



Epidemiological evidence indicates that social determinants and biological conditions are predictors of fetal development and health conditions as well as chronic non-communicable diseases in adult life(Reference Barker1). Birth weight and prematurity are considered indicators of the overall health of the fetus and of the child(Reference Coelho, Cunha and Esteves2) and related to prenatal quality.
It is known that social inequities such as low income and maternal education level along with a lack of focus on health and social service policies are associated with morbidity and mortality in pregnant women and their children(Reference Wehby and López-Camelo3,Reference Rasella, Aquino and Santos4) . In the context of social inequalities, specific nutritional deficiencies may coexist(Reference Assis, Barreto and Santos5), such as vitamin D deficiency (Fig. 1).
Fig. 1. Monitoring flowchart of pregnant women, ‘Nutritional and genetic risk factors during pregnancy associated with low birth weight/prematurity. NISAMI cohort’. Santo Antônio de Jesus, Bahia, 2013–2015.
Vitamin D deficiency (<50 nmol/l) in pregnant women has been associated with compromised health during the gestational phase, which is reflected in the health of the fetus and newborn(Reference Leffelaar, Vrijkotte and van Eijsden6). Vitamin D deficiency is also associated with the occurrence of gestational diabetes, eclampsia and excessive weight gain among other morbidities during pregnancy, all of which have repercussions later in life for both mother and child(Reference Aghajafari, Nagulesapillai and Ronksley7). The association between poor concentrations of maternal vitamin D and the occurrence of low birth weight and prematurity has also been reported(Reference Aghajafari, Nagulesapillai and Ronksley7). However, other studies did not find any associations between these events(Reference Javaid, Crozier and Harvey8,Reference Viljakainen, Saarnio and Hytinantti9) .
Although the importance of micronutrients, particularly vitamin D, and social determinants in the health of the population is recognised, epidemiological studies that adopt methodologies to analyse the direct link between these associations and determine the mediating factors, particularly in the reproductive life phase, are rare. Thus, the present study evaluates the relationship among maternal vitamin D serum concentration, prenatal monitoring, social determinants and birth weight.
Methods
Study design and sample
This prospective, dynamic cohort study took place from June 2013 to September 2015, and included pregnant women who were receiving prenatal services from Family Health Units.
The study was conducted in the municipality of Santo Antônio de Jesus in the Recôncavo Sul Baiano; this municipality has an area of 261 km2 and is 187 km from the city of Salvador, the capital of the State of Bahia. Santo Antônio de Jesus has 90 949 inhabitants, 79 271 residents in urban areas and 116 763 in rural areas, of which 47 963 are women and 42 986 men. In 2012, 874 children were born and 9·6 % had low birth weight(10). Santo Antônio de Jesus is located at 12°58′S, 36°16′W and has a tropical climate (annual average of 23·0°C). Seasons of the year were defined as summer (December–January–February), fall (March–April–May), winter (June–July–August) and spring (September–October–November).
Exclusion and inclusion criteria
The study included women who lived in the urban area of the municipality, were at least over 18 years old, had gestational ages up to 34 weeks at the time of enrolment and received prenatal care from the Public Health System.
The criteria for exclusion after the baseline consisted of multiple gestations, pre-eclampsia, renal problems, HIV, abortion or fetal or embryonic death. Pregnant women previously enrolled who did not give birth in the medical units of the municipality and/or who could not be reached by telephone after delivery were excluded from the study.
Those women who met the following eligibility criteria (n 349) were referred to a clinical laboratory in the city and blood samples were collected after overnight fasting. Four women were excluded in addition to 18 women who did not give birth in the municipality of Santo Antônio de Jesus and were not located by telephone. After these exclusions, 327 pregnant women were effectively monitored (Fig. 1).
Data collection and definition of variables
After understanding the objectives of the investigation and the possible risks, the pregnant woman who consented to participate in the study signed the free informed consent form. After the agreement was signed, interviews about socio-economic, demographic and lifestyle characteristics were performed by trained interviewers and the information was recorded using a standardised questionnaire.
