



A 10-day-old neonate was referred to us for evaluation of cyanosis. An echocardiogram revealed an obstructed supra-cardiac totally anomalous pulmonary venous connection. We obtained a computed tomographic angiogram pre-operatively to define the pulmonary venous anatomy. The angiogram showed that all four pulmonary veins formed a confluence behind the left atrium which drained into the brachiocephalic vein through an ascending vertical vein. The vertical vein, however, was distant from the left bronchus. It was compressed by a vise formed between the left pulmonary artery and the arterial duct (Fig. 1a, b).
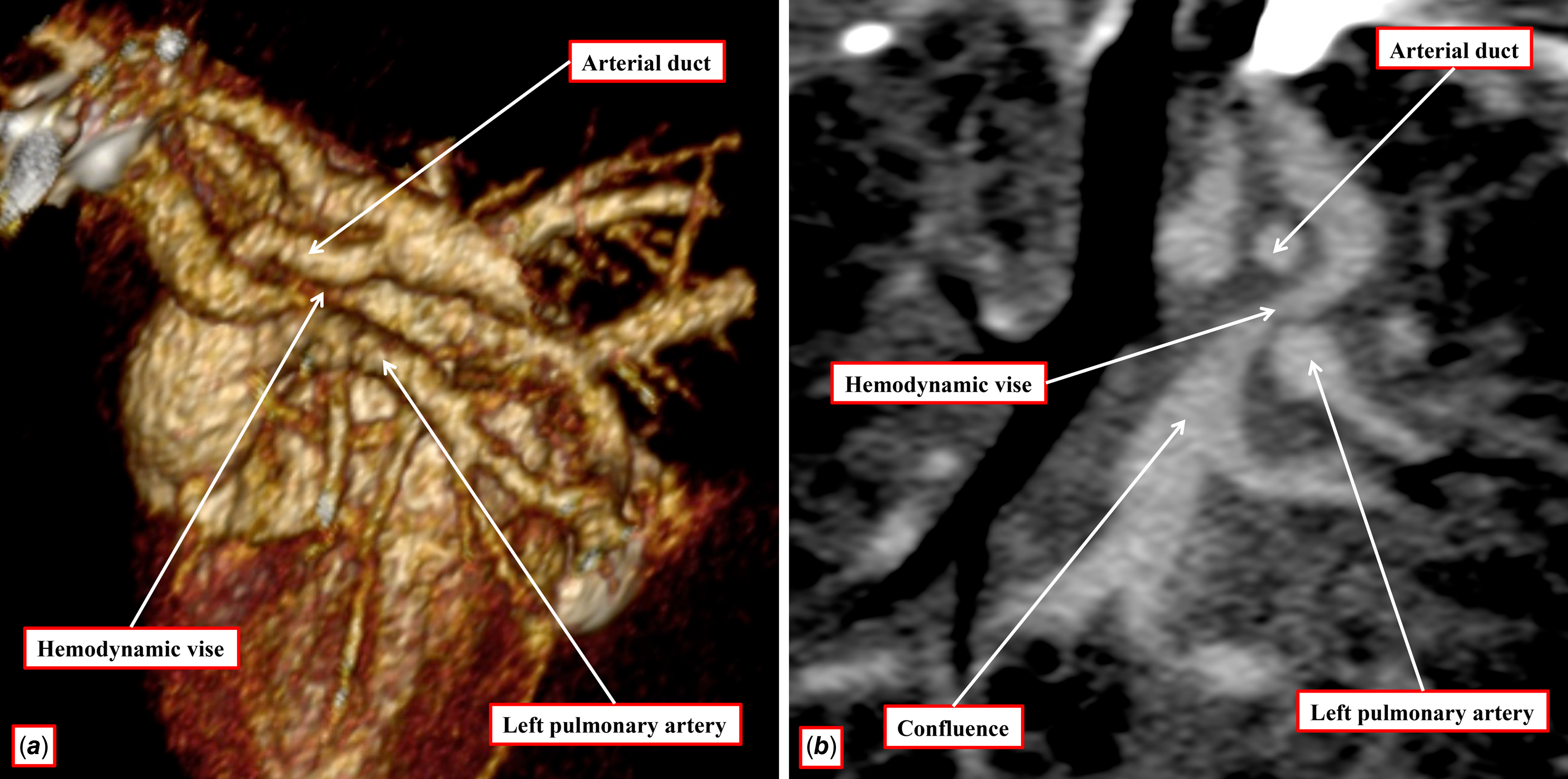
Figure 1. a. Three dimensional volume rendered image of the computerized tomogram image in a left oblique projection demonstrating the site of compression (star) between the left pulmonary artery and the arterial duct. b. Reconstructed computerized tomogram (CT) image in the coronal plane demonstrating the compression (arrow) of the vertical vein between the left pulmonary artery and the arterial duct.
Comment
Totally anomalous pulmonary venous connections according to the site of drainage are classified into supracardiac, cardiac, infracardiac, and mixed variants. More pertinent to clinical management is the obstructed as opposed to unobstructed nature of the drainage. Whilst the infracardiac variant is almost always obstructed subsequent to closure of the venous duct, the supracardiac variant is often unobstructed, since the ascending vertical vein usually traverses the mediastinum anterior to the vascular structures. Obstruction, when present, is usually the consequence of passage of the vertical vein between the left pulmonary artery and the left main bronchus – the so-called “haemodynamic vise.” In our case, the vertical vein was anterior to the left pulmonary artery, but was compressed by a persistent arterial duct. To the best of our knowledge, such an occurrence has been described previously but once. Reference Muneuchi, Takenaka, Ochiai and Joo1 These variants are pertinent to the developmental origin of the vertical vein. In the past, the vein has been interpreted by some as a remnant of the left superior caval vein. Such a channel, however, would not be found between the left pulmonary artery and the arterial duct. It is much more plausible to interpret the vessels as representing pulmonary-to-systemic collateral channels. This case also illustrates the utility of cross-sectional imaging in recognising unusual anatomical features in CHDs as these variations cannot be identified by echocardiogram alone.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Financial support
None.
Competing interests
None.

