


Maternal nutrition is a fundamental determinant of fetal growth, birth weight and infant morbidity; poor nutrition often leads to long-term, irreversible and detrimental consequences to the fetus( 1 ). Although government policies and programmes in Indonesia address nutrition among children (<5 years) and pregnant women (PW), 12·3 % of the Indonesian women are yet underweight( 2 ). The prevalence of anaemia and chronic energy deficiency in women (>15 years old) is 19·7 and 13·6 %, respectively( 3 ). Among Indonesian PW, anaemia and micronutrient deficiencies (folic acid, Zn, vitamin A, vitamin B12) are quite high (40–50 %), which may lead to poor pregnancy outcomes. Earlier studies from Indonesia have shown an inadequate intake of food and several nutrients by PW( Reference Hartriyanti, Suyoto and Muhammad 4 – Reference Prihartini, Jahari and Sebayang 6 ). Women are undernourished in the first trimester of the pregnancy and have an insufficient weight gain during pregnancy (79 %)( Reference Winkvist, Stenlund and Hakimi 7 ). Nutritional status during pregnancy not only puts the mother ‘at risk’ but is also a risk factor for the infant being born with low birth weight (LBW: 9–11 % in Indonesia)( Reference Requejo, Bryce and Lawn 8 ).
There are limited recent data on the nutritional status of women of reproductive age in Indonesia. Thus, the aim of the present cross-sectional study conducted in Bogor municipality, West Java, Indonesia, was to obtain data on food patterns, nutrient intakes and nutritional status of pre-pregnant women (PPW) and PW and to investigate whether and to what extent they differ. The secondary aim was to compare the intakes of the women across different economic quintiles (Q).
Methods
The present cross-sectional study was conducted in the six sub-districts of Bogor city: north, west, south, east and central Bogor and Tanah Sareal. Ethics approval for the study was granted by the Health Research Institute at the Ministry of Health (No. LB.03.02/KE/6433/2010). The data were collected between January and May 2011 by study assistants with an educational qualification in community nutrition and previous experience in conducting nutritional surveys. They were further trained in the methods utilised in the present study.
Eligible PPW and PW were randomly selected from the records available at the participating integrated community services posts (Pos Pelayan Terpadu; POSYANDU) covering the various regions of Bogor district and contacted by study field workers, after having obtained permission from the respective public health centres (Pusat Kesehetan Masyarakat; PUSKESMAS) with equal representation out of the six sub-districts: west, north, south, east and central Bogor and Tanah Sareal. Non-PW in the age group of 20–40 years, not suffering from any chronic disease affecting their dietary intake pattern and without any acute morbidity condition on the day of survey, married and not committed to any form of family planning or aware of infertility were considered as women preparing for pregnancy and were recruited to the PPW group. Similarly, PW free from any disease either pregnancy related or non-pregnancy related with gestational age between 13 and <28 weeks were recruited to the PW group. The second trimester was preferred for our study as physiological changes are more pronounced compared with the first trimester and compliance to our protocol and procedures during the third trimester were expected to be less good. The household expenditure was used to obtain proxy information on the socio-economic status, thus classifying the women into their appropriate Bogor district household expenditure quintiles (HHEQ)( 9 ): HHEQ-2: 250–330 000, HHEQ-3: 330–430 000 and HHEQ-4: 430–620 000 IDR/cap per month. These levels mainly cover the wider ‘middle-income’ group, representing 60 % of the households in Bogor district: HHEQ-2, clearly lower middle income and HHEQ-4, clearly higher middle income. We did not study women in the lowest and in the highest quintiles of household expenditure, because in our pre-study we experienced a clearly lower willingness to comply with our protocol and procedures among these groups. Women qualifying for HHEQ-2–4 and meeting the inclusion/exclusion criteria were enrolled for the study. A total of 221 PPW and 220 PW were approached to obtain verbal consent to participate in the study. In all, 200 PPW and 203 PW participated in the study. In addition, written consent to have a blood sample drawn to assess biomarkers for micronutrient status was obtained from both forty-five PPW and PW equally divided into the three HHEQ.
A pre-tested semi-structured close-ended questionnaire was administered to each enrolled woman to obtain information on socio-demographic profile (age, education, occupation and family size), dietary intake and anthropometric profile.
