


Several national and international organisations have provided guidance on desirable dietary intakes of the long-chain PUFA DHA and EPA from fish for adults and for infants (Table 1). For adults, these recommendations are based mainly on primary and secondary prevention of CVD, ranging from one to two portions of fatty fish per week or about 500 mg EPA and DHA per d(Reference Mozaffarian and Rimm1, Reference Kris-Etherton and Innis2). For pregnant and lactating women, the advice of an average daily intake of at least 200 mg DHA is based on optimal pregnancy outcomes(Reference Szajewska, Horvath and Koletzko3–Reference Makrides, Duley and Olsen5), and on possible beneficial effects on fetal and infant development(Reference Koletzko, Cetin and Brenna6, Reference Koletzko, Lien and Agostoni7). For infants (0–2 years of age), in 1994, the FAO/WHO(8) recommended 20 mg DHA per kg body weight per d for optimal growth and development. However, there are no agreed recommendations for the advisable dietary intake of EPA and/or DHA for children above 2 years of age.
Table 1 Recommendations for daily intake of DHA and EPA in adults and infants
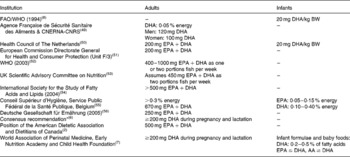
BW, body weight; CNERNA-CNRS, Centre Nationale d'Etudes et de Recommendations sur la Nutrition et l'Alimentation & Centre National de la Recherche Scientifique; AA, arachidonic acid.
* Supported by Perinatal Lipid Nutrition Project, Early Nutrition Programming Project, Child Health Foundation, Diabetic Pregnancy Study Group, European Association of Perinatal Medicine, European Society for Clinical Nutrition and Metabolism, European Society for Paediatric Gastroenterology, Hepatology and Nutrition, International Federation of Placenta Associations, and International Society for the Study of Fatty Acids and Lipids.
A workshop was organised in July 2007 to review and discuss the available evidence on dietary intakes of EPA and DHA and their potential physiological relevance to growth and health in children, and to evaluate whether there are sufficient scientific data for issuing evidence-based guidelines on EPA and DHA intake in 2- to 12-year-old children. The present paper summarises the outcomes of the discussions held at the workshop on current knowledge of dietary intakes among children 2–12 years of age and published literature regarding the potential importance of EPA and DHA at this stage of the life cycle.
EPA and DHA intakes in children
The richest food sources of both EPA and DHA are fatty fish, with smaller amounts in lean fish and other seafood(Reference Innis and Elias9, Reference Meyer, Mann and Lewis10). The distributions of dietary EPA and DHA intakes within populations are generally skewed with lower median than mean intakes, explained by a substantial number of individuals eating no or very little fish(Reference Meyer, Mann and Lewis10–Reference Welch, Lund and Amiano12). However, information of dietary intakes of EPA and DHA, particularly among children, is limited. This has several reasons, including the limitations of dietary intake methodology, collecting accurate information on dietary intakes from children, and the completeness of fatty acid data on foods listed in databases. For example, the fat and fatty acid composition of fish varies widely, meaning that specific information on the types of fish and seafood consumed is essential; eggs can be an important source of fatty acids and are often hidden in other foods such as cakes and puddings, but depending on the recall method their intake may be missed. Moreover, children frequently consume food outside of the home, and without the parents' knowledge.
The rather limited available information on dietary intake in children suggests that EPA and DHA intake tends to be lower than in adults(13). Similarly, the intake of children may also be lower per kg body weight than in infants who are breast-fed or fed infant formulas containing DHA(Reference Koletzko, Lien and Agostoni7, Reference Koletzko, Rodriguez-Palmero and Demmelmair14). Children's current dietary intake of EPA and DHA may also be lower than some decades ago(Reference Ailhaud, Massiera and Weill15). Whether current intakes of EPA and DHA among children are adequate for optimal functional and health outcomes requires information on dietary intakes of children following different diets together with measures of functional endpoints sensitive to potential biological effects of these fatty acids. It is conceivable that EPA and/or DHA intakes might contribute to health promotion and chronic disease prevention, but reliable and comparable data on dietary intake of n-3 fatty acids and on biochemical markers of status in different populations of children are scarce. The available data do not allow us to conclude that changing intakes of EPA and/or DHA can affect physical or mental development or yield specific functional benefits.
The effects of EPA and DHA on biological function, health and prevention of disease
Historically, recommended intake levels for nutrients have been defined to prevent signs of deficiency in the general population. In recent years, however, nutritional recommendations and guidelines are being progressively formulated based on evidence linking specific nutrients at given intakes to disease prevention and optimal performance and health(16). An example is the Acceptable Macronutrient Distribution Range used by the Institute of Medicine(17), which represents the range of energy intakes from the different macronutrient intakes that, when consumed as part of a diet providing an appropriate amount of energy to maintain ideal body weight, are associated with low risk of chronic disease.
