



Rhodiola rosea (RR) is a flowering perennial plant found in Arctic regions of Europe, Asia and North America. Known by several other names – including roseroot, rosenroot, golden root, arctic root and more – this member of the Crassulaceae family has been used for medicinal purposes for centuries, with the Greek physician Dioscorides describing medicinal application in 77 AD(Reference Panossian, Wikman and Sarris1,Reference Tao, Wu and Cao2) . The physiological effects of RR ingestion are thought to arise from its roles as an adaptogen, a term historically applied to substances that cause ‘a state of non-specifically increased resistance to stress’(Reference Brekhman and Dardymov3). Adaptogens can be defined as substances that promote physiological resilience, resistance to stress and maintenance or restoration of physiological function when homoeostasis is challenged. In this regard, adaptogens may enhance physical and cognitive performance under duress, as well as general well-being, and several purported adaptogens are experiencing increased popularity in the dietary supplement industry(4). The adaptogenic actions of RR are primarily attributed to bioactive compounds within the root, with salidroside and rosavin often noted as the most influential compounds(Reference Yousef, Grace and Cheng5). As a result, many commercial RR preparations are standardised to specific concentrations of salidroside and rosavin. However, at least 109 chemical compounds have been identified in RR (Reference Tao, Wu and Cao2). Collectively, these bioactive components have been observed to exert anti-stress and anti-fatigue effects, as well as enhance aspects of cognitive and physical performance, in part through their antioxidant properties(Reference Olsson, von Schéele and Panossian6,Reference Lekomtseva, Zhukova and Wacker7,Reference Hung, Perry and Ernst8,Reference Lu, Deng and Xu9) . The effects of RR on cognitive and physical function could also relate to interactions with components of physiological stress-response systems, such as monoamine neurotransmitters (e.g. serotonin and catecholamines) and opioid peptides (e.g. β-endorphins)(Reference Ivanova Stojcheva and Quintela10).
The longstanding medicinal use of RR and the marked popularity of dietary supplements containing extracts of this plant(4) warrant cohesive summaries of research detailing its physiological effects. While RR has been widely studied for aiding mental health and cognitive function(Reference Lewis, Poles and Shaw11), as well as general stress and fatigue resistance(Reference Ivanova Stojcheva and Quintela10), the purpose of this narrative review is to describe the potential roles of RR as an adaptogen within the context of physical performance. We begin by considering preclinical research on RR’s putative mechanisms of action and then summarise the available clinical research on the efficacy of RR supplementation.
Potential mechanisms of physical performance benefits
Multiple mechanisms have been proposed to explain the potential ergogenic effects of RR on exercise performance, recovery and long-term adaptations to exercise training. Several rodent studies that have demonstrated improvements in exercise performance following supplementation have probed the means by which RR acts(Reference Lee, Kuo and Liou12,Reference Abidov, Crendal and Grachev13) . Four weeks of RR ingestion (5–125 mg/d) increased resting liver glycogen content and attenuated muscle glycogen depletion during 90-min unloaded swimming exercise in Wistar rats, although the mechanism for these findings was not established(Reference Lee, Kuo and Liou12). RR prolonged time-to-exhaustion (TTE) during weight-loaded swimming by 21–65 %, with increasing doses providing greater benefits. Compared with the control group, RR supplementation reduced post-exercise fatigue biomarkers, including glutamic oxaloacetic transaminase, glutamic pyruvic transaminase and lactate dehydrogenase, and supplementation increased skeletal muscle and liver tissue oxygenation and expression of proteins involved in TAG synthesis (sterol regulatory element-binding protein-1 and fatty acid synthase)(Reference Lee, Kuo and Liou12). Other work has corroborated the reduction in post-exercise lactate dehydrogenase following 30 d of RR supplementation and also finding reductions in creatine kinase, suggesting an attenuation of exercise-induced muscle damage during strenuous activity(Reference Bang, Aranão and Nogueira14). A separate investigation reported that 6 d of supplementation with 50 mg/kg/d of RR (3 % rosavin, 0·9 % salidroside) administered 30 min prior to daily exercise sessions increased swimming TTE by 25 % in Sprague-Dawley rats(Reference Abidov, Crendal and Grachev13). Mitochondrial ATP content, as estimated by a bioluminescence assay quantifying ATP reactivity with recombinant firefly luciferase(Reference Drew and Leeuwenburgh15), was better preserved following exercise in the supplemented group, implying RR may improve mitochondrial ATP synthesis during or after intense exercise. In rat skeletal muscle cells, isolated salidroside has been found to activate AMP-activated protein kinase(Reference Li, Ge and Zheng16), a master regulator of exercise signalling pathways that senses cellular energy status and exerts numerous downstream effects on carbohydrate and lipid metabolism at times of energy stress(Reference Spaulding and Yan17). Together, these studies show that RR supplementation may enhance endurance exercise performance in rodents by countering fatigue associated with changes in cellular bioenergetics.
Additional research has assessed the potential roles of RR as an antioxidant, which may be relevant to exercise training, recovery and adaptation. While reactive oxygen species have important signalling roles that affect physiological adaptations to exercise, the antioxidant status of individuals influences whether antioxidant supplementation will have positive, negative or null effects on exercise performance and adaptations(Reference Margaritelis, Paschalis and Theodorou18). As such, potential antioxidant effects of bioactive compounds should be considered alongside baseline antioxidant status, which is influenced by dietary intake, adaptations to exercise and numerous other factors. In a rodent model, Huang et al.(Reference Huang, Lee and Kuo19) demonstrated the free radical-scavenging activity of several of RR’s bioactive phytochemicals (e.g. salidroside, rosavin, rosin and rosarin) and found RR supplementation enhanced weight-loaded swimming performance. In this study, 4 weeks of RR supplementation increased liver expression of the antioxidant enzymes catalase, manganese superoxide dismutase and copper/zinc superoxide dismutase; suppressed exercise-induced increases in oxygen-free radicals in blood, liver and skeletal muscle and reduced levels of the lipid peroxidation product malondialdehyde(Reference Huang, Lee and Kuo19). Other work has highlighted the potential of isolated salidroside to increase antioxidant enzyme activity, bolster liver glycogen and improve exercise performance following 4 weeks of supplementation(Reference Xu and Li20). Collectively, murine research that has assessed antioxidant activity alongside exercise performance has generally reported that ergogenic effects of RR supplementation are concurrent with augmented antioxidant defence systems. In these studies, RR’s antioxidant activity appears not to hinder beneficial exercise adaptations due to suppression of signalling by reactive species, as has been reported for certain other antioxidant supplements, such as high doses of vitamins C and E (1000 mg/d vitamin C and 400 mg/d vitamin E)(Reference Ristow, Zarse and Oberbach21). It is also possible that the other advantageous effects of supplementation may outweigh any detrimental effects resulting from acutely increased antioxidant activity. Additionally, it is plausible that the antioxidant status of the animals used in this research may have been conducive to demonstrating ergogenic effects of a supplement with antioxidant activity(Reference Margaritelis, Paschalis and Theodorou18).