Anthropometric measurements of mid-upper-arm circumference (MUAC) and weight from the participating PPW and PW were obtained by the study field workers using standard methodology( Reference Gibson 10 ). We used a MUAC cut-off value of <23·5 cm and maternal weight <45 kg as risk indicators for poor pregnancy outcomes( Reference Sebayang, Dibley and Kelly 11 , Reference Ververs, Antierens and Sackl 12 ).
A semi-quantitative FFQ was administered to assess the frequency and amount of intake of different food groups during the past 1 week. The frequency of consumption of foods from eight major food groups was collected: (1) cereal and cereal products; (2) meat/poultry and their products; (3) fish and fish products; (4) egg and egg products; (5) milk and dairy products; (6) legumes and their products; (7) vegetables and their products; and (8) fruits and their products. Indonesian women have a significant intake of intermittent snack foods. Thus, snacks and beverages were added to the list of the above-mentioned eight food groups.
Two daily dietary intake data sets were collected utilising the 24-h dietary recall method( Reference Gibson 10 ). Intake was calculated using the food composition data from the Indonesian Food Composition Table (IFCT) (2004 and 2008)( 13 , Reference Mahmud, Zulfianto and Apriyantotono 14 ) as a leading source. In case items not covered in the IFCT were consumed, other food composition databases such as NutriSurvey( 15 ) were used. Country-specific nutrient intakes issued in 2004 were considered as the reference recommendations( 16 ) for the study group. Women with energy and protein intakes <70 % of the recommended levels were classified as having clear deficient intakes( 17 ). Women with micronutrient intakes (Fe, Ca, Zn, vitamin A, vitamin C) <77 % of the recommended levels as a proxy for estimated average requirements (EAR) were considered as having ‘deficient intakes’( Reference Gibson 10 ). PW were also asked about their intake of supplements, but nutrient intakes from supplements were not included in our analysis.
Blood samples (10–12 ml) for biochemical analyses were obtained from a subset of women (forty-five PPW and PW each) to assess selected micronutrient status. Women were invited to the central laboratory Prodia, Bogor City, for drawing blood from the antecubital vein. Samples were stored at −80°C until analysis. Hb, serum ferritin, serum retinol and serum Zn levels were analysed using the cyanmethemoglobin method( 18 ), chemiluminescent immunoassay( 19 ), HPLC( 20 ) and atomic absorption spectrophotometry( Reference Kruse-Jarres, Rükgauer and Schmitt 21 ), respectively. C-reactive protein (CRP) was measured using immunoturbidimetry, and was used as an indicator of inflammation. Ferritin values from samples with CRP>5 mg/l were excluded from further analysis. Analysis was performed within 6 months of blood collection.
To detect a meaningful difference of about 20 % in any nutrient deficiency, a typical sample size of 100 subjects/group is commonly used. Our comparison between total PPW and PW among all 200 subjects is clearly over-powered and using three individual HHEQ (n 65) may be somewhat under-powered, but still meaningful. Owing to wide variations in similar surveys, we considered it not to be very helpful to apply whatever formulas and choose rather arbitrary distribution characteristics. The number of forty-five PPW and PW for biochemical analysis reflected a practical limitation. We made sure that the three HHEQ were equally distributed among these women, but did not carry out a separate analysis. All the data were entered into a database and double-checked for any possible keyboard error. Data analysis was carried out using SPSS 17.0 for Windows. We used descriptive analysis (percentages, medians and interquartile ranges (IQR) of nutrients) on demographic characteristics including age, education level, household income, income per capita, family size, nutritional status, food consumption and nutrient intake. To compare food consumption and nutrient intakes between HHEQ, we first applied ANOVA testing and subsequently compared HHEQ-2 with HHEQ-4 using the Mann–Whitney test in non-normally distributed data sets and the t test when both data sets were normally distributed. Medians and IQR levels were reported instead of mean values and standard deviations due to the wide variability and non-normal distributions in the data. Results were considered statistically significant at 5 % level of significance.
