



The bidirectional cavopulmonary shunt (BCPS) is a standard intermediate procedure for patients with functional single ventricle, followed by the total cavopulmonary connection (TCPC). Reference Ono, Burri and Mayr1–Reference Tan, Iyengar and Donath3 However, there is a fundamental concern for the pulmonary circulation of BCPS physiology, which is entirely dependent on the single passive venous flow through the superior caval vein (SCV). Therefore, maintaining antegrade pulmonary blood flow (APBF) at BCPS remains a highly debated topic with different opinions regarding its beneficial effects. Reference Frommelt, Frommelt and Berger4–Reference Caspi, Pettitt, Ferguson, Stopa and Sandhu9 Since we believe that early volume unloading is most important to preserve systemic ventricular function, our institution carries the policy to discontinue any form of APBF at BCPS and to perform swift Fontan completion. Reference Mainwaring, Lamberti, Uzark and Spicer6,Reference Mainwaring, Lamberti, Uzark, Spicer, Cocalis and Moore8,Reference Alghamdi15 However, the quantity of pulmonary blood flow produced in this setting (BCPS alone) is much less than that of either the normal or the Fontan circulation. Based on our clinical experiences, we recognise that APBF may be necessary in high-risk patients to maintain/support BCPS circuit. The advantages of APBF include improving arterial oxygen saturation (SaO2), Reference Frommelt, Frommelt and Berger4,Reference Webber, Horvath and LeBlanc5,Reference Chen, Tulloh, Caputo, Stoica, Kia and Parry14,Reference Yan, Tong and Zhang17 promoting pulmonary artery (PA) growth, Reference Berdat, Belli, Lacour-Gayet, Planché and Serraf10,Reference Yoshida, Yamaguchi, Yoshimura, Murakami, Matsuhisa and Okita11,Reference Ferns, El Zein and Multani13,Reference Sughimoto, Zannino and Mathew16 and preventing pulmonary arteriovenous malformation (PAVM). Reference McElhinney, Marianeschi and Reddy7,Reference Henaine, Vergnat and Mercier20,Reference Hickey, Alghamdi and Elmi21 Conversely, APBF might increase the systemic venous pressure and the incidence of postoperative complications such as chylothorax, pleural effusion, longer hospital stays, Reference Frommelt, Frommelt and Berger4,Reference Webber, Horvath and LeBlanc5,Reference Yan, Tong and Zhang17 and the incidence of surgery for the atrioventricular valve (AVV). Reference Davidson, Zannino and d’Udekem19 The highest concern is the deleterious impact of imposing a volume load on the systemic single ventricle. We hypothesise that APBF might be beneficial only in high-risk patients in the current era of the early staged Fontan palliation strategy.
The purpose of this retrospective study is to clarify the indication for APBF and to evaluate the outcomes after BCPS in patients with APBF after BCPS.
Methods
Ethical statement
This study was approved by the Institutional Review Board of the Technical University of Munich (approval number 2023-422-S-KR on the 14 August 2023). Because of the retrospective nature of the study, the need for individual patient consent was waived.
Patients and data collection
We retrospectively evaluated all patients who underwent a BCPS at the German Heart Center Munich from May 1997 to December 2022. Patients with hypoplastic left heart syndrome were excluded from this study. Medical records included baseline morphology and demographics as well as pre-, intra-, and postoperative data, using digital and paper chart reviews of each patient.
Pre-BCPS assessment
All patients underwent cardiac catheterisation as the preoperative evaluation before BCPS when they were around 3 months old. Haemodynamic measurements collected included PA pressure (PAP), left atrial pressure (LAP), systemic ventricular end-diastolic pressure (EDP), arterial pressure and SaO2. Conventional systemic and pulmonary angiography was performed to identify evidence of PA distortion, aortopulmonary collaterals, veno-venous collaterals, and any other lesions. Assessment of AVV regurgitation and systemic ventricular function was evaluated with echocardiography. Reference Dietzman, Soria and DePaolo18,Reference Davidson, Zannino and d’Udekem19 Indication for leaving APBF was obtained from the records of the preoperative conference between paediatric cardiologists and surgeons.