In the first stage of the cohort (baseline) when a pregnant woman was included in the study, the woman’s pre-gestational weight was collected from the pregnancy chart. When not available, the weight provided by the woman was taken during the interview. Maternal height was measured by the health team at the clinic, who were trained according to the recommendations of Lohman et al. (Reference Lohman, Roche and Martorell11). After these procedures, a date was scheduled for blood collection.
Gestational age was calculated based on the date of the last menstrual cycle, available on the pregnant woman’s chart, or the gestational age was recorded from the first ultrasound, which was performed by the end of the first trimester.
Blood collection was performed between 7:00 and 9:00 a.m. after at least 8 hours of fasting at the Research Center in Maternal and Child Health of the municipality. After collection, the blood was centrifuged for 15 min at 2000 rpm in an environment protected from ultraviolet light for serum separation. Serological samples were identified by codes and stored at −32°C in a freezer until the serum concentration of 25-hydroxyvitamin D (25(OH)D) was measured. The dosage of vitamin D was performed with the quantitative determination method, based on the chemiluminescence principle (CLIA. A 25(OH)D dosing kit was used (DiaSorin®), with an intra-assay CV of 8·4–12·5 % and an intra-assay CV of 8·6–11·0 %.
Serum concentrations of 25(OH)D were classified as deficient (<50 nmol/l), insufficient (50–75 nmol/l) and sufficient (>75 nmol/l)(Reference Holick, Binkley and Bischoff-Ferrari12). A complete blood count and total Ca levels were also obtained. The haemogram was performed by fluorescence flow cytometry with a semiconductor laser (Sysmex XT 1800i®) and total Ca was measured by the Vitros dry chemical method (Johnson & Johnson®) in a reference laboratory of the municipality.
In the second step of the study between September 2013 and December 2015, the pregnant women were monitored until the birth of their child. The gestational weight gain was measured by the study team; in cases where information was missing, the data were collected from the pregnant woman’s chart in the Family Health Units. The gestational weight gain was classified according to the maternal pre-gestational BMI, adopting the criteria of the Institute of Medicine (13).
The birth weight was measured with the child naked using a digital paediatric scale, Welmy® brand, with a capacity of 15 kg and a 10 g interval. The anthropometric measurement was performed in duplicate and a maximum variation of 10 g for the weight was acceptable. When different values were obtained, a third measurement was performed. The final measurement was calculated as the mean of the values of the closest measurements(Reference Queiroz, Assis and Pinheiro14).
Data related to the children’s birth were collected from the Department of Epidemiological Monitoring (VIEP) of the Municipal Health Department. Home visits were performed at the end of the study for those pregnant women whose data on gestational outcomes were not found in the VIEP.
The Z score of birth weight for gestational age was classified according to the sex of the newborn(15). Birth weight was classified as small for gestational age (below the tenth percentile), appropriate for gestational age (tenth to ninetieth percentile) and large for gestational age (above the ninetieth percentile)(Reference Villar, Cheikh Ismail and Victora16).
Theoretical model
The theoretical model of the study is presented in Fig. 2. The response variable (endogenous) of this model is observable and represented by the birth weight. It expresses a single event in the individual’s life and is integrated into the regression model in a continuous form.
