



Psychological distress refers to a state of impaired mental health, commonly presented by nonspecific symptoms of stress, anxiety and depression(Reference Arvidsdotter, Marklund and Kylén1,Reference Viertiö, Kiviruusu and Piirtola2) . Psychological distress is quite common among adolescents – nearly 10 % to 20 % of adolescents globally suffer from various forms of psychological distress(3). Psychological distress can often lead to more serious mental health illnesses, including major depressive disorder and suicide. Suicide is responsible for an estimated 67 000 deaths among adolescents each year, which makes it the second leading cause of death among this group(4). Although psychological distress often starts in childhood and adolescence, its adverse effects continue beyond adolescence. Psychological distress is strongly related to other forms of mental illnesses, personality disorders, poorer quality of life and lower academic performance in adulthood(Reference Baranne and Falissard5,Reference Merikangas, Nakamura and Kessler6) .
Alongside, worldwide, a significant portion of adolescents are consuming various unhealthy and suboptimal diets, which is not only affecting their current health status but also increasing future risk of developing various noncommunicable diseases(Reference Anand, Hawkes and de Souza7,Reference Dahm, Chomistek and Jakobsen8) . Unhealthy dietary habits among adolescents are characterised by inadequate consumption of fruits and vegetables, higher intake of sugar-sweetened and carbonated soft drinks and energy-dense and nutrient-poor fast-foods(Reference Beal, Morris and Tumilowicz9,Reference Darfour-Oduro, Buchner and Andrade10) . Previous studies have shown that these dietary habits are associated with increased risk of obesity, diabetes and CVD(Reference Anand, Hawkes and de Souza7,Reference Dahm, Chomistek and Jakobsen8) . Since dietary habits are formed during adolescence and these habits are difficult to change in later life, dietary habits in adolescents warrant specific attention(Reference Movassagh, Baxter-Jones and Kontulainen11).
It has been hypothesised that individuals suffering from psychological distress might be more likely to consume unhealthy diets. The underlying biological mechanisms for the association between psychological stress and unhealthy dietary behaviours may include alterations in the hypothalamic–pituitary–adrenal axis, gut microbiome, glucose metabolism, insulin sensitivity and other appetite-related hormones and hypothalamic neuropeptides, which, in turn, potentiate reward sensitivity for hyperpalatable foods and consumption of higher energy foods(Reference Yau and Potenza12). However, disentangling relationships between mental health and unhealthy dietary behaviour is complex particularly due to their potential bidirectional nature. Although the causal roles of unhealthy dietary habits in mental health have not yet been established, inflammatory pathways associated with diets with high energies, trans fat and refined carbohydrates have been proposed as mechanisms through which unhealthy diets may increase the risk of mental health problems(Reference Firth, Gangwisch and Borsini13). Previous studies have shown some evidence on the associations between mental health problems and unhealthy dietary practices in adults(Reference Murakami and Sasaki14) as well as in young people(Reference Khalid, Williams and Reynolds15,Reference O’Neil, Quirk and Housden16) . Most of the evidence on such association among adolescents came from the developed countries, and there is a paucity in evidence coming from developing countries(Reference Khalid, Williams and Reynolds15,Reference O’Neil, Quirk and Housden16) . Previous studies have also showed that adolescent girls are more likely to suffer from mental health problems but adhere to healthier dietary behaviours than boys(Reference Otsuka, Kaneita and Itani17,Reference Kushal, Amin and Reza18) . Therefore, it is important to quantify potential sex differences in the burdens of psychological distress and unhealthy dietary behaviours. While some previous studies investigated the prevalence of mental health problems(19–Reference Hossain and Purohit21) and unhealthy dietary habits(Reference Rathi, Riddell and Worsley22–Reference Aguayo and Paintal25) in adolescents residing in South-East Asian countries, they were limited by nonrepresentative and smaller samples, and differences in variable definitions and analytic approaches made cross-country comparisons difficult. Moreover, to the best of our knowledge, no study examined the potential association between psychological distress and unhealthy dietary practices among adolescents from South-East Asian region. Understanding such relationship would be helpful for researchers and policy makers to design and implement interventions to improve mental health as well as dietary behaviours of adolescents.
Using country-representative samples from the Global School-based Student Health Survey (GSHS)(26) from nine South-East Asian countries, we aimed to (i) quantify the country-level prevalence of psychological distress and various unhealthy dietary habits among adolescents and then combine those estimates to get region-specific prevalence; (ii) investigate the associations between psychological distress and unhealthy dietary habits and (iii) assess any possible differences in the prevalence or association estimates by sex.
Methods
Data sources
We used the GSHS data collected between 2014 and 2016 from nine South-East Asian countries, namely Bangladesh, Bhutan, Indonesia, Maldives, Myanmar, Nepal, Sri Lanka, Thailand and Timor-Leste. Latest GSHS data from these countries had information on psychological distress variables and unhealthy dietary behaviours among school-going adolescents. In each participating country, the ethics approval for GSHS was taken from a national government administrative body or an institutional ethics review committee, or both. Informed written or verbal consent for participation in the survey was obtained from students and their parents or guardians. We used publicly available data from GSHS, so no separate ethics approval was required for this study.
