



Worldwide, both the proportion and the absolute number of older adults are increasing rapidly. It is estimated that the population aged ≥ 60 years will grow from 10 % of the total population in 2021 to nearly 17 % by 2050(1,Reference He, Goodkind and Kowal2) . This demographic shift necessitates proactive measures to boost healthy ageing, defined by the WHO as ‘the process of developing and maintaining the functional ability that enables wellbeing in older age’(3). Lifestyle behaviours, including a healthy diet (e.g. healthy snacks), are particularly important in pursuing the challenge of healthy ageing(Reference Black and Bowman4). Existing literature shows a clear link between snacking behaviour and health status in older adults, which can yield positive and negative health effects(Reference Volkert5–Reference Skoczek-Rubinska and Bajerska8). Negative effects are linked to a disturbed energy and nutrient balance. The consumption of energy-dense snacks can contribute to higher energy intake and subsequent weight gain(Reference Skoczek-Rubinska and Bajerska8). Still, this does not mean that snacking automatically leads to weight gain as this depends on various factors, including frequency, portion size and type of snack. It is important to note, however, that depending on nutritional requirements, what is considered healthy for some older adults, is not necessarily healthy for all older adults. It has been shown, for example, that the risk of malnutrition, an inadequate intake of energy and nutrients, is higher in older adults compared with other age groups(Reference Volkert5). Reduced appetite is often reported as one of the main factors that lead to a reduction in energy or nutrient intake(Reference Volkert5). Therefore, specifically in older adults suffering from malnutrition, consuming energy-dense snacks between meals may be an effective way to increase energy intake and improve nutritional status(Reference Zizza, Tayie and Lino6). On the contrary, a potential positive effect of snacking is related to sarcopenia (i.e. progressive loss of skeletal muscle mass and strength)(Reference Marzetti, Calvani and Tosato9). Snacks containing protein help both in preventing and treating sarcopenia and are therefore not only beneficial for malnourished individuals but for all older adults, despite their satiating effect and the risk of reducing intake at the next meal(Reference Nazri, Vanoh and Soo10). Malnutrition is, however, beyond the scope of this paper and will not be discussed further in detail. Altogether, it is clear that snacking can have both positive and negative consequences on the health of older adults, making it an important health behaviour to investigate further.
The phenomenon of snacking gradually made its way into daily eating patterns over the past decades, particularly in high-income countries(Reference Mena, Ashman and Dunshea7). In the present paper, snacking is defined as an eating moment that falls outside of the three main meals (i.e. breakfast, lunch and dinner)(Reference de Graaf11). Only solid foods, but not beverages, were assessed to reduce confusion surrounding snack definitions(Reference Johnson and Anderson12) and to reduce participant burden(Reference Yao, Yang and Wang13). Studies on snacking among older adults reveal diverse prevalence numbers, with variations in the energy contribution of snacks to total daily intake ranging across European countries from 6 % in France to 32 % in The Netherlands(Reference Schlettwein-Gsell, Decarli and De Groot14). Several studies concluded that older adults have steeper peaks in energy intake during the main meals compared with young adults(Reference Vatanparast, Islam and Masoodi15,Reference Andersson, Nydahl and Gustafsson16) . The proportion of older adults who consumed at least one snack per day ranged from 77 to 84 %, which is significantly higher compared with other age groups(Reference Mena, Ashman and Dunshea7,Reference Vatanparast, Islam and Masoodi15,Reference Higgins17) .
To achieve a comprehensive understanding of snacking behaviour in older adults, it is important to identify the underlying factors. The present study identifies these determinants by using a socio-ecological model as the guiding theoretical framework(Reference Meltzer, Brantsaeter and Trolle18). This model categorises factors affecting food intake into three levels: macro- (policies), meso- (community settings) and micro-level (inter- and intrapersonal factors). The present study focuses on determinants at the meso- (i.e. visibility of snacks(Reference Elliston, Ferguson and Schuz19,Reference Elliston, Ferguson and Schuz20) ) and micro-level (i.e. emotions(Reference Reichenberger, Kuppens and Liedlgruber21,Reference Eskelinen, Hartikainen and Nykanen22) , intention(Reference Glanz, Rimer and Viswanath23) and social modelling(Reference Elliston, Ferguson and Schuz19,Reference Hess, Jonnalagadda and Slavin24) ). A considerable amount of literature has been published on the drivers of eating behaviour and some are briefly outlined here. First, literature on the influence of emotions is ambiguous. Previous research has demonstrated that negative emotions negatively affect dietary intake (e.g. among older adults, feelings of loneliness have been linked to malnutrition)(Reference Eskelinen, Hartikainen and Nykanen22). In the context of diet quality, a study in older adults showed that mood was not an important barrier or motivator in making food choices(Reference Locher, Ritchie and Roth25). Conversely, other studies found that positive affect was associated with healthier dietary patterns, while negative affect was not significantly related to dietary quality(Reference Whitehead26,Reference Walker-Clarke, Walasek and Meyer27) . The paradox of emotional well-being in ageing suggests that older adults often maintain or even improve their emotional well-being despite physical and mental decline(Reference Mather28,Reference Charles29) . This phenomenon is attributed to older adults’ superior emotional regulation skills compared with younger adults(Reference Carstensen, Pasupathi and Mayr30,Reference Hay and Diehl31) . With this in mind, more research is needed to clarify the role of emotions in dietary behaviour among older adults. Second, according to the socio-ecological model, someone’s intention is an important determinant of behaviour. Nonetheless, high levels of intention to eat healthy will not automatically lead to actual healthy eating behaviour. Thus, someone’s intention does play a role, but can be influenced by, for example, environmental cues (e.g. seeing others eat or having snacks available)(Reference Elliston, Ferguson and Schuz19). Lastly, Elliston et al. found that observing others eat increased the likelihood of eating because being exposed to food increases subjective experiences of desire to eat(Reference Elliston, Ferguson and Schuz19,Reference Elliston, Ferguson and Schuz20) . However, older adults exhibit more habitual behaviours and eating patterns, possibly making them less susceptible to social modelling compared with younger adults(Reference Cruwys, Bevelander and Hermans32). Differences in motives for the consumption of regular meals (i.e. breakfast, lunch and dinner) compared with motives for snack consumption can be identified(Reference Hess, Jonnalagadda and Slavin24,Reference Cleobury and Tapper33–Reference de Gooijer, van Kraaij and Fabius36) . On the one hand, individuals commonly attribute eating motives such as habit and hunger to regular meals(Reference Cleobury and Tapper33). On the other hand, for snack consumption, emotional and external motives (e.g. visual and aromatic food cues) are reported more frequently(Reference Cleobury and Tapper33,Reference Verhoeven, Adriaanse and de Vet35) . Nevertheless, to our knowledge, there is a notable dearth of studies examining the association between these determinants and snacking behaviour, particularly among older adults.
