Reference Earley, Guo, Németh, Harsányi and Thase 25 Participants (n = 530) that did not show response during the open-label ADT phase were randomized with a 1:1 allocation of placebo or cariprazine. Participants randomized to cariprazine (n = 213) were titrated to a dose of 3.0 mg/day. The dose was increased to 0.5 mg/day. Participants that did not show any response (as shown by <40% MADRS total score change) were increased to 4.5 mg/day.Reference Earley, Guo, Németh, Harsányi and Thase 25 Participants allocated to the cariprazine group that completed the double-blind phase (n = 108), participants that completed the single-blind open-label placebo+ADT (n = 94), or participants that received double-blind placebo+ADT (n = 109) were enrolled in the open-label follow-up study.Reference Vieta, Earley and Burgess 23 Participants were given 0.5 mg/day of cariprazine on day 1. The dosage was increased by 0.5 mg/day until it reached 3.0 mg/day on either day 6 or day 7.Reference Vieta, Earley and Burgess 23
Moreover, Fava et al.Reference Fava, Durgam and Earley 26 conducted a 19-week randomized, double-blind, placebo-controlled study of cariprazine ADT in participants with MDD who failed one or two previous ADTs. They randomized the participants into three groups: a placebo group (n = 72), an ADT group administered 0.1–0.3 mg/day cariprazine (n = 70), and an ADT group administered 1.0–2.0 mg/day cariprazine (n = 63). The highest dose of cariprazine for the respective groups (0.3 mg or 2.0 mg) was titrated after 4 weeks. Similarly, Durgam et al.Reference Durgam, Gommoll, Migliore, Chen, Chang, Aguirre and Thase 28 randomized participants in an 8-week double-blind design with three groups: a placebo group (n = 234), an ADT group administered 1–2 mg/day cariprazine (n = 226), and an ADT group administered 2.0–4.5 mg/day cariprazine (n = 210). Prior to titration, all participants in the treatment groups began at 0.5 mg/day. Sachs et al.Reference Sachs, Yeung, Rekeda, Khan, Adams and Fava 27 randomized adults with MDD to receive either placebo, 1.5 mg/day cariprazine, or 3.0 mg/day cariprazine.
Adjunctive cariprazine treatment
All studies evaluated the treatment effects of cariprazine ADT in participants with MDD. Two studies employed a double-blind, placebo-controlled, parallel-group study design that had one placebo group and two cariprazine ADT groups (ie, high- and low-dose groups).Reference Durgam, Earley and Guo 24 , Reference Fava, Durgam and Earley 26 Durgam et al.Reference Durgam, Earley and Guo 24 found that participants receiving 2.0–4.5 mg/day cariprazine versus placebo had statistically significant mean reductions in MADRS total score at week 2. There was a LSMD of −2.2 in MADRS total score at week 8 between the 2.0–4.5 mg/day cariprazine dose group and the placebo group (P = .0057). For the 1–2 mg/day cariprazine group, the LSMD compared to the placebo group was −0.9. This was not significant (P = .2404).Reference Durgam, Earley and Guo 24 Participants in both cariprazine groups met MADRS response criteria at week 8 [(1–2 mg/day cariprazine group: odds ratio (OR): 1.49, 95 percent confidence interval (95% CI): 1.06 to 2.11) and (2–4.5 mg/day: OR: 1.59, 95% CI: 1.13 to 2.25)]. This was statistically significant for both the 1–2 mg/day (P = .0223) and 2.0–4.5 mg/day (P = .0080) cariprazine groups. Both groups did not demonstrate statistically significant changes in MADRS remission at week 2 (P = .5908 and P = .4594, respectively).
In contrast, Fava et al.Reference Fava, Durgam and Earley 26 did not observe statistically significant LSMD in MADRS in either cariprazine ADT group. The 1.0–2.0 mg/day cariprazine group showed a reduction in MADRS total score LSMD compared to the placebo group. However, this was not significant (P = .227). There were no observed changes in the 0.1–0.3 mg/day treatment group compared to the placebo group.Reference Fava, Durgam and Earley 26 The MADRS response and remission rates were greater in both cariprazine groups compared to the placebo group. However, the response and remission rates were not statistically significant in either the 0.1–0.3 mg/day cariprazine group (P = .533 and P = .705, respectively) or the 1.0–2.0 mg/day cariprazine group (P = .100 and P = .273, respectively).