The details about GSHS data have been described previously elsewhere(27) and summarised here. GSHS is a population-based survey for school-going adolescents conducted in many countries around the world with the support of WHO and the US Centers for Disease Control and Prevention and in collaboration with other international development partners. The main objective of these surveys is to help countries develop appropriate interventions and policies for promoting adolescent health and to facilitate cross-country comparisons for various adolescents’ behaviours and protective factors.
The GSHS uses the same methodology for sampling in each country. Participants from each country were selected using a standardised two-stage cluster sampling process. First, schools were selected using a probability-proportionate-to-size sampling method. Second, classrooms with students of target age group were randomly selected from these schools, and all students in the selected classrooms were asked to participate in the survey. The age range of participating students varied across these countries. We, therefore, restricted our analysis to adolescents aged 12–15 years because all countries had available data for this age range.
The GSHS used a validated questionnaire that was self-administered during one regular class period. Where necessary, the questionnaire was translated into an appropriate language using standard protocols and country-specific examples, options and phrases were used to incorporate socio-cultural adaptation(27).
Variable definitions
The definitions, questions and coding methods for the variables used in this study are shown in Supplementary Table S1. Following previous studies(Reference Amu, Seidu and Agbemavi28), investigating psychological distress, we defined ‘psychological distress’ based on five mental health variables available in the GSHS data – anxiety, loneliness, suicidal ideation, suicide planning and suicide attempt. The original responses to the survey questions for these variables were converted into dichotomous responses where 0 = no and 1 = yes. Adolescents with ‘yes’ response in two or more of these five variables were considered to have psychological distress.
The GSHS data had information on frequency of consumption of fruits, vegetables, soft drink and fast-food, and we defined four unhealthy dietary behaviours based these food items. For fruits and vegetables, we defined inadequate consumption if adolescents’ reported consumption was less than once per day. We also defined daily soft drink consumption and weekly fast-food consumption(Reference Beal, Morris and Tumilowicz9). However, there are no clear cut-offs for defining unhealthy dietary behaviours based on frequency of consumption of these foods. Therefore, we defined unhealthy dietary behaviours based on a previous global study on adolescents’ dietary habits(Reference Beal, Morris and Tumilowicz9).
We used several covariables in our study: age, sex, hunger (as a proxy for below average socio-economic status), having close friends, peer support, parental support, being bullied, smoking, physical activity and overweight. Detailed description of these variables and their coding are also presented in Supplementary Table S1.
Statistical analysis
We conducted data analysis following the instructions provided by the US Centers for Disease Control and Prevention(27). Using country-specific sampling weights, we computed weighted prevalence estimates for psychological distress and unhealthy dietary behaviours, overall and according to sex. The sampling weights accounted for non-response and the varying probability of selection of schools, classrooms and students in each survey. We used the exact method to compute 95 % CI for prevalence estimates. We then conducted random-effect meta-analysis using the ‘metaprop’ programme in Stata 16·0 to calculate pooled regional estimates of psychological distress and unhealthy dietary behaviours(Reference Kushal, Amin and Reza18). Random-effect meta-analysis was used because of substantial heterogeneity in prevalence estimates among countries, as indicated by I2 > 95 %.
To investigate the association between psychological distress and unhealthy dietary behaviours, we got country-specific OR with 95 % CI by conducting separate multivariable logistic regressions for each country and then we pooled the OR by using random-effect meta-analysis in ‘meta’ programme in Stata 16.0. Multivariable logistic regressions were adjusted for age, sex, hunger, close friends, peer support, parental support, being bullied, smoking, physical activity and overweight. We looked at the associations separately among boys and girls to explore whether there were any sex-specific differences in those associations. We examined the associations of individual psychological variable with unhealthy dietary behaviours. Furthermore, we divided the adolescents into six groups (0 to 5) based on the number of psychological distress variable present and then examined at the associations by using those with no presence of psychological distress factor as the reference category.
We also explored any further potential for effect modification by various factors for the associations between psychological distress and unhealthy dietary behaviours by comparing OR across sub-groups of those factors and tested for heterogeneity by likelihood ratio tests comparing models with and without cross-product interaction term.
Participants who had valid information on the variables denoting psychological distress were included in the analysis. Missing or non-applicable values for covariables were treated as a separate category. We did sensitivity analysis restricting to participants who had valid information for all variables and found no substantial differences (data not shown). Statistical significance was set at a two tailed P < 0·05.
Results
We included GSHS data sets from nine South-East Asian countries, with 30 013 adolescents (56 % girls) aged 12–15 years in this analysis. Table 1 shows the characteristics of included surveys. The sample size ranged between 1509 from Timor-Leste and 8523 in Indonesia. The mean age of all participants across nine countries was 13·8 (sd 1·0) years, and there was no substantial between-country difference in adolescents’ mean age.
Table 1. Characteristics of included surveys

Figure 1 shows the correlation matrices for psychological distress and unhealthy dietary behaviours variables. We observed weak to moderate positive correlations for the five psychological distress variables, suggesting that each of them represents a slightly different aspect of psychological distress. For dietary behaviours, we found both positive and negative correlations, but those correlations were very weak.