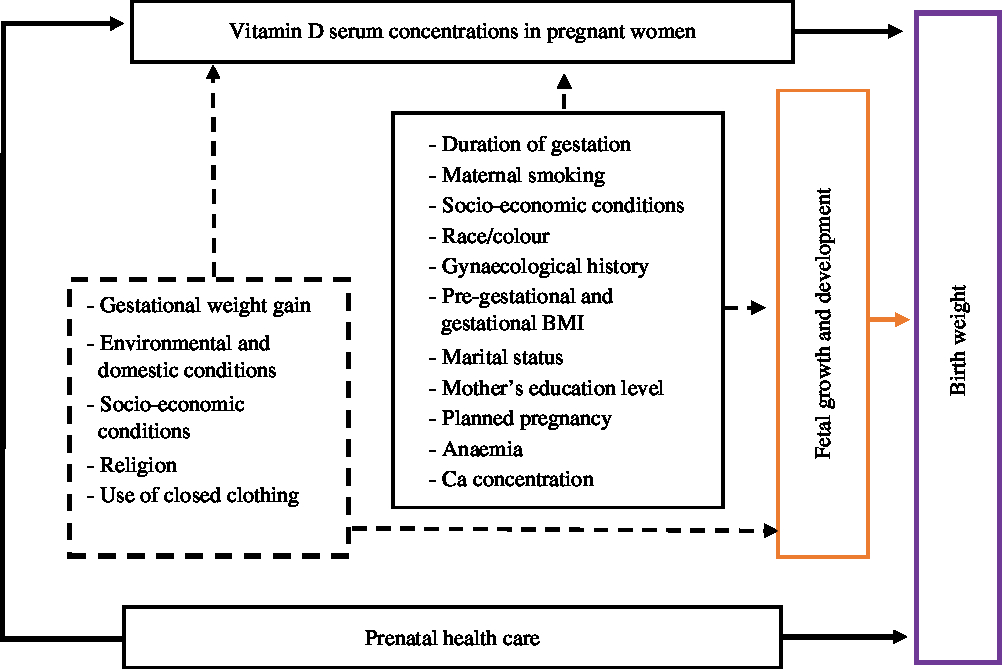
Fig. 2. Relationship between vitamin D serum concentration, prenatal care and social determinants and birth weight.
Exposure variables (exogenous) are observable and integrated by those that are directly associated with birth weight, according to references in the literature. They were included in a continuous form: maternal 25(OH)D concentration, total Ca, Hb, maternal education and age, family income, number of pregnancies, starting month of prenatal care, pre-gestational and gestational BMI, maternal weight gain, duration of gestation and number of consultations during pregnancy. The other items integrated into the model in the categorical form include: sex of the child (male (0), female (1)); skin colour (yellow, white, indigenous (0), brown (1), black (2)); smoker (yes (1), no (0)); alcohol consumer (yes (1), no (0)); marital status (living with partner (0), no partner (1)); planned pregnancy (yes (0), no (1)); and socio-economic class according to the Brazilian Association of Research Companies (ABEP), which considers the possession of goods (television, radio, car, washing machine, VCR or DVD, refrigerator and freezer), education level of the head of the family, number of toilets/bathrooms in the household and presence of a monthly maid, later categorised into A or B, C, D or E, respectively.
In addition to the exogenous variables, intermediate variables of the relationship between vitamin D serum concentration and birth weight were also selected based on those indicated in the literature, including the use of closed clothing (≤1 time per week (0), 2–4 times per week (1)); religion (Catholic (1), protestant (2), spiritism (3), Afro-Brazilian religions (4)); and season that the blood was collected (summer (0), spring (1), autumn (2), winter (3)).
Statistical analyses
Justification of sample size
The sample of the present study was calculated based on the equation for the cross-sectional mean test, an alternative that can be used when the longitudinal study response variable is a single event such as birth weight, as suggested by Twisk(Reference Twisk17). Mean serum vitamin D levels of 62·8 (sd 7·8) nmol/l were considered as the mean values for eutrophic pregnant women(Reference Bodnar, Catov and Roberts18), with 25 % of concentrations(Reference Kovacs19), mean weight at birth of 3196 g, standard deviation of 56 g(Reference Queiroz, Assis and Pinheiro14) and type I error (α) of 5 and 80 % of power (1 − α). Thus, the sample size requirement was 149 women. Considering that during the study period it was possible to accompany 327 pregnant women, it was decided to include all of them in the sample to analyse the theoretical model with the path analysis.
Descriptive analysis
Prevalence was adopted to describe the categorical variables. Mean and standard deviation were used for the continuous variables. To characterise the study sample, the quantitative variables were categorised as shown in Table 1. The mean Z score according to the exposure variables was compared using Student’s t test for equal variances and ANOVA.
Table 1. Percentage distribution and mean Z score of birth weight according to sociodemographic characteristics and biological variables of mothers and newborns, NISAMI cohort, Santo Antônio de Jesus, Bahia, Brazil, 2013–2015
25(OH)D, 25-hydroxyvitamin D.