Individuals that have low EPA and/or DHA intakes but eat plentiful sources of α-linolenic acid, such as vegans and vegetarians, do have a lower EPA and DHA status than omnivores, but are not known to develop signs of deficiency(Reference Davis and Kris-Etherton18). Higher intake levels of EPA and DHA have been associated with a range of possible physiological and health benefits in humans(Reference Akabas and Deckelbaum19), such as the improvement in neurological functions in infancy(Reference Cheatham, Colombo and Carlson20), the primary and secondary prevention of CVD and the metabolic syndrome in adults(Reference Mozaffarian and Rimm1, Reference Carpentier, Portois and Malaisse21), modulation of immune response(Reference Sijben and Calder22) and improved pregnancy outcomes(Reference Szajewska, Horvath and Koletzko3–Reference Makrides, Duley and Olsen5). The evidence for beneficial effects of EPA and DHA intakes on health outcomes in children is limited and will be summarised here.
The importance of attaining optimal brain and retina DHA for visual and neurological development and function is considered critical in the perinatal period(Reference Eilander, Hundscheid and Osendarp23). Beyond infancy, evidence linking DHA intake or blood levels of DHA with neurological benefits is limited to children following restricted diets with very low dietary intakes of EPA and DHA, such as children with phenylketonuria(Reference Beblo, Reinhardt and Muntau24–Reference Agostoni, Massetto and Biasucci26). These studies show that increasing DHA status with fish oil supplements is consistent with improvements in speed of information processing in the central nervous system as assessed by latencies of visual evoked potentials(Reference Beblo, Reinhardt and Muntau24), as well as significant improvements of coordination and fine motor skills(Reference Beblo, Reinhardt and Demmelmair25). These findings indicate that a continuous dietary supply of preformed DHA and/or EPA may be essential for achieving optimal neural function even in children who have a high intake of the precursor α-linolenic acid with restricted diets due to phenylketonuria(Reference Agostoni, Verduci and Massetto27). This conclusion may be relevant for healthy children as well, since children with early treated phenylketonuria are generally healthy and have no detectable alterations of energy and fatty acid metabolism.
EPA and DHA in combination with n-6 fatty acids have also been reported to improve behaviour in children with neurodevelopmental disorders such as attention-deficit hyperactivity disorder and dyspraxia in some(Reference Stevens, Zhang and Peck28–Reference Richardson and Montgomery30) but not all(Reference Hirayama, Hamazaki and Terasawa31, Reference Voigt, Llorente and Jensen32) studies. A recent systematic review of these studies concluded that there is insufficient evidence to identify any effect of nutrition, diet and dietary change on learning, education or performance of school-aged children from the developed world(Reference Ells, Hillier and Summerbell33). Further research of high quality, representative of all populations, undertaken for longer durations and using universal standardised measures of educational attainment is needed(Reference Ells, Hillier and Summerbell33) and should evaluate the potential relative roles of EPA and DHA, respectively, in children with neurodevelopmental disorders.
High intakes of EPA and/or DHA may beneficially modulate the immune system by decreasing the synthesis of pro-inflammatory arachidonic acid-derived eicosanoids(Reference Calder34) and by shifting the balance of T helper 1 (Th1), T helper 2 (Th2) and T regulatory cells(Reference Krauss-Etschmann, Hartl and Rzehak35). Evidence for beneficial effects on asthma in children is not established, but some studies suggested that for certain subgroups of respondent children, symptoms of asthma may be alleviated with DHA/EPA supplementation(Reference Nagakura, Matsuda and Shichijyo36). It is unclear to what extent these and other observations using high dosages of EPA and DHA supplements relate to possible effects with lower intakes achieved with foods.
A regular intake of fatty fish is widely advised to adult populations for the prevention of CVD, and a large part of associated beneficial effects is thought to be mediated by the supply of EPA and DHA with fatty fish(Reference Mozaffarian and Rimm1). Potential beneficial effects of EPA and DHA intakes in children on their future risk of developing CVD have not been documented. However, food preferences and eating habits that are established in childhood appear to show a certain degree of tracking into adulthood(Reference Parsons, Manor and Power37, Reference Lanigan, Turnbull and Singhal38). Therefore, it seems desirable to accustom children to dietary patterns that are likely to promote health in adulthood.
Approaches to develop possible advice on dietary intakes of EPA and DHA
Advice on dietary nutrient intake values for children is based on a variety of different methodological approaches, including consideration of deficiency states, usual intake levels, factorial approaches to calculate needs for maintenance and growth, effects on physiological function and health(Reference Prentice, Branca and Decsi39) and extrapolation from reference values established for other age groups such as adults or infants(Reference Atkinson and Koletzko40). The authors of the present paper conclude that the current lack of reliable data on the relationship between EPA and DHA intake or status and functional and health outcomes in 2- to 12-year-old children does not allow determination of physiological requirements or nutrient intake levels using classical approaches to derive dietary recommendations. Extrapolating n-3 fatty acid intake levels, including those for EPA and DHA, for children from existing reference values for either adults or infants (Table 1) seems inappropriate, not only because there is still considerable uncertainty regarding nutrient intake levels for DHA and/or EPA in both adults and infants, but also because extrapolation based for example on body mass or energy expenditure is expected to inadequately reflect age-specific physiological requirements, such as continuing neurological development and lean tissue growth, that determine dietary nutrient needs(Reference Atkinson and Koletzko40). Thus, at present the available evidence is insufficient to formulate quantitative nutrient intake values for EPA and DHA in children. However, it seems reasonable that dietary advice for children should be consistent with advice for the adult population, such as regular intake of one to two fatty fish meals per week providing DHA and EPA associated with the risk reduction of CVD. If such a habit can be established early in life and be maintained, it may also support a desirable long-chain n-3 fatty acid supply among females of child-bearing age to support optimal pregnancy outcomes. There is no reason why children in a family setting should be excluded from the consumption of at least one to two meals of fatty fish per week, which is recommended for the adult population(Reference Kris-Etherton and Innis2).