Fig. 1. Correlation matrices for psychological distress and unhealthy dietary behaviours variables. The colour gradient goes from blue to red, with smaller correlation coefficients represented as blue and larger correlation coefficients represented as red.
Prevalence of psychological distress
Overall, 11·0 % (95 % CI: 8·1, 13·9) adolescents had psychological distress, with girls reporting slightly higher than boys (11·8 % v. 10·1 %) (Table 2). The prevalence of psychological distress was higher among girls than boys in all countries except Timor-Leste. Adolescents in Indonesia reported the lowest prevalence (5·1 %) of psychological distress, while those in Maldives reported the highest prevalence (20·2 %). When we looked at the prevalence separately for boys and girls, Indonesia and Maldives, respectively, had the lowest and highest sex-specific prevalence (Table 2). We also presented the prevalence of individual items in psychological distress in Supplementary Table S2. The pooled prevalence for loneliness, anxiety, suicide ideation, suicide planning and suicide attempt was 9·1 %, 5·8 %, 9·0 %, 10·1 % and 7·8 %, respectively. Compared with boys, girls were more likely to have loneliness (9·8 % v. 8·0 %), anxiety (6·4 % v. 4·9 %), suicide ideation (9·5 % v. 8·4 %), suicide planning (10·4 % v. 9·7 %) and suicide attempt (7·9 % v. 7·7 %).
Table 2. Prevalence of psychological distress among adolescents aged 12–15 years, pooled and by country*
(Prevalence and 95 % confidence intervals)
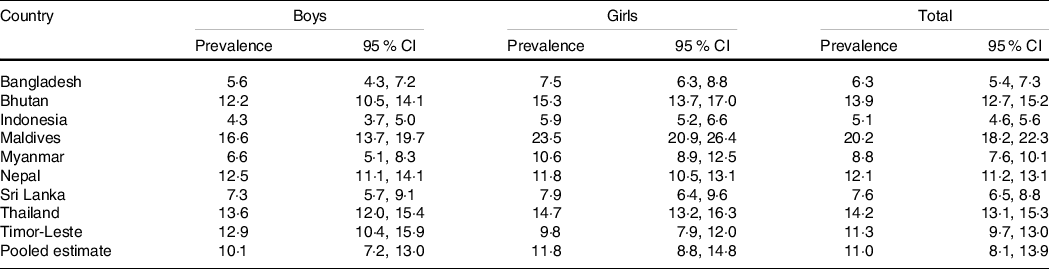
* Country-specific sampling weights were used to yield country representative estimates.
Random-effect meta-analysis was used to calculate the pooled prevalence estimates.
Prevalence of unhealthy dietary behaviours
The pooled prevalence of inadequate fruit intake among South-East Asian adolescents was 41·6 % (Table 3). However, the pooled prevalence of inadequate vegetable intake was much lower (25·7 %) than inadequate fruit intake. Adolescents in Maldives had the highest prevalence of both inadequate fruit intake (59·1 %) and inadequate vegetable intake (59·8 %). The prevalence of inadequate fruit and inadequate vegetable intake was the lowest in Thailand (23·9 %) and Sri Lanka (10·1 %), respectively. Nearly 40 % adolescents in these countries consumed soft drink daily, with those in Thailand (56·4 %) consumed the most and those in Sri Lanka consumed the least (26·3 %). For weekly fast-food consumption, Thailand had the highest prevalence (79·3 %) and Maldives had the lowest prevalence (33·7 %). Bhutan and Myanmar did not have information on fast-food consumption, and the pooled prevalence for rest of the countries was 57·4 %. We did not observe significant differences between boys and girls for these unhealthy dietary behaviours (Table 3).
