



Life events have been defined as discrete or significant experiences that disrupt the usual activities of an individual, resulting in a substantial change and readjustment.Reference Beards, Gayer-Anderson, Borges, Dewey, Fisher and Morgan1 Such events can be considered as stressors, and have been shown to have important effects on health and psychological well-being.Reference Cleland, Kearns, Tannahill and Ellaway2 The effect of life events depends partly on their nature, with undesirable, unpredictable or uncontrollable events more likely to have negative consequences for mental health than events without these characteristics.Reference Avison and Gotlib3 The impact of life events may also depend on the subjective significance given to these events by the individuals who experienced them.Reference Boals4
Life events have been shown to affect the onset, course and outcome of psychotic disorders.Reference Mayo, Corey, Kelly, Yohannes, Youngquist and Stuart5 The biological mechanism through which life events affect psychosis remains unclear,Reference Sumich, Chitnis, Fannon, O'Ceallaigh, Doku and Falrowicz6 although various models have been postulated.Reference Nuechterlein and Dawson7,Reference Selten and Cantor-Graae8 Events throughout the life course, including adverse childhood experiences, have been hypothesised to increase predisposition to psychosis,Reference Faravelli, Catena, Scarpato and Ricca9 whereas recent events occurring shortly before the onset of psychosis may trigger the onset of symptoms in those who are already vulnerable.Reference Horan, Ventura, Nuechterlein, Subotnik, Hwang and Mintz10
Associations between life events and psychosis
A meta-analysis of the association between childhood adverse experiences and psychosis showed a three-fold increase in the odds of psychosis among people who suffered childhood trauma compared with people without such experiences.Reference Varese, Smeets, Drukker, Lieverse, Lataster and Viechtbauer11 The majority of studies that have investigated the associations between recent life events and psychosis have also observed an increase in life events before the onset of psychosis.Reference Beards, Gayer-Anderson, Borges, Dewey, Fisher and Morgan1 However, almost all of these studies were conducted in Western Europe, North America and Australasia, so the extent to which the associations hold in other populations is unknown. Since the effect of life events is dependent on the nature of the events and their significance to those who experienced them, the experience of life events may differ between settings not only in terms of their types and frequency, but also in how they are interpreted and responded to. Further, the impact of life events may be buffered by social support,Reference Morgan and Gayer-Anderson12 which varies both in nature and extent between contexts.Reference Chronister, Chou, Kwan, Lawton and Silver13 Thus, caution must be exercised in generalising findings from Western Europe, North America and Australasia to the rest of the world.
Few studies have investigated the associations between life events and psychosis in the Global South. In Nigeria, Gureje and AdewunmiReference Gureje and Adewunmi14 compared 42 people with a diagnosis of schizophrenia, at their first episode, with 57 controls, and found that the onset of illness among cases was not preceded by an increase in life events relative to controls. In India, Chakraborty et alReference Chakraborty, Chatterjee, Choudhary, Singh and Chakraborty15 compared life events (lifetime, 6 months, 3 months and 2 weeks) occurring in 18 participants before the onset of acute and transient psychotic disorder, and manic episodes occurring in 20 participants. They observed a higher frequency of impersonal events, undesirable events and higher stress scores among those with acute and transient psychotic disorder compared with those with mania without psychosis.Reference Chakraborty, Chatterjee, Choudhary, Singh and Chakraborty15 In a Tanzanian study where 899 community members were studied, individuals who had experienced two or more recent life events in the previous 6 months had higher odds of experiencing psychotic symptoms than those who experienced one or fewer life events.Reference Jenkins R, Mbatia, Singleton and White16 All of these studies explored life events within 6 months preceding onset of psychosis (i.e. recent events that may have triggered psychosis) rather than events occurring across the lifetime (i.e. events increasing vulnerability to psychosis).
Current study
This present study addresses an evidence gap of the possible impact of life events (not restricted to recent events) on the causes of psychosis in more diverse settings.