Compared with endurance-based exercise models, there has been less research on the potential mechanisms by which RR modifies responses to resistance training. Roumanille et al.(Reference Roumanille, Vernus and Brioche22) studied both acute and chronic effects of RR supplementation (2 % rosavin, 1 % salidroside) in rats performing climbing resistance exercise. The authors observed no effects of supplementation on post-exercise skeletal muscle protein synthesis. In keeping with this finding, RR had no influence on muscle growth, strength or power following 4 weeks of exercise training plus supplementation. Clearly, additional mechanistic research is needed to establish any influences of RR on adaptations to resistance training. While yet to be demonstrated in a preclinical model of resistance training, one might speculate that the aforementioned RR-induced reductions in exercise-induced muscle damage and improvements in cellular bioenergetics could positively affect resistance training.
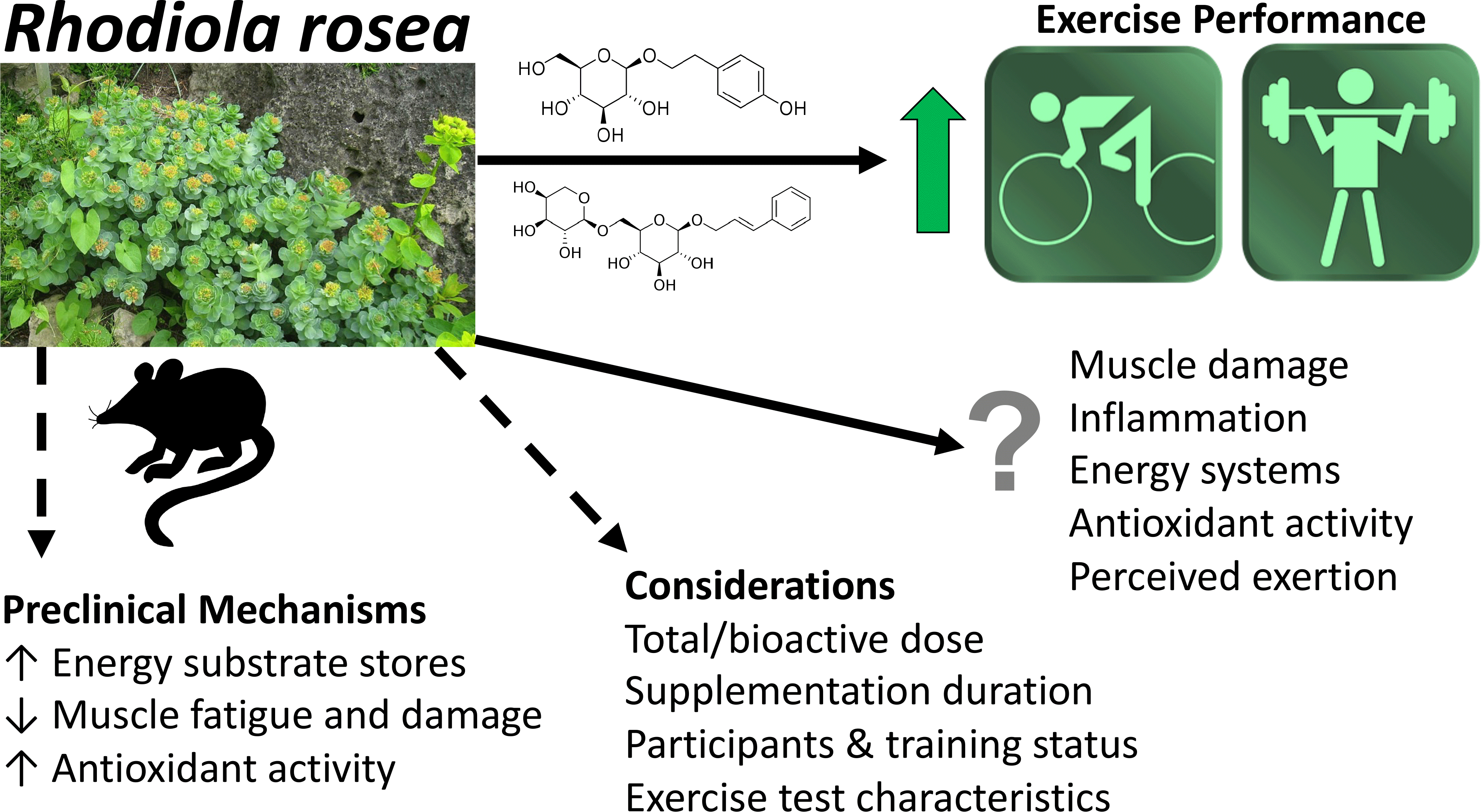
In summary, preclinical data suggest that RR modulates energy substrate storage and use, reduces fatigue and muscle damage and increases antioxidant status. Despite the promise of this research, clinical studies are needed to identify whether these findings translate to humans, as well as to elucidate ergogenic dosing protocols.
Studies of humans
Study characteristics
Literature search
Over the past two decades, more than a dozen clinical trials have examined the effects of RR on exercise performance and adaptations (Table 1)(Reference Spasov, Wikman and Mandrikov23,Reference Abidov, Grachev and Seifulla24,Reference De Bock, Eijnde and Ramaekers25,Reference Walker, Altobelli and Caprihan26,Reference Skarpanska-Stejnborn, Pilaczynska-Szczesniak and Basta27,Reference Parisi, Tranchita and Duranti28,Reference Noreen, Buckley and Lewis29,Reference Duncan and Clarke30,Reference Shanely, Nieman and Zwetsloot31,Reference Ahmed, Henson and Sanderson32,Reference Duncan, Tallis and Wilson33,Reference Timpmann, Hackney and Tamm34,Reference Jówko, Sadowski and Długołęcka35,Reference Ballmann, Maze and Wells36,Reference Lin, Hsu and Lin37,Reference Williams, Langley and Roberson38,Reference Liu, Zhao and Yan39) . To ensure this narrative review accurately represents the current body of scientific evidence, searches were performed using several electronic databases (PubMed®, Web of ScienceTM and Scopus), with screening of relevant articles to identify research reporting the effects of RR on exercise performance and related outcomes in humans. We only considered trials providing RR in isolation, excluding those providing it as a component of a multi-ingredient supplement. In this process, we identified sixteen trials, primarily randomised controlled trials, published between 2000 and 2023, collectively totalling 363 total participants.