Table 3. Prevalence of unhealthy dietary behaviours among adolescents aged 12–15 years, pooled and by country*
(Prevalence and 95 % confidence intervals)
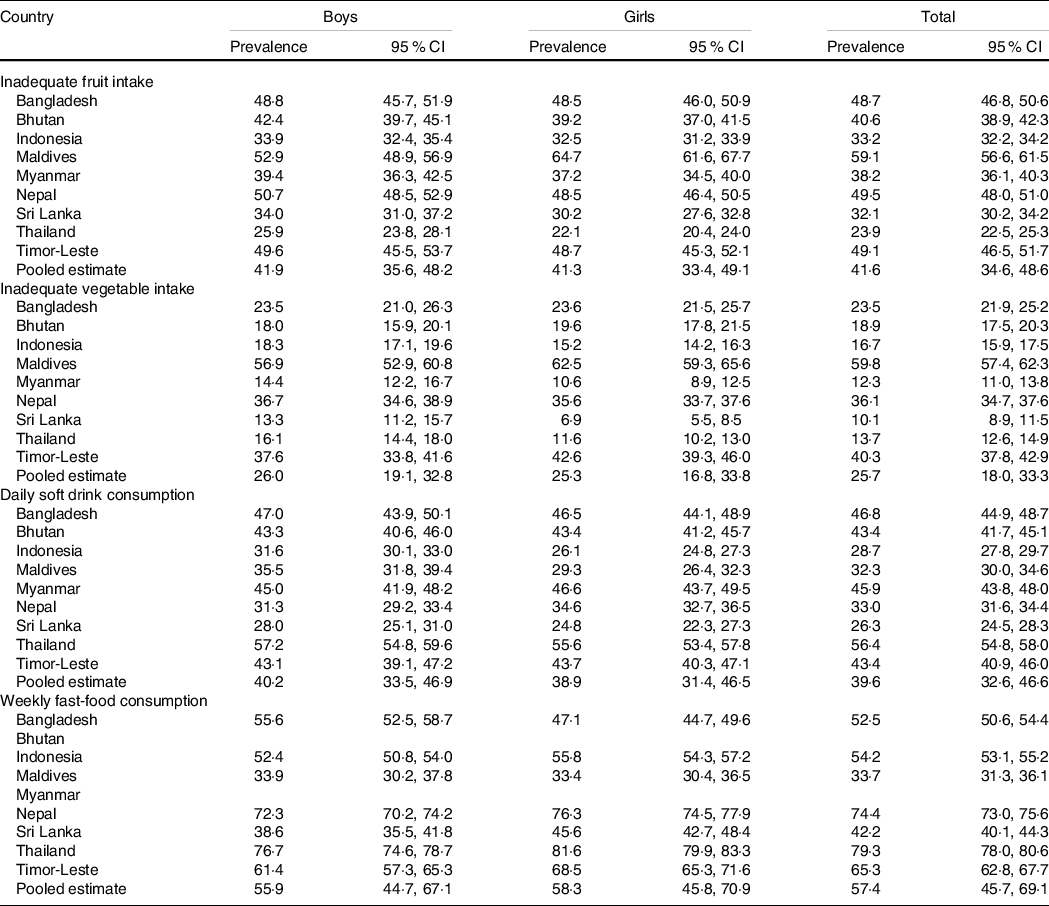
* Country-specific sampling weights were used to yield country representative estimates.
Random-effect meta-analysis was used to calculate the pooled prevalence estimates.
Associations between psychological distress and unhealthy dietary behaviours
Figure 2 shows the overall and country-specific associations between psychological distress and unhealthy dietary behaviours. Overall, psychological distress was associated with inadequate fruit intake (pooled OR = 1·20, 95 % CI 1·03, 1·40), inadequate vegetable intake (pooled OR = 1·17, 95 % CI 1·05, 1·31) and daily soft drink consumption (pooled OR = 1·14, 95 % CI 1·03, 1·26); but not with weekly fast-food consumption (pooled OR = 1·13, 95 % CI 0·96, 1·31). We observed significant heterogeneity for country-specific OR for the associations between psychological distress and unhealthy dietary behaviours. When we looked at the associations separately among boys and girls, we found that psychological distress was significantly associated with inadequate vegetable intake and daily soft drink consumption among boys (online Supplementary Fig. S1), whereas psychological distress was only associated with inadequate fruit intake among girls (online Supplementary Fig. S2). Supplementary Figures S3–S7 show that loneliness was associated with inadequate fruit intake; anxiety was associated with inadequate fruit intake and daily soft drink consumption; suicide ideation was associated with inadequate vegetable intake; suicide planning was associated with inadequate fruit intake, inadequate vegetable intake and daily soft drink consumption and suicide attempt was associated with inadequate vegetable intake, daily soft drink consumption and weekly fast-food consumption. In sub-group analysis, we found that the observed associations were consistent in each level of various factors, and there was no significant heterogeneity (Fig. 3).