Results
All women had at least basic education. Most of the women (80 %) were housewives. All women, except one, had attended primary school with a higher percentage in HHEQ-4 having tertiary education. Education and family size distribution are given in Table 1. Other background variables such as occupation and education level of the husband, current minor health discomfort and recent infectious diseases were also recorded and provided a similar picture according to differences in socio-economic status. Almost 12·5 and 18·3 % of the PPW and PW, respectively, were chronic-energy-deficient women based on MUAC (<23·5 cm). Weight measures revealed that 15·5 and 9·9 % of PPW and PW weighed <45 kg, respectively, indicative of increased risk of LBW in Asian countries regardless of gestational age( Reference Ververs, Antierens and Sackl 12 ). BMI among the PPW revealed that 14 % of them were underweight (BMI<18·5 kg/m2), whereas 31 % of them were overweight/obese (BMI>25·0 kg/m2). As for many PW, we had no accurate record on pre-pregnancy weight; BMI was not calculated for PW (Table 1).
Table 1 Background characteristics and the anthropometric profile of enrolled study subjects (Numbers and percentages; medians and interquartile ranges (IQR))

Q, quintiles; PPW, pre-pregnant women; PW, pregnant women; MUAC, mid-upper-arm circumference.
FFQ showed that cereals (mainly rice and their products) and beverages were consumed by all women across the HHEQ. Legumes, vegetables and fish consumption was an inherent part of the women’s daily diet; overall >70 % consumed these foods and their products. Overall, more PW (57 %) consumed milk (and dairy products) as compared with the PPW (26 %). Similarly, more PW (40 %) consumed fruits as compared with the PPW (26 %). Consumption patterns of legumes and vegetables (and their products) were similar among the two groups of women, whereas consumption pattern of poultry showed higher values among PPW compared with PW (45 v. 35 %).
With respect to HHEQ, consumption pattern of poultry and milk showed an economic gradient. The consumption pattern of fruits was least frequent among women in the lowest HHEQ (both groups). Consumption pattern of fish decreased with increasing HHEQ among PW. Snacking was highly prevalent among both groups of women. Typically, for Indonesia, more than 80 % of the women across all studied HHEQ consumed home-made and manufactured snack foods.
The total amount of food intake increased with increasing HHEQ. Cereals were the largest amount of solid food consumed by women. Comparing cereal intake, no significant difference was observed between PW and PPW despite the different physiological conditions (P=0·42). Median intake of milk was significantly higher among PW (P=0·01). Similarly, intakes of vegetables and fruits were greater among PW. Upon increasing HHEQ, PPW had a significant increase in cereals and meat/poultry intakes (P<0·05) and a trend for significance (P=0·06) for increasing vegetable consumption. For PW, a significant increase upon HHEQ was found for milk and dairy products (P<0·05) and a trend for meat/poultry, eggs and legumes (P=0·05–0·10). These relationships according HHEQ for PPW and PW were confirmed by comparing HHEQ-2 with HHEQ-4. Overall, PW consumed more snack foods compared with PPW (P<0·05), and the median amounts of snack food intake increased with increasing HHEQ (Table 2).
Table 2 Daily intake of different food groups (g) by women across socio-economic layers (Medians and interquartile ranges (IQR))

HHEQ, household expenditure quintiles; PPW, pre-pregnant women; PW, pregnant women.
* Statistically significant trend according to HHEQ (P<0·05) using ANOVA test.
† Statistically different between Q2 and Q4 (P<0·05) using t test.
‡ Statistically different between Q2 and Q4 (P<0·05) using Mann–Whitney test.
§ Statistically different between PPW and PW (P<0·05) using Mann–Whitney test.
Median protein intake was similar in the two groups of women, whereas median energy intake was higher among the PW (significant only in HHEQ-2: P<0·05). Energy and protein intakes increased with economic gradient (Table 3). Almost half of the PW and 45 % of the PPW were having inadequate energy intakes (<70 % RDA) (Fig. 1). Overall, 24 and 44 % of the PPW and PW, respectively, had combined deficiency of energy and protein (data not shown). Among PPW, there was no significant difference in energy intake between overweight/obese PPW (BMI≥25·0 kg/m2) v. normal BMI women (BMI 18·5–<25·0 kg/m2). Protein quality in the current context is considered as the proportion of protein derived from animal foods. We found median proportions between 31 and 44 % in the studied HHEQ of PW and PPW. Among PW (HHEQ-2), only 31 % protein was derived from animal sources, and in PPW of HHEQ-2 and HHEQ-3 only 35 and 32 % of protein was from animal sources (data not shown).