Table 1. Human studies of RR supplementation for physical performance enhancement

1-RM, 1-repetition maximum; ALT, alanine transaminase; AST, aspartate aminotransferase; BM, body mass; CK, creatine kinase; CRP, C-reactive protein; DOMS, delayed onset muscle soreness; EE, energy expenditure; eHSP72, extracellular heat-shock protein 72; F, female; G-CSF, granulocyte-colony stimulating factor; GH, growth hormone; GPx, glutathione peroxidase; HR, heart rate; M, male; MCP-1, monocyte chemoattractant protein-1; MVIC, maximum voluntary isometric contraction; n, number of participants; N/A, not applicable; NR, not reported; PCr, phosphocreatine; Pi, inorganic phosphate; PL, placebo; RPE, ratings of perceived exertion; RR, Rhodiola rosea; RTF, repetitions to failure; SOD, superoxide dismutase; TAC, total antioxidant capacity; TBARS, thiobarbituric acid reactive substances; TTE, time-to-exhaustion.
* Acute is defined here as 1–7 d of supplementation, with chronic defined as >7 d of supplementation.
Exercise protocols
Eight of the clinical studies identified included bicycle ergometry as an exercise testing modality, and the specific protocols varied widely(Reference Spasov, Wikman and Mandrikov23,Reference Abidov, Grachev and Seifulla24,Reference De Bock, Eijnde and Ramaekers25,Reference Parisi, Tranchita and Duranti28,Reference Noreen, Buckley and Lewis29,Reference Duncan and Clarke30,Reference Jówko, Sadowski and Długołęcka35,Reference Ballmann, Maze and Wells36) . Three trials included running, either on a treadmill(Reference Duncan, Tallis and Wilson33,Reference Lin, Hsu and Lin37) or as a marathon race(Reference Shanely, Nieman and Zwetsloot31,Reference Ahmed, Henson and Sanderson32) , one trial employed walking on a treadmill in a climate chamber(Reference Timpmann, Hackney and Tamm34), one trial used rowing ergometry(Reference Skarpanska-Stejnborn, Pilaczynska-Szczesniak and Basta27) and three trials incorporated resistance exercise, including wrist flexion(Reference Walker, Altobelli and Caprihan26), bench press(Reference Williams, Langley and Roberson38,Reference Liu, Zhao and Yan39) and/or squat exercises(Reference Liu, Zhao and Yan39).
Participant demographics
The participants in most trials were healthy young adults, with mean ages <30 years in all trials except one, which contained participants with mean ages of ∼40 to 44 years and was described in two articles(Reference Shanely, Nieman and Zwetsloot31,Reference Ahmed, Henson and Sanderson32) . Eleven studies included only male participants, two only included female participants, two included both sexes and biological sex was not reported in one investigation. Training status ranged from untrained to highly trained, although some descriptions of training status were vague, precluding the ability to determine the true training status of participants. Nonetheless, training statuses were designated by study authors as untrained (n 2), recreationally active (n 4), active (n 4) and trained/athletes (n 5), with training status not reported in one investigation. Collectively, based on a recent Participation Classification Framework(Reference McKay, Stellingwerff and Smith40), most participants likely fell within the tier 1 (recreationally active) or tier 2 (trained/developmental) categories, with the possibility of some untrained participants falling within tier 0 (sedentary)(Reference Abidov, Grachev and Seifulla24,Reference Liu, Zhao and Yan39) and some highly trained participants belonging to tier 3 (highly trained/national level)(Reference Skarpanska-Stejnborn, Pilaczynska-Szczesniak and Basta27). Six studies used acute RR supplementation protocols(Reference Walker, Altobelli and Caprihan26,Reference Noreen, Buckley and Lewis29,Reference Duncan and Clarke30,Reference Duncan, Tallis and Wilson33,Reference Ballmann, Maze and Wells36,Reference Williams, Langley and Roberson38) , defined here as 1–7 d of supplementation, nine implemented chronic supplementation (>7 d; range 8–38 d)(Reference Spasov, Wikman and Mandrikov23,Reference Abidov, Grachev and Seifulla24,Reference Skarpanska-Stejnborn, Pilaczynska-Szczesniak and Basta27,Reference Parisi, Tranchita and Duranti28,Reference Shanely, Nieman and Zwetsloot31,Reference Ahmed, Henson and Sanderson32,Reference Timpmann, Hackney and Tamm34,Reference Lin, Hsu and Lin37,Reference Liu, Zhao and Yan39) and one incorporated both acute and chronic supplementation strategies(Reference De Bock, Eijnde and Ramaekers25). Daily doses of RR ranged from 100 to 2400 mg/d. While not all studies reported the concentration of bioactive compounds, the most commonly reported concentrations were ∼1 % salidroside and ∼3 % rosavin.
Endurance exercise capacity and performance
Several trials included in this review assessed the effects of RR on endurance exercise performance. One crossover study of ‘physically active’ males and females reported 2·4 % longer cycling TTE following acute RR ingestion(Reference De Bock, Eijnde and Ramaekers25), and a separate parallel-arm trial of male physical education students ‘not engaged in high-performance sports’ at the time of testing found a similar increase in cycling TTE of 2·6 %, although this was not statistically significant(Reference Jówko, Sadowski and Długołęcka35). Both studies provided a 200 mg dose of RR (3 % rosavin) 60–90 min before the incremental maximum effort TTE test. However, one trial evaluated TTE both after acute (2-d) and chronic (28-d) supplementation(Reference De Bock, Eijnde and Ramaekers25), whereas the other only tested TTE after chronic (28-d) supplementation(Reference Jówko, Sadowski and Długołęcka35). In the study of De Bock et al.(Reference De Bock, Eijnde and Ramaekers25), an increase in TTE (+24 s, on average; RR 17·2 (se 0·8) min v. placebo 16·8 (se 0·7) min) was only observed in the acute crossover trial, and there were no between-condition differences in the subsequent parallel-arm trial included in the same report, which included 200 mg/d RR supplementation over 4 weeks. This could be due to the larger sample size per condition/group and greater statistical power in the acute trial (n 24, crossover design) compared with the chronic trial (n 11–12 per group, parallel arm). Similarly, the trial of Jówko et al.(Reference Jówko, Sadowski and Długołęcka35) used chronic supplementation (600 mg/d, with 200 mg/d provided before TTE tests) in a parallel-arm design (n 13 per group) and found no statistically significant effects of chronic supplementation on TTE. However, the mean difference in TTE in the RR group was +20·8 s (+2·6 %) after 4 weeks of supplementation compared with −10·1 s (-1·3 %) with placebo. As such, it is possible these trials of chronic supplementation were underpowered to detect a small-but-meaningful influence of supplementation on TTE performance. Additionally, analysis of changes in maximal cycling power from the incremental maximum effort TTE tests indicated a significant difference between RR (+5·7 %) and placebo (-4·1 %)(Reference Jówko, Sadowski and Długołęcka35).