In the third study, an 8-week double-blind placebo-controlled trial, placebo ADT non-responders were assigned 1:1 allocation to the placebo and cariprazine ADT groups. Beginning at 0.5 mg/day, the cariprazine ADT group had the dose titrated to 3.0 mg/day (and a maximum of 4.5 mg/day for non-responders at week 2).Reference Earley, Guo, Németh, Harsányi and Thase 25 The LSMD in MADRS total score was −0.2 between the 1.5–4.5 mg/day cariprazine group and the placebo group. The difference was not statistically significant (P = .2784). There were no differences in the MADRS response rates between the cariprazine and placebo groups. The MADRS remission rates were improved between the cariprazine and placebo groups (24.4% vs 19.1%). However, this was not statistically significant (P = 0.2321).Reference Earley, Guo, Németh, Harsányi and Thase 25 In the fourth study, an open-label flexible-dose trial, we are only reporting the results from new patients that were enrolled and completed (n = 64) to account for bias treatment effects of rollover participants. Notably, newly enrolled participants had higher symptom severity than rollover participants. The MADRS total scores decreased by −7.3 mean points across all groups. The MADRS response and remission rates were calculated using either an observed case (n = 210) or a last observation carried forward method (n = 336). At week 26, MADRS response and remission rates were 43.3% and 53.3%, respectively, using the observed case method, and 37.2% and 45.8%, respectively, using the last observation carried forward method. This was pooled across all cariprazine groups. No comparison was completed between groups.Reference Vieta, Earley and Burgess 23
The fifth study was a randomized, double-blind, placebo-controlled, parallel-group, fixed-dose study. Participants were randomized using a 1:1:1 ratio to receive either placebo (n = 254) or 1.5 mg/day (n = 252) or 3.0 mg/day (n = 253) cariprazine. Participants in the cariprazine groups (n = 505) began at 1.5 mg/day. The 3.0 mg/day cariprazine group received the higher dose after 14 days.Reference Sachs, Yeung, Rekeda, Khan, Adams and Fava 27 The mean reduction in MADRS total score was significantly greater in the 1.5 mg/day cariprazine group than in the placebo group (P = 0.005). The MADRS response was also significantly greater for the 1.5 mg/day cariprazine group than for the placebo group at week 6 (P = 0.3409). Notably, the 3.0 mg/day cariprazine group did not have statistically significant reductions in MADRS score compared to the placebo group (P = 0.072). Similarly, the MADRS remission rates between the placebo group and the 1.5 mg/day and 3.0 mg/day cariprazine groups were not statistically significant (P = 0.3691 and P = 0.1155, respectively).Reference Sachs, Yeung, Rekeda, Khan, Adams and Fava 27
Main effects of adjunctive cariprazine treatment on depressive symptomatology
The four studies included in the random-effects model were all randomized, double-blind, placebo-controlled trials.Reference Durgam, Earley and Guo 24 -Reference Sachs, Yeung, Rekeda, Khan, Adams and Fava 27 The included studies had a combined total of 1470 participants that received cariprazine ADT at any dose and 857 participants in the placebo group. All included studies measured depression outcomes using the MADRS total score. The SMD in MADRS scores was −1.79 (95% CI: −2.89, −0.69) and the overall effect size was 3.19 (P = 0.001) with a trend toward favoring cariprazine (Figure 2). The I2 value was 99%, indicating the included studies were highly heterogeneous.

Figure 2. Standard mean difference in MADRS change.
For Durgam et al.Reference Durgam, Earley and Guo 24, the LSMD in MADRS scores in the 1.0–2.0 mg/d cariprazine group was −13.4 (SD = 0.5), while the LSMD in MADRS score in the 2.0–4.0 mg/d cariprazine group was −14.6 (SD = 0.6). The LSMD in MADRS score in the placebo group was −12.5 (SD = 0.5).Reference Durgam, Earley and Guo 24 Fava et al.Reference Fava, Durgam and Earley 26 had a total of 231 participants, with 81 randomized into the placebo group and 149 randomized into treatment groups. The LSMD in MADRS scores in the 0.1–0.3 mg/d arm was −7.5 (SD = 1.1), while the LSMD in MADRS score in the 1.0–2.0 mg/d arm was −9.8 (SD = 1.1). The LSMD in the placebo arm was −8.0 (SD = 1.0).Reference Fava, Durgam and Earley 26 Earley et al.Reference Earley, Guo, Németh, Harsányi and Thase 25 had a total of 527 participants, with 258 randomized into the placebo arm and 269 randomized into the treatment arm.Reference Earley, Guo, Németh, Harsányi and Thase 25 Participants randomized into the treatment arm received 1.5–4.5 mg/d of cariprazine as an adjunct to antidepressant therapy.Reference Earley, Guo, Németh, Harsányi and Thase 25 The LSMD in MADRS scores of participants given cariprazine was −7.7 (SD = 0.5) compared to the LSMD for placebo, which was −7.5 (SD = 0.5).Reference Earley, Guo, Németh, Harsányi and Thase 25 For Sachs et al.Reference Sachs, Yeung, Rekeda, Khan, Adams and Fava 27, the LSMD in MADRS scores in the 1.5 mg/day cariprazine group was −14.1 (SD = 0.7), while the LSMD in MADRS score in the 3.0 mg/day cariprazine group was −13.1 (SD = 0.7). The LSMD in MADRS score in the placebo group was −11.5 (SD = 0.7).
