



Introduction
Diastolic heart failure may be noted in children, specifically those with CHD, cardiomyopathy, and malignancies requiring chemotherapy. Reference Bu’Lock, Mott, Oakhill and Martin1–Reference Butnariu, Zamfir, Iancu, Iacob, Samasca and Lupan4 There is a paucity of data regarding the management of diastolic heart failure in children. Management of diastolic heart failure in children is often based on data from adult trials or based on theoretic or anecdotal evidence. Unfortunately, paediatric and adult heart failure differ in their aetiology, molecular manifestations, and response to specific treatments. Reference Pan, Hu, Sun, Lv, Xu and Tian3,Reference Das5 Much of the published work regarding diastolic heart failure in children focuses on etiologic associations and various diagnostic associations. Reference Pan, Hu, Sun, Lv, Xu and Tian3,Reference Butnariu, Zamfir, Iancu, Iacob, Samasca and Lupan4
The primary aim of this study was to use data from a national paediatric inpatient database to determine comorbidities, mechanical interventions, and pharmacologic interventions associated with mortality in critically ill children with isolated diastolic left heart failure.
Methods
As this study utilised deidentified data from a national database, no consents were obtained by the authors of this study. This study is in concordance with the Helsinki Declaration.
Pediatric Health Information System database
Data for this study were obtained from the Pediatric Health Information System (database. Pediatric Health Information System is an administrative and billing database that contains inpatient, emergency department, ambulatory surgery, and observation data from not-for-profit, tertiary-care paediatric hospitals in the United States. The 49 hospitals that contribute data to Pediatric Health Information System are affiliated with the Children’s Hospital Association (Lenexa, KS), a business alliance of children’s hospitals. Data quality and reliability are assured through a joint effort between the Children’s Hospital Association and participating hospitals. For the purposes of external benchmarking, participating hospitals provide discharge/encounter data including demographics, diagnoses, procedures, and charges. Data are de-identified at the time of data submission, and data are subjected to a number of reliability and validity checks before being included in the database.
Admission identification
Pediatric Health Information System database data from 2016 to 2021 were utilised for this study. Only data from those who were admitted to the neonatal ICU, pediatric ICU, or pediatric cardiac ICU at some point during the admission were extracted.
First, paediatric patients under 18 years of age were identified. Next, these paediatric admissions were then filtered on whether or not diastolic left heart failure was present. Admissions with diastolic left heart failure with systolic left heart failure or right ventricular failure were then excluded. This was done to result in only paediatric admissions with isolated diastolic left heart failure. “Isolated” is used to refer only to cardiac function, admissions with other cardiac or non-cardiac comorbidities were not excluded.
Paediatric admissions pertaining to isolated diastolic left heart failure were then divided into two groups: those with inpatient mortality and those without.
Admission characteristics
Several data points were captured for each of the included admissions. Age of admission, gender, and year of admission were captured for all admissions. Total hospital length of stay and inpatient mortality were also recorded for all admissions. Any use of “mortality” from here on after will refer to inpatient mortality during the admission of interest.
The presence of comorbidities was captured using ICD-10 codes or database flags. Database flags were utilised for infection, malignancy, need for mechanical ventilation, and need for extracorporeal membrane oxygenation. CHD was captured using ICD-10 codes for the individual lesions and then developing a composite. ICD-10 codes were also utilised to capture the following comorbidities: acute kidney injury, acute hepatic failure, cardiomyopathy, obesity, asthma, pulmonary hypertension, arrhythmia, fluid overload, acidosis, alkalosis, respiratory failure, cardiogenic shock, and cardiac arrest.