The objective of this exploratory analysis of data from a pilot study in India, Nigeria, and Trinidad and Tobago is to assess the association between witnessing or experiencing life events and psychotic disorder (both affective and non-affective). This will generate preliminary findings to inform future studies in these countries.
Method
Study design
This is a secondary analysis of data from a case–control study entitled International Research Programme on Psychoses in Diverse Settings I (INTREPID I);Reference Morgan, Hibben, Esan, John, Patel and Weiss17 data were collected in 2014. INTREPID I was a population-based programme designed to implement and evaluate methods of identifying, assessing and following untreated cases of psychosis (affective and non-affective psychosis) and matched controls in catchment areas of India, Nigeria, and Trinidad and Tobago.Reference Morgan, Hibben, Esan, John, Patel and Weiss17,Reference Morgan, John, Esan, Hibben, Patel and Weiss18 It was a pilot study to inform subsequent larger-scale studies.
Setting
Data were collected from catchment areas in three sites: Chengalpet taluk (near Chennai), Tamil Nadu, India (population 412 289);19 Ibadan South East and Ona Ara Ibadan, Oyo-State, Nigeria (population 532 032);20 and Tunapuna-Piarco, Trinidad, Trinidad and Tobago (population 248 656).21
In India, 32.7% live below the poverty line ($1.25 per day)22 and 74% are literate,22 according to 2010 figures. In Nigeria, 68.2% live in poverty22 and 60% are literate.Reference James23 In Trinidad and Tobago, 4% live in poverty22 and 99% are literate.Reference Olojede, Adekunle, Samuel and Esther24 Detailed socioeconomic data are not available at the level of the catchment areas, but more details about the health systems in the catchment areas have been published previously.Reference Morgan, Hibben, Esan, John, Patel and Weiss17
Participant recruitment and sample size
Details on recruitment of cases and controls have been reported previously.Reference Morgan, Hibben, Esan, John, Patel and Weiss17 Brief details are provided below.
Cases sampling and recruitments
Mapping exercises of service providers and investigations of help-seeking patterns in each site established comprehensive, bespoke case detection systems, which incorporated all public and private professional mental health providers, the major spiritual and traditional healers, and a network of key informants.Reference Morgan, Hibben, Esan, John, Patel and Weiss17 These networks are regularly monitored by the research teams in each site to identify potential cases, who were then screened with the Screening Schedule for Psychosis,25 and those who screened positive were invited to participate.
Inclusion criteria for cases
Inclusion criteria were as follows: age 18–64 years, resident in the catchment area at the time of case detection, meet the ICD-10 diagnostic criteria for psychotic disorder in past 12 months and not treated with antipsychotics for 3 continuous months before the start of recruitment.
Exclusion criteria for cases
Exclusion criteria were as follows: evidence of psychotic symptoms precipitated by an organic cause, central nervous system disease and transient psychotic symptoms resulting from acute intoxication.
Control sampling and recruitments
Controls were individually matched to cases by gender, age and neighbourhood; Trinidad and Tobago also matched by ethnicity. To identify controls, the ten most proximal households to where each case lived were identified, and each of these ten households were then contacted. The age and gender of each resident was recorded, and all gender- and age- (within 5 years of the case) matched residents were listed in random order and approached consecutively until a suitable control was recruited. If a suitable control was not recruited from the list of ten households, the process was repeated with the next ten households.
Inclusion criteria for controls
Inclusion criteria were as follows: residents in catchment areas, aged 18–64 years, within 5 years of age of the matched case, same gender as matched case, screened negative for psychosis with the Screening Schedule for Psychosis25 not related to the cases and consented to participate.
Data collection
Data were collected by trained research workers via face-to-face interviews.
Measures
The Screening Schedule for Psychosis25 was used to screen all potential cases and controls to determine eligibility. This has been widely used to screen for psychosis across settings.