Previous studies on snacking have typically relied on traditional assessment methods (e.g. dietary recall), but these methods have several limitations including low compliance rates, under-reporting of events(Reference Berkman, Giuliani and Pruitt37) or backfilling of past events(Reference Stone, Shiffman and Schwartz38). Moreover, these methods usually assess determinants only once and at the start of the study, while in reality determinants may vary throughout the day(Reference Maes, Mertens and Poppe39). To address these limitations, ecological momentary zssessment (EMA) emerges as a promising solution, with previous studies already confirming that it is a feasible method to examine eating behaviour in older adults(Reference Yao, Yang and Wang13,Reference Spanakis, Weiss and Boh40) . EMA enables the assessments of determinants in real-life situations at multiple moments throughout the day and maximises ecological validity and minimises recall bias(Reference Maugeri and Barchitta41). These repeated assessments are necessary to reveal underlying dynamic behavioural processes(Reference Spanakis, Weiss and Boh40) and offer useful information to develop personalised or just-in-time adaptive interventions, which aim to provide the right type and intensity of support to individuals at the right time(Reference Nahum-Shani, Hekler and Spruijt-Metz42). For example, suggestions to eat a healthy snack can be adjusted to the emotional ‘state’ of the individual, i.e. when the individual is more prone to engage in unhealthy snacking.
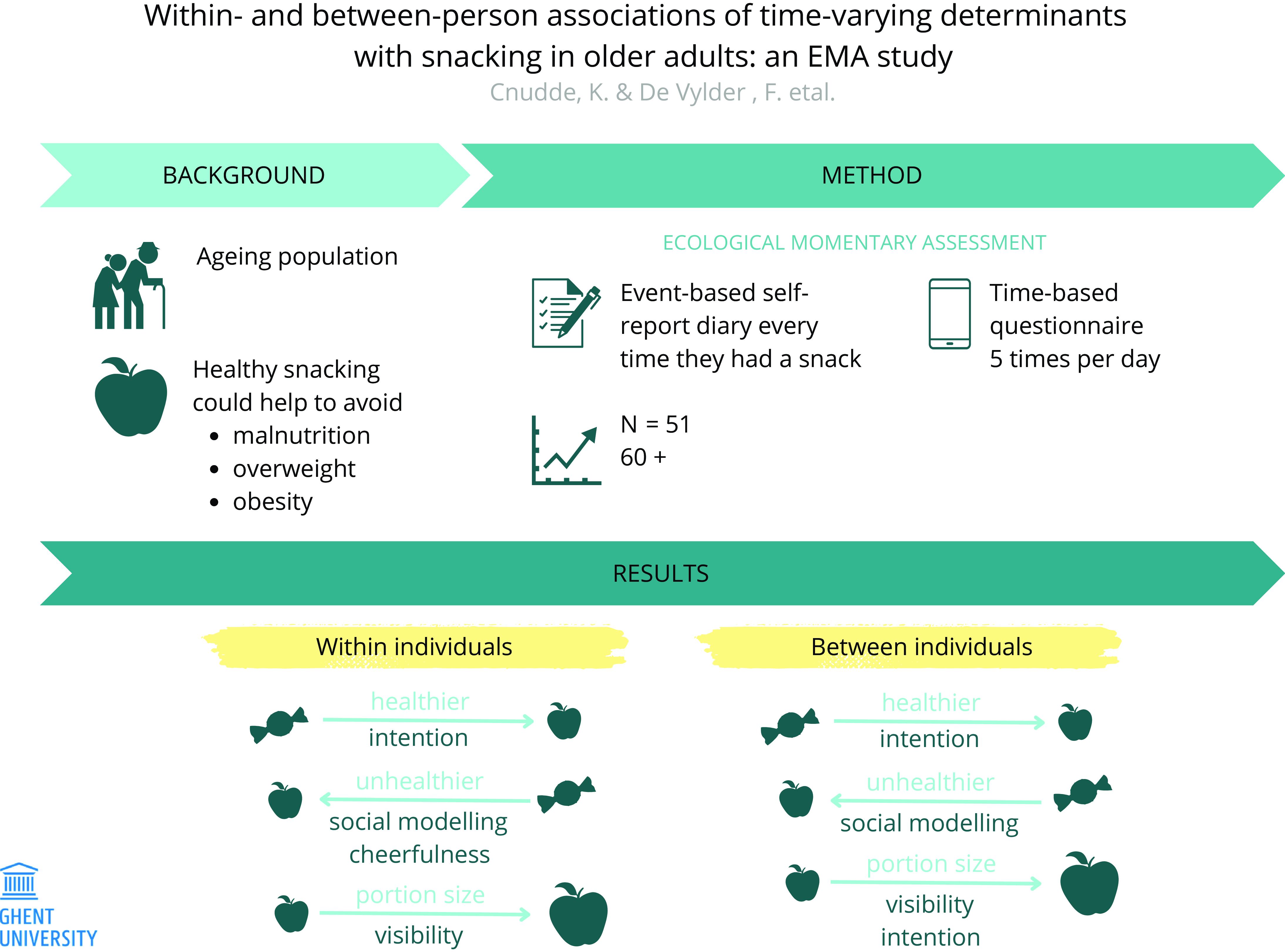
The purpose of the current study was to investigate within- and between-person associations of various determinants at the meso- and micro level of the socio-ecological model and snacking behaviours (i.e. decision to snack, health factor of the snack and portion size) in older adults. The uniqueness of this paper lies mainly in the repeated-measures design throughout the day, which allows to draw conclusions about both between- and within-person associations. Because there has been little research conducted on the determinants of snacking within persons, especially in older adults and with repeated assessments within days, this study is primarily exploratory in nature.
