



The potential dramatic consequences of coercive measures such as seclusion, restraint and forced medication are well-known.Reference Chieze, Hurst, Kaiser and Sentissi1 There is great variation in the use of coercion among countries, regions and institutions that has not been fully explained to date. Factors directly related to staff members have been discussed as potentially influencing the use of coercion,Reference Zinkler and Priebe2 and professionals’ attitudes towards coercion have been investigated as potential factors that might reflect individual and institutional perceptions of coercive practices.Reference Husum, Bjørngaard, Finset and Ruud3–Reference Efkemann, Scholten, Bottlender, Juckel and Gather5
Cultural, ward-related, individual and patient-related factors all seem to influence staff members’ attitudes.Reference Happell and Koehn6 Regarding differences between professional groups, a study reported that psychiatrists and psychologists tend to have more critical, less positive attitudes towards coercion than nurses.Reference Lickiewicz, Husum, Ruud, Siqveland, Musiał and Makara-Studzińska7 Another study yielded similar results, with psychiatrists, especially senior clinicians, and experienced staff members showing more critical attitudes towards coercion.Reference Morandi, Silva, Mendez Rubio, Bonsack and Golay8 An Indian study also found that psychiatrists tended to have a more critical view of coercion compared with patients’ relatives.Reference Raveesh, Pathare, Noorthoorn, Gowda, Lepping and Bunders-Aelen9 Steinert et al also showed that social workers and psychologists tended to approve coercion less than psychiatrists or nurses,Reference Steinert, Lepping, Baranyai, Hoffmann and Leherr10 and findings by Vandamme et al similarly supported the hypothesis that nurses were more positive regarding the use of coercion.Reference Vandamme, Wullschleger, Garbe, Cole, Heinz and Bermpohl11
Recent work by Krieger et al supported the hypothesis that staff attitudes are directly related to particular emotional aspects linked to their experiences at work.Reference Krieger, Moritz, Lincoln, Fischer and Nagel12 As an example, high levels of emotional exhaustion are related to more positive appraisal of coercion among nurses.Reference Happell and Koehn13 Most studies show that staff members tend to have a pragmatic view of coercion as necessary for providing care and security.Reference Husum, Siqveland, Ruud and Lickiewicz4,Reference Doedens, Vermeulen, Boyette, Latour and de Haan14 Regarding this aspect, the perceived level of aggression on wards and the impression of insufficient safety measures seem to be associated with the use of coercion.Reference De Benedictis, Dumais, Sieu, Mailhot, Létourneau and Tran15 Nurses’ feeling of safety was also shown to be potentially associated with the use of seclusion in another study.Reference Vollema, Hollants, Severs and Hondius16 According to the scientific literature, nurses are among the professional categories most at risk of experiencing violence at work during their career, especially in mental health settings.Reference Rasmussen, Hogh and Andersen17,Reference Bilici, Sercan and Izci18 A history of assault by a patient was found to be associated with more frequent use of mechanical restraint in a study by Moyan and colleagues.Reference Moylan and Cullinan19 Violence and coercion in psychiatric care are thus highly entangled issues. However, there has not yet been any research investigating the influence of experience by staff members of violence and their attitudes towards coercion.
The present work thus aimed to investigate potential correlates of attitudes of staff members towards coercion, especially their experience of violence in the workplace. We hypothesised that experiences of violence at work would be correlated with less critical, more positive attitudes towards coercion.
Method
Participants and procedures
This was an observational, cross-sectional study. Staff members of the Department of Psychiatry of the Geneva University Hospital were contacted and asked to complete a single anonymous online survey (n = 881). These included nurses, psychiatrists, psychologists, social workers, occupational and psychomotor therapists, and administrative and cleaning staff.
Study data were collected through an anonymous online questionnaire using the Research Electronic Data Capture (REDCap) tools.Reference Harris, Taylor, Thielke, Payne, Gonzalez and Conde20,Reference Harris, Taylor, Minor, Elliott, Fernandez and O'Neal21 The survey included comprehensive information about the study protocol, and participants were asked to give their explicit consent to participation. Data were gathered during an 8 month period.
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. The local ethics committee waived the project because it did not fall under national legislation on human research (Commission cantonale d’éthique de la recherche; no. 2021-00303).
Legal framework of coercive measures in Switzerland
The Swiss Civil Code regulates the use of coercive measures in Switzerland. Measures physically limiting movement such as seclusion or mechanical restraint are only allowed in cases of severe danger to oneself or others, or serious disruption to community life. All decisions to apply a coercive measure are prescribed by medical doctors after the approval of a senior physician. Prescriptions are valid for a 24 h period and must be renewed if necessary. A written decision is handed to the patient or his/her authorised representatives. Patients can appeal against this decision within 10 days.
Outcomes and instruments
Sociodemographic data
We collected data regarding gender, age category, job position, part-time activity, service, work setting (in- or out-patient) and years of experience in psychiatry.
Experience of violence in the workplace and feeling of insecurity
Using an ad hoc questionnaire developed for the project, the following data were gathered: experience of violent events (physical or verbal assault) during the past 12 months; nature and number of events experienced, number and duration of periods of sick leave following a violent incident during the past 12 months; feeling of insecurity at work, rated on a visual analogue scale ranging from 0 (no insecurity) to 100 (extreme insecurity); quality of support received after violent events, rated on a five-point Likert scale; and completion of violence prevention training in the past 3 years. Participants were also asked whether they had witnessed or used coercive measures (seclusion, restraint, forced medication) during the past 12 months and to rate the emotional burden of such measures on a scale ranging from 0 (no burden) to 100 (extreme burden).
Attitude to coercion
Staff attitudes to coercion were assessed with the Staff Attitude to Coercion Scale (SACS).Reference Husum, Finset and Ruud22 The SACS comprises 15 items rated using a five-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree) and assesses three dimensions of the individual's attitude towards coercion. Critical attitude relates to coercion as offensive towards patients. It includes six items with a score range of 6–30. The higher the score, the more staff perceive coercion as offending patients. Pragmatic attitude views coercion as a means of providing care and safety. It consists of six items and scores between 6 and 30. Higher scores indicate greater appraisal of coercion as necessary for care and security reasons. Positive attitude relates to coercion as treatment and consists of three items (scores 3–15). Here, higher scores indicate a stronger perception of