Other studies have yielded conflicting or null results. In a crossover study including recreationally active females, RR improved time trial performance in a 6-mile bicycle ergometry test (RR 25·4 (se 2·7) min, placebo 25·8 (se 3·0) min, P = 0·04) following acute supplementation with 3 mg/kg (∼170 mg) RR provided 60 min before exercise(Reference Noreen, Buckley and Lewis29). RR also reduced average heart rate during the warm-up period (RR 136 (se 17) bpm, placebo 140 (se 17) bpm). In contrast, supplementation did not affect 2000-m rowing time in male rowers(Reference Skarpanska-Stejnborn, Pilaczynska-Szczesniak and Basta27) or marathon performance in male and female runners(Reference Shanely, Nieman and Zwetsloot31,Reference Ahmed, Henson and Sanderson32) . Additional research reported no benefit of acute RR supplementation for 5-km run time trial performance in recreationally active males(Reference Duncan, Tallis and Wilson33), nor any benefit of chronic supplementation for a treadmill walk to exhaustion conducted in a climate chamber(Reference Timpmann, Hackney and Tamm34). However, a separate trial found RR decreased heart rate during bicycle ergometry work capacity testing following 20 d of supplementation with 100 mg/d(Reference Spasov, Wikman and Mandrikov23). These findings are discordant with other investigations reporting no influence of RR on heart rate during exercise(Reference Parisi, Tranchita and Duranti28,Reference Duncan and Clarke30,Reference Duncan, Tallis and Wilson33,Reference Timpmann, Hackney and Tamm34,Reference Jówko, Sadowski and Długołęcka35) . The divergent training statuses, exercise testing modalities and RR dosing protocols may contribute to differences in endurance exercise performance outcomes.
As discussed, improvements in TTE with RR supplementation in murine models have been associated with higher resting liver glycogen content and attenuated exercise-induced reductions in muscle glycogen(Reference Lee, Kuo and Liou12), suggesting that alterations in glycogen turnover potentially contribute to ergogenic effects on endurance exercise following chronic supplementation. RR has also been found to support mitochondrial ATP content(Reference Abidov, Crendal and Grachev13), representing another mechanism by which RR may improve prolonged exercise performance. However, similar outcomes have not been examined in human participants to determine whether these mechanisms contribute to the observed results.
Power and resistance exercise performance
Although limited, clinical research examining the effects of RR supplementation on power and resistance exercise performance has demonstrated potentially meaningful ergogenic effects. In their study of physically active (>150 min/week of moderate physical activity) young adult females, Ballmann et al.(Reference Ballmann, Maze and Wells36) observed improvements in nearly all outcomes during repeated Wingate tests (3 × 15-s tests) performed on a bicycle ergometer, including mean and peak power, total work, anaerobic capacity and anaerobic power following RR supplementation. Effect sizes indicating the magnitude of performance improvements ranged from small to large, with the largest values observed for anaerobic capacity (RR 10·5 (se 0·9) watts/kg body mass, placebo 10·1 (se 1·1) watts/kg; P = 0·01; Cohen’s d effect size 0·96 (large)) and anaerobic power (RR 15·2 (se 1·1) watts/kg body mass, placebo 14·0 (se 1·2) watts/kg; P = 0·03; Cohen’s d effect size 1·07 (large)). The supplementation protocol included 3 d of 1500 mg/d RR (1 % salidroside, 3 % rosavin), followed by 500 mg ingestion on the fourth day, 30 min prior to exercise testing. This trial, along with a subsequent trial from the same research group(Reference Williams, Langley and Roberson38), used a higher dose of RR than nearly all other trials we identified (Table 1). The origin of this higher dose appears to be a study conducted by Walker et al.(Reference Walker, Altobelli and Caprihan26), who sought to employ a dose higher than manufacturer recommendations in an attempt to approach doses shown to exert beneficial effects on mitochondrial ATP content in rodents(Reference Abidov, Crendal and Grachev13). While one other investigation used a higher total dose of RR (2400 mg/d), the lower concentration of bioactive compounds (0·5 % salidroside, rosavin not reported)(Reference Liu, Zhao and Yan39) led to a lower absolute dose of these compounds compared with the aforementioned studies. The trial of Walker et al.(Reference Walker, Altobelli and Caprihan26) first administered a daily dose of 1500 mg/d (3 % rosavin, salidroside not reported), although this was in the context of a muscular endurance test (incremental forearm wrist flexion to exhaustion). In this instance, there were no benefits of acute (4-d) supplementation, although the forearm exercise protocol is dissimilar to those employing multiple larger muscle groups and inducing greater systemic stress and fatigue. As discussed, other research also supports potential benefits of RR for improving maximal cycling power(Reference Jówko, Sadowski and Długołęcka35).