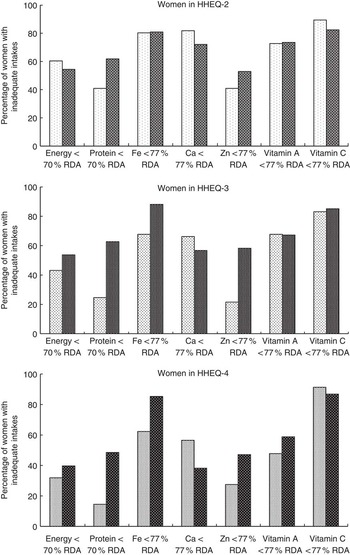
Fig. 1 Nutrient deficiencies among women enrolled in the study according to household expenditure quintile (HHEQ). Cut-off point 70 % RDA for energy and protein according to Ministry of Health (Indonesia)(
17
); cut-off point 77 % RDA for micronutrients according to estimated average requirement estimate(
Reference Gibson
10
). ![]() , Pre-pregnant women;
, Pre-pregnant women; ![]() , pregnant women.
, pregnant women.
Table 3 Nutrient intakes of pregnant (PW) and pre-pregnant women (PPW) (Medians and interquartile ranges (IQR))

AKG, Angka Kecukupan Gizi – Country-Specific Nutrient Recommendations for Indonesia; HHEQ, household expenditure quintiles; RE, retinol equivalents.
* Requirements for energy and Zn are age specific.
† Statistically different between PPW and PW (P<0·05) using t test.
‡ Statistically significant trend according to HHEQ (P<0·05) using ANOVA test.
§ Statistically different between Q2 and Q4 (P<0·05) using t test.
|| Statistically different between Q2 and Q4 (P<0·05) using Mann–Whitney test.
¶ Statistically different between PPW and PW (P<0·05) using Mann–Whitney test.
Overall, median intake of Fe and Zn was similar among the two groups of women. More than 80 % of the PW were having an inadequate dietary Fe intake. Median dietary Zn intake among the PPW (except for HHEQ-2) showed that the intake was more than the recommendations. In PPW, there was a significant difference in Fe and Zn comparing HHEQ-2 with HHEQ-4 (Table 3). Ca intake was significantly higher among the PW (P<0·05) and its intake showed an economic gradient in PPW (P<0·05). Upon comparing HHEQ-2 with HHEQ-4, a significantly higher intake was found in both Q4-PW and Q4-PPW (P<0·05). In spite of this, overall 68 and 56 % of the PPW and PW, respectively, were having inadequate dietary Ca intake (P<0·05). Intakes of vitamin A and vitamin C were significantly higher among the PW as compared with the PPW (P<0·05). In PPW, both vitamin A and vitamin C were significantly higher in HHEQ-4 compared with HHEQ-2 and in PW this was only the case for vitamin A. Nevertheless, overall >60 and >80 % of the women (PW and PPW) were having vitamin A and vitamin C deficiency, respectively (Fig. 1). Supplement intake data showed that 45 and 19 % of PW consumed Fe or multi-vitamin supplements, respectively. For PPW, 10 and 2 % of the subjects reported intake of these supplements, respectively.
Prevalence of anaemia, Fe deficiency, Zn deficiency and vitamin A deficiency in a subset of the respondents is given in Table 4. Particularly, Fe and Zn deficiency were widely prevalent. Owing to the limited sample size, differences among the two groups of women were not statistically significant (P>0·05; data considered as categorical and tested according to χ 2 method).
Table 4 Biochemical analysis of blood samples collected (pre-pregnant women (PPW): n 45; pregnant women (PW): n 45)

* For serum ferritin determination, n 39 for PPW and n 34 for PW.
Discussion
The present study reports on the nutritional status of women of reproductive age as per anthropometric measurements, dietary intake and biochemical parameters (in a subset of women). At least 10 % of the women are likely to initiate their pregnancy with poor health status. MUAC measurement is a good indicator of the protein reserves in a body, and a thinner arm reflects wasted lean mass, that is malnutrition( Reference Cogill 22 ). MUAC measures <23·5 cm among Indonesian PW have been associated with risk of LBW as well as pre-term births( Reference Sebayang, Dibley and Kelly 11 ). A study in Bogor district showed a poor nutritional status as per MUAC measurements among PW with poor socio-economic status( Reference Yongky 23 ). Maternal weight of <45 kg in the second trimester among Indian populations has shown more than a 2-fold risk for LBW( Reference Bisai, Mahalanabis and Sen 24 ). The gross agreement except for PW-Q3 in the proportion of women with either MUAC<23·5 cm, BMI<18·5 kg/m2 or weight<45 kg as a risk parameter for poor pregnancy outcome is interesting as there is no guidance on different cut-offs for maternal weight before and during pregnancy. As per BMI, nearly half (44 %) of the PPW in our study population were either underweight (13 %) or overweight (31 %), indicating that these women initiate their pregnancy without an optimal weight status and are possibly not ready to fully cope with the physiological changes during pregnancy.