For Durgam et al.Reference Durgam, Earley and Guo 24, the pooled response and remission RRs were calculated to be 1.27 (95% CI: 1.07, 1.52) and 1.07 (95% CI: 0.86, 1.33), respectively, and the pooled all-cause dropout RR was 1.68 (95% CI: 1.17, 2.42). For Earley et al.Reference Earley, Guo, Németh, Harsányi and Thase 25, the response and remission RRs were calculated to be 1.03 (95% CI: 0.78, 1.35) and 0.84 (95% CI: 0.64, 1.12), respectively, and the pooled all-cause dropout RR was 1.49 (95% CI: 1.02, 2.19). For Fava et al.Reference Fava, Durgam and Earley 26, the pooled response and remission RRs were 1.32 (95% CI: 0.86, 2.03) and 1.12 (95% CI: 0.68, 1.83), respectively, and the pooled all-cause dropout RR was 1.02 (95% CI: 0.48, 2.18). For Sachs et al.Reference Sachs, Yeung, Rekeda, Khan, Adams and Fava 27, the pooled response and remission RRs were 1.19 (95% CI: 1.07, 1.35) and 0.90 (95% CI: 0.84, 1.11), respectively, and the pooled all-cause dropout RR was 1.74 (95% CI: 0.71, 4.25). The pooled remission, response and all-cause drop-out RR are illustrated in Figures 2–5.
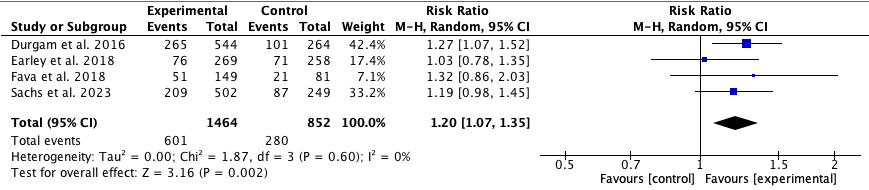
Figure 3. Pooled response RR.

Figure 4. Pooled remission RR.
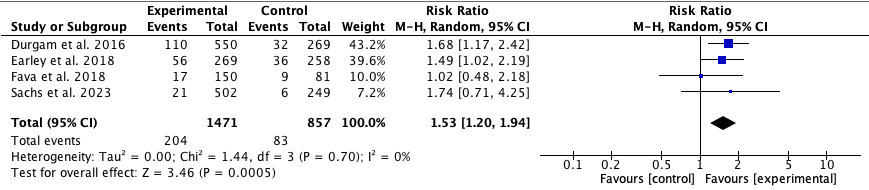
Figure 5. Pooled all-cause dropout RR.