Two recent trials have examined whether RR supplementation improves resistance exercise performance, with one employing acute supplementation prior to exercise testing(Reference Williams, Langley and Roberson38) and the other pairing chronic supplementation with supervised resistance training(Reference Liu, Zhao and Yan39). In untrained participants, Liu et al.(Reference Liu, Zhao and Yan39) found that 30 d of supplementation with 2400 mg/d RR (0·5 % salidroside, rosavin not reported) alongside supervised resistance training produced superior performance adaptations compared with placebo. The resistance training programme contained thirteen training sessions over the 30-d study and included the bench press and deep squat exercises, with 4 sets of 10 repetitions at 60 % of the pre-training 1-repetition maximum (1RM) for the first 15 d and 4 sets of 8 repetitions at 70 % of the pre-training 1RM for the last 15 d. In the RR group, greater increases were observed for bench press 1RM (9 % greater increase with RR compared with placebo; P = 0·01), squat 1RM (7·5 % greater increase with RR compared with placebo; P = 0·01), knee extension maximal voluntary isometric contraction (8·6 % greater increase with RR compared with placebo; P = 0·008) and bench press repetitions to failure (12·7 % greater increase with RR than placebo; P = 0·005). The same study also found potentially additive effects of RR and caffeine ingestion in untrained participants, leading to a follow-up examination of RR plus caffeine in resistance-trained participants. This subsequent work also found improvements in select resistance exercise performance metrics compared with placebo(Reference Liu, Zhao and Yan39). Interestingly, Williams et al.(Reference Williams, Langley and Roberson38) observed some beneficial and some disadvantageous effects of acute RR supplementation (1500 mg/d, 1 % salidroside, 3 % rosavin) on bench press performance in resistance-trained males (8·7 (se 6·3) years resistance training experience). RR supplementation led to an ∼8 % greater increase in mean concentric velocity (P = 0·049; Cohen’s d effect size 0·73 (medium-to-large)) during a set of 2 repetitions at 75 % of 1RM, performed with maximal explosive intent, compared with placebo. However, in a subsequent test of repetitions to failure across 3 sets at 75 % 1RM, RR supplementation reduced total repetitions completed compared with placebo (P < 0·001; Cohen’s d 1·90 (large)), although the difference was small (∼2 repetitions across 3 sets). Although the test of concentric velocity can be viewed as non-fatiguing, and a 5-min rest took place between the velocity test and subsequent repetitions to failure protocol, it is possible the superior performance in the RR condition during the concentric velocity test influenced subsequent performance during the repetitions to failure test. Nonetheless, a potential tradeoff between mean concentric velocity and total training volume should be considered, as the relative importance of these variables depends on training goals and other contextual factors.
Muscle damage and inflammation
Several trials have examined the potential influence of RR on post-exercise markers of muscle damage. While RR supplementation has been found to reduce creatine kinase concentrations at rest and following fatiguing bicycle ergometry tests(Reference Abidov, Grachev and Seifulla24,Reference Parisi, Tranchita and Duranti28) and treadmill running(Reference Lin, Hsu and Lin37), this has not been found consistently in all studies(Reference Skarpanska-Stejnborn, Pilaczynska-Szczesniak and Basta27,Reference Shanely, Nieman and Zwetsloot31,Reference Ahmed, Henson and Sanderson32,Reference Jówko, Sadowski and Długołęcka35) . When untrained adults performed an incremental bicycle ergometry test to exhaustion, Abidov et al. (Reference Abidov, Grachev and Seifulla24) found a substantial increase in creatine kinase concentrations (∼166 U/ml at baseline to ∼1650 U/ml 5 h after exercise), which did not appear to be influenced by RR supplementation (30 d of 680 mg/d prior to test). However, 5 d after the test, creatine kinase fell to ∼1450 U/ml in RR condition, whereas values remained at ∼2750 U/ml in the placebo condition, on average, suggesting a delayed effect of RR. In the same study, RR supplementation reduced C-reactive protein both 5 h and 5 d after the exercise test. Following 30 d of supplementation with 170 mg RR/d, Parisi et al.(Reference Parisi, Tranchita and Duranti28) reported lower creatine kinase concentrations compared with placebo, both at rest and during exercise recovery. Most of the investigations showing no effect of RR supplementation on creatine kinase and other markers of muscle damage or inflammation have included well-trained participants, such as marathon runners(Reference Shanely, Nieman and Zwetsloot31,Reference Ahmed, Henson and Sanderson32) and members of a national rowing team(Reference Skarpanska-Stejnborn, Pilaczynska-Szczesniak and Basta27). As such, it is plausible that adaptations to habitual exercise training – such as the neural, connective tissue and cellular factors potentially contributing to the repeated bout effect(Reference McHugh, Connolly and Eston41) – either minimised muscle damage or otherwise reduced the likelihood of an influence of supplementation. Additional trials have reported no changes in multiple markers of inflammation, including C-reactive protein, various IL and liver enzymes following treadmill or marathon running(Reference Shanely, Nieman and Zwetsloot31,Reference Ahmed, Henson and Sanderson32,Reference Lin, Hsu and Lin37) .
Energy systems
As mentioned, RR influences ATP production, energy substrate storage and signalling pathways involved in cellular energy status in rodents(Reference Lee, Kuo and Liou12,Reference Abidov, Crendal and Grachev13,Reference Li, Ge and Zheng16) . A few clinical studies have investigated outcomes related to energy metabolism. For instance, RR supplementation has been found to increase(Reference Williams, Langley and Roberson38), decrease(Reference Parisi, Tranchita and Duranti28) or exert no discernible influence(Reference Skarpanska-Stejnborn, Pilaczynska-Szczesniak and Basta27,Reference Noreen, Buckley and Lewis29,Reference Duncan, Tallis and Wilson33,Reference Timpmann, Hackney and Tamm34,Reference Lin, Hsu and Lin37) on post-exercise lactate concentrations compared with placebo. The sole study reporting an increase in lactate concentrations with supplementation used resistance training in resistance-trained males(Reference Williams, Langley and Roberson38), while the only trial indicating a decrease in post-exercise lactate included cycling to exhaustion in male athletes(Reference Parisi, Tranchita and Duranti28). The studies reporting no influence on lactate used varying exercise modalities and participants (i.e. rowing in male rowers(Reference Skarpanska-Stejnborn, Pilaczynska-Szczesniak and Basta27), treadmill running in active males(Reference Duncan, Tallis and Wilson33,Reference Lin, Hsu and Lin37) , cycling in recreationally active females(Reference Noreen, Buckley and Lewis29) and treadmill walking in active males(Reference Timpmann, Hackney and Tamm34)).
As mentioned, RR supplementation has been reported to improve Wingate test performance, implying potential benefits related to the energy substrates and metabolic pathways involved in rapid ATP production (i.e. ATP storage, the ATP-phosphocreatine system and anaerobic glycolysis). However, one of the most informative studies relevant to these outcomes(Reference Walker, Altobelli and Caprihan26) demonstrated no clear influence of RR on the phosphocreatine energy system. Specifically, there were no differences in concentrations of phosphocreatine, ATP, inorganic phosphate or pH during incremental wrist flexion performed to exhaustion in resistance-trained (> 6 months training experience) males following 4 d of RR supplementation (1500 mg/d for 3 d, 1000 mg on the testing day; 3 % rosavin). The authors speculated the lack of effect on muscle phosphate kinetics, in contrast to rodent research(Reference Abidov, Crendal and Grachev13), could have been related to supplement dosing. Specifically, they estimated that a dose of ∼4000 mg/d RR for humans would be needed to match the dose provided by Abidov et al.(Reference Abidov, Crendal and Grachev13), who reported superior mitochondrial ATP preservation following exercise in rodents supplemented with RR. Additionally, the authors acknowledged that if RR influences central fatigue, the model of wrist flexion may not be optimal to detect ergogenic effects(Reference Walker, Altobelli and Caprihan26). Other relevant effects observed in murine models, such as increased glycogen storage and delayed glycogen depletion(Reference Lee, Kuo and Liou12), have yet to be examined in humans.