The Schedule for Clinical Assessment in NeuropsychiatryReference Jablensky, Sartorius, Ernberg, Anker, Korten and Cooper26 interview was used to confirm diagnosis in cases and was administered by experienced clinicians in each site.
The Medical Research Council Sociodemographic Schedule27 was used to collect information about gender, age, education level, employment status, income, housing and relationship status. Information regarding income was obtained in the local currency of each country, which was then grouped by centiles within each site into ‘high’, ‘middle’ and ‘low’ to relativise them to the setting; these values were then converted to dollars, using the exchange rate for the year of the study.Reference Mallett28–30 Educational level was operationalised based on the number of years spent schooling, and then grouped.
The Global Assessment of Functioning31 is a numeric scale used to rate individuals’ social, occupational, and psychological functioning. The split version with separate scales for symptoms and functioning/disability was used.Reference Jones, Thornicroft, Coffey and Dunn32
The Harvard Trauma Questionnaire (HTQ) (Supplementary Material available at https://doi.org/10.1192/bjo.2022.562) was used to assess lifetime occurrence of traumatic life events among study participants.Reference Pedersen, Hagtvet and Karterud33 It contained a list of 17 traumatic events with options to mark as ‘no event’, ‘witnessed’ and ‘experienced’. Traumatic events were recorded as ‘no event’ (0) and ‘witnesses or experienced’ (1). The time period when the life event occurred was not indicated.
Statistical analysis
A descriptive exploration of the data was conducted by examining the variables range, mean and s.d. (for normally distributed continuous variables), median and interquartile range (for continuous variables with skewed distributions), percentages (for categorical variables) and missing values. Histograms were plotted to assess the distributions of the continuous variables.
Cross-tabulations were used to summarise sociodemographic characteristics, clinical characteristics and exposure to life events by case–control status. Fishers exact test was used when cells contained five or fewer participants. Life events were the main exposure of interest and were treated as a continuous variable. Individuals who reported having either experienced or witnessed a life event were categorised as exposed.Reference Pedersen, Hagtvet and Karterud33
As cases and controls were individually matched on age group, gender and neighbourhood, a matched analysis was conducted, using conditional logistic regression to estimate odds ratios and 95% confidence intervals. We first performed univariable analysis, and then proceeded to multivariable analysis, adjusting for potential confounders (age and educational level). Even though participants had been matched by age group (within 5 years), we still adjusted for age since it was not an exact age match. Sensitivity analyses were conducted with unconditional logistic regression, adjusting for matching factors. The effect of each potential confounder was explored individually on the association between life events and psychosis, and those that changed the odds ratio by 10% or more were included sequentially into the model. The final model was chosen after assessing the fit of the models with likelihood-ratio tests. Since a matched analysis was carried out, only matched pairs contributed to the analysis; as such, five participants with missing items or unmatched sets were dropped from the analysis.
The data were analysed with statistical software Stata version 15.1 for Windows.
Ethics
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. All procedures involving human patients were approved by the Psychiatry, Nursing and Midwifery Research Ethics Subcommittees of King's College London (approval number PNM1213 119), the Institutional Ethics Committee of the Schizophrenia Research Foundation in India, the University of Ibadan Ethics Committee in Nigeria and the University of the West Indies St Augustine Campus Ethics Committee in Trinidad and Tobago, and permission was also granted by all the relevant local health authorities for the parent study.
Ethical approval for this secondary data analysis was obtained from the London School of Hygiene and Tropical Medicine MSc Research Ethics Committee (approval number 17044).
All participants were informed about the study, that the data would be anonymised and that they were free to withdraw from the study at any time. A written information sheet in the local language was provided to the participants; this was signed by all literate participants and read out to non-literate participants in the presence of a witness, to obtain recorded verbal informed consent.
Results
Sociodemographic characteristics of the study population
Overall, 97 cases and 97 controls were included in the study. The mean age of cases was 35 years (s.d. 10.8) and the majority (61.5%) were female. There was evidence that cases had lower levels of education, were less likely to be employed and were more likely to be living with their parents (Table 1).