Discussion
Our current review systematically evaluated the effects of adjunct cariprazine treatment in populations with MDD. Four studies employed a randomized double-blind, placebo-controlled study design.Reference Durgam, Earley and Guo 24 -Reference Sachs, Yeung, Rekeda, Khan, Adams and Fava 27 One study was an open-label study design with no placebo group.Reference Vieta, Earley and Burgess 23 Two studies found significant reductions in depressive symptoms as measured by the MADRS total score.Reference Durgam, Earley and Guo 24 , Reference Sachs, Yeung, Rekeda, Khan, Adams and Fava 27 Sachs et al.Reference Sachs, Yeung, Rekeda, Khan, Adams and Fava 27 found that participants randomized to 1.5 mg/day had statistically significant reductions in depressive symptoms and met MADRS response criteria compared to placebo. Interestingly, there was a statistical difference between the 1.5 mg/day cariprazine group and the placebo group, but not the 3.0 mg/day cariprazine group and the placebo group at week 2, despite both groups receiving 3.0 mg/day at that point (since there was titration to 3.0 mg/day at day 15).Reference Sachs, Yeung, Rekeda, Khan, Adams and Fava 27 This may reflect random variations as well as reflect the literature regarding increased placebo response in trials with two intervention arms rather than one.Reference Papakostas and Fava 29 Notably, there were no statistically significant reductions in depressive symptoms, as well as MADRS remission and response for the 3.0 mg/day cariprazine group compared to the placebo group. In contrast, Durgam et al.Reference Durgam, Earley and Guo 24 found that participants in both cariprazine groups met MADRS response criteria at week 8. While participants receiving 2–4.5 mg/day cariprazine had significant mean reductions in MADRS compared to placebo, the 1.0–2.0 mg/day cariprazine group demonstrated no statistically significant change.Reference Durgam, Earley and Guo 24 Moreover, in Fava et al.Reference Fava, Durgam and Earley 26 findings, the 1.0–2.0 mg/day and 0.1–0.3 mg/day treatment groups demonstrated no significant improvements in depression scores compared to the placebo group.Reference Fava, Durgam and Earley 26 This trial suggests that higher doses of adjunctive cariprazine treatment are necessary to have significant antidepressant effects, although this was not the case for the most recent cariprazine study, which suggested that the antidepressant response in the 3.0 mg/day dose did not separate from placebo after 6 weeks, while the 1.5 mg/day dose did.Reference Sachs, Yeung, Rekeda, Khan, Adams and Fava 27 These conflicting findings suggest that further dose optimization studies are required to determine the appropriate dose of adjunctive cariprazine treatment to be administered in real-world clinical settings. In the findings from Earley et al.Reference Earley, Guo, Németh, Harsányi and Thase 25, when participants were administered 1.5–4.5 mg/day of cariprazine ADT, there was no statistically significant LSMD in MADRS compared to placebo despite the higher dose.Reference Earley, Guo, Németh, Harsányi and Thase 25 Importantly, all studies showed non-significant improvements in MADRS remission rates.
Moreover, our random-effects model revealed moderate antidepressant effects of cariprazine as an adjunct therapy, with a mean difference in MADRS scores of −1.79 (95% CI: −2.89, −0.69, P = 0.001). As such, current findings regarding the potential antidepressant and anti-anhedonic effects of cariprazine ADT may be less consistent compared to other SGAs. Additionally, our pooled response RR and remission RR were calculated as 1.20 (95% CI: 1.07, 1.35, P = 0.002) and 0.97 (95% CI: 0.84, 1.11, P = 0.65), respectively, indicating that individuals prescribed cariprazine ADT have 1.20 times the risk of responding and 0.97 times the risk of remitting. The RR for response was statistically significant with a P-value of <0.05; however, the RR for remission was not statistically significant with a P-value of >0.05. These results suggest that cariprazine ADT is efficacious for achieving antidepressant response in patients.
A 2016 meta-analysis of RCTs that observed the relapse and remission rates of patients with MDD treated with adjunctive SGAs reported that at the time, cariprazine with an ADT did not demonstrate antidepressive effects compared to placebo with ADT.Reference Wang, Han and Lee 30 This conclusion was reached from unpublished data, and the authors did mention that current RCTs were still ongoing.
The remission rates of cariprazine at the endpoint of two clinical trialsReference Durgam, Earley and Guo 24 , Reference Earley, Guo, Németh, Harsányi and Thase 25 ranged from 24.4% to 32.1%, which is comparable to remission rates reported from clinical trials determining the efficacy of other SGAs. For example, aripiprazole was found to have a remission rate of 29.9% in a clinical trial with 905 patients who showed no response to traditional ADTs.Reference Nelson, Rahman and Laubmeier 31 A clinical trial looking at the efficacy of ziprasidone in 120 patients had a remission rate of 32.7%.Reference Papakostas, Vitolo and Ishak 32 Adjunctive olanzapine seemed to have a much higher remission rate of 41.9% in a study with 259 subjects,Reference Meyers, Flint and Rothschild 33 suggesting that this SGA may lead to remission of depression more effectively than other antipsychotics. However, it should be noted that the remission rates reported in the trials with cariprazine were not significant when compared to remission rates of the placebo groups. Therefore, we conclude that adjunctive cariprazine treatment does not show efficacy for remission of depressive episodes in MDD.