Pharmacologic interventions captured included epinephrine, norepinephrine, dobutamine, dopamine, milrinone, vasopressin, enalapril, captopril, lisinopril, labetalol, metoprolol, carvedilol, propranolol, atenolol, esmolol, losartan, sacubitril/valsartan, furosemide, chlorothiazide, acetazolamide, bumetanide, spironolactone, metolazone, torsemide, digoxin, vitamin D, cholecalciferol, carnitine, iron, thiamine, calcium chloride, calcium gluconate, sodium bicarbonate, macitentan, sildenafil, bosentan, inhaled nitric oxide, hydrocortisone, methylprednisolone, dexamethasone, and prednisolone, levothyroxine, liothyronine. Labetalol, metoprolol, carvedilol, propranolol, atenolol, and esmolol were categorised as beta-blockers. Enalapril, captopril, and lisinopril were categorised as angiotensin converting enzyme inhibitors. Sacubitril/valsartan was the only angiotensin receptor blocker and neprolysin inhibitor and was categorised as such. Furosemide, chlorothiazide, acetazolamide, bumetanide, spironolactone, metolazone, and torsemide were categorised as diuretics. Levothyroxine and liothyronine were categorised as thyroid hormone replacement.
Statistical analyses
Continuous variables were described as median and range while categorical variables were described as absolute frequency and percentage. Analyses of continuous variables across groups were conducted using a Mann–Whitney U test while analyses of categorical variables were conducted using a Fisher exact test. Characteristics were compared between paediatric diastolic left heart failure admissions with and without mortality.
Next, regression analyses were conducted to model mortality and then total hospital length of stay in only those who survived. A logistic stepwise regression was conducted to model mortality with mortality as the dependent variable and the collected comorbidities, mechanical interventions, and pharmacologic interventions as independent variables. A p-value of 0.10 was used for entry into the model and a p-value of 0.05 was used for exclusion.
Next, a linear regression was conducted to model total hospital of length of stay in admissions with survival to discharge with total hospital length of stay in days as the dependent variable and the collected comorbidities, mechanical interventions, and pharmacologic interventions as independent variables. This was done as a stepwise regression as well with a p-value of 0.10 used for entry and a p-value of 0.05 used for exclusion.
Statistical analyses were conducted using SPSS Version 23.0. A p-value of less than 0.05 was considered statistically significant. Any use of the word “significant”, “significantly”, or “significance” here after will refer to statistical significance unless explicitly stated otherwise.
Results
Cohort information
A total of 2,394 admissions with isolated diastolic left heart failure were included in the final analyses. As the source dataset included 426,029 admissions total, this represents a 0.5% incidence of isolated diastolic left heart failure among critically ill paediatric patients. Among the 2,273 admissions included in the final analyses, 121 (5%) experienced mortality, and 460 (20%) were single ventricle.
Mortality, univariate analysis
Tables 1 and 2 demonstrate differences in demographics, comorbidities, pharmacologic interventions, and mechanical interventions between admissions with and without mortality.
Table 1. Comparison of characteristics and comorbidities between those with and without mortality

Table 2. Pharmacologic interventions in paediatric admissions with isolated diastolic left heart failure with and without inpatient mortality

Mortality, regression analyses
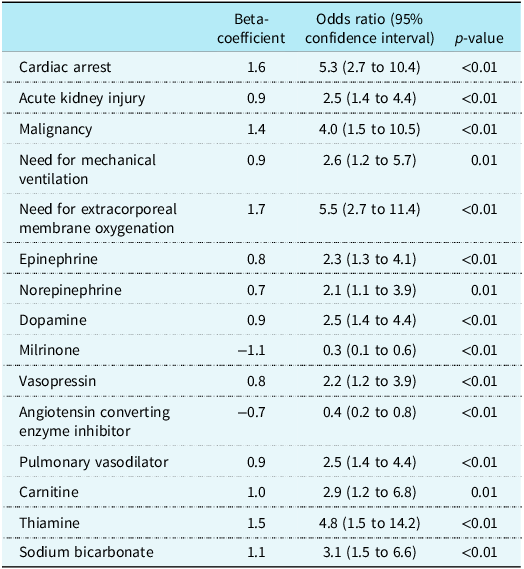
Table 3 demonstrates significant results of the multivariable logistic regression modelling for inpatient mortality. Independent variables entered into the regression that did not yield a significant result are not included in the table. The following factors were found to be associated with decreased mortality: milrinone and angiotensin converting enzyme inhibitors. Milrinone was associated with a 70% reduction in the odds of mortality while angiotensin converting enzyme inhibitors were associated with a 60% reduction in the odds of mortality (Figure 1). The following factors were found to be associated with increased mortality: acute kidney injury, malignancy, cardiac arrest, need for mechanical ventilation, need for extracorporeal membrane oxygenation, epinephrine, norepinephrine, dopamine, vasopressin, pulmonary vasodilators, carnitine, thiamine, and sodium bicarbonate.