Methods
Procedure and participants
Fifty-one healthy older adults, aged 60 or above, were recruited for this prospective observational study with an intensive longitudinal design. Participants were recruited through convenience and snowball sampling in the personal network of the researchers and via community associations for older adults. Inclusion criteria were (1) no impaired cognition (i.e. diagnosis of dementia; Alzheimer or other cognitive diseases), (2) living at home independently, (3) no impairment of fine motor skills (i.e. being able to complete data collection with a smartphone), (4) no severe impairment of vision and/or hearing (i.e. being able to hear the triggers for the EMA questions and read the questions on the smartphone) and (5) be Dutch-speaking. During the initial contact via email, the inclusion criteria were discussed with the participant. Data were collected between August and November 2021. This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects were approved by the Ghent University Hospital Ethics Committee (registration number B6702021000698). Written informed consent was obtained from all subjects.
During a first home visit, all participants completed a baseline questionnaire on socio-demographic variables. Thereafter, face-to-face instructions for the measurement period were given and participants received a short introduction on how to use the smartphone-based EMA application, supported by a user manual (online Supplementary file 1). They were encouraged to use their own smartphone (the lowest operating systems used were Android 5.0 and iOS 12.4), but if this was impossible a smartphone (Motorola Moto G20 64GB, Android 6·0) was provided by the researchers. The first home visit was followed by a measurement period of seven consecutive days (i.e. 5 weekdays and 2 weekend days), during which the participants answered a combination of time-based and event-based EMA questionnaires. Data collection started on a randomly selected day during the week, with this starting day varying between participants. Afterwards, all measurement instruments were collected during a second home visit and a short follow-up interview took place. The study design is presented in Fig. 1.

Fig. 1. Example of the study design.
Questionnaires
Baseline
Participants self-reported the socio-demographic variables age, gender, height, weight, educational level, main occupation (before retirement) and marital status. Waist circumference was measured by the researchers using a tape measure.
Event-based ecological momentary assessment
Participants were asked to keep a paper-based snack diary, where they self-reported specific information every time they consumed a snack (i.e. decision to snack). A snack was defined as a solid food that was consumed outside of the three main meals (i.e. breakfast, lunch and dinner)(Reference de Graaf11). For every snack, participants reported time, the type of snack, portion size (in grams, household measures (e.g. a teaspoon) or by using a food model booklet(Reference Peersman43)), visibility of the snack and social modelling. Visibility was queried with the item ‘Was the snack visible when you decided to snack?’ (Reference Elliston, Ferguson and Schuz20). Participants were instructed to answer (Yes) if the snack was visible in their immediate environment. They were instructed to answer (No) if the snack was available but not visible or if they bought the snack at the store. Social modelling was questioned with the item ‘While eating your snack, could you see someone else eating in your surroundings?’ (Yes, No)(Reference Elliston, Ferguson and Schuz19).
Thereafter, the UK Nutrient Profiling Model was used by the researchers to calculate a health factor and divide the types of snacks into two categories (i.e. healthy and less healthy)(44). The scoring system uses a formula taking into account energy content (kJ/100 g), saturated fat (g/100 g), sugar (g/100 g), salt (mg/100 g), fruit-vegetables-nuts (%), fibre (g/100 g) and protein (g/100 g) to classify a snack as ‘healthy’ (< 4) or ‘less healthy’ (> 4). The Dutch Food Composition Database (NEVO online version 2021/7.1) was used to analyse the nutrients of the foods mentioned in the snack diary. When portion sizes were not recorded in weight units, they were converted into grams through the utilisation of the Belgian manual for standardised quantification of food(45).