In particular, the proposed tolerated dose in MDD populations has varied and improvements in depressive symptoms were only observed in a high-dose (ie, 4.5 mg/day) intervention for a single double-blind study design.Reference Durgam, Earley and Guo 24 In the only open-label study, clinically significant reductions were observed in depression scores following 1.5–4.5 mg/day of cariprazine ADT. However, the primary outcome of this study was the safety and tolerability of cariprazine. As such, no comparator placebo group was included to evaluate the effects of cariprazine ADT on the change in depressive symptoms.Reference Vieta, Earley and Burgess 23 It was previously proposed that 2.0 mg/day is the highest tolerated dose in MDD populations.Reference Papp, Gruca, Lasoń-Tyburkiewicz, Adham, Kiss and Gyertyán 34 Further investigation is required regarding dose finding for the demonstrated antidepressant effects of adjunct cariprazine therapy.
Mechanism of action
Cariprazine obtained FDA approval as an adjunct treatment for MDD, under the brand name Vraylar®, in December 2022. Originally, it was approved as an atypical antipsychotic for the treatment of schizophrenia and the various mood episodes associated with bipolar I disorder, and subsequent reviews of efficacy across clinical trials have shown positive results.Reference Citrome 35 , Reference Stahl, Laredo and Morrissette 36 Cariprazine joins a growing list of atypical antipsychotics approved for the adjunctive treatment of MDD.
Other atypical antipsychotics (eg, aripiprazole, brexpiprazole, olanzapine, and quetiapine) act on dopaminergic and serotonergic pathways in the brain. The SGAs are typically classified based on their affinity and effects on dopaminergic receptors.Reference Ragguett and McIntyre 15 Recently, third-generation antipsychotics have shown potential anti-anhedonic effects through partial agonism of the D2 receptor.Reference Calabrese, Sanchez and Jin 37 Partial agonists have lower intrinsic affinity and may act as functional agonists or functional antagonists depending on the neurotransmitter environment.Reference Lieberman 38 Cariprazine is a novel third-generation antipsychotic that is a partial agonist of the dopamine D2/D3t, with a reported 10-fold greater binding affinity for the D3 receptor, which is an important finding considering the expression pattern of the D3 receptor in the brain.Reference Delcourte, Ashby and Rovera 39 , Reference Kiss, Horváth and Némethy 40
Although both subtypes of receptors are implicated in corticostriatal and limbic circuits, D3 receptors are often expressed in brain areas associated with motivation and reward-related behavior such as the substantia nigra pars compacta.Reference Carnicella, Drui and Boulet 12
Cariprazine is also a partial agonist of serotonin 5-hydroxytryptamine receptor 1A (5-HT1A) receptors, which has been purported to explain the efficacy of its use as an adjunctive treatment alongside pharmacotherapies targeting serotonin.Reference Celada, Puig, Amargós-Bosch, Adell and Artigas 41 Cariprazine has been shown to have postsynaptic 5-HT2A receptor antagonism, but at a lower affinity compared to most other atypical antipsychotics.Reference Eison and Mullins 42 Yet, from a drug mechanism perspective, RCTs have failed to show a mechanistic relationship between the efficacy of atypical antipsychotics and their antidepressant effect, such as for ziprasidone with one of the highest 5-HT2A receptor affinities.Reference Papakostas, Fava and Baer 43 Preclinical findings support the efficacy of cariprazine in reducing depressive symptoms such as anhedonia and anxiety, which lends support to the findings of the clinical trials discussed in this analysis.Reference Papp, Gruca, Lasoń-Tyburkiewicz, Adham, Kiss and Gyertyán 34 , Reference Duric, Banasr and Franklin 44
Cariprazine is broken down into two major metabolites in the body: desmethyl cariprazine (DCAR) and didesmethyl cariprazine (DDCAR), which show high affinity for D3, D2, and 5HT receptors in rat brains.Reference Kiss, Némethy and Fazekas 45 DCAR and DDCAR may play a role in significantly contributing to the antidepressant efficacy of cariprazine, although only pharmacokinetic and pharmacodynamic modeling studies of these compounds have been published.Reference Kiss, Némethy and Fazekas 45 , Reference Periclou, Phillips, Ghahramani, Kapás, Carrothers and Khariton 46
Limitations and future direction
There are several limitations to this meta-analysis. First, there was no active comparator group in any included study. Indeed, all studies that included a placebo were based just on an inert placebo. The absence of an active treatment comparator group limits the significance of findings because it remains unclear whether cariprazine represents a meaningful improvement to existing treatment options. Second, the studies analyzed used a flexible dose of adjunctive cariprazine. While this may be more representative of real-world practice, it does not allow for the determination of a specific and optimal dose. Third, the findings reported cannot be generalized to MDD patients with certain comorbid psychiatric disorders as the heterogeneity between clinical groups in the separate studies limited the interpretation of the findings. For example, two of the studies analyzed excluded patients who had a comorbid axis I disorder as defined by the DSM-IV. This finding excludes the large majority of real-world MDD patients who do have one or more comorbid diagnoses. As such, the findings may be limited in their real-world, clinical implications. In addition, the patient characteristics were different across the groups studied. For example, Fava et al.Reference Fava, Durgam and Earley 26 noted that the proportion of placebo patients with a duration of MDD that lasted more than 5 years was higher than in the patients assigned cariprazine. Consequently, the heterogeneity between clinical groups in the separate studies limited the interpretation and generalizability of the findings. Cariprazine may not be an effective treatment for patients with certain comorbid conditions that require further attention and consideration.