In a post hoc sub-group analysis among PPW to investigate whether there are differences in nutrient intakes of overweight+obese women (BMI>25 kg/m2) and women with normal BMI (18·5–25 kg/m2), we found statistical significances (P<0·05, according to t test or Mann–Whitney test based on normal/non-normal distribution) in four among twenty-eight possible comparisons (seven nutrients, three economic quintiles+total group), all of which indicated lower intake in the overweight+obese sub-group compared with the normal BMI sub-group. We are, however, reluctant to conclude that there may be a tendency among overweight+obese women to actually consume less of the specific nutrients including energy, but would rather attribute this finding to a tendency for under-reporting, especially by overweight and obese subjects as reported from various studies( Reference Kerr, Schap and Johnson 25 – Reference Litchman, Pisarska and Berman 27 ).
Earlier studies from Indonesia have already reported that PW subsist on plant foods, mainly based on rice, pulses, nuts and vegetables. Studies from other countries also have reported PW diet to be dominated by cereals and cereal products( Reference Andersen, Thilsted and Nielsen 28 , Reference Piirainen, Isolauri and Lagström 29 ). Intake of animal foods such as meat and chicken decreased with the increasing costs, and thus we observed the lowest intake in the lowest HHEQ for PPW and PW. Earlier studies from Indonesia have reported similar inadequate food intake mainly due to the socio-economic factor( Reference Hartini, Winkvist and Lindholm 30 ). Our study confirms that there is still an economic gradient to meat consumption in PPW. Interestingly, the same holds true for vegetables intake, which are more expensive than staple foods in our studied urban area. Milk consumption in PW was higher compared with PPW across all HHEQ, indicating milk to be considered a nutritious food for PW. An earlier study showed that milk intake during pregnancy was associated with a reduced risk of small-for-gestational age, an increased risk of large-for-gestational age and an increased mean birth weight, abdominal circumference, placental weight, birth length and head circumference adjusted for gestational age at birth( Reference Olsen, Halldorsson and Willett 31 ).Typical for Indonesia, food consumed between main meals (snacking) was also common among the women of the present study contributing to their daily energy intake; however, as many snack foods are deep fried, they may not be the optimal choice( Reference Sartika 32 ). Because of the high energy density of several deep-fried snack foods, the contribution of snack foods is substantial and simply recommending to abstain from these foods would aggravate the energy deficiency. Nevertheless, good, nutritious, low-cost, non-fried but still energy-dense snack foods rich in/or fortified with adequate nutrients are needed to improve the nutritional status of women in this region.
Nutrient intake data showed that at least half of the women (PPW and PW), with their habitual diet, across the studied HHEQ could not meet their nutrient requirements. A recent review of various studies conducted among Indonesian PW confirms that women do not change their dietary intakes on becoming pregnant and are not able to meet their EAR for several nutrients( Reference Hartriyanti, Suyoto and Muhammad 4 ). Increasing HHEQ showed increase in the energy and protein intakes, but not enough to meet adequacy, similar to another study( Reference Mawaddah and Hardinsyah 33 ). Inadequate energy intake is indicative of an overall low intake of food. It is remarkable and possibly a paradox to observe a clear energy deficiency (<70 % RDA) in 32–60 % of PPW, whereas in this group 31 % were overweight or obese as well. We have no clear explanation for this except for the fact that physical activity may be far lower in our group than what is considered typical in establishing RDA. Another reason might be that we witnessed the consequence of differences in food availability in early life of the PW, making them especially vulnerable for obesity. Protein intake as %RDA among the PW was less as compared with the PPW. Low protein intake is associated with poor pregnancy outcomes. Explicit recommendations regarding the minimal or optimal proportion of animal protein are lacking, but a recent review has suggested that about one-third of protein intakes should come from animal-source foods to make a significant impact on growth( Reference Michaelsen, Hoppe and Roos 34 ). Although these recommendations are for young children, we consider them relevant for women of reproductive age as well, especially PW. Thus, the median proportion of 31 % animal protein intake in HHEQ-2 among PW, together with a total protein intake of only 55 % of Indonesian RDA, increases the level of concern.