Antioxidant activity
Multiple bioactive compounds within RR have antioxidant activity in rodent models(Reference Huang, Lee and Kuo19,Reference Xu and Li20) . In human trials, two studies have reported an increase in total antioxidant capacity, an overall measure of plasma antioxidant activity, following 28 d of 200–600 mg/d RR supplementation in recreationally active or highly trained individuals(Reference Skarpanska-Stejnborn, Pilaczynska-Szczesniak and Basta27,Reference Jówko, Sadowski and Długołęcka35) . This was observed for resting (pre-exercise) values in both studies and for post-exercise values in one trial(Reference Skarpanska-Stejnborn, Pilaczynska-Szczesniak and Basta27). The differences in exercise testing protocol (i.e. 2000-m maximal effort rowing(Reference Skarpanska-Stejnborn, Pilaczynska-Szczesniak and Basta27) v. incremental maximal effort bicycle ergometry test(Reference Jówko, Sadowski and Długołęcka35)) and participant training status (national rowing team members(Reference Skarpanska-Stejnborn, Pilaczynska-Szczesniak and Basta27) v. recreationally active(Reference Jówko, Sadowski and Długołęcka35)) may have influenced the difference in post-exercise total antioxidant capacity values. Alongside the increase in total antioxidant capacity, a decrease in post-exercise erythrocyte superoxide dismutase activity was observed by Skarpanska-Stejnborn et al.(Reference Skarpanska-Stejnborn, Pilaczynska-Szczesniak and Basta27), which the authors interpreted as an indication that RR led to more effective elimination of superoxide anions in erythrocytes. However, Jówko et al.(Reference Jówko, Sadowski and Długołęcka35), who also reported increased total antioxidant capacity at rest, found no effect of supplementation on erythrocyte superoxide dismutase activity at rest, post-exercise or 24 h after exercise. Additional research is needed to clarify the degree to which RR exerts antioxidant effects in humans. Based on the lack of investigations reporting ergolytic effects of supplementation, coupled with several trials reporting positive effects, the current evidence does not suggest that any supplementation-associated increases in antioxidant status compromise exercise performance in the short term(Reference Margaritelis, Paschalis and Theodorou18). However, while ten studies employed RR supplementation lasting 8–38 d, most investigations have not included supervised or structured exercise training alongside supplementation. As such, the influence of long-term RR supplementation on adaptations to chronic exercise training is currently unclear. Future research should employ adequately powered parallel-arm trials to establish whether long-term RR supplementation alongside progressive exercise training influences adaptations to exercise, not only in terms of antioxidant capacity but also for exercise performance, body composition and other exercise- and health-relevant outcomes.
Other outcomes
In addition to the effects of RR on exercise performance, muscle damage, inflammation, energy systems and antioxidant activity, a few other outcomes from trials in humans are noteworthy. For instance, some research groups have documented reductions in ratings of perceived exertion following acute RR supplementation (3 mg/kg; ∼170 to 203 mg) provided 30 min prior to time trial cycling(Reference Noreen, Buckley and Lewis29) or cycling with a fixed duration and intensity(Reference Duncan and Clarke30). In one of these trials, reduced ratings of perceived exertion were concurrent with increases in self-reported arousal, pleasure and vigour(Reference Duncan and Clarke30). These beneficial subjective responses are aligned with other documented effects of RR, such as its anti-stress and anti-fatigue effects(Reference Hung, Perry and Ernst8,Reference Lu, Deng and Xu9) . While speculative, these effects could possibly be due to the influence of bioactive compounds on monoamine neurotransmitters and opioid peptides(Reference Ivanova Stojcheva and Quintela10). However, several other trials have reported no influence of supplementation on ratings of perceived exertion(Reference Walker, Altobelli and Caprihan26,Reference Parisi, Tranchita and Duranti28,Reference Duncan, Tallis and Wilson33,Reference Timpmann, Hackney and Tamm34) . Due to potential antidepressant properties of RR (Reference Amsterdam and Panossian42), the possibility of varying effects, including downstream consequences for exercise performance, based on the presence of affective disorders should be considered. Furthermore, it should be noted that RR has been widely studied for aiding mental health and cognitive function(Reference Lewis, Poles and Shaw11) and promoting resistance to general stress and fatigue(Reference Ivanova Stojcheva and Quintela10), although the purpose of the present review is to describe the roles of RR within the context of physical performance.
Additional trials have reported beneficial effects of RR supplementation that may be relevant to sports performance, such as improvements in movement speed and accuracy, reductions in mental fatigue(Reference Spasov, Wikman and Mandrikov23) and quicker reaction time(Reference Jówko, Sadowski and Długołęcka35). Spasov et al.(Reference Spasov, Wikman and Mandrikov23) found that 20 d of supplementation with 100 mg/d RR (2 % salidroside, 3 % rosavin) reduced self-assessed mental fatigue, with a ∼30 % decrease in fatigue – based on a questionnaire evaluating various forms of fatigue, sleeping patterns, mood and mental states – compared with a ∼21 % increase in the placebo group. In a study of 28 d of supplementation with 600 mg/d RR (3 % rosavin), Jówko et al.(Reference Jówko, Sadowski and Długołęcka35) found significant differences in relative changes in simple reaction (median reaction time and total response time) and choice reaction (number of correct responses) with supplementation compared with placebo. Median reaction time and total response time decreased by 5·7–9·5 % on average with supplementation, with mean increases of ∼4 to 5 % in the placebo group. The increase in correct responses in the choice reaction test was 16 % on average with supplementation compared with an increase in 6·6 % on average with placebo. However, changes in other reaction metrics, such as median movement time during the simple reaction test and median response time in the choice reaction test, were unaffected by supplementation(Reference Jówko, Sadowski and Długołęcka35). Collectively, these findings provide initial support for benefits of RR for cognitive and subjective outcomes ancillary to exercise performance per se.
While limited data are available, one trial assessed the potential immunomodulatory actions of RR in exercising adults. After 30 d of supplementation with 600 mg/d RR or placebo, male and female runners provided serum samples before and after completing a marathon race, to examine various components of the immune system(Reference Ahmed, Henson and Sanderson32). While RR did not exert any obvious antibacterial effects, a decrease in viral replication following vesicular stomatitis virus was evident in the serum of runners supplementing with RR, leading the authors to conclude that supplementation could help defend against exercise-induced susceptibility to viral infections(Reference Ahmed, Henson and Sanderson32). If this is the case, the finding is potentially meaningful due to the detrimental impacts of acute illnesses in athletes, the inability to train and compete due to infection and the risk of infection transmission to team members(Reference Jaworski and Rygiel43).