Moreover, findings from recent network meta-analysis (NMA) evaluating the efficacy of other SGAs show greater response rates compared to placebo. For example, in a 2015 NMA investigating the efficacy of SGA augmentation for treatment-resistant depression (TRD), all included SGAs were found to have significantly more antidepressant efficacy than placebo.Reference Zhou, Keitner and Qin 47 These SGAs included risperidone, aripiprazole, olanzapine, and quetiapine. This finding is significant as the efficacy of these SGAs has been established in the literature with high-level evidence, whereas the results of this meta-analysis report mixed results. This suggests that cariprazine may be inferior to the other SGAs currently approved for adjunctive use in MDD. Future studies should attempt to compare the efficacy of cariprazine to other approved SGAs currently used in MDD treatment to effectively evaluate whether cariprazine represents a clinically meaningful improvement to existing SGA treatment options.
Conclusion
In conclusion, our current meta-analysis evaluated the effects of adjunct cariprazine treatment in populations with MDD. Only one study found significant reductions in depressive symptoms as measured by MADRS indicating treatment response to cariprazine. This was seen with 2–4.5 mg/day cariprazine dose. However, all studies showed non-significant improvements in MADRS remission rates. Pooled response RR was significant and indicated a greater risk of response; however, pooled remission RR was not significant. Notably, findings from NMAs have shown a significant treatment response of several existing SGAs (ie, risperidone, aripiprazole, olanzapine, and quetiapine). Therefore, the mixed findings from the current meta-analysis indicate that cariprazine does not offer improved treatment efficacy compared to existing SGAs. Future clinical trials should compare cariprazine treatment to existing SGAs to accurately evaluate whether cariprazine offers improvements over existing treatment options rather than trials using a non-treatment placebo.
Author contribution
Investigation: R.B.M., D.C.C., R.S.M., S.S., S.H.; Supervision: R.B.M.; Validation: R.B.M., J.D.D., L.P.; Writing – review & editing: J.D.D., D.C.C., L.P., R.S.M., S.S., S.H., H.G.; Data curation: D.C.C., H.G.; Methodology: D.C.C., R.S.M., S.S., S.H., H.G.; Writing – original draft: D.C.C., S.S., S.H., H.G.; Project administration: R.S.M., H.G.
Disclosure
Dr. Roger S. McIntyre has received research grant support from Canadian Institute of Health Research (CIHR)/Global Alliance for Chronic Diseases (GACD)/National Natural Science Foundation of China (NSFC) and the Milken Institute and speaker/consultation fees from Lundbeck, Janssen, Alkermes, Neumora Therapeutics, Boehringer Ingelheim, Sage, Biogen, Mitsubishi Tanabe, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular Therapies, NewBridge Pharmaceuticals, Viatris, AbbVie, and atai Life Sciences. Dr. Roger S. McIntyre is the CEO of Braxia Scientific Corp. Dr. Joshua D. Rosenblat has received research grant support from the Canadian Institute of Health Research (CIHR), Physician Services Inc. (PSI) Foundation, Labatt Brain Health Network, Brain and Cognition Discovery Foundation (BCDF), Canadian Cancer Society, Canadian Psychiatric Association, Academic Scholars Award, American Psychiatric Association, American Society of Psychopharmacology, University of Toronto, University Health Network Centre for Mental Health, Joseph M. West Family Memorial Fund, and Timeposters Fellowship and industry funding for speaker/consultation/research fees from iGan, Boehringer Ingelheim, Janssen, Allergan, Lundbeck, Sunovion, and COMPASS.