Path analysis
To evaluate the association between vitamin D serum concentration, prenatal care and social determinants and birth weight, modelling with path analysis was used. Adjustment of the theoretical model and observed values were evaluated through different tests. To evaluate the acceptance of the theoretical model, the Bentler’s comparative fit index and the Tucker–Lewis index were used to analyse the adequacy of the theoretical model. In these indices, the results equal to 1 reflect a perfect fit, corresponding to the best fit of the model to the data(Reference Amorim, Fiaccone and Santos20) and thus acceptance of the proposed theoretical model.
Data were analysed by the Stata software version 13.
Ethical considerations
The study protocol was approved by the Research Ethics Committee of the School of Nutrition of the Universidade Federal da Bahia and the Faculdade Adventista da Bahia and conducted according to the guidelines laid down in the Declaration of Helsinki and Brazilian Resolution 466/2012. Informed consent was obtained from all individual participants included in the study.
Results
Of the 349 pregnant women, 327 (94 %) completed the monitoring required by the study. The mean vitamin D serum concentration did not differ between those who completed and those who did not complete the monitoring (P = 0·81). The maternal and newborn characteristics are presented in Table 1 and include a mean age of 26·91 (sd 5·87) years, low income (80 %) and maternal education level between 8 and 11 years (69 %).
Pre-gestational BMI classified 32 % of the pregnant women as overweight (≥25 kg/m²) and 27·0 % gained excessive weight during pregnancy. The mean total plasma Ca was 9·39 (sd 4·39) mg/l and anaemia affected 20·0 % of the mothers. Late starting of prenatal care was reported for 60 % of the mothers.
Tables 2 and 3 present the structural modelling results obtained according to the proposed theoretical model (Fig. 2). The coefficients express the direct, indirect and total association of each variable on maternal vitamin D serum concentration and birth weight.
Table 2. Coefficients of path analysis, the relationship between prenatal care, social determinants and vitamin D concentration in pregnant women (n 326), Santo Antônio de Jesus, Bahia, 2013–2015Footnote *
(β-Coefficients and 95 % confidence intervals)
* Root mean square error of approximation: 000, comparative fit index: 1·0, Tucker–Lewis index: 1·0.
Table 3. Coefficients of path analysis, the relationship between prenatal care, social determinants and vitamin D concentration in pregnant women on birth weight (n 326), Santo Antônio de Jesus, Bahia, 2013–2015Footnote *
(β-Coefficients and 95 % confidence intervals)
25(OH)D, 25-hydroxyvitamin D.
* Root mean square error of approximation: 000, comparative fit index: 1·0, Tucker–Lewis index: 1·0.
Concentration of vitamin D in pregnant women
The mean concentrations of 25(OH)D were 72·29 (sd 30·34) nmol/l. The percentages of insufficient and deficient serum concentrations of vitamin D were 45·0 and 21·0 %, respectively, totalling 66·0 % of hypovitaminosis D. A direct association was found among low socio-economic class (β 6·19; 95 % CI 0·79, 11·59; P = 0·02), Afro-Brazilian religions (β 2·82; 95 % CI 0·76, 4·88; P = 0·01) and high vitamin D levels in pregnant women. However, during the winter period, decreased serum vitamin D 25(OH)D levels were observed at −3·60 (95 % CI −6·84, 0·35; P = 0·03) nmol/l. The use of closed clothing favoured a decrease of −8·29 (95 % CI −15·15, 1·44; P = 0·01) nmol/l vitamin D serum concentration (Table 2).
Determinants of birth weight
Caesarean delivery occurred in 66·26 % of the births and 48·46 % of the newborns were male. The mean birth weight was 3296·7 (sd 572·48) g and the prevalence of very low birth weight (<2500 g) was 4·7 %, while the prevalence of low birth weight (<3000 g) was 17·18 %. There was a high frequency of large for gestational age (25 %) and a low occurrence of small for gestational age (5·0 %). Of the pregnant women monitored, 8 % gave birth to a newborn at less than 37 weeks gestation, and this was directly associated with birth weight (P ≤ 0·01).