Recommendations for supplementation
Supplement quality and third-party testing
As with any dietary supplement, practitioners and consumers considering supplementation with RR should ensure a high-quality product from a reputable manufacturer is selected. Currently, third-party testing is one of the most objective ways to ensure the purity, quality and ingredient doses within a product. Examples of well-recognised third-party testing organisations include NSF, Informed, U.S. Pharmacopeia, the Banned Substances Control Group and Labdoor. Those who may be subject to drug testing, particularly athletes, may benefit from the rigour of testing associate with services such as NSF Certified for Sport® and Informed Sport. While details of specific testing services vary, most include components of verification of the stated ingredients and doses, examination to ensure banned or dangerous substances are not present and confirmation of good manufacturing practices. Further details of each testing service are available on their respective websites.
Salidroside and rosavin concentration
While commercially available RR preparations vary in their concentration of the primary active components, it is recommended to choose a product that states the concentration of salidroside and rosavin within the product, preferably with verification of these concentrations via a certificate of analysis or third-party testing. As described, many of the RR preparations discussed in the present review contained ∼1 % salidroside and ∼3 % rosavin, although variability was present (Table 1). As described in the following sections, most studies demonstrating ergogenic effects for either endurance or strength and power outcomes have also used this common concentration of salidroside and rosavin.
Supplementation for endurance outcomes
The disparity in RR doses and mixed findings in extant research preclude definitive recommendations for an optimal dosing protocol. However, the trials reporting ergogenic effects of supplementation can be examined to provide tentative recommendations. Ergogenic effects of RR for TTE during an incremental bicycle ergometer test lasting ∼17 min have been seen at doses of 200 mg (1 % salidroside, 3 % rosavin)(Reference De Bock, Eijnde and Ramaekers25), with a benefit for time to completion during a 6-mile bicycle ergometer time trial lasting ∼25 min observed at ∼170 mg (3 mg/kg; 1 % salidroside, 3 % rosavin)(Reference Noreen, Buckley and Lewis29). These studies were conducted in ‘active’ or ‘recreationally active’ individuals. While other trials have shown no such benefits at similar doses, a tentative recommendation of an absolute dose of ≥200 mg RR containing ≥1 % salidroside and ≥3 % rosavin, consumed 60 min prior to exercise, may be appropriate for those planning to consume RR for the purpose of enhancing endurance exercise performance or capacity. These doses are also consistent with those producing some of previously discussed effects, albeit inconsistently, of reducing heart rate, improving subjective outcomes (e.g. general well-being, mental fatigue, vigour) and increasing total antioxidant capacity. To date, the highest located doses of RR employed the context of endurance exercise capacity and performance are 600–680 mg(Reference Abidov, Grachev and Seifulla24,Reference Shanely, Nieman and Zwetsloot31,Reference Jówko, Sadowski and Długołęcka35) , with primarily null results for exercise performance, except for changes in maximum power during a bicycle ergometry maximum effort test(Reference Jówko, Sadowski and Długołęcka35). However, these doses are less than half the 1500–2400-mg doses employed in models of forearm wrist flexion(Reference Walker, Altobelli and Caprihan26), Wingate anaerobic testing(Reference Ballmann, Maze and Wells36) and resistance exercise(Reference Williams, Langley and Roberson38,Reference Liu, Zhao and Yan39) .
Supplementation for strength and power outcomes
When compared with endurance exercise trials, the studies reporting ergogenic effects of RR for strength and power outcomes have generally utilised higher doses. Two trials found benefits of 1500 mg/d RR (1 % salidroside, 3 % rosavin) on various metrics of power during repeated 15-s Wingate anaerobic tests on a bicycle ergometer and mean concentric velocity during the bench press exercise. An additional study found a benefit of 2400 mg/d RR (0·5 % salidroside) on adaptations to 30 d of resistance training, although this was in untrained individuals. Based on the total dose and concentration of salidroside, these trials collectively used ∼12 to 15 mg salidroside. Using the common concentrations of ∼1 % salidroside and ∼3 % rosavin, a potentially ergogenic dose of RR for strength and power outcomes based on current research would be ∼1500 mg/d, with ∼500 mg consumed within 1 h before commencing exercise. Importantly, the apparent difference in recommended RR dose for endurance v. strength/power outcomes is based on the doses investigated in existing research rather than a comprehensive dose–response examination to inform whether ergogenic doses truly vary between these categories. As such, future research is needed to clarify and confirm the optimal doses of RR for those seeking to improve diverse exercise performance outcomes.
Training status
The current literature does not allow for definitive conclusions regarding the effects of exercise training status on RR supplementation recommendations. Most studies (13/16) were conducted in participants who were ‘recreationally active,’ ‘active’ or ‘trained,’ sometimes referred to as ‘athletes.’ In most cases, there was limited information regarding the precise meaning of these descriptors and terms were used disparately across studies. Collectively, as most studies likely contained participants in the tier 1 (recreationally active) or tier 2 (trained/developmental) categories(Reference McKay, Stellingwerff and Smith40), the current literature is generally not conducive to establishing whether RR supplementation differentially affects individuals of differing training statuses.
Sex differences
While potential sex differences related to RR supplementation are worth considering, the current literature has limited ability to inform this discussion. As noted, eleven studies included only male participants, two only included female participants, two included both sexes and biological sex was not reported in one investigation (Table 1). Additionally, the two investigations including both males and females did not present detailed sex-specific analysis(Reference De Bock, Eijnde and Ramaekers25,Reference Shanely, Nieman and Zwetsloot31) . Future research that is adequately powered to examine sex differences will help provide guidance regarding the possibility of sex-specific effects of supplementation.