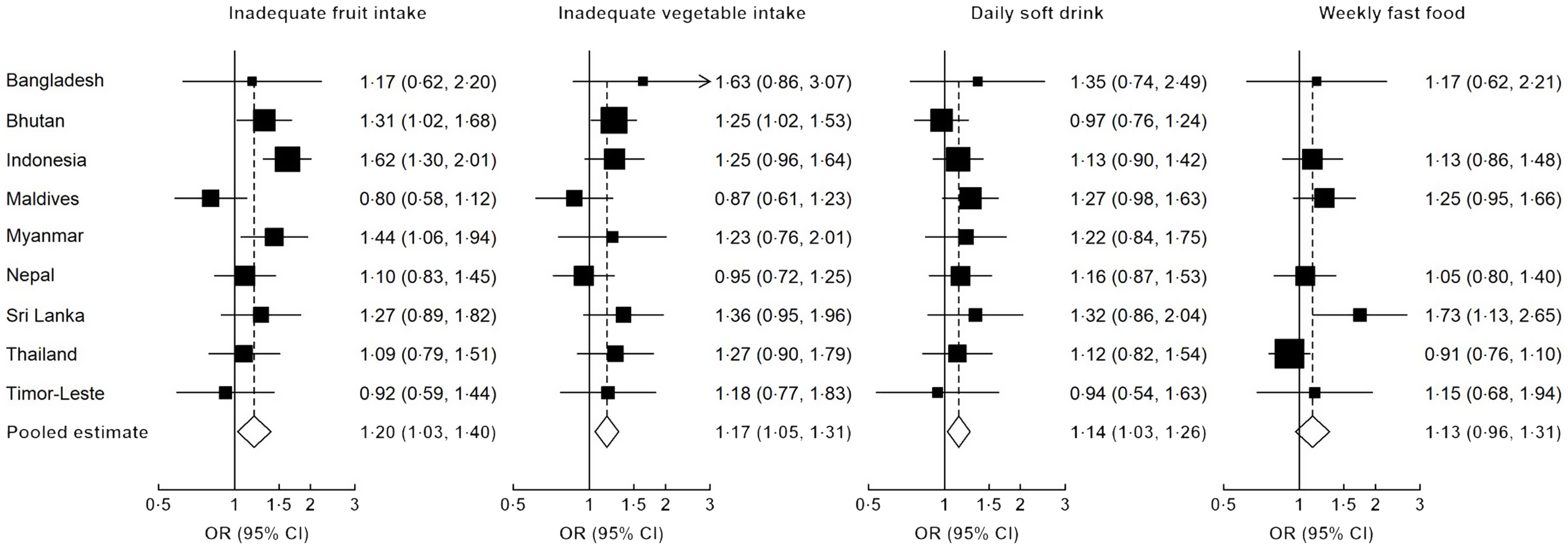
Fig. 2. Associations between psychological distress and various unhealthy dietary behaviours among adolescents. We used multivariable logistic regression models to estimate country-specific OR and then conducted a random-effect meta-analysis to pool the OR. Regression models were adjusted for age, sex, proxy for low socio-economic status, peer support, parental support, bullying, having close friends, smoking, physical activity and overweight.
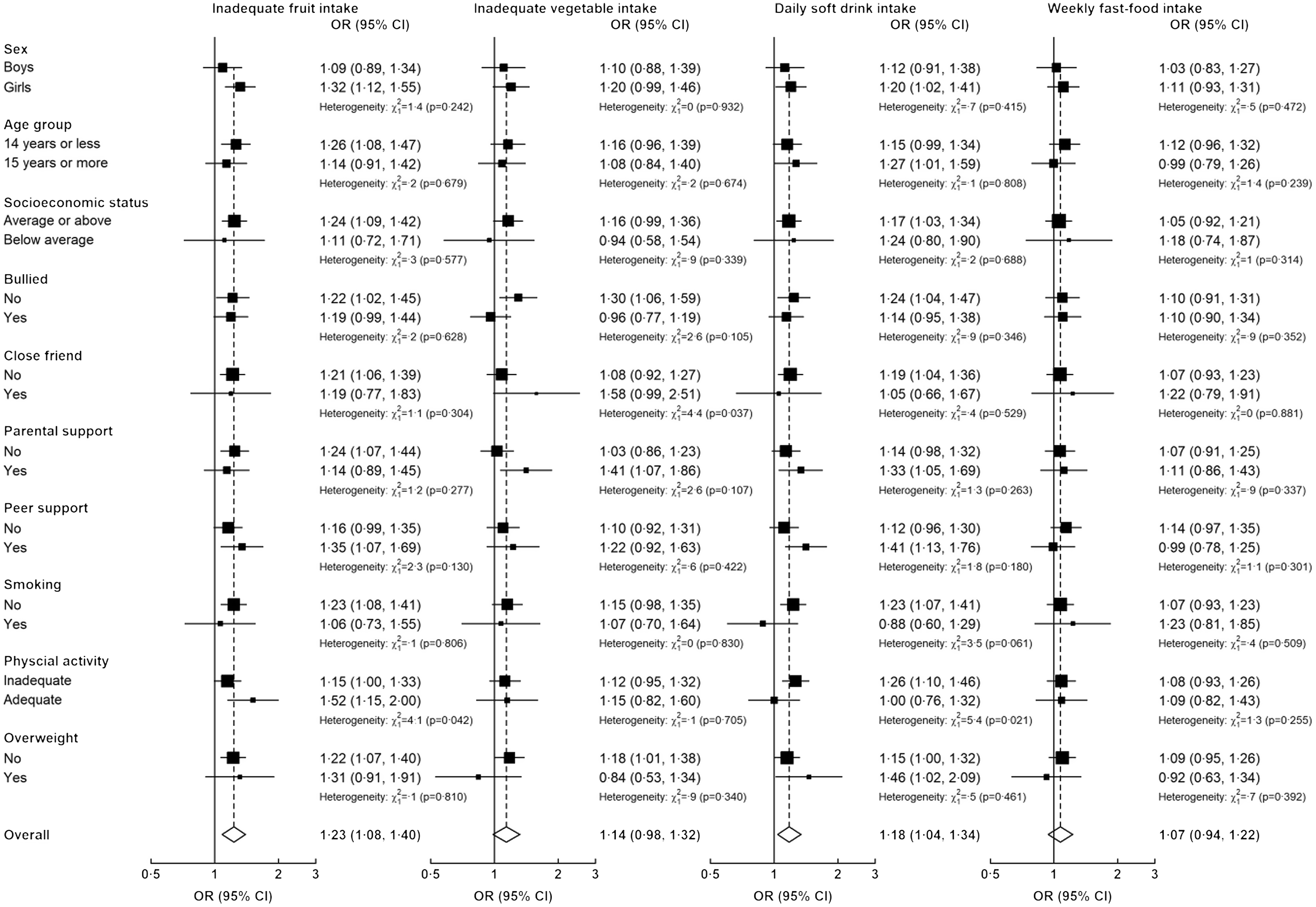
Fig. 3. Associations of psychological distress with unhealthy dietary behaviours among South-East Asian adolescents, in various subgroups. Models were adjusted for age, sex, low socio-economic status, survey year, region, bullying, close friend, parental support, peer support, smoking, physical activity and overweight, as appropriate. Heterogeneity between groups was tested by likelihood ratio tests comparing models with and without cross-product interaction term.