Table 1 Sociodemographic and clinical characteristics of cases and controls
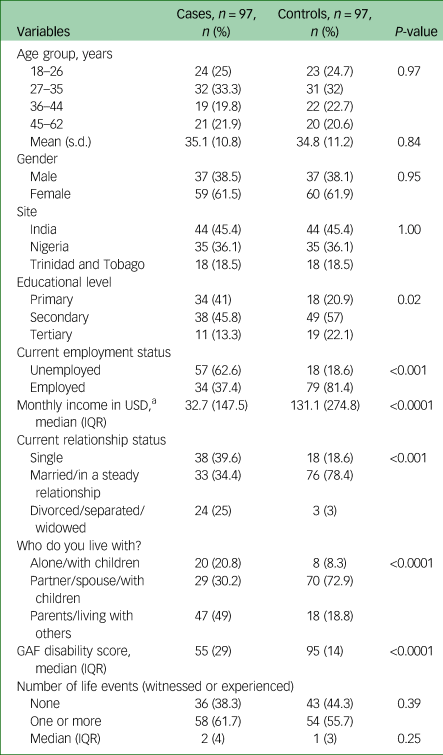
USD, United States Dollars; IQR, interquartile range; GAF, Global Assessment of Functioning.
a. 2014 currency rate 1USD = 61.00759 Indian Rupees,Reference Mollica, Caspi-Yavin, Bollini, Truong, Tor and Lavelle34 1USD = 156.483 Nigerian NairaReference Marshall, Lewis, Lockwood, Drake, Jones and Croudace35 and 1USD = 6.3613 Trinidad and Tobago Dollars.Reference Raune, Kuipers and Bebbington36
Among the cases, 61.7% reported witnessing or experiencing lifetime traumatic events, compared with 55.7% of the controls experiencing at least one life event during their lifetime (P = 0.39; Table 2).
Table 2 Lifetime exposure to life events among participants in India, Nigeria, and Trinidad and Tobago
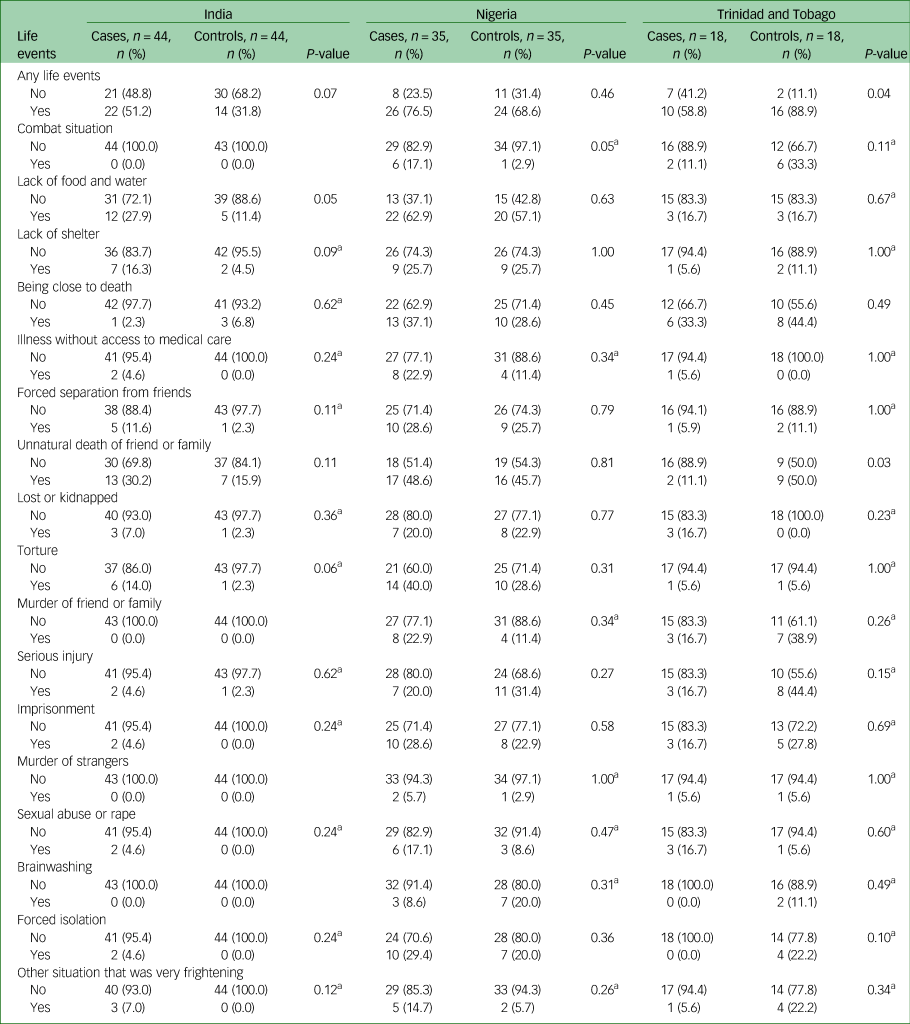
a. Fisher's exact test.
Life events were explored by site. Regarding the total number of life events experienced by participants, in India, 51.2% of cases reported witnessing or experiencing lifetime traumatic events, compared with 31.8% of controls (P = 0.07). In Nigeria, 76.5% of cases reported witnessing or experiencing lifetime traumatic events, compared with 68.6% of controls. In Trinidad and Tobago, 58.8% of cases reported witnessing or experiencing lifetime traumatic events, compared with 88.9% of controls (P = 0.04).
Association between life events and psychosis
The crude odds ratio of the association between psychosis and life events witnessed or experienced (as binary) was 1.32 (95% CI 0.72–2.39). Age and education were independently associated with the outcome, and adjustment for age and education yielded an adjusted OR (aOR) of 1.19 (95% CI 0.62–2.28) for the association between psychosis and life events witnessed or experienced. Fitting number of life events as a continuous exposure showed little evidence of extra-linear variability, with an increase in odds of psychosis for every additional life event experienced (aOR 1.07, 95% CI 0.92–1.24).
The sensitivity analysis using unconditional logistic regression showed similar results (aOR for the association of psychosis with binary exposure 1.32, 95% CI 0.71–2.46; aOR for association with every additional life event experienced 1.05, 95% CI 0.95–1.17).