Vitamin D serum concentration had a direct and statistically significant association with birth weight. Each nmol increase in maternal vitamin D serum concentration correlated with an increase in birth weight of 3·06 (95 % CI −1·37, 4·75) g (P ≤ 0·01) (Fig. 3).
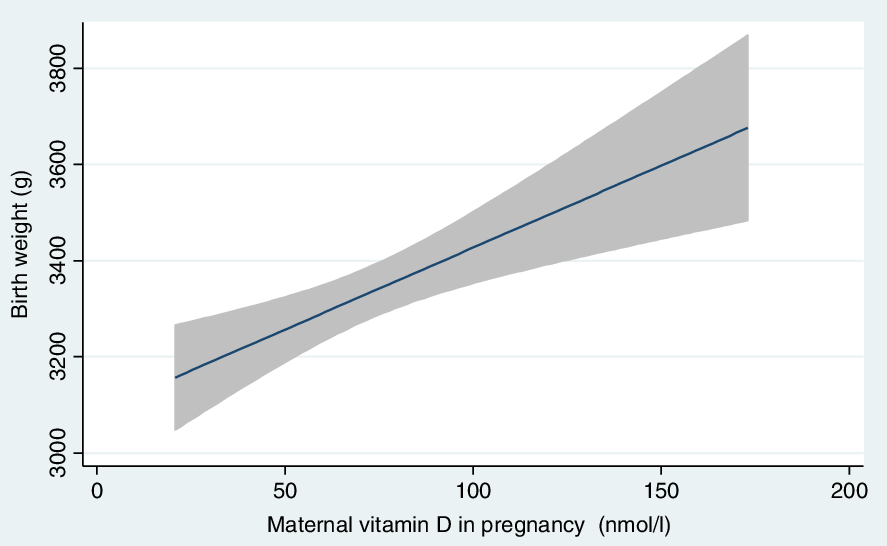
Fig. 3. Association of concentration of vitamin D in pregnant women and weight of newborns. NISAMI cohort, Santo Antônio de Jesus, Bahia, 2013–2015. ![]() , Fitted values;
, Fitted values; ![]() , 95 % CI.
, 95 % CI.
Social determinants had a strong influence on birth weight (Table 3). An increase in maternal education level favoured a higher birth weight (β 24·52 g; 95 % CI 1·82, 47·23; P = 0·03). Late onset of prenatal care was associated with a decrease in birth weight (β −39·24 g; 95 % CI −73·31, 5·16; P = 002) when compared with women who started monitoring in the first months of gestation. Fewer consultations during pregnancy were also associated with a decrease in newborn weight (β −41·49 g; 95 % CI −79·27, 3·71; P = 0·03).
In relation to maternal and obstetric characteristics, gestational BMI was associated with an increase in birth weight of 23·84 g for each unit increase (kg/m2) in BMI (95 % CI 4·37, 43·31; P = 0·01). Gestational age showed a strong association with birth weight. A 1-week increase in the duration of gestation favoured a gain of 79·71 g (95 % CI 52·81, 106·6; P ≤ 0·01). The girls on average had a lower birth weight of 186 g than the boys (95 % CI −283·40, −89·42 g; P ≤ 001).
Intervening variables with indirect associations influenced the relationship between maternal vitamin D serum concentration and birth weight, such as maternal smoking (β −15·37 g; 95 % CI −26·10, 4·64; P ≤ 0·01), the use of closed clothing during pregnancy (β −8·29; 95 % CI −15·15, 1·44; P = 0·01) and the winter season (β −3·60; 95 % CI −6·8, 0·35; P = 0·03), which all contributed to the lower birth weight. Low socio-economic class was associated with a higher birth weight (β 6·19; 95 % CI 0·79, 1·59; P = 0·05) as was the practice of an Afro-Brazilian religion by the mother (β 2·82; 95 % CI 0·76, 4·88; P ≤ 0·01).
The model presented an adequate fit index (comparative fit index = 1; Tucker–Lewis index = 1), indicating that it explains well the relationships tested in the present study.
Discussion
The results of the present study indicate that social determinants act directly on maternal vitamin D serum concentrations and birth weight. The number of consultations during pregnancy and the month of beginning prenatal care are direct determinants of birth weight. Vitamin D serum concentration also directly affects birth weight. Thus, biological determinants and social inequalities in healthcare directly affect maternal health conditions and, consequently, infant birth weight.