The majority of the women had dietary Fe deficiency similar to earlier findings( Reference Hartini, Winkvist and Lindholm 35 , Reference Susilo and Hadi 36 ). Although Indonesia has an Fe supplementation programme in place for PW, compliance and possibly execution is suboptimal. One study reported that 85 % of PW receive Fe supplements( Reference Hartini, Winkvist and Lindholm 35 ), and in our study only 45 % of the PW indicated actual consumption of the Fe+folic acid supplement. We did not take the Fe supplements into account in the dietary intake analysis. Among PW, 22 % were found to be anaemic and 41 % showed Fe deficiency based on serum ferritin levels, with limited overlap, indicating that in >50 % of PW at least one indicator was affected. Zn is necessary for normal growth and development of the fetus and placenta, deficiency of which may cause intra-uterine growth retardation( 37 ). Animal foods are good sources of Zn; however, these were less frequently consumed by the study group. A recent study showed that dietary Zn intake from animal food sources and their proportions relative to total Zn intake were positively associated with birth weight and height. Conversely, the percentage of Zn intake from plant food sources relative to total Zn intake was negatively associated with birth height, indicating not only the amount of dietary Zn intake to be important but also the source of dietary Zn to be equally important( Reference Lee, Hwang and Kim 38 ).The main food consumed by our population was cereals (rice) with little animal foods, posing a risk for poor fetal outcome. This is supported by the proportions of 42 and 56 % of PPW and PW, respectively, with plasma Zn below healthy reference values.
Ca is required for bone formation, muscle contraction, and enzyme and hormone functioning( 39 ). Women with clearly suboptimal amounts of Ca intake (<500 mg/d) may be at risk for bone loss during pregnancy and may not meet fetal bone requirements( Reference Hacker, Fung and King 40 ). On the basis of our results, this is the case in >25 % of HHEQ-2/HHEQ-3 PW. In spite of an increased intake of milk (source of Ca), half of the PPW as well as PW were not able to meet the dietary requirements for Ca across HHEQ, also indicated in other studies( Reference Hartini, Winkvist and Lindholm 35 , Reference Susilo and Hadi 36 , Reference Piammongkol, Marks and Williams 41 ).
Poor vitamin A intake has effects on fetal development and child health, for example, increased risk of pre-term birth, reduced intra-uterine growth, decreased birth weight and reduced vitamin A content in breast milk( Reference Persson, Hartini and Greiner 5 ). Vitamin C cannot be synthesised or stored in the human body, and thus a daily supply is required for collagen synthesis and for increasing non-haem Fe absorption. Maternal vitamin C levels decrease during pregnancy, whereas in the fetal blood at delivery the levels are two to four times higher than in maternal blood( 37 ). Women in our study had deficient intakes of these vitamins, suggesting initiation of pregnancy with poor stores that possibly worsen during pregnancy and may result in inadequate fetal levels. The deficient vitamin A and C intakes were mainly driven by low vegetable and fruit consumption illustrated by our finding that only <35 and <45 % of the PPW and PW, respectively, reported any consumption of fruits. It is interesting to note that other studies from Indonesia show average intakes of vitamins A and C above 100 % of EAR( Reference Susilo and Hadi 36 , Reference Zakiyah and Kusmiyati 42 ), although Prihartini et al.( Reference Prihartini, Jahari and Sebayang 6 ) also reported from their Lombok study mean vitamin C levels well below EAR. These studies are older studies and may not be similar to the current dietary intake pattern of the women. Study area, method of assessment and inclusion–exclusion criteria in those studies were different from the current study, thus possibly affecting the study results.