Surgical strategy and operative techniques
BCPS was performed using cardiopulmonary bypass (CPB) as described in our previous reports. Reference Schreiber, Cleuziou, Cornelsen, Hörer, Eicken and Lange22,Reference Ono, Burri and Mayr23 Cardioplegic arrest was used only for patients who required intracardiac procedures. The azygos vein was routinely divided before the initiation of CPB. The BCPS anastomosis and PA reconstruction were performed in an on-pump beating state. The SCV was anastomosed to the right PA in an end-to-side fashion using 7-0 or 8-0 polydioxanone continuous sutures (Ethicon Inc.). APBF was closed in most of the patients and left open only in high-risk patients. The indications for APBF included high PAP more than 20 mmHg, hypoxaemia below 75% of SaO2, hypoplastic left PA (smaller than 3 mm, LPA index below 60 mm2/m2), late BCPS older than 18 months, or early BCPS younger than 90 days. When APBF was through the native pulmonary valve, we did not close the main PA, and APBF was distributed into both the right and left PA. When APBF was through the aortopulmonary shunt (APS), the shunt flow was left open and the main PA was narrowed or ligated/clipped between the distal anastomosis of BCPS and the APS. The techniques of creation of APBF in the setting of APS were described in our previous study. Reference Euringer, Kido and Ruf24
Postoperative management and follow-up data collection
A catheter to monitor central venous pressure was routinely inserted into the right internal jugular vein. As for the anticoagulation strategies, postoperative standard thrombosis prophylaxis after BCPS in the intensive care unit consisted of intravenous administration of unfractionated heparin (5000 IU/m2/d) with a target partial thromboplastin time of 60 s, until all central lines (usually a 4.5 Fr catheter) were removed (usually 4–5 postoperative days). Patients were followed up by paediatric cardiologists as outpatients and follow-up times were defined per patient as the time from the day of BCPS to the last visit. For the patients who died, the data were collected at the time of death. The follow-up data from the time of the surgery until the last known record of the patients were regularly tracked using our institutional single ventricle patient database system.
Statistical analysis
Categorical variables were presented as absolute numbers and percentages. A chi-squared test was used for categorical data. Continuous variables are expressed as medians with interquartile ranges (IQRs). An independent sample t-test was used to compare normally distributed variables. The Mann-Whitney U test was used for variables that were not normally distributed. Survival after BCPS and completion of TCPC were calculated using the Kaplan–Meier method, and comparison was performed using the log-rank test. Risk factors for mortality after BCPS were identified using uni- and multivariate Cox regression models. Data analysis and graphing were performed with the Statistical Package for the Social Sciences (SPSS) version 28.0 for Windows (IBM, Ehningen, Germany) and the R-statistical software (state package).
Results
Patients’ characteristics and pre-BCPS haemodynamic assessment
Among 461 patients who underwent BCPS at our centre during the study period, 38 patients (8.3%) had APBF, and 423 (91.7%) did not. Patients’ characteristics are shown in Table 1, and the flow chart of the patients is shown in Supplementary Figure S1. There was no difference in the distribution of primary diagnosis, associated anomalies, or stage I palliations between patients with and without APBF. Pre-BCPS cardiac catheterisation data are shown in Supplementary Table S1. Median PAP (16 versus 14 mmHg, p = 0.175), LAP (7 versus 6 mmHg, p = 0.204), transpulmonary gradient (8.5 versus 8.0 mmHg, p = 0.660), and SaO2 (76 versus 77%, p = 0.687) were similar between both groups. However, the percentage of patients with PAP more than 20 mmHg was higher in patients with APBF than those without APBF (29.2 versus 11.0 %, p = 0.010).
Table 1. Baseline characteristics of patients

APBF = antegrade pulmonary blood flow; PAIVS = pulmonary atresia with intact ventricular septum; TGA = transposition of the great arteries.
Indication for APBF and perioperative data
The indications for APBF included high PAP in 13 patients, hypoxaemia in 10, hypoplastic left PA in 8, late BCPS older than 18 months in 4, early BCPS younger than 90 days in 2, and association of diaphragm paralysis in 1 (Fig. 1). The source of APBF was native antegrade flow through the pulmonary trunk in 9 (23.7%) patients and APS in 29 (76.3%) patients. Of 29 patients with APS, the central PA was ligated/clipped between BCPS and APS in 7 patients, and APBF was directed to the left PA. In two patients, the central PA was narrowed between BCPS and APS, and APBF was directed to both PAs. In the remaining 20 patients, the APBF through APS was distributed to the PAs without restriction. The flow distribution of the BCPS and APBF is shown in Figure 2. Among 38 patients with APBF, APBF was left at the time of BCPS in 25 patients, and APBF was added in a separate procedure in 13 patients, a median of 66 days after BCPS.