Figure 1. Forest plot showing odds ratio of all-cause mortality with pharmacologic interventions.
Table 3. Logistic regression analysis results modelling mortality in those with isolated diastolic left heart failure
Total hospital length of stay in survivors, regression analysis
Table 4 demonstrates significant results of the multivariable linear regression modelling for total hospital length of stay in survivors. Independent variables entered into the regression that did not yield a significant result are not included in the table. The following factors were found to be associated with decreased total hospital length of stay in survivors: increasing age and diuretics.
Table 4. Linear regression analysis results modelling total hospital length of stay in those with isolated diastolic left heart failure
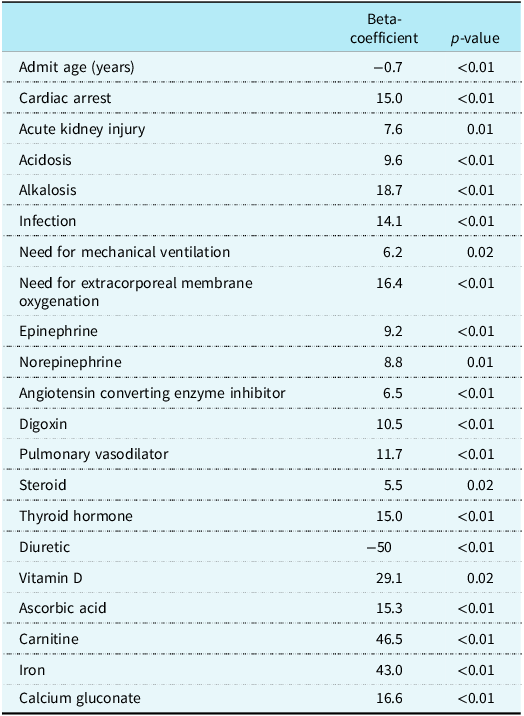
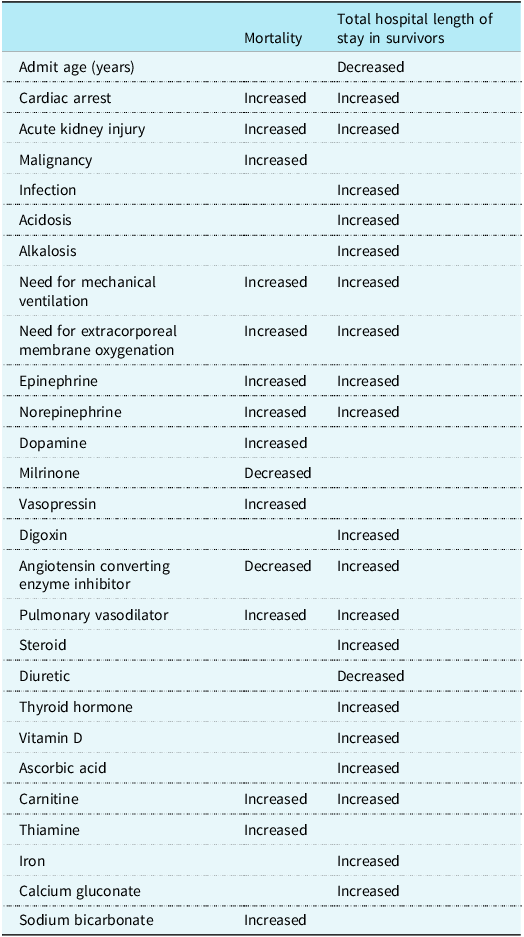
Table 5 summarises the general effects of interventions on mortality and length of stay.