The cross-sectional design with reasonable number of subjects well distributed among the broad middle-class household expenditure covering three of the five HHEQ in a well-defined area is a major strength of the present study as most other studies do not focus on socio-economic status. The sample size of sixty-five to sixty-nine subjects per HQ for each group may be slightly under-powered, considering a typical sample size of about 100 subjects/group to be sufficient to detect a 20 % difference in any nutrient deficiency. Because of the cross-sectional design, our study provides no direct evidence about changing diet from pre-pregnancy to pregnancy as only a longitudinal study will be able to prove this. Nevertheless, we have no indications for severe dissimilarities in measured background variables, and thus conclude that both populations are sufficiently similar. We studied PW only in their second trimester of pregnancy, but from the results of the much larger Supplementation with Multiple Micronutrients Intervention Trial (SUMMIT) study( Reference Prihartini, Jahari and Sebayang 6 ) in Lombok it may be inferred that major nutrient intakes and their deficiencies during the three trimesters of pregnancy are very similar if extrapolation to West Java is acceptable. Unfortunately, nutrient intake information for several other relevant nutrients (e.g. dietary fibre, fat quality, DHA, Se) could not be calculated in this study due to limited database in the currently available country-specific Food Composition Tables. Information on the quantitative intake of supplements by the women is limiting. The non-normal distribution of several variables presented a challenge for statistical analysis. We therefore used medians and IQR all over this report. Testing for the socio-economic gradient among the study’s HHEQ was carried out by ANOVA, realising that this may not be fully appropriate with non-normally distributed variables. Therefore, post hoc tests were also used, comparing HHEQ-2 with HHEQ-4, using Mann–Whitney tests if needed. Any specific correction for subject under- and over-reporting was not carried out; however, because of non-normal distribution of many variables, we think that providing only the medians and the 25th and 75th percentiles is an acceptable approach. For energy intake, actual intakes may be compared with predicted total energy expenditure (pTEE) and reported values <2 sd would surely not be plausible( Reference McCrory, Hajduk and Roberts 43 ). For typical PPW in our study, 30 years of age, weight 50 kg and height 150 cm, the −2 sd cut-off for pTEE amounts to 3950 kJ (944 kcal). Thus, we have reasonable confidence that reported energy intakes upwards from 4196 kJ (1003 kcal) (the 25th percentile for Q2-PPW) should not be rejected because of physiological incompatibility. Biochemical estimations could be performed for only a limited number of women because of both study logistics and cultural reasons among the women. Despite of this, there is reasonable agreement between both approaches, indicating little selection bias, if any.
Conclusion
Our study shows that at least half of the women of reproductive age (PPW and PW), with their habitual diets and irrespective of their income–expenditure status, are not able to meet the country-specific nutrient recommendations. As per the MUAC measurements, more than one in ten women initiate their pregnancy being chronically energy deficient, and the situation worsens to almost one in five during pregnancy. PW reported higher food intakes during pregnancy compared with PPW, and yet the extent of this higher intake was not enough to even meet the additional requirements defined by the Indonesian RDA for PW compared with non-PW. In 24 and 44 % of the PPW and PW, respectively, a combined inadequate intake of energy and protein was found. Improving food quantity and quality to increase intake of specific macro- and micronutrients, possibly through food fortification, is recommended, even though affordability/poverty may still be an issue in the lowest income–expenditure quintile. Clearly, more nutrition education is needed across all socio-economic classes to increase understanding of nutrient requirements during this specific stage in life.
Acknowledgements
The authors are extremely grateful to all the pre-pregnant and pregnant women and their families for their willingness to participate in the present study. The authors thank the women volunteers (kaders) and enumerators for their contribution during the data collection; and to the government and health representatives at all levels for their contribution to the study. The authors also thank PT Sarihusada Generasi Mahardhika and PT Nutricia Indonesia Sejahtera for providing financial support to the present study.
The study was sponsored by PT Sarihusada Generasi Mahardhika (SGM) and PT Nutricia Indonesia Sejahtera (NIS), but this had no influence on the outcome of the study.
The authors’ contributions are as follows: S. M., D. B., R. R., N. A., L. N., L. M., J. B. conceived and designed the study; S. M., D. B., R. R., Z. Z., T. S., L. M. were involved in the execution of the study; and S. M., D. B., R. R., Z. Z., N. A., L. N., T. S., L. M., P. S., J. B. were involved in evaluation of the data and writing of the manuscript. T. S., L. M., P. S., J. B. are employees of SGM, NIS and Nutricia Research, respectively.
None of the authors has any personal or financial conflicts of interest to declare.