Figure 1. Indication for the APBF. APBF = antegrade pulmonary blood flow; PAP = pulmonary artery pressure; LPA = left pulmonary artery; BCPS = bidirectional cavopulmonary shunt.
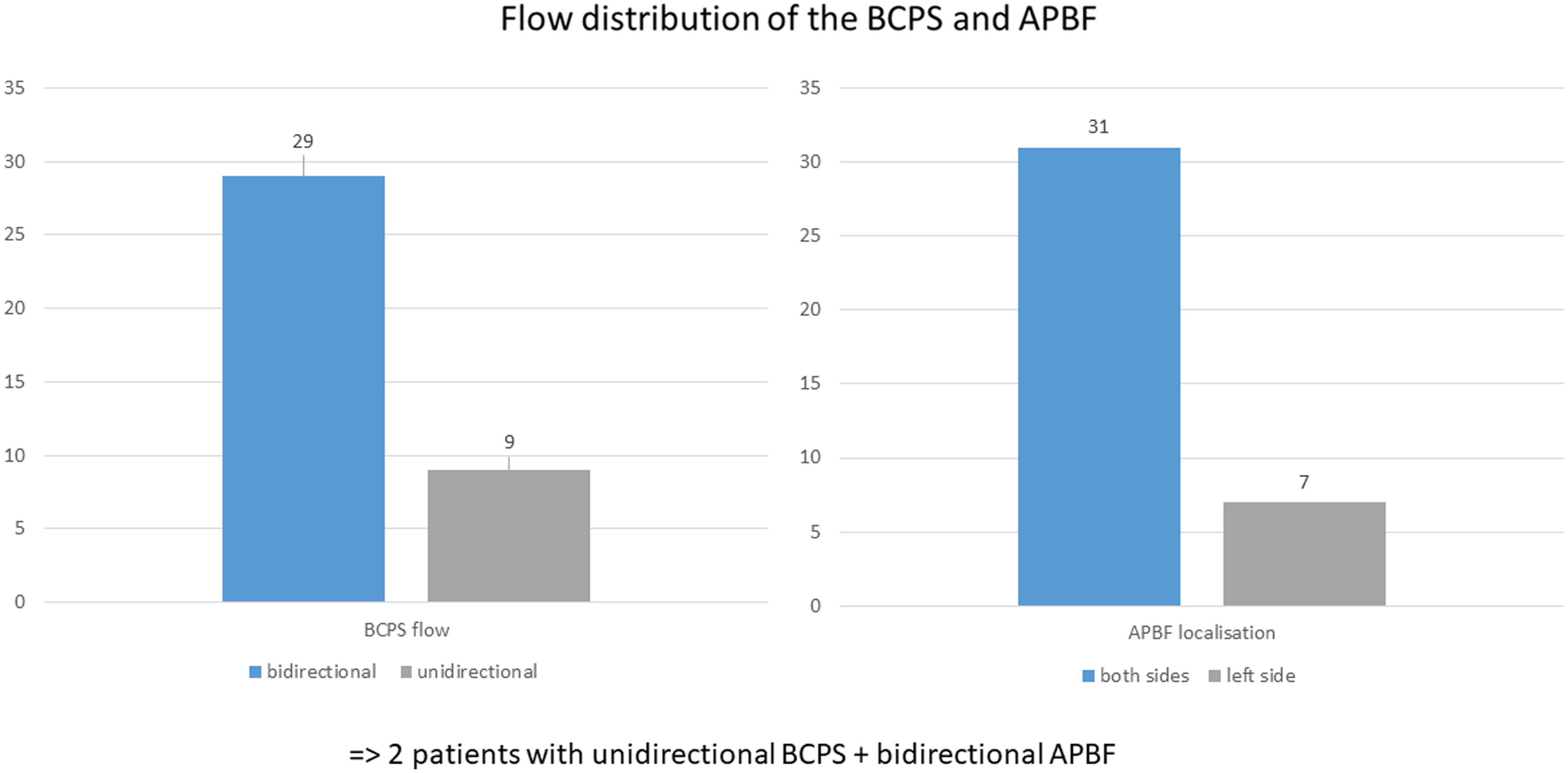
Figure 2. Flow distribution of the BCPS and APBF. BCPS = bidirectional cavopulmonary shunt; APBF = antegrade pulmonary blood flow.