Present and future research
The possible relationships between intake and effects of DHA and/or EPA need to be studied in detail. Presently, the research project ‘Nutrition and Mental Health’ funded by the European Commission's 7th Framework Research Programme will try to establish whether there is a relationship between the level of dietary DHA supply and neurological functions in children. Further studies should also include evaluating effects of the intake of α-linolenic acid, as well as factors affecting its endogenous conversion to EPA and DHA, such as the concomitant intake of linoleic acid(Reference Blank, Neumann and Makrides41) and the role of genetic polymorphisms of the desaturating enzymes Δ-6 and Δ-5 desaturases(Reference Schaeffer, Gohlke and Muller42).
Relevant public health outcomes that are likely to be linked to lifelong intakes of EPA and DHA include the risk of (future) CVD and the metabolic syndrome, optimal mental development and behaviour, and immune response.
Dietary studies should be carefully conducted and analysed, with a specific and standardised methodology, considering the substantial challenges in assessing individual intakes of EPA and DHA in children. Since assessment methods for dietary intake are imprecise, age-specific information on fatty acid status based on biological markers are also required. Cross-sectional analyses from prospective birth and childhood cohort studies are likely to provide valuable insights that can contribute to designing intervention trials. Age-specific effects of different fatty acid intakes and dosages on relevant endpoints should be assessed in controlled intervention studies. The data obtained should aim at establishing the effect of different doses of individual fatty acids, and of different combinations and ratios of PUFA, on well-defined and quantifiable outcomes. Such outcomes may include:
(1) Markers of cardiovascular risk and the metabolic syndrome;
(2) Measures of neural function, cognition and behaviour;
(3) Markers of inflammatory response, immune function and their related diseases, such as allergy or autoimmune disease.
Studies in children aiming at evaluating these and other outcomes must respect the limitations determined by the ethical rules for research with children(Reference Ungar, Joffe and Kodish43, Reference Knudson44).
Although recent risk analyses tend to support the safety and overall benefit of increased fish consumption(Reference Cohen, Bellinger and Connor45, Reference Sioen, De and Verbeke46), potential adverse effects of recommending increased dietary intakes of EPA and DHA from fish oil concentrates or fatty fish, such as the risk of adverse effects of contamination with environmental pollutants(Reference Oken, Radesky and Wright47, Reference Halldorsson, Meltzer and Thorsdottir48), should be taken into account.
Conclusions
A better understanding of the functional roles of EPA and DHA in children is required in order to determine adequate dietary intakes. Currently there is a lack of sufficient evidence to link levels of dietary intake of DHA and/or EPA to improved physical, mental or other functional benefits in children. Therefore, quantitative dietary intake recommendations for children cannot be established at this time.
Food-based dietary guidelines that apply to adults for enhancing health and preventing chronic diseases such as CVD will usually apply to the whole population, including children, unless there are specific arguments for alternative guidelines or recommendations. There is no reason why children should be excluded from the advice to consume at least one to two meals of fatty fish per week as recommended for adults. Establishing a quantitative dietary intake recommendation for EPA and DHA for children aged 2–12 years will require a research programme focusing on well-defined, public health-relevant and age-specific outcomes in this specific age group.
Acknowledgements
All authors reviewed and discussed the available evidence on dietary intakes of EPA and DHA and agreed on the conclusions at the workshop held in July 2007. B. K., A. E., D. M. and S. I. wrote the first draft of the manuscript. All authors reviewed and contributed to the revision of the manuscript.
S. O., D. M., A. E. and P. Z. are employees of Unilever. Unilever markets foods, among which products rich in n-3 fatty acids. Unilever Food and Health Research Institute organised and funded the workshop attended by all authors.
Research by B. K. on functional effects of EPA and DHA has been carried out with partial financial support from the Commission of the European Communities, within the 7th Framework Programme, contract no. FP7-212652. This paper does not necessarily reflect the views of the Commission and in no way anticipates future policy in this area.
B. K. and S. I. are recipients of Freedom-to-Discover Awards of the Bristol-Myers-Squibb Foundation (New York, NY, USA).
R. U. was President of the International Union of Nutrition Sciences (IUNS), he does not receive personal income from Unilever, his research funding comes from the Wellcome Trust and the Chilean Council for Scientific and Technological Development; he declares no conflicting interests relative to the content of this paper.