Table 5. Summary of regression findings on inpatient mortality and total hospital length of stay in survivors only
Discussion
The findings of this study utilising data from a national inpatient database demonstrate that isolated diastolic dysfunction is present in 0.5% of paediatric admissions in the neonatal ICU, paediatric ICU, or paediatric cardiac ICU. Inpatient mortality is approximately 5% in such admissions. Several comorbidities are associated with increased inpatient mortality. Several pharmacologic interventions are also associated with increased risk of inpatient mortality although milrinone and angiotensin converting enzyme inhibitors are associated with decreased risk of inpatient mortality. When only admissions with survival to discharge were considered, several factors were associated with increased length of stay while only older age and diuretics were associated with decreased length of stay in survivors.
There are very limited data regarding paediatric diastolic heart failure in general. Much of the data that exist are focused on echocardiographic evaluation of diastolic heart failure. Reference Recher, Botte, Soquet, Baudelet, Godart and Leteurtre6,Reference Dragulescu, Mertens and Friedberg7 Medical management of isolated paediatric diastolic left heart failure is largely anecdotal, based on theory as well as adult data. The issue with this approach is that theory does not always translate into reality. Furthermore, children and adults have physiologic differences which may lead to different effects of interventions. Reference Das5
What is currently present in the adult literature regarding diastolic heart failure, commonly referred to as heart failure with preserved ejection fraction consists of few large trials. The J-DHF and SENIORS trials demonstrated no benefit of angiotensin converting enzyme inhibitors with all-cause mortality. Reference Yamamoto, Origasa, Hori and Investigators8,Reference Flather, Shibata and Coats9 With respect to angiotensin receptor blockers, the CHARM-preserved and I-PRESERVED trials have demonstrated that these agents are not associated with decreased hospitalisation or mortality in those with heart failure with preserved ejection fraction. Reference Yusuf, Pfeffer and Swedberg10 The PARAGON heart failure trial did not find benefit of a combined angiotensin receptor and neprolysin receptor blocker in the entire study cohort with respect to heart failure hospitalisation or cardiovascular mortality. Reference Solomon, McMurray and Anand11 The TOPCAT trial found no benefit of spironolactone on a composite outcome of heart failure hospitalisation, cardiac arrest, or cardiovascular death. Reference Pitt, Pfeffer and Assmann12 The SENIORS and J-DHF trials did not find benefit of beta-blockers with respect to heart failure hospitalisation, cardiovascular death, or all-cause mortality although significant was noted in a subset of patients with higher dose carvedilol. Reference Yamamoto, Origasa, Hori and Investigators8,Reference Flather, Shibata and Coats9 The trials DILATE-1, SOCRATES-PRESERVED, and RELAX did not find benefit of pulmonary vasodilators in mean pulmonary artery pressure, left atrial volume, n-terminal pro-beta-natriuretic peptide levels, or exercise capacity. Reference Bonderman, Pretsch and Steringer-Mascherbauer13– Reference Hussain, Mohammed and Forfia15 As previously stated, due to difference in children and adults all the way down to the cellular level, this adult data should not directly be applied to the management of children although it may offer a starting point to help design paediatric trials.