Perioperative data are shown in Table 2. Median age (7.8 versus 6.3 months, p = 0.548) and weight (5.6 versus 6.1 kg, p = 0.750) at BCPS were similar between the groups. The median CPB time (73 versus 63 minutes, p < 0.01) was longer, and the frequency of PA reconstruction (44.7 versus 26.5%, p = 0.016) was higher in patients with APBF compared to those without APBF. Postoperatively, patients with APBF demonstrated a longer hospital stay (median: 22 versus 14 days, p = 0.018), higher incidence of prolonged pleural effusion (p = 0.041), higher incidence of thromboembolic complications (p < 0.001), and higher in-hospital mortality (10.5 versus 2.1 %, p = 0.003), compared to those without APBF. Four patients with APBF died in the hospital on days 6, 43, 46, and 63 after BCPS, due to progressive hypoxaemia. All of them had APS as the source of APBF (Supplementary Figure S2).
Table 2. Perioperative variables
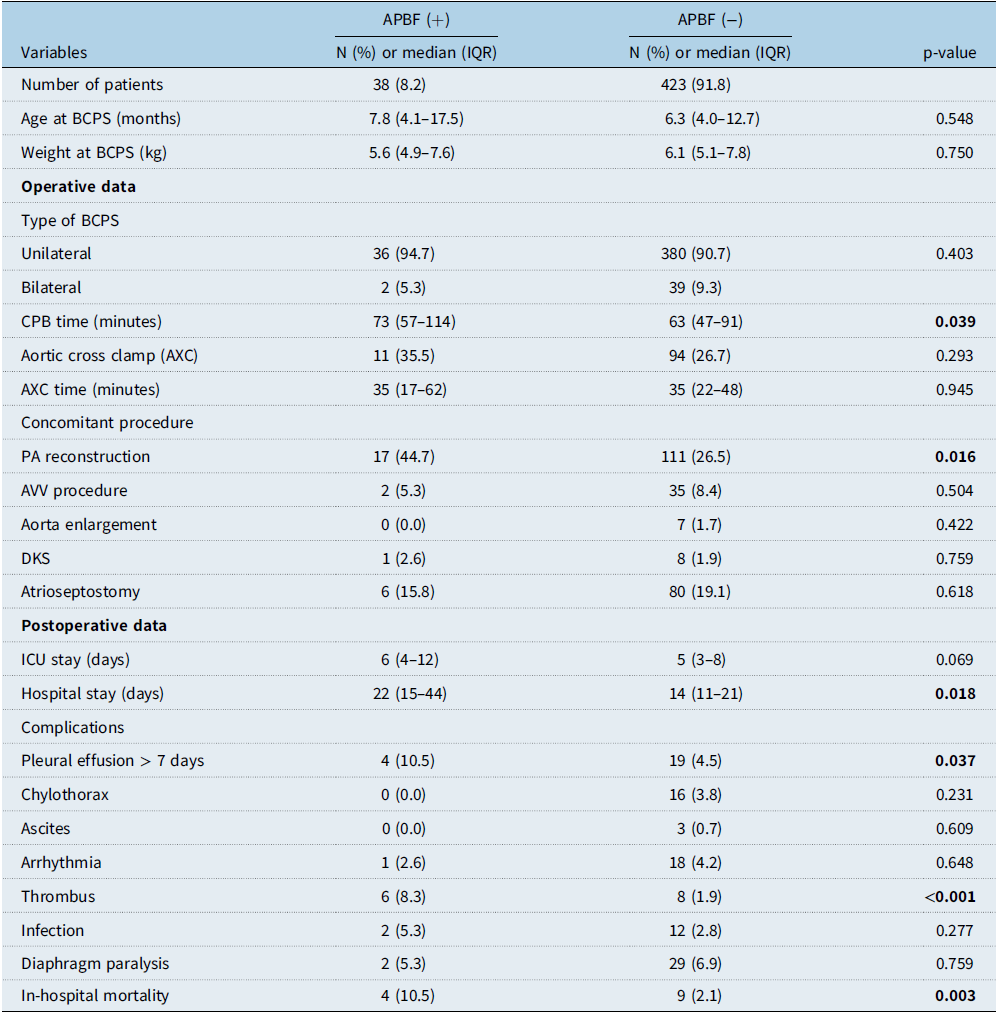
APBF = antegrade pulmonary blood flow; BCPS = bidirectional cavopulmonary shunt; CPB = cardiopulmonary bypass; PA = pulmonary artery; AVV = atrioventricular valve; DKS = Damus–Kaye–Stansel; ICU = intensive care unit; IQR = interquartile range.