There was evidence of an interaction between life events and country (P = 0.002). The aOR for the association between number of life events and psychosis was 1.56 (95% CI 1.03–2.35) for India, 1.17 (95% CI 0.95–1.45) for Nigeria, and 0.66 (95% CI 0.45–0.97) for Trinidad and Tobago (Table 3).
Table 3 Site-specific association with number of life events (as a continuous variable)

a. Adjusted for age group and education level. Test of homogeneity, P = 0.002.
Discussion
This study found no evidence of an association between increased exposure to life events and psychosis.
However, there was evidence of effect modification by site, with evidence of an association observed in India, no evidence of an association in Nigeria, and evidence that controls were more exposed to life events in Trinidad and Tobago (number of controls with life event divided by the total number of controls v. number of cases with life event divided by the total number of controls: 16/18 (88.9%) v. 10/18 (55.6%)). The reversal in the association between life events and psychosis in Trinidad and Tobago may be a result of recall bias owing to differences in education and symptom profile. Again, these findings should be treated with caution because of the small numbers in each group. This study also provided very preliminary evidence of increased exposure to specific life events among cases compared with controls.
Strengths and weaknesses
This was a small pilot study with 194 participants (97 cases and 97 controls), which limited the power of the study. A strength of this study was its use of a representative sample of cases obtained via rigorous, comprehensive case-finding methods, which drew on religious and traditional healing sites and key informants in addition to mental health services, unlike studies that recruit solely from psychiatric facilities,Reference Canton and Fraccon37,Reference Kulhara and Wig38 which are unlikely to be representative of people with psychosis in the general population, especially in low-resource settings where many do not present to formal psychiatric services. To our knowledge, this is the first study to examine life events across multiple countries in the Global South.