Time-based ecological momentary assessment
Prior studies have indicated that a minimum of five daily assessments is necessary to effectively record the dynamic fluctuations of determinants linked to health behaviours within individuals(Reference Degroote, Van Dyck and De Bourdeaudhuij46,Reference Liao, Skelton and Dunton47) . Therefore, participants received auditory signals on their smartphone five times per day for seven consecutive days, alerting them to fill in a questionnaire using the Smartphone Ecological Momentary Assessment3 application (i.e. the participants were asked to answer the questionnaire thirty-five times in total)(Reference O’Brien, Dozo and Hinton48). Smartphone Ecological Momentary Assessment3 randomly selected a triggering time within 2-hour intervals, being: 09.30–11.30, 13.30–15.30, 16.00–18.00, 18.30–20.30 and 21.00–23.00. The timeframes were chosen based on previous research looking at prevalence of snacking in older adults throughout the day(Reference Vatanparast, Islam and Masoodi15). The minimum interval between two successive signals was 30 min. If participants did not immediately respond to the signal, they received up to two reminders. If the questionnaire was still unanswered after 30 min, the questionnaire became inaccessible. The assessment time used in further analysis was the time point at which the questionnaire was completed. In the time-based EMA questionnaire, intention for healthy snacking and emotions were assessed. Intention for healthy snacking was assessed by the item ‘If I eat a snack in the next 2 h, I want to choose a healthy snack’ and answers ranged from (strongly disagree) to (strongly agree) on a seven-point Likert scale(Reference Dunton49). Whether or not a snack was seen as (un)healthy was based on the subjective opinion of the participant. Five negative emotions (i.e. loneliness, insecurity, anxiousness, irritation and feeling down) and four positive emotions (i.e. cheerfulness, relaxation, enthusiasm and satisfaction) were selected from a list of items that are frequently used for EMA by the Department of Psychiatry and Neuropsychology at the University of Maastricht(Reference Delespaul50). These nine emotions were captured on a seven-point Likert scale in a similar way. An example of an item is ‘How lonely were you just before you received the trigger?’ with answers ranging from (not at all lonely) to (very lonely).
Statistical analyses
The data were analysed using R version 4.2.3(51). To investigate the effect of the determinants on participants’ snacking behaviour, the time-based and event-based datasets were combined. If a snack was consumed in the subsequent 2 h following the time-based EMA trigger, all corresponding details from the snack diary were associated with the respective time-based EMA trigger. In case multiple time-based EMA triggers preceded a snack, the trigger closest to the eating moment was chosen. If multiple snacking moments (i.e. event-based EMA) could be associated with one trigger, both were linked to the same time-based EMA information. The determinants visibility and social modelling were not included in the analyses for the dependent variable ‘decision to snack’, since they were only assessed if people actually snacked. The determinant health factor was rescored to a positive number by adding ten units to each value to allow further analysis to be interpreted more easily. To take the clustering of the data within participants into account, (generalised) linear mixed models (two-level models, triggers within individuals), as implemented in the package lme4 version 1.1–34, were used to analyse the data(Reference Bates, Maechler and Bolker52). The percentage of between- and within-subject variance of the determinants was calculated by running intercept-only models (i.e. models only including a fixed and random intercept) with each of the determinants as outcome variables. To examine the effect of the determinants on participants’ snacking behaviour (outcome variables: decision to snack, health factor and portion size), different models were fitted with the determinants as between-subject (i.e. mean of the variable at the subject level) as well as within-subject (i.e. individuals’ score at the time of the trigger minus their mean score) variables. For the outcome variable decision to snack (yes; no), logistic regression models were used. Two models (i.e. a random intercept-fixed slope model and a random intercept-random slope model) were fitted for each determinant separately, which led to twenty-four models in total (i.e. twelve determinants × two models). Of those two models per determinant, the model with the lowest Akaike’s information criterion value indicating a better model fit was chosen. For the outcome variables health factor and portion size, three different generalised linear models (i.e. Gaussian with identity, Gamma with identity and Gamma with log) and both a random intercept-fixed slope model and random intercept-random slope model were tested for each determinant separately. To check which model fitted the data best, the Akaike’s information criterion value was defined. To standardise the analyses, one model was chosen per outcome variable, since the Akaike’s information criterion values across models were very similar. The random intercept-fixed slope model with gamma variance and identity function was applied in all analyses for the outcome variable health factor and the random intercept-fixed slope model with γ variance and log function was used for portion size. Model assumptions were visually checked (i.e. normality of the residuals, homoscedasticity, outliers and influential observations). Statistical significance was determined at P < 0·05.
Power analysis
Since this is an exploratory study, the sample size was determined aiming to avoid overfitting (i.e. a model becomes more complicated than necessary and is modelling spurious relationships) instead of obtaining the desired power. In general, for linear and logistic regression models, a minimum of ten observations per predictor allows good estimates(Reference Babyak53,Reference Peduzzi, Concato and Kemper54) . Because univariable models were used in the current study, leading to only one degree of freedom per model, we set a minimum of ten participants for the models with continuous outcome variables. Previous studies report snacking prevalence ranging from 77 to 84 % in older adults(Reference Higgins17,Reference Vatanparast, Islam and Patil55) . Therefore, in the models with a binary outcome measure, assuming that 80 % of the participants consume snacks, ten participants account for the 20 % in the smallest group who do not snack on a daily basis. Added together with forty participants who do snack (10/0·2 × 0·8), this results in a minimum of fifty participants to be recruited. However, the above reasoning has an important limitation. In EMA studies, the collected data are not independent but hierarchical (two-level models, triggers within individuals). Neglecting the clustering when modelling data frequently leads to underestimated standard error estimates, especially when the outcome variable shows dependence based on the clustering of data. The impact of the number of clusters on model estimates is moderated by the sample size within these clusters. Although a specific sample size to ensure unbiased estimates cannot be pinpointed, prior research recommends a minimum of thirty participants (representing the number of clusters) with thirty observations per participant, assuming equal sample sizes within each cluster(Reference McNeish and Stapleton56). A review found that the compliance rate for EMA studies in European older adults was on average 86·19 %(Reference Yao, Yang and Wang13), which confirms the feasibility of this method for data collection among older adults. Therefore, presuming a compliance rate of 86 % for older adults in EMA studies, we aimed to include a minimum of fifty participants to which each a total of thirty-five (30/0·86 × 1) triggers were sent.