Follow-up data
Among 448 hospital survivors, the median follow-up after BCPS was 6.9 (IQR: 3.0–16.7) years. Eleven patients died a median of 0.6 (IQR: 0.4–1.7) years after BCPS (3 patients with APBF and 8 patients without APBF, p = 0.046), and 413 patients (30 with APBF and 383 without APBF) underwent TCPC. The remaining 24 patients waited for TCPC or did not indicate Fontan completion (Supplementary Figure S1). Pre-TCPC cardiac catheterisation demonstrated a significantly higher PAP (11.5 versus 9.0 mmHg, p < 0.001) and LAP (6.0 versus 5.0 mmHg, p = 0.030) in patients with APBF, compared to those without (Table 3). The pre-TCPC PA index was similar between the groups (p = 0.335). Survival after hospital discharge following BCPS at 5 years was 90.7% in patients with APBF and 95.5% in patients without APBF (p = 0.244, Fig. 3). The rate of Fontan completion was lower in patients with APBF compared to those without APBF (p < 0.001, Supplementary Figure S3). The median time between BCPS and TCPC (2.3 versus 1.5 years, p = 0.025) was longer, and the median age at TCPC (3.9 versus 2.2 years, p = 0.010) was older in patients with APBF, compared to those without APBF. Survival after TCPC was essentially identical between both patient groups (93.8 versus 94.5% at 10 years, p = 0.753, Fig. 4).

Figure 3. Transplant-free survival of hospital survivors after BCPS comparing the patients who had APBF and those who did not. BCPS = bidirectional cavopulmonary shunt; APBF = antegrade pulmonary blood flow.

Figure 4. Transplant-free survival after TCPC comparing the patients who had APBF left and those who did not. TCPC = total cavopulmonary connection; APBF = antegrade pulmonary blood flow.
Table 3. Pre-total cavopulmonary connection (TCPC) data

APBF = antegrade pulmonary blood flow; PA = pulmonary artery; IQR = interquartile range.
Risk factor analysis
The risk analysis for mortality after BCPS was performed in all patients (Table 4). Extracardiac anomalies (p < 0.001, HR: 5.359), unbalanced atrioventricular septal defect (UAVSD) (p < 0.001, HR: 6.517), anomalous pulmonary venous drainage (p = 0.034, HR: 3.302), heterotaxy (p = 0.044, HR: 2.132), previous pulmonary artery banding (PAB) (p = 0.012, HR: 2.307), number of palliations (p = 0.049, HR: 1.453), PAP before BCPS (p < 0.001, HR: 1.148), LAP before BCPS (p < 0.001, HR: 1.139), systemic ventricular systolic pressure (p = 0.028, HR: 1.023), EDP (p = 0.001, HR: 1.147), CPB time at BCPS (p < 0.001, HR: 1.010), and APBF (p = 0.012, HR: 2.681) were identified as risk factors in the univariate model. The multivariate models revealed extracardiac anomalies (p < 0.001, HR: 28.552), previous PAB (p = 0.017, HR: 5.790), PAP before BCPS (p = 0.009, HR: 1.228), and systemic ventricular systolic pressure (p = 0,015, HR: 1.045) as independent risk factors.