Summary and future directions
Regarding exercise performance, RR supplementation has demonstrated select benefits for improved TTE during incremental maximum effort testing and time trial performance, both using bicycle ergometry. However, null results have also been observed in several trials using running, walking and rowing exercise. Adequately powered trials incorporating different doses of RR are needed to establish the effects of supplementation more clearly, and meta-analysis of exercise-relevant outcomes may provide additional insight. Interestingly, several trials have reported reduced heart rate or ratings of perceived exertion during exercise with RR supplementation, which could relate to the adaptogenic properties of the compounds within this plant. However, other trials have failed to confirm this effect. While less studied than endurance exercise, initial studies have indicated the potential for ergogenic effects of RR supplementation on power during anaerobic capacity and resistance exercise tests. Importantly, these trials have also administered higher doses of RR (1500–2400 mg/d; 0·5–1 % salidroside, ∼3 % rosavin) compared with much of the work on endurance exercise (100–680 mg/d; typically ∼1 % salidroside and ∼3 % rosavin, when reported). As such, dissimilarity in doses of bioactive components of RR should be considered, in addition to the potential for RR to differentially influence disparate types of physical performance. The optimal doses of different RR bioactives to maximise performance benefits in different exercise contexts have not yet been established. Future trials examining multiple dosing protocols using standardised RR extracts with known concentrations of salidroside and rosavin may illuminate optimal dosing protocols as well as whether acute and chronic supplementation differentially affect physical performance. In the existing literature, both acute and chronic supplementation have produced, or failed to produce, ergogenic effects. While select ergogenic benefits have been observed for endurance exercise outcomes at relatively low doses of ∼200 mg RR, investigation of higher doses may be warranted due to the positive effects observed for doses of ≥1500 mg for strength and power outcomes. Conversely, whether the higher doses of RR for strength and power outcomes are truly needed is unclear due to the lack of research employing lower doses. As such, studies examining both endurance- and strength- or power-related outcomes would benefit from incorporating multiple doses of RR to better establish effective dosing. Additionally, based on the limited inclusion of female participants in extant research, future studies should better establish the effects of RR supplementation in females and explore whether sex differences in the efficacy of supplementation are observed. Finally, the current research minimally addresses the question of whether RR supplementation influences adaptations to chronic exercise training. As such, randomised, placebo-controlled, parallel-arm trials incorporating supervised exercise training should be conducted to help address this research gap in groups of varying training status.
Beyond exercise performance itself, RR may influence exercise-relevant outcomes, such as muscle damage, inflammation, substrate metabolism, antioxidant capacity and perceptions of activity. While some trials reported benefits of supplementation on markers of muscle damage and inflammation, others have failed to observe such effects, particularly in exercise-trained individuals. Most trials have not reported an influence of supplementation on lactate production, with some exceptions. During wrist flexion exercise, there was no clear influence of acute RR supplementation on the phosphocreatine energy system. Other components of energy storage and turnover have yet to be examined in humans, despite the beneficial effects of supplementation observed in murine models. Total antioxidant capacity, measured at rest or following exercise, may increase in humans following supplementation, although the influence on specific antioxidant enzymes has been inconsistent. Nonetheless, the current evidence does not support an ergolytic effect of RR due to its potential antioxidant activity. Some studies reporting subjective outcomes have demonstrated the potential for supplementation to reduce perceived exertion and improve other psychological variables, while others have reported no benefits. Finally, the limited research to date has supported select immunomodulatory effects of supplementation in exercising humans, but additional studies are needed to establish any clinical significance of these findings. Additional confirmatory studies are needed for the aforementioned outcomes, particularly using chronic supplementation of varying doses, due to the limited existing research. Within these examinations, elucidation of the mechanisms by which bioactive components of RR exert their physiological effects is also warranted. Importantly, while the focus of the present review was physical performance and related outcomes, it is noteworthy that RR has been investigated for numerous other performance-enhancing effects, notably those related to cognitive function and general well-being(Reference Ivanova Stojcheva and Quintela10,Reference Lewis, Poles and Shaw11,Reference Panossian and Wikman44,Reference Crawford, Boyd and Deuster45,Reference Baker, Nuccio and Jeukendrup46) .
While a comprehensive discussion RR’s safety profile is beyond the scope of the present review, this botanical was deemed to have ‘acceptable safety data’ by the World Federation of Societies of Biological Psychiatry and Canadian Network for Mood and Anxiety Treatments Taskforce(Reference Sarris, Ravindran and Yatham47). Human data indicate RR and other Rhodiola species are well tolerated and produce minimal side effects(Reference Tao, Wu and Cao2,Reference Yu, Qin and Wang48) . Toxicological investigations in mice also indicate a low risk of toxicity(Reference Tao, Wu and Cao2,Reference Montiel-Ruiz, Roa-Coria and Patiño-Camacho49) . Nonetheless, the potential for interactions between RR and pharmaceuticals or dietary supplements should be explored in future research. Additionally, while not discussed here, other Rhodiola species, such as Rhodiola crenulata, may warrant investigation for potential ergogenic effects(Reference Abidov, Crendal and Grachev13,Reference Hou, Tang and Wang50) . Importantly, in addition to some trials not reporting the concentration of bioactive compounds within RR, most investigations do not include analytical confirmation of the purity of RR, even when concentrations of bioactive compounds are stated. As such, variation in the purity and true concentrations of bioactive components in RR supplements used in extant research could help explain divergent effects.
To conclude, RR has the potential to enhance performance and performance-related outcomes in several types of exercise; however, the current literature does not unanimously show ergogenic effects of supplementation with this plant. Variability in the supplementation dose and duration, concentrations of bioactive compounds, participant characteristics, exercise tests employed and statistical power may in part explain the disparate findings in the existing literature. While studies to date provide informative first steps, subsequent investigation of the potential ergogenic effects of RR will undoubtedly help clarify remaining questions regarding effects of RR based on supplementation protocol, exercise modality, exercise training status and more. The longstanding use of RR, the existing animal research and contemporary clinical trials in humans indicate that this botanical may have physiological effects that enhance exercise performance and related outcomes.
Acknowledgements
This work was financially supported by BioMolecular Athlete, LLC.
G. M. T., D. G. and A. J. G. formulated the research question; G. M. T. performed the literature search and wrote the initial version of the manuscript; G. M. T., A. R. J., G. D. M. P. and A. J. G. contributed to revisions of the manuscript; all authors read and approved the manuscript.
G. M. T. has received support for his research laboratory through research funding or in-kind gifts from nutrition and sports nutrition companies, including EHP Labs, Nutraceutical International Corporation, 8 POiNT LLC, Legion Athletics Inc., Vital Pharmaceuticals and MTI Biotech Inc. G. M. T. is the Owner of Tinsley Consulting LLC, which provides paid consulting services to dietary supplement manufacturers. A. R. J. has consulted with and received external funding from companies who sell certain dietary ingredients and also writes for online and other media outlets on topics related to exercise and nutrition. G. D. M. P. is a cofounder and shareholder of Resilient Nutrition. D. G. has a partnership with Momentous Supplements. A. J. G. is a paid scientific advisor for Momentous & XPT Life, is a founder of BioMolecular Athlete, LLC, RAPID Health & Performance, LLC, Absolute Rest, Inc. and is on the board of directors for the Health and Human Performance Foundation.


 Open access
Open access