Results
Descriptive statistics
In total, fifty-one older adults completed the measurements for a period of seven consecutive days. Based on the time-based assessments, three individuals had an overall response rate lower than 33 % (i.e. < 12 of 35 triggers) on the EMA questionnaire and were excluded from further analyses, in line with methodology used in other research(Reference Maes, Mertens and Poppe39,Reference Myin-Germeys and Kuppens57) . In a follow-up interview, these drop-out participants reported difficulties with the use of the smartphone or indicated to be unable to answer signals during working hours. Ultimately, forty-eight participants were included in the analyses (smartphone ownership: 91·7 %). The characteristics of the study population are presented in Table 1.
Table 1. Descriptive characteristics of the participants

M, mean; Min, minimum; Max, maximum.
* Self-employed, worker.
† Employee, education, executives, free professions and officer.
Throughout the study, a total of 1680 time-based EMA triggers were sent. Of these triggers, 475 were not answered and six contained missing information, which led to their exclusion from the analysis. Eventually, 1199 triggers were completed (overall response rate = 71·4 %; mean of 23·9 completed questionnaires per participant) and were included for analysis of the dependent variable decision to snack. In 35·0 % of the moments where a time-based EMA questionnaire was triggered, participants reported a snack moment (event-based EMA) in the subsequent 2 h following the trigger. Out of the 761 snacking moments recorded in the snack diaries, 420 could be matched with a time-based EMA trigger and were included for further analysis of the dependent variables health factor and portion size. Table 2 contains the descriptive statistics pertaining to the snack diary. Online Supplementary file 2 provides more detailed information about the snack frequency per participant individually.
Table 2. Descriptive statistics of the snack diary

M, mean. sd, standard deviation. Min, minimum. Max, maximum.
* (e.g. cheese, bread, charcuterie, vegetables …).
† Health factor < 4.
Table 3 displays the mean scores, the between-subject variance and the within-subject variance between days and within days of the time-based determinants. For the determinants intention, loneliness, relaxation, enthusiasm, anxiousness and feeling down, the between-subject variance (i.e. ranging from 48·6 % to 66·3 %) is higher than the within-subject variance within days (i.e. ranging from 31·1 % to 48·0 %). The opposite is true for the determinants cheerfulness, satisfaction, insecurity and irritation (i.e. the between-subject variance ranges from 30·4 % to 47·7 % and the within-subject variance within days ranges from 47·9 % to 64·4 %). Within-subject variance between days explained only 1·5 % to 14·6 % of the variance, indicating that the variation of the examined determinants within persons, but between days, was limited. Online Supplementary file 3 provides the individual scores on the determinants over the measurement period. This way, an overview of the extent to which the determinants fluctuate is given.
Table 3. Mean scores, between subject variance, within-subject variance (between days – within days)

M, mean; Min, minimum; Max, maximum.
Within- and between-person associations with the decision to snack
Table 4 shows the results for the logistic regression models of the determinants related to the decision to snack (yes/no). No significant within- or between-person associations were found between the determinants and the decision whether or not to snack within 2 hours after the trigger.
Table 4. Within- and between-person associations between different possible determinants of snacking with the decision to snack, health factor and portion size

ExpB, exponentiated estimate (representing a proportional difference in portion size).
Significant results (P < 0·05) are highlighted in bold.
Within- and between-person associations with health factor
Table 4 provides the results for the models with γ variance and identity function of the determinants related to the health factor of the snack. A significant within-person association was found for intention to eat a healthy snack (P < 0·01), social modelling (P < 0·01) and cheerfulness (P = 0·04). If a person’s intention to eat a healthy snack is one unit higher than his own average intention level, the health factor score is associated with a decrease of 2·53 units (= healthier snack). If a person sees someone eating in their environment compared with when they do not see someone eating in their environment, the health factor is associated with an increase of 6·57 units (= unhealthier snack). If a person scores one unit higher on cheerfulness than his own average cheerfulness level, the health factor is associated with an increase of 2·14 units (= unhealthier snack). A significant between-person association was found for intention (P < 0·01). Per one-unit increase in intention to eat a healthy snack, the health factor is associated with a decrease of 2·81 units (= healthier snack). No significant associations were found for the other determinants.
Within- and between-person associations with portion size
Table 4 also provides the results for the models with γ variance and log function of the determinants related to the portion size of the snack. A significant within-person association was found for visibility (P < 0·01) and significant between-person associations were found for intention (P = 0·03) and visibility (P < 0·01). If a snack is visible to the person compared with when the snack is not visible for that same person, the portion size of the snack is associated with an increase of 3 %. Per one-unit increase in intention, the portion size is associated with an increase of 15 %. If a snack is visible compared with when it is not visible, the portion size is associated with an increase of 35 %. No other significant associations were found.