Table 4. Preoperative variables influencing mortality after BCPS in all patients
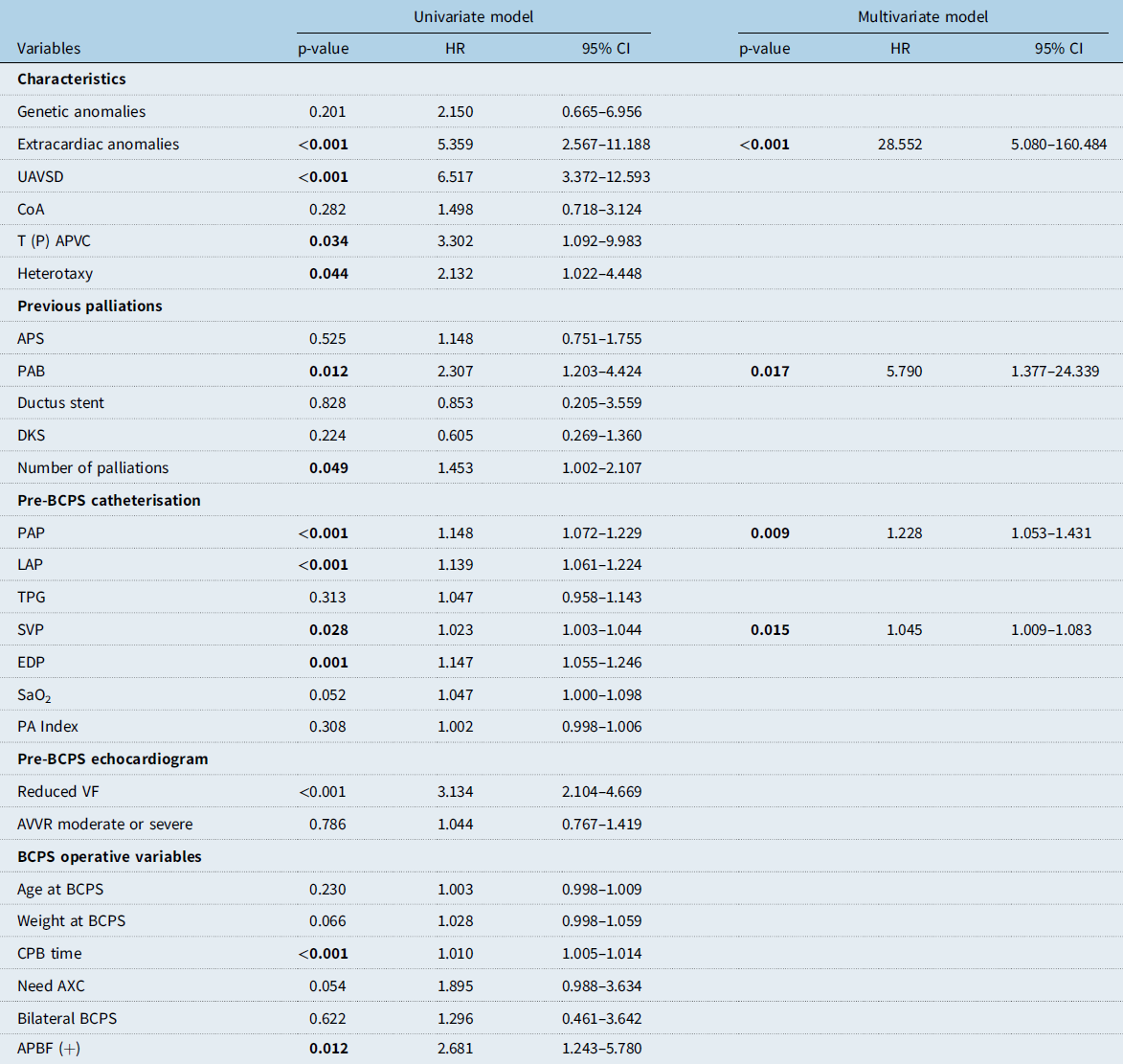
BCPS = bidirectional cavopulmonary shunt; UAVSD = unbalanced atrioventricular septal defect; CoA = coarctation of the aorta; T(P)APVC = total (partial) anomalous pulmonary venous connection; APS = aortopulmonary shunt; PAB = pulmonary artery banding; DKS = Damus–Kaye–Stansel; PAP = pulmonary artery pressure; LAP = left atrial pressure; TPG = transpulmonary gradient; SVP = systemic venous pressure; EDP = end-diastolic pressure; SaO2 = oxygen saturation; PA = pulmonary artery; VF = ventricular function; AVVR = atrioventricular valve regurgitation; CPB = cardiopulmonary bypass; AXC = aortic cross clamp; APBF = antegrade pulmonary blood flow.