No data on treatment of isolated paediatric diastolic left heart failure truly exist. This is for both the inpatient and outpatient settings. A previous study looked at the impact of inpatient vasoactive medications in those with heart failure after cardiac surgery and found that epinephrine, norepinephrine, dopamine, dobutamine, and vasopressin were associated with increased inpatient mortality. Only milrinone was associated with decreased inpatient mortality. Reference Loomba and Flores16
The current study presents the most robust data regarding inpatient paediatric admissions with isolated diastolic heart failure. This study is able to characterise the cohort in general but also identifies factors associated with inpatient mortality. Such data may be helpful in risk-stratifying patients, particularly those at high risk for mortality. The current study also characterises the effect of pharmacologic interventions on inpatient mortality as well as length of stay in those who survive to discharge.
The current study demonstrates that acute kidney injury, malignancy, and cardiac arrest are associated with increased mortality in those with diastolic left heart failure. Malignancy is likely to be a contributing factor to the development of diastolic left heart failure while acute kidney injury and cardiac arrest are likely to be, at least in part, due to the diastolic heart failure. Previous studies have demonstrated that chemotherapy agents utilised for the treatment of malignancy, specifically anthracycline medications, are associated with the development of both diastolic and systolic left heart failure. Acute kidney injury and cardiac arrest, however, are likely a result of impaired oxygen delivery as a result of diastolic left heart failure. It has been well demonstrated that impaired oxygen delivery, as can be clinically monitored by venous saturations, or near-infrared spectroscopy, is associated with increased risk for acute kidney injury and cardiac arrest. Reference Loomba, Rausa and Sheikholeslami17–Reference Sheikholeslami, Dyson and Villarreal24
In regard to mechanical interventions, the need for mechanical ventilation and extracorporeal membrane oxygenation is noted to be associated with increased mortality in diastolic left heart failure. These likely represent a cohort of patients with greater severity of illness which may be due to the diastolic left heart failure itself or other comorbidities. The association of need for mechanical ventilation and need for extracorporeal membrane oxygenation with increased mortality is previously described.
With regards to vasoactive medications, epinephrine, norepinephrine, dopamine, and vasopressin were all associated with increased mortality while milrinone was the only agent that was associated with decreased mortality. No significant association of dobutamine with mortality is noted by the current study. The association of most vasoactive medications with increased mortality, even after adjusting for comorbidities and other pharmacologic interventions, likely represents some underlying effect of the vasoactive medications themselves but also likely is also modulated by severity of illness as sicker patients are more likely to require vasoactive medications. This is not the first study to have noted that vasoactive medications may be associated with increased inpatient mortality. This has been demonstrated in both paediatric and adult patients, in those with and without heart failure. Reference Loomba and Flores16,Reference Abraham, Adams and Fonarow25
Systemic oxygen delivery is the product of oxygen content and cardiac output. Oxygen content can further be broken down into the components of arterial saturation and haemoglobin while cardiac output can further be broken down into the components of preload, afterload, and contractility. Many vasoactive agents increase myocardial oxygen consumption which may come at the expense of systemic oxygen delivery. Many vasoactive agents also have an arterial constrictor effect. Increasing left ventricular afterload may further impact stroke volume and systemic oxygen delivery. It is important to note that simply augmenting mean arterial blood pressure does not imply augmentation of stroke volume and that increased mean arterial blood pressure may be associated with decreased stroke volume if systemic vascular resistance increases a substantial amount. Milrinone can decrease afterload and improve contractility, both of which can help augment cardiac output. Furthermore, milrinone’s leusotropic properties can help improve ventricular filling, which in the setting of diastolic left heart failure may be of obvious benefit. This may explain the beneficial effect milrinone on survival noted in this study. Previous studies have also demonstrated the beneficial effects of milrinone on systemic oxygen delivery and outcomes, specifically in prevention of low cardiac output syndrome after cardiac surgery. Reference Hoffman, Wernovsky and Atz26
With regards to enteral medications, digoxin and beta-blockers are noted to have a significant association with mortality. Angiotensin converting enzyme inhibitors are noted to be associated with decreased mortality. This may be due to the afterload reduction effects of these agents.