Discussion
This study examined the within- and between-person associations of multiple determinants on snacking behaviours (i.e. decision to snack, health factor and portion size). At the intra-individual (within-person) level, intention to eat a healthy snack was negatively associated with health factor (= healthier snack), social modelling and cheerfulness were positively associated with health factor (= unhealthier snack), and visibility was positively linked with portion size. Furthermore, at the inter-individual (between-person) level, intention to eat a healthy snack was negatively associated with health factor (= healthier snack), and intention to eat a healthy snack and visibility were positively linked with portion size. However, the other determinants (i.e. loneliness, relaxation, enthusiasm, satisfaction, insecurity, anxiousness, irritation, feeling down) were not related to health factor and portion size, nor at the within-person, nor the between-person level. Strikingly, none of the included determinants were related to the decision of whether or not to eat a snack at the within- or between-person level. To our knowledge, this is the first study focusing on within-person associations of specific determinants with snacking in an older age group, so most findings can only be compared with between-person associations examined in other studies.
The intention to eat a healthy snack leads to actually eating a healthier snack and this applies to both the within- and between-person level. To put it another way, both an increase in intention within a subject (i.e. a higher intention level than his own average level) and differences in intention between subjects (i.e. subjects with higher intention levels v. subjects with lower intention levels) are linked to health factor. These findings align with the theory of plannedb and socio-ecological models, in which intention serves as a significant predictor of behaviour(Reference Glanz, Rimer and Viswanath23,Reference Mcleroy, Bibeau and Steckler58) . This is also supported by Inauen et al., who were the first to examine the relationship between intention and snacking behaviour while disentangling the within- and between-person level(Reference Inauen, Shrout and Bolger59). They found strong intention–behaviour associations at the within-person level, aligning with the assumptions of many health behaviour theories(Reference Ajzen60,Reference Schwarzer61) . Besides, no significant intention–behaviour relations were found at the between-person level, supporting previous findings of an intention–behaviour gap(Reference Elliston, Ferguson and Schuz19,Reference Rhodes and Dickau62,Reference Webb and Sheeran63) . The contradiction in literature may be attributed to the methodology and analysis employed because intention was mostly assessed only once at baseline.
In the current study, observing someone else eating was associated with a less healthy snack choice at both the within- and between-person level, indicating that seeing other people eat plays an important role in the snack behaviour in older adults. In other words, the association is not only present at a group level (i.e. across individuals in the study) but also at an individual level (i.e. within one participant). Other research suggests that observing someone else eating has a greater impact on the consumption of unhealthy snacks compared with healthy snacks(Reference Cruwys, Bevelander and Hermans32). Both in previous studies and in the current study, the snacking behaviour of the opposing individual remains mostly unknown (e.g. the type of snack they ate), making it difficult to draw definitive conclusions on the mechanisms behind social modelling and the health factor of the snack. In contrast, the results of the current study also show that social modelling was not related to the decision to snack or to portion size. This finding contradicts other research suggesting that observing someone else eating is linked to a higher likelihood of snacking(Reference Elliston, Ferguson and Schuz19,Reference Elliston, Ferguson and Schuz20,Reference Hess, Jonnalagadda and Slavin24) . This is noteworthy, as social modelling is a well-established determinant, which is demonstrated in research involving numerous demographic groups(Reference Herman, Koenig-Nobert and Peterson64). A systematic review on psychosocial factors influencing eating behaviours of older adults confirms that solitary eating is consistently negatively associated with the quantity of food consumed(Reference Walker-Clarke, Walasek and Meyer27,Reference Wham and Bowden65) . Furthermore, it is associated with an increased probability of having a lower BMI(Reference Wham and Bowden65–Reference Kimura, Wada and Okumiya67), lower dietary variety(Reference Kimura, Wada and Okumiya67,Reference Schnettler, Lobos and Lapo68) , lower consumption of fruits and vegetables(Reference Tani, Kondo and Takagi66,Reference Schnettler, Lobos and Lapo68,Reference Rugel and Carpiano69) and an elevated tendency to skip meals(Reference Tani, Kondo and Takagi66). It may be possible that the association between observing someone else eating and choosing to eat a snack as well as portion size may be weaker in older adults compared with other age groups, since older adults exhibit more habitual behaviours and eating patterns, making them less susceptible to social modelling(Reference Cruwys, Bevelander and Hermans32). Further research should clarify the specific role of social modelling on older adults’ snacking behaviour. Some considerations can be taken into account: (1) Is the effect size of social modelling different when their eating partner or other surrounding people eat healthy or non-preferred foods compared with unhealthy or preferred foods?, (2) Are habitual snacking patterns responsible for conformity effects between eating companions? and (3) In a scenario in which both co-eaters are free to choose the type or amount of food to consume, which person is modelling and which person is being modelled?
When someone’s feelings of cheerfulness were higher than their own average feelings of cheerfulness, they tended to make less healthy snack choices. Yet, no significant associations with health factor were found for negative emotions. These findings partially align with prior research reporting that older adults did not perceive emotions as important barriers or motivators in making food choices(Reference Locher, Ritchie and Roth25). This suggests that while emotional states may influence dietary behaviours, older adults might not be fully aware of this influence(Reference Walker-Clarke, Walasek and Meyer27). Another study indicated that positive affect was associated with healthier diets, but that negative affect was not significantly related to dietary quality(Reference Whitehead26). Though this seems contradictory to the results of the current study, it is important to note that previous research is based at the between-person level. Contrarily, our findings also differ from previous research. Research on emotional eating in adults, characterised by overeating in response to negative emotions, indicates that negative emotions are associated with weight gain(Reference Barak, Shuval and Li70). On the contrary, a study within older adults demonstrated that negative emotions negatively affect dietary intake, with feelings of loneliness being linked to malnutrition(Reference Hess, Jonnalagadda and Slavin24). The foregoing suggests a nuanced relationship between eating behaviours and emotions across the lifespan, despite no associations being found at the between- or within-subject level with decision to snack or portion size in the current study. Discrepancies could arise from the interchangeable use of the terms ‘mood’ and ‘emotion’(Reference Köster and Mojet71). Emotions and moods have distinct definitions; emotions refer to short-term affective responses to the appraisal of specific stimuli(Reference Frijda72–Reference Rolls74), while moods are more prolonged psychological states that may persist independently of external triggers(Reference Thayer75). Additionally, the discrepancies in findings may also be partially attributed to differences in methodologies employed, with only the present study using EMA to capture emotions at multiple time points. Loneliness, for example, is a longer lasting and more stable mood compared with cheerfulness that tends to be of more intense but short duration, and therefore is more suitable to be queried via EMA.