Subgroup analysis was performed in 38 patients with APBF. The risk analysis for mortality after BCPS was performed, and the results are shown in Supplementary Table S2. In the univariate model, genetic anomalies (p = 0.015, HR: 7.736), extracardiac anomalies (p = 0.024, HR: 7.262), UAVSD (p = 0.005, HR: 8.896), systemic ventricular pressure (p = 0.015, HR: 1.054) and EDP (p = 0.005, HR: 1.294), SaO2 (p = 0.034, HR: 1.197), and late (separate) APBF (p = 0.033, HR: 4.739) were identified as risks. Kaplan–Meier survival in patients with concomitant APBF and late APBF is shown in Supplementary Figure S4. In the multivariate model, genetic anomalies (p = 0.011, HR: 44.464), extracardiac anomalies (p = 0.023, HR: 31.866), and an elevated pre-BCPS systolic ventricular pressure (p = 0.002, HR: 1.089) were identified as independent predictors of mortality after BCPS.
Discussion
In this study, APBF was open in 8.3% following BCPS in high-risk patients. The main indications for APBF included high PAP, hypoxaemia, and hypoplastic PA. In patients with APBF, increased hospital mortality and morbidities were observed, compared with those who did not have APBF at the time of BCPS. However, survival after TCPC was similar between patients with and without APBF although the patients with APBF were older at TCPC compared to those without.
APBF at the time of BCPS
Historically, BCPS was introduced as an intermediate procedure for high-risk Fontan patients and was proved as a useful staging procedure before the Fontan procedure. The rationale for BCPS as an interstage procedure is to provide an effective ventricular volume unloading which has been associated with advantageous changes to the single ventricle. Reference Bridges, Jonas, Mayer, Flanagan, Keane and Castaneda25,Reference Freedom, Nykanen and Benson26 These beneficial effects of BCPS are age dependent and less likely to occur in older infants and children. Reference Mahle, Wernovsky, Bridges, Linton and Paridon27 Leaving APBF may mitigate these beneficial effects of BCPS, might be the cause of insufficient reduction of the volume overload, and also increase the complexity of the Fontan completion, as it requires cross-clamping and arresting the heart for the transection and over-sewing of the pulmonary valve and the pulmonary trunk. On this basis, we have adopted our institutional policy of early BCPS without APBF and swift Fontan completion over 20 years. With this strategy, most of the patients successfully achieved Fontan completion with excellent results. Reference Ono, Kasnar-Samprec and Hager28 However, we must reconsider leaving APBF in certain high-risk patients at the time of BCPS. The main reasons for leaving APBF are as follows: high PAP, hypoplastic PA, hypoxaemia, or very early BCPS at an age below 90 days. Adding APBF to the BCPS circuit might provide higher SaO2, improved PA growth, and prevention of PAVM (Supplementary Figure S5). In this study, we did not experience significant PAVM. The SaO2 and the PA Index were similar between patients with and without APBF at TCPC. We suspect that high-risk patients might have low pulmonary blood flow after BCPS resulting in hypoxaemia and failing BCPS, when APBF was not added into the BCPS circuit. APBF might be a rescue strategy in this scenario, by maintaining acceptable SaO2 and cardiac output. Although the short outcomes of these patients were worse than in patients without APBF, we believe most of them got good Fontan results by this option even though they needed a longer period until the Fontan procedures than normal-risk patients do. The survival after TCPC in patients with APBF was essentially identical to the patients without APBF, and this result is quite understandable as all of the patients with unfavourable physiology have been eliminated and are only now looking at the “survivors” who have demonstrated favourable physiology. Therefore, it is reasonable to maintain acceptable SaO2 for a relatively long period until Fontan completion with APBF for high-risk patients. Our results demonstrated that there was still relatively high hospital mortality after BCPS in patients with APBF. The interval between BCPS and TCPC was significantly longer in patients with APBF compared to those without. Pre-TCPC haemodynamic data demonstrated higher PAP and LAP in patients with APBF, compared to those without APBF. We interpret these last findings as the result of problematic pulmonary circulation in these patients, at the time of BCPS and even after a longer interval after BCPS.
Risk factors for mortality after BCPS
In this study, extracardiac anomalies, previous PAB, higher PAP, and higher systemic ventricular systolic pressure were identified as risk factors for mortality after the BCPS. Although there was significant overlapping in pre-BCPS PAP in patients with and without APBF, we think a PAP value of 20 mmHg or more indicates APBF. As for systemic ventricular systolic pressure, we could not explain why this variable was identified as a risk for mortality, we assume that low pulmonary blood flow might be associated with higher systolic ventricular pressure, and it might be a surrogate marker.