An important limitation in interpreting the findings is the difficulty of determining the direction of causation, because the timing of life events and psychosis was not indicated in this study, and the median duration of untreated psychosis was 232 weeks, 13 weeks and 38 weeks in India, Nigeria, and Trinidad and Tobago, respectively.Reference Morgan, Hibben, Esan, John, Patel and Weiss17 Determining the timing of life events among individuals with and without psychosis will be important in future studies to provide evidence of a causal association, and to achieve a better understanding of the effect of childhood versus recent life events on psychosis.
Some important life events of relevance to people in India, Nigeria, and Trinidad and Tobago may not have been fully captured by the HTQ. For instance, the HTQ does not include job losses, unemployment and relationship challenges. These are common occurrences with major potential ramifications, particularly in low- and middle-income countries with little or no welfare or unemployment benefits. This may also highlight the subjective effect of life events on different individuals; it is theoretically possible that the events included in the questionnaire are not those that are experienced to be most intrusive or traumatic in all cultural settings. Although the HTQ has been widely used and validated in the Global South,Reference Kulhara and Wig38 it has been mainly used to assess post-traumatic stress disorder in these settings. It has not been validated in India, Nigeria, or Trinidad and Tobago, but it has been used in diverse populations such as Indochinese,Reference Pedersen, Hagtvet and Karterud33 Iraqi refugeesReference Makanjuola and Adedapo39 and refugees from Sub-Saharan Africa to France,Reference Shoeb, Weinstein and Mollica40 among others. Omission of locally salient life events may have led us to underestimate the prevalence of traumatic life events. The use of a locally generated life event scale may be important to consider in capturing life events of importance in different sites.
It is possible that some variables that we treated as confounders could lie on the causal pathway, such as education; however, there was very minimal change in the results when education was excluded.
Since this study is a case–control study, recall bias cannot be ruled out. However, recent studies suggest that the accuracy of reported life events by people with psychosis is high.Reference de Fouchier, Blanchet, Hopkins, Bui, Ait-Aoudia and Jehel41 Since data were collected through face-to-face interviews, and some of the items in the HTQ are sensitive, reporting bias is also a possibility, especially if relatives are more likely to be present during interviews with cases than with controls (as is common when conducting research in settings such as rural India). This may have differentially affected data from different sites, given variation in cultural norms.
Comparison with other studies
This study included more women than men (61.5% v. 38.5%). This is in contrast to findings from higher-income countries. where typically there are more men than women with psychotic disorders.Reference Mollica, Caspi-Yavin, Bollini, Truong, Tor and Lavelle34 This finding may be directly related to the active case finding method employed in this study,Reference Morgan, Hibben, Esan, John, Patel and Weiss17 as well as differences in risk of psychosis among men and women in different populations. Individuals with psychosis did not experience a significantly higher median number of overall life events than controls, and there was no overall evidence of an association between total number of events experienced and odds of psychosis. This association is not in the same direction as most studies conducted in Europe, North America and Australasia,Reference Marshall, Lewis, Lockwood, Drake, Jones and Croudace35,Reference Raune, Kuipers and Bebbington36 which have found a positive association between exposure to life events and psychosis.