In general terms, the high occurrence of deficiency (21 %) and insufficiency (45 %) of vitamin D in pregnant women registered in the present study follow the trends reported in countries with cold climates, even though Brazil has a predominantly tropical climate. Due to the greater availability of ultraviolet rays in tropical countries such as Brazil, the population has an increased ability to generate photoproduction of vitamin D, which reduces deficiency of this vitamin(Reference Saraf, Morton, Camargo and Grant21).
In pregnant women, an estimated 18–90 % of vitamin D deficiency occurs in European countries, 66–96 % in Southeast Asia and 41–97 % in the Pacific region(Reference Saraf, Morton, Camargo and Grant21). Observational studies have registered a slightly lower occurrence of vitamin D insufficiency in pregnant women, ranging from 9·3(Reference Karras, Paschou and Kandaraki22) to 53 %(Reference Bowyer, Catling-Paull and Diamond23). Studies show that deficiency and insufficiency are associated with low birth weight(Reference Aghajafari, Nagulesapillai and Ronksley7). This is because vitamin D actively participates in the process of fetal growth and development.
The pregnant women in our study were not supplemented with vitamin D(Reference Costa, Coelho and Santos24), (Reference Farias, Poston and Franco-Sena25). Furthermore, in Brazil, vitamin D intake through dietary sources is low and pregnant women who participate in public prenatal care programmes do not use vitamin D supplementation(Reference Pereira-Santos, Santos and Carvalho26,Reference Benaim, Cocate and de Barros27) . In Brazil, only supplementation with Fe (40 mg) and folic acid (400 μg) is mandatory for pregnant women(Reference Benaim, Cocate and de Barros27).
In our study, the mean birth weight values (3296·7 (sd 572·48) g) are higher than those found in pregnant women in neighbouring municipalities (3229·1 (sd 402·4) g)(Reference Queiroz, Assis and Pinheiro14). A study in Rio de Janeiro also registered a low value of mean birth weight (3253 g)(Reference Fonseca28). Therefore, the results show that the mean birth weight of newborns reaches expected values under adequate conditions of fetal growth.
The analytical challenge of understanding the relationship between social determinants, vitamin D serum concentrations and birth weight is to establish a hierarchy of determinants among macrosocial factors and to identify how these factors impact individual and group health mainly by understanding that relationship is not causal. This perspective can be modelled with path analysis or a path diagram.
In this context, maternal education and low socio-economic status were directly related to maternal vitamin D serum concentration and birth weight. The maternal education level is indicated as decisive in influencing health conditions in childhood, especially in gestational outcomes(Reference Fonseca28). This condition extends to the protection of newborns from prematurity, low birth weight and respiratory complications(Reference Marchi, Berg, Dencker, Olander and Begley29). However, low socio-economic level was associated with an increase in vitamin D serum concentration and fetal weight gain. This could be due to issues related to work situations, such as being subject to underemployment and to working in hostile conditions associated with high sun exposure and little access to long clothing and protective sunblock.
Although climate is a key factor in the photoproduction of vitamin D, studies have observed a positive association between vitamin D deficiency and low socio-economic status in countries with a cold climate(Reference Wang, Mao and Wang30). Aspects of habits and lifestyle, which include diets with low dietary and supplemental sources of vitamin D, impact the health of this population(Reference Cantarutti, Franchi and Monzio Compagnoni31,Reference Rodriguez, Santa Marina and Jimenez32) .
Other records of the relationship between the socio-economic class of pregnant women and higher birth weight have also been considered(Reference Coelho, Cunha and Esteves2). In the context of social inequality, eating habits can manifest in the consumption of high-calorie foods(Reference Coelho, Cunha and Esteves2,Reference Santana, Queiroz and Brito33) . This may lead to excessive weight gain during the gestational phase and therefore the birth of heavier children.