Adding or leaving APBF was a risk for mortality in the univariate analysis. We could not show the direct evidence in this study that APBF is beneficial for high-risk candidates for BCPS. The patients who had APBF in this study were extremely high-risk for BCPS, and simple high-risk/standard-risk group analysis was not suitable to demonstrate the usefulness of APBF.
Impact of APBF on PA development
Sugimoto et al. demonstrated that the PA index at the time of Fontan completion was higher in patients with APBF. Reference Sughimoto, Zannino and Mathew16 Gray and colleagues showed a modest increase in the PA index from BCPS to the Fontan procedure for patients with maintained APBF, compared to patients who had APBF removed at BCPS. Reference Gray, Altmann and Mosca12 Dietzman et al. demonstrated no difference in absolute PA size by the Nakata index. Reference Dietzman, Soria and DePaolo18 We found a similar PA index at TCPC between patients with and without APBF, although patients who needed APBF had a relatively high incidence of hypoplastic PA at the time of BCPS. These results might suggest the growth potential of hypoplastic PA with maintaining APBF after BCPS.
The debate over adding APBF at the BCPS for single ventricle palliation continues, as the current literature has shown mixed results on both short-term morbidity and potential long-term benefit. We think that APBF is not necessary in standard-risk patients. Early volume unloading by BCPS and swift Fontan completion by extracardiac TCPC demonstrated excellent results. Reference Ono, Kasnar-Samprec and Hager28 Of note, patients who needed APBF had a relatively high incidence of genetic anomalies. The intrinsic pathology of the pulmonary vascular system in these patients with genetic anomalies might contribute to their inadequate results after BCPS and need for APBF. In such circumstances, the inclusion of APBF in the BCPS circuit may prevent a failing BCPS and may improve the chance of achieving Fontan completion through potential mechanisms, such as better SaO2, better PA growth, and the ability to delay the timing of Fontan completion. However, these benefits must be balanced against the risks of a residual volume load for the systemic single ventricle and an increase in AVV regurgitation. Reference Davidson, Zannino and d’Udekem19
Impact of APBF on outcome after the Fontan completion
Chen et al. demonstrated lower mortality after the Fontan procedure in patients with APBF compared to those without APBF. Reference Chen, Tulloh, Caputo, Stoica, Kia and Parry14 Dietzman et al. demonstrated a comparable survival between the patients with and without APBF after the Fontan procedure. Reference Dietzman, Soria and DePaolo18 In our larger study cohort, the majority of deaths occurred between BCPS and Fontan completion. After Fontan completion, we found no impact of leaving or eliminating APBF on the composite endpoint of death and transplantation. Further research into what makes a patient a good candidate for inclusion of APBF in the BCPS circuit is warranted. Clinical decision-making on whether the APBF should be eliminated or maintained at the time of BCPS might be patient dependent. Despite trends towards enhancing PA growth and concerns of morbidity and mortality, there are insufficient data to make recommendations for or against the routine removal of ABPF at the time of BCPS. More detailed criteria for leaving APBF are mandatory through quality randomised studies with appropriate power and follow-up.
Study limitations
This study was limited by its retrospective and single-centre design and because of our relatively small sample size. Surgical and medical management may have changed during the study period, probably influencing the long-term outcomes. Our institutional approach has tended to favour maintaining APBF when pre-BCPS catheterisation demonstrates high PAP and low development of the pulmonary arteries. This study was also limited in the ability to assess differences in the presence of PAVM as there was not enough catheterisation data available to compare the two groups.
Conclusions
APBF was open at 8% following BCPS. The most frequent indication for APBF was high PAP, hypoplastic left PA, and hypoxaemia. Patients with APBF had higher hospital mortality and morbidities. However, hospital survivors with APBF demonstrated comparable survival compared to those without APBF. Survival after TCPC was also similar in patients with and without APBF, although TCPC was performed later in patients with APBF. Maintaining APBF at the time of BCPS might have a potential benefit in high-risk patients for BCPS.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951124025502.
Financial support
None.
Competing interests
None.