The results of the current study show that there is both a within-subject and between-subject association between the visibility of the snack and portion size. In other words, if a snack is visible to the person compared with when the snack is not visible for that same person (i.e. within-subject) or if a snack is visible compared with when it is not visible in general (i.e. between-subject), the portion size of the snack increases. These results are in line with previous research, although, only between-subject associations were taken into account in these previous studies(Reference Elliston, Ferguson and Schuz19,Reference Elliston, Ferguson and Schuz20) . It was observed that being exposed to food increased subjective experiences of hunger or desire to eat(Reference Ferriday and Brunstrom76). This finding indicates that the presence of visible food can serve as a stimulus for eating a larger portion of the snack. However these larger portion sizes should only be considered as negative when this is not in line with the nutritional requirements of the individual. With this in mind, future interventions should address visibility in an appropriate way for a specific individual (e.g. eliminating unhealthy snacks from the view of a person who is overweight).
The lack of significant results for the other determinants also deserves attention. There are different possible explanations for the lack of significant results and a distinction must be made between the within-person variance and the between-person variance. On the one hand, the lack of within-person associations detected might be attributed to the limited intra-individual variability of some of the reported determinants within days. Online Supplementary file 3 shows in detail how a determinant fluctuates for each participant individually. The majority of the participants reported limited variation within days for the negative emotions (i.e. loneliness, insecurity, anxiousness, irritation, feeling down). For example, on 62 % (i.e. 211 out of 339) of the total amount of triggers studied, the determinant loneliness did not fluctuate within a participant. Consequently, it is possible that within-person variability in these determinants is not relevant for the subgroup of older adults. On the other hand, the fluctuation of determinants is also rather limited at the between-person level. In the current study, the standard deviation of negative emotions, loneliness, insecurity, anxiousness, irritation and feeling down was overall low (i.e. sd ranged between 0·6 (negative emotions) to 0·9 (irritation)). A slightly higher variation was found for positive emotions, cheerfulness, relaxation, enthusiasm and satisfaction (i.e. sd ranged between 0·8 (positive emotions) to 1·1 (relaxation)), but remained rather limited. Not only the variation of these determinants is quite limited, but also the reported scores were overall low (i.e. the mean score ranged between 1·4 (anxiousness) and 1·6 (irritation) on 7). Consequently, the level of these determinants might have been too low to influence participant’s snacking behaviour. Our findings could be explained in light of the paradox of emotional well-being in ageing(Reference Mather28). With ageing, physical health, strength, cognitive agility and social networks decline. Yet, on average, emotional well-being is somehow maintained or even improved as older adults age(Reference Charles29). This is because older adults excel in regulating their emotions compared with younger adults, enabling them to more effectively diffuse negative feelings and situations(Reference Carstensen, Pasupathi and Mayr30,Reference Hay and Diehl31) . In conclusion, there may potentially be no relationship between the fluctuation in someone’s emotions and snacking behaviour. However, further investigation in a more representative target group is warranted to clarify the findings from the current study and better understand the role of emotions in snack consumption among older adults.
Neither significant within- nor between-subject associations were found for the determinants and the outcome variable decision to snack. This lack of association may be attributed to the tendency of older adults to not base their decision to snack on factors such as emotions, social modelling or the visibility of snacks. Older adults may exhibit more habitual snacking behaviours, making them less susceptible to the influence of determinants(Reference Vatanparast, Islam and Patil55). In addition, eating a snack is not necessarily considered negative, as long as one chooses a healthy snack with an adequate portion size. The question arises if the outcome variable decision to snack may not be suited to interventions that offer support at specific moments (e.g. JITAI).
The present study has several strengths. A first strength is the use of the innovative monitoring strategy EMA. It involves repeated sampling of experiences during people’s everyday lives, which maximises ecological validity and minimises recall bias(Reference Maugeri and Barchitta41). It also allowed us to identify time-dependent as well as context-dependent variations of determinants. More detailed results on the compliance rate in this study are reported elsewhere (Compernolle et al., under review). A second strength is that this study fills an important gap in literature, since studies on snacking behaviour and the determinants are very limited, especially in older adults. This study encompasses a comprehensive assessment of various food items, with both unhealthy and healthy snacks, and their portion sizes. Future studies, however, could delve deeper into the needs of specific groups, such as malnourished, overweight or obese older adults. Lastly, according to our knowledge, this is the first study examining both the within- and between-person associations between snacking behaviour and determinants. The focus on the within-individual processes demonstrates the uniqueness of the paper. This is an important perspective, as not everyone follows the same behaviour (change) processes(Reference Heino, Knittle and Noone77).