To understand whether the odds of unhealthy dietary habits increased with having increasing number of psychological distress variables, we divided the adolescents into six groups (0 to 5) and looked at the associations by using those with no presence of psychological distress factor as the reference category (Fig. 4). We found that although not all associations reached significance level, there were increasing odds of consuming inadequate fruit, inadequate vegetable and daily soft drink with presence of higher number of psychological distress factors.
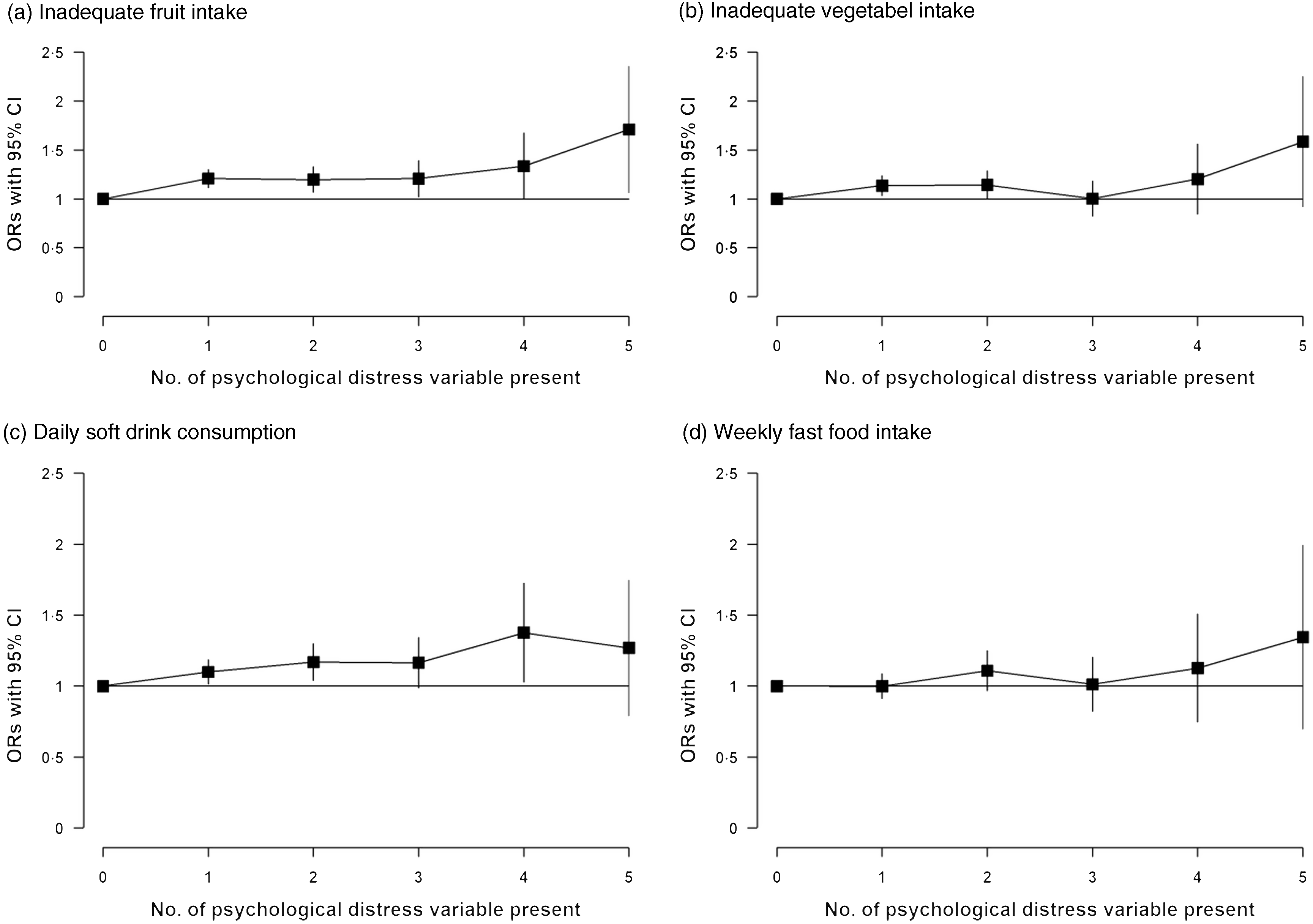
Fig. 4. OR for various unhealthy dietary behaviours according to number of psychological distress variable present in adolescents. We used multivariable logistic regression models with adjustment for age, sex, proxy for low socio-economic status, peer support, parental support, bullying, having close friends, smoking, physical activity and overweight. Those with no psychological distress variable were considered the reference group.