Pulmonary vasodilators are noted to be associated with increased mortality in the current study. This differs from adult studies which demonstrate no change.
With respect to length of stay in survivors, older age and diuretics tended to be associated with decreased length of stay. The association of younger age with increased mortality in paediatric heart failure has been previously described. The association of diuretics with decreased length of stay is likely secondary to symptomatic management and underlying decrease in left ventricular filling pressures associated with diuretics.
While these data are additive to the current literature, specifically for a physiology for which much data do not exist, these data are not without their limitations. First, the definition of paediatric diastolic heart failure is not clearly defined, so its diagnosis and timing likely have physician and institutional variability. Second, the timing of onset of diastolic left heart failure and the comorbidities is not available. Thus, temporal associations cannot be characterised objectively. The temporal associations are discussed elsewhere in this manuscript in the setting of previously published data. Third, the dose and duration of mechanical and pharmacologic interventions cannot be characterised. Thus, dose-dependent effects of medications are not able to be characterised. Fourth, comorbidities are captured by coding. How specific comorbidities are defined may differ at the physician and institution levels. Thus, what one individual or institution defines as acute kidney injury or liver failure, for instance, may be different. Fifth, laboratory data such as N-terminal-pro-brain-natriuretic peptide and serum creatinine are not available in the database. Sixth, imaging data are also not available in the database. Specifically, with respect to the specific aims of this study, echocardiographic data such as tissue Doppler around the mitral valve, mitral valve inflow Doppler, or pulmonary venous Doppler data to characterise left heart diastolic function are not available. Seventh, as with any data that are sourced from multiple centres, individual and institutional-level variability is present. Eight, the overall frequency of use of the combined angiotensin receptor blocker and neprolysin inhibitor combination was too low to allow for regression analysis. Finally, these findings are representative of the average in this cohort, conclusions cannot be drawn for outlying subsets.
To overcome the issue of severity of illness which is exacerbated by the lack of laboratory, haemodynamic, and imaging data this study used various comorbidities that are associated with severity of illness. Examples of this include acute kidney injury, liver failure, and respiratory failure. It is well demonstrated that the number of impacted organ systems correlates well with severity of illness and mortality in critically ill children. Medications also serve as a surrogate marker, specifically vasoactive medications. The vasoinotrope score is based on this very principle and is demonstrated to correlate with severity of illness and mortality. Being able to include a large number of comorbidities and pharmacologic agents in the regression analyses allows for an indirect adjustment for severity of illness. To overcome the issue of institutional variability in clinical practice, centre was entered as an independent variable into the regression analyses to adjust for some of the institutional-level variability.
It must also be noted that the data are specific to outcomes of inpatient admissions. Chronic effects, outpatient symptom effects, and readmission effects cannot be assessed by these data.
On the most general level with regard to any inpatient admission the most general goal is survival. More specific goals for inpatient admissions then become minimising morbidity to maximise quality of life, minimising length of stay for survivors, and optimising systemic and regional oxygen delivery. The nature of the database allowed for modelling survival and length of stay. More granular analyses were not possible from this database. Nonetheless, these data offer objective insight into inpatient management of this unique patient population. These data can be used to help guide acute clinical management in an ICU setting but, more importantly, can be used as pilot data to help with design of future studies.
Conclusion
In the cohort studied, isolated diastolic left heart failure has a 5% mortality. Several comorbidities and interventions are associated with increased mortality with milrinone and angiotensin converting enzyme inhibitors being associated with decreased risk of mortality. When only admissions with survival to discharge are considered, older age and diuretics are associated with lower total hospital length of stay.
Availability of data and material
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgements
None.
Financial support
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Ethical standard
These analyses did not require institutional review board approval as they used previously published data that were deidentified. These analyses are in compliance with the Helsinki Declaration of 1975 and its subsequent revisions.






