


CASE STUDY
A 94-year-old woman with a history of advanced dementia presented to the emergency department (ED) from her nursing home with a urinary tract infection (UTI) and abdominal pain. On presentation, her vital signs were normal, but mild abdominal distention was found and she vomited once. Her past medical history was also significant for hiatal hernia, bilateral hip fractures five years prior, permanent urinary catheter, and recurrent UTIs. She was on no medications. Although the referral letter said she was being fed by percutaneous endoscopic gastrostomy (PEG) tube, the ED team noted immediately that no tube could be found. Plain flat x-ray revealed partial small bowel obstruction, but the tube could not be visualized. An urgent CT was ordered which identified the inflated balloon and indicating its position in the terminal ileum (Figure 1). The patient was admitted. A percutaneous needle puncture of the balloon failed. Laparotomy was refused by the patient’s substitute decision-maker. She died a few days later.
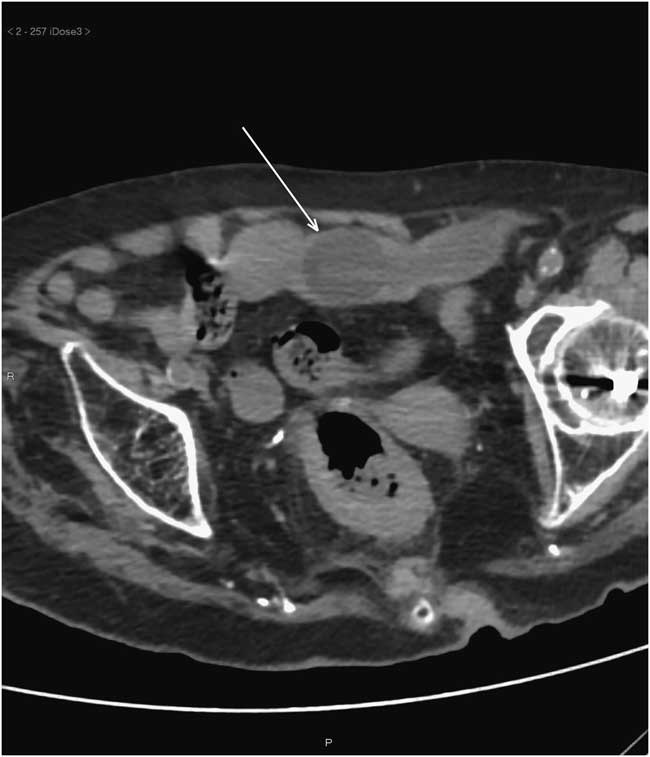
Figure 1 Single axial image of abdominal CT scan without contrast demonstrating an inflated Foley catheter (arrow) lodged in the terminal ileum. Proximal to it, moderate bowel loop dilatation was present (not shown).
DISCUSSION
PEG is being increasingly used to provide nutrition and fluid balance in patients who cannot eat or refuse to eat, although it has not been shown to prolong survival in elderly patients with advanced dementia.Reference Teno, Gozalo and Mitchell 1 , Reference Mendiratta, Tilford and Prodhan 2 Late complications include local infections, aspiration pneumonia, and tube dislodgement with sliding either out of (common) or into (rare) the gastrointestinal tract.Reference Rahnemai, Rahnemaiazar and Naghshizadian 3 When the external bolster moves inward, migration of the tube to the pyloric area can cause gastric outlet obstruction,Reference Rahnemai, Rahnemaiazar and Naghshizadian 3 but migration into the small bowel or transverse colon has also been reported with life-threatening obstruction or fistula formation.Reference Waxman, al-Kawas and Bass 4 Since gastrostomy tubes are expensive, their replacement by a Foley catheter when expelled or malfunctioning has become prevalent.Reference Kadakia, Cassaday and Shaffer 5 We found no relevant statistics, but a current review of published literature (PubMed since inception, using “foley catheter” AND gastrostomy) revealed 38 publications in the English language which indicate that Foley catheters were being used worldwide as temporary gastrostomy tubes and that their use for prolonged periods (median 15 months) was acceptable and cost-effective.Reference Metussin, Sia and Bakar 6 Short-term trials of Foley catheters have yielded safety data comparable to commercial gastrostomy tubesReference Kadakia, Cassaday and Shaffer 5 , but our patient case is a reminder of the ease of a catheter being “swallowed” unless properly cared for and fixated, and the need for emergency physicians to be aware of these potential complications which may not be apparent on presentation and to also consider “wandering” tube in the differential diagnosis of obstruction or ileus in the elderly.
Acknowledgements
Patient consent was signed by guardian. All authors treated the patient and participated in preparing the manuscript.
Competing Interests: None identified.