Discussion
To the best of our knowledge, this is one of the first studies examining the association between psychological distress and unhealthy dietary behaviours among adolescents in the South-East Asian region. Our study revealed that (i) nearly one in ten adolescents had psychological distress, and the prevalence of inadequate fruit intake, inadequate vegetable intake, daily consumption of soft drink, and weekly consumption of fast-food was 42 %, 26 %, 40 %, and 57 %, respectively; (ii) although girls had slightly higher prevalence of psychological distress than boys, no substantial sex differences were observed for various dietary behaviours and (iii) psychological distress was significantly associated with inadequate fruit intake, inadequate vegetable intake and daily soft drink consumption, and the associations were consistent across various socio-demographic, psychosocial and lifestyle factors.
We provided a comprehensive assessment of adolescents’ psychological distress by looking at different aspects, such as loneliness, anxiety, suicide ideation, suicide planning and suicide attempt. Our study confirms that there is a substantial burden of psychological distress among adolescents living in South-East Asia, and the burden varies widely across countries. Previous studies also reported high burden of common mental problems among children and adolescents in South-East Asia(19–Reference Hossain and Purohit21). However, results from those studies are not directly comparable to our findings, particularly because they used different definitions for such measures. The variations in the prevalence of psychological distress across countries may be due to varying levels of psychological, cultural, economic, religious and political stressors(Reference Naveed, Waqas and Chaudhary20). We found that girls were more likely to have psychological distress than boys, and this is in line with previous research exploring sex differences for mental health problems among adolescents(Reference Kushal, Amin and Reza18). Previously, we showed that the prevalence of any suicidal behaviour among adolescent boys and girls in this region was 16·1 % and 16·9 %, respectively(Reference Kushal, Amin and Reza18). A study based on adolescents from seventy-three OECD countries showed that adolescent girls had worse psychological distress than boys(Reference Campbell, Bann and Patalay29). The observed gender difference in psychological distress might be due to higher levels of internalising problems, domestic and sexual abuse(Reference Campbell, Bann and Patalay29,Reference Elliott30) . Furthermore, balancing between multiple gender norms (participation in academic and economic activities v. maintaining female identity and appearances) can induce more anxiety among girls than boys(Reference West and Sweeting31).
We looked at different aspects of unhealthy dietary behaviours among adolescents. Our results showed that adolescents in South-East Asia region were less likely to eat inadequate quantity of fruits and vegetables, with no substantial sex differences. Although we could not measure the actual quantity of fruits and vegetable consumption, we looked at the frequency of consumption and used cut-offs from a previous global study on dietary behaviours(Reference Beal, Morris and Tumilowicz9). However, since the overall frequencies of fruit and vegetable consumption were low, consumption in all countries was likely below the minimum recommended amount (at least 400 g) by the WHO. Previous studies from this region have reported that a significant proportion of adolescents do not consume adequate quantities of fruits and vegetable, but the results are not directly comparable because of different definitions and measures(Reference Rathi, Riddell and Worsley22–Reference Aguayo and Paintal25). A previous global study reported that compared with other WHO regions, the mean daily consumption of fruit among adolescents from South and East Asia was higher, whereas the mean daily consumption of fruits was lower(Reference Beal, Morris and Tumilowicz9). Our findings also highlighted that the percentages of adolescents consuming inadequate fruits was much higher than the percentages of adolescents consuming inadequate vegetables in all countries. The reasons for inadequate fruits and vegetable consumption include but not limited to – supply issues, financial concerns, urbanisation-induced price inflation and changes in food shopping patterns(Reference Cheung, Lok and Gietel-Basten32). Many previous studies examining adolescents’ dietary behaviours did not include estimates for carbonated soft drinks and fast-food consumption. It was evident from our results that a large portion of adolescents in this region were consuming soft drinks and fast-food. We found that adolescents residing in Thailand and Nepal had particularly high prevalence of consuming fast-food at least once weekly. This might be due to wide availability of street foods and fast-food restaurants in those countries. Due to the impacts of globalisation and McDonaldization (i.e. adopting the cultures of fast-food restaurant) in the digital age, food environments in South-East Asian countries are shifting rapidly(Reference Ritzer and Miles33).
Our study shows that adolescents suffering from psychological distress are more likely to have unhealthy dietary behaviours – low consumption of fruits and vegetables and high consumption of carbonated soft drinks. Some previous studies examined the associations between mental health problems and diet among children and adolescents(Reference Oddy, Robinson and Ambrosini34–Reference Mooreville, Shomaker and Reina36). A study conducted among Chinese adolescents found a positive association between consumption of soft drinks and sweet food and risks of suicidal behaviours(Reference Pan, Zhang and Shi37). It has also been found that ‘Westernised’ eating patterns can be linked to an increased risk of developing psychological distress(Reference Oddy, Robinson and Ambrosini34–Reference Mooreville, Shomaker and Reina36). We found substantial heterogeneity across countries for the observed associations, which highlights the importance of avoiding ‘one size fits all’ approach while designing public health and clinical interventions to tackle these problems. More research is needed to explore the potential roles of socio-cultural, political, religious and economic factors on these associations. Also, further research should assess the impacts of integrated school and family intervention programmes to inform policy and related public health actions.