However, the study also holds limitations. First, the study results may have limited generalisability due to nonprobability sampling, as this sample may not accurately represent the population of older adults (e.g. a high number of highly educated participants) and may have left out more socially isolated individuals. It is therefore recommended that future studies adopt a more random sampling approach to obtain a more heterogeneous study sample to be able to generalise the study results to a wider population of older adults. Second, a hybrid design was adopted (i.e. utilising both pencil-paper diaries and smartphone-based questions for data collection). However, it is crucial to acknowledge an important disadvantage associated with the use of paper diaries(Reference Myin-Germeys and Kuppens57). Ensuring accurate combination of time- and event-based datasets relies heavily on precise time stamps recorded in the paper diaries. Another concern is the potential occurrence of backfilling, when participants fail to complete the questionnaire at the required times and hastily fill them in before returning to the researchers(Reference Smyth and Stone78,Reference Stone, Broderick and Schwartz79) . This practice could have detrimental consequences for the validity of the data. In light of these limitations, researchers could offer participants the flexibility to choose between paper-and-pencil or smartphone-based methods for event-based diary entries in future research. Moreover, when utilising a smartphone-based approach, there may be merit in developing clear and tailored manuals and training sessions in collaboration with the target population. This may enhance participants’ digital literacy, thereby optimising data collection efficiency and reliability. Third, using a consistent definition of ‘snack’ provides both an advantage and a disadvantage. While it offers a clear delineation of the concept, it excludes food immediately following the main meal and all beverages. For solid foods, valuable information linked to main meals, such as post-meal dessert consumption has been not taken into account. For beverages, the consumption patterns differ from those of solid foods due to unique consumer psychology. For instance, alcoholic drinks enjoyed socially or alone, coffee consumed either away from home or at home are typically not consumed in response to hunger and are not commonly considered snacks(Reference Johnson and Anderson12). In the current study, researchers deemed it important to minimise participant burden and reduce confusion surrounding snack definitions, especially within this vulnerable group where the use of EMA via smartphones was already challenging(Reference Yao, Yang and Wang13). Putting that aside, future research could indeed focus on beverage consumption among older adults as there is still a gap in the literature on this topic. Fourth, in other EMA research, participants reported moderate reactivity in becoming more aware of their eating behaviour during the study (i.e. mean = 54·94 on a scale from 0–100), and low to moderate reactivity regarding the influence of morning assessments on the eating behaviour on the respective days (mean = 27·22 on a scale from 0–100)(Reference Pannicke, Kaiser and Reichenberger80). The question about intention for healthy snacking could have induced the craving for snacks, although we cannot say this with certainty since reactivity was not queried in the current study. Fifth, due to the matching of the time-based and event-based data sets, a number of measurements have been lost, possibly resulting in insufficient power for the outcome variables health factor and portion size. Future research should consider a larger sample size or longer measurement period rather than increasing the number of triggers per day, as the number of snacking moments in a day is limited. Lastly, possible confounding factors, such as preceding eating moments, other emotions, or other unmeasured variables, were not accounted for in this study. Hence, it would be interesting to further examine possible confounding factors in future EMA research.
The insights gained from understanding the determinants can inform future health interventions and can specifically inform decisions regarding which determinants to focus on to promote health behaviours. Based on our findings, it can be suggested that these interventions should focus on the determinants intention and social modelling. Moreover, in the future, more personalised interventions (e.g. JITAI) could be designed to provide appropriate support to participants at the right moments to further enhance their effectiveness in changing behaviour. JITAI could for instance focus on determinants like cheerfulness because these vary the most intra-individually (within-person). Besides, the results for the other determinants (i.e. loneliness, relaxation, enthusiasm, satisfaction, insecurity, anxiousness, irritation and feeling down), showing limited variation over days and within days and a lack of significant associations with snacking behaviour, imply that interventions targeting these determinants might have limited impact. All in all, as this study was primarily exploratory in nature, more research, which addresses a more representative sample size, is required to formulate clearer guidelines for future health interventions.
Conclusions
The present study revealed that levels of intention, social modelling and cheerfulness within individuals were associated with health factor. Having a higher intention level than someone’s average intention level leads to healthier snacking while seeing someone in the environment compared with not seeing someone in the environment and a higher cheerfulness level than someone’s average cheerfulness level promotes unhealthier choices. Additionally, intention and social modelling show a between-person association with health factor, where higher intention aligns with healthier choices, and higher levels of social modelling lead to unhealthier choices. Furthermore, visibility affects portion size both on a within- and between-person level. The portion size increases when the snack is visible. Besides, no associations were found between the determinants and the decision to snack. Through the implementation of EMA, this study has generated novel insights into the within-person associations between time-varying determinants and snacking, thereby offering valuable implications for future research. Such information holds the potential for incorporation into JITAI, allowing for personalized tailoring, more effective promotion of healthier snacking behaviours and thus pursuing the challenge of healthy ageing.
Acknowledgements
The authors would like to thank Fran Bogaert for her contribution to conceptualisation of the study and data collection and Louise Poppe for her contribution to the data analysis.
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
K. C.: Conceptualisation, methodology, investigation, resources, formal analysis, writing – original draft, writing – review and editing, visualisation, and project administration. F. D. V.: Conceptualisation, formal analysis, writing – original draft, writing – review and editing, visualisation, and project administration. G. C.: Writing – review and editing and supervision. I. M.: Formal analysis and writing – review and editing. D. V. D.: Conceptualisation, methodology, formal analysis, writing – review and editing, and supervision.
The authors declare none.
Ethical approval was obtained from the Ghent University Hospital ethics committee (registration number B6702021000698). Written informed consent was obtained from all participants.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S0007114524001004