The lack of an association in the current study may be because a majority of participants reported exposure to life events: 58% of cases and 54% of controls. Alternatively, it is possible that protective factors such as social support may be more prevalent in some settings, which cushion the effects of life events. Another possible reason for this lack of association may be the higher percentage of women among our study population. Zarulli et alReference Fisher, Craig, Fearon, Morgan, Dazzan and Lappin42 found that women were more resilient and survived better even during harsh conditions. A previous Nigerian study of life events among patients with first-episode schizophrenia also found no significant difference in the number of life events between patients and controls 6 months before the first episode.Reference Gureje and Adewunmi14
Some of the life events seemed to be more common among individuals with psychosis than the controls, and others were not, although this must be interpreted with caution because of multiple testing. There was some evidence in this study that lack of food and water, as well as torture in India and combat situation in Nigeria, may be associated with increased odds of psychosis. Some evidence suggests that events that are threatening, intrusive or involve a lack of control (such as physical assaults or invasive operations) specifically increase susceptibility to psychosis.Reference Beards, Gayer-Anderson, Borges, Dewey, Fisher and Morgan1 It is also possible that these events (lack of food and water, torture, combat situations) have an additive effect with current and long-standing social disadvantages. such as unemployment, living alone, being single and lower levels of education.Reference Zarulli, Jones, Oksuzyan, Lindahl-Jacobsen, Christensen and Vaupel43
The HTQ has generally been used to measure exposure to life events among groups who have faced adversity, such as refugees, rather than the general population. These studies typically show a higher prevalence of exposure to traumatic events than observed in our study; for example, a study of Mandaean refugees in SydneyReference Morgan, Charalambides, Hutchinson and Murray44 found that 40%, 69%, 54% and 30% of the participants experienced torture, lack of food and water, illness without access to medical care and lack of shelter, respectively, compared with 23%, 39%, 11% and 18%, respectively, for the participants of this study. More research is needed to assess the extent to which variation in exposure to traumatic life events contributes to variation in the incidence of psychosis across settings.
Because of the small sample size of the current study, it was not possible to investigate interactions between different factors or compare the prevalence and impact of specific types of events between settings.
Recommendations for future research
If confirmed in larger studies, potential implications of these preliminary findings could include the provision of trauma-informed services for individuals with psychotic disorders and policies targeted at reducing exposure to trauma (e.g. child protection interventions), to reduce the incidence of psychosis. International Research Programme on Psychoses in Diverse Settings II (INTREPID II),Reference Steel, Silove, Brooks, Momartin, Alzuhairi and Susljik45 which is the next phase of this study, will attempt to replicate these findings with larger samples. Future research must capture the timing of life events to establish the temporal order of these relative to the onset of psychosis, as well as the relative importance of recent events and earlier exposure. The local validity of the HTQ to capture the most relevant events to each setting should also be explored, and researchers should consider adapting these measures as needed. With larger samples, it should also be possible to investigate the impact of specific types of events, and interactions between exposure to life events and other forms of disadvantage as well as protective factors, to better understand the causes of psychosis and identify opportunities for intervention. Finally, protective factors such as social support that may buffer the effects of life events across diverse settings, potentially leading to less strong associations with psychosis in some contexts, should be investigated.
In conclusion, this exploratory study showed no overall evidence of an increase in the odds of psychosis with increasing exposure to life events, in three culturally and economically diverse countries of the Global South; however, there was some evidence of variation across settings. Further studies with larger samples should attempt to replicate these findings.
Supplementary material
Supplementary material is available online at https://doi.org/10.1192/bjo.2022.562
Data availability
Data is available upon reasonable request to C.M. ([email protected]).
Author contributions
S.J., M.H., O.E., R.T., O.G., G.H., V.P., H.A.W., R.M.M., A.C. and C.M. contributed to the design and conduct of the original INTREPID I study. I.O.O. and T.R. conceptualised the research idea for this secondary analysis. I.O.O. analysed the data and wrote the draft manuscript, which T.R. and C.M. commented on and revised. H.A.W. provided advice on statistical methods and interpreting the results. C.M. contributed to the interpretation of data. All authors reviewed the manuscript and approved the final submission.
Funding
The pilot study was funded by the Wellcome Trust (grant number WT094525 awarded to C.M.), and further supported by the US National Institute for Mental Health Research (grant number R21- MH093304-01).
Declaration of interest
None.






 Open access
Open access
eLetters
No eLetters have been published for this article.