Another fundamentally important aspect for good gestational development and women’s health is the prenatal care provided by the Family Health teams. The mothers who started prenatal care in the first months of gestation and had more consultations during pregnancy delivered heavier babies. Prenatal care reduces prematurity and neonatal mortality. Maternal healthcare reduces complication rates during pregnancy and at delivery(Reference Anjos and Boing34).
The maternal and obstetric characteristics of pre-gestational BMI and duration of gestation are important. Gestational BMI directly impacted birth weight. Excess weight at the start of gestation is an important determinant of excessive weight gain during pregnancy. This explains the large number of children born who are classified as large for gestational age in the present study. For each increase of 1 kg in weight gain during pregnancy, there is an increase from 16·7 to 22·6 g in birth weight(13). Children of women who had excessive weight gain are predisposed to being born with more body fat(Reference Marchi, Berg and Dencker35,Reference Wang, Mao and Wang36) and to having a greater risk of developing obesity and chronic diseases during childhood and adulthood(Reference Barker1).
It is also noteworthy that pregnant women involved in Afro-Brazilian religions had increased vitamin D serum concentrations and showed an indirect association with increasing birth weight. An explanation for these results could be that the women who feed pregnant women practising Afro-Brazilian religions may provide a greater content of liposoluble vitamins and antioxidant compounds derived from palm oil(Reference Sundram, Sambanthamurthi and Tan37), which may indirectly contribute to better absorption of vitamin D from the diet and consequently higher birth weight. The result related to this aspect requires more study on the identified association, considering that the epidemiological literature does not report studies on gestational outcomes in women who practise Afro-Brazilian religions.
Cigarette smoking during pregnancy was associated with a low serum concentration of vitamin D, and smokers gave birth to lighter weight children. The chemical substances in tobacco can compromise the hepatic metabolism of vitamin D and fetal development(Reference Van Den Berg, Van Eijsden and Vrijkotte38). A meta-analysis found that the implementation of policies aimed at controlling smoking was associated with significant reductions in the rates of preterm birth(Reference Faber, Kumar and Mackenbach39).
The present study has some limitations. We did not analyse the impact of haemodilution on the concentrations of 25(OH)D during pregnancy. In our cohort, there are many different gestational ages, and vitamin D binding protein (VDBP) changes throughout pregnancy should be considered(Reference Zhang, Lucey and Horgan40). VDBP is the major carrier of vitamin D and its derivatives and can be used in the diagnosis of vitamin D status during pregnancy. Therefore, we recommend that future studies consider this variable.
Another limitation of the present study is the lack of evaluation of the influence of food consumption and physical activity level on birth weight. Likewise, we do not have information about vitamin D metabolite concentrations in umbilical cord blood serum. Thus, our results may be confounded when those data are missing. However, this aspect did not affect the achievement of adjustments of the theoretical model considered excellent to evaluate the relationships between serum concentrations of vitamin D, birth weight and mediating factors.
The longitudinal data and the robust statistical analysis in our study are additional strengths. In addition, we examined both the overall predicted status of vitamin D and the influence of maternal vitamin D serum concentration on birth weight.
To our knowledge, the present study is the first in Brazil to address the relationship among vitamin D serum concentration, social determinants and birth weight. The results of the present investigation indicate that the maternal serum concentration of vitamin D, the social determinants and the prenatal care carried out in the Primary Healthcare Units determined the birth weight. The present study indicates that prenatal care performed by Family Health Units is important to prevent nutritional disorders and to promote the health of women and children.
Acknowledgements
The authors thank all participants, principal investigators and collaborators of the NISAMI study.
The present study has been supported by the Brazilian National Research Council (CNPQ – project nos. 481509/2012-7: Factors of nutritional and genetic risk during pregnancy associated with low birth weight/prematurity).
M. P.-S. was involved in the project conception, development of the overall research plan, study oversight and analysed the data and wrote the paper. G. Q. C. was involved in the development of the overall research plan and with the writing of the manuscript. D. B. d. S. contributed to the project conception, supervised the study and drafted the manuscript. A. M. O. supervised the study and contributed to the design, statistical analyses, data interpretation and manuscript drafting. All authors approved the final manuscript for submission.
All authors declare no potential personal or financial conflicts of interest.