Elucidating the relationships between mental health problems and diet among is complex(Reference Khalid, Williams and Reynolds15). Previous studies have suggested that the relationship is potentially bidirectional and can be confounded by a wide range of factors, including age, sex, socio-economic status and other social and cultural practices(Reference Khalid, Williams and Reynolds15,Reference O’Neil, Quirk and Housden16) . While it can be hypothesised that psychological distress can lead to poorer dietary habits, others can argue that poorer diet possibly can cause psychological distress. Recent systematic reviews found that there is an association between unhealthy dietary pattern and worsening of mental health in children and adolescents(Reference Khalid, Williams and Reynolds15,Reference O’Neil, Quirk and Housden16) . Although causality for such association cannot be ascertained, low mood can lead to increased consumption of unhealthy foods like fast food, chocolates and decreased consumption of healthy foods. Future research should deal with methodological issues to delineate the cause from effect.
Our study has several strengths. First, our study is the first study to include a large number of adolescents from nationally representative samples from nine South-East Asian countries. We also presented country-specific prevalence estimates weighted for probability of selection and age–sex distributions in each country. These steps will facilitate generalisation of our prevalence estimates to each country’s population. By restricting our analysis to surveys conducted between 2014 and 2016, we are confident that our cross-country comparisons are less likely to be driven by period effect. Second, the GSHS followed the same standardised methods in each participating country, while we used the same definitions for exposure and outcome variables. Therefore, the cross-country comparisons in our study are more likely to be valid. Third, we used random-effects meta-analysis to pool the country-specific prevalence estimates and OR to allow for differences in those estimates from country to country. Fourth, we investigated the associations between psychological distress and unhealthy dietary behaviours with adjustment for a wide range of confounders as well as explored any further potential for effect modification by sex.
While these are clear strengths of our study, there are also several limitations. We defined psychological distress among adolescents based on self-reported data on five mental health variables, according to a previously published study(Reference Amu, Seidu and Agbemavi28). We acknowledge that the conceptualisation of a complex phenomenon like psychological distress can still be incomplete. We defined unhealthy dietary behaviours based on the self-reported frequency of food in the previous 30 d instead of quantities (i.e. servings) consumed. Previous studies showed that recall of food frequency was less valid than 24-h recall(Reference Beal, Morris and Tumilowicz9). Additionally, data on fast food consumption were not available for Bhutan and Myanmar. However, by looking at the other three dietary behaviours, we can assume that fast food consumption in these two countries should not be widely different. Self-reported measures can also introduce reporting bias, for example reporting about mental health problems is considered as taboo in some countries and cultures(Reference Gopalkrishnan38). These issues might warrant careful comparison of our findings to other studies’ findings. The GSHS data are based on responses from school-going adolescents who might have different attributes than those who do not attend school. However, majority of the included countries generally have very high enrolment rate for secondary school. Due to the cross-sectional nature of our data, we could not establish the temporality of the observed associations between psychological distress and unhealthy dietary behaviours. Although we adjusted for several factors in our analyses, there might be residual confounding in the observed associations, particularly for socio-economic status. We used hunger as proxy for low socio-economic status because several previous studies based on GSHS used such measure(Reference Kushal, Amin and Reza18,Reference Biswas, Scott and Munir39) . Therefore, our results should be interpreted with cautions.
In conclusion, our study highlights significant high burdens of psychological distress and unhealthy dietary behaviours (e.g. low consumption of fruits and vegetables intake and high consumption of carbonated soft drinks and fast foods) among adolescents in South-East Asian region, with wide variability across countries. While adolescent girls were more likely to suffer from psychological distress, there was no significant sex difference for unhealthy dietary behaviours. Adolescents with psychological distress have increased likelihood of following unhealthy dietary behaviours, which was consistent across various factors. Our findings will help to shape public health interventions reducing the burdens of mental health and unhealthy diet among adolescents in South-East Asian region. Estimates for individual country will promote country-specific resource allocation and support relevant policies. Future research should examine the directionality of this association and any specific dietary deficits among adolescents suffering from psychological distress to guide preventative interventions and inform relevant policies.
Acknowledgements
This paper uses data from the Global School-Based Student Health Survey (GSHS). GSHS is supported by the WHO and the US Centers for Disease Control and Prevention’.
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
M. S. has the full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. M. S. and F. H. were involved in study concept and design. M. S. involved in statistical analysis and interpretations of results. E. J. and R. R. conducted relevant literature search and review. M. S., E. J. and R. R. were involved in drafting of the manuscript. M. S. and F. H. were involved in critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript. The authors have no conflicts of interest to disclose.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114522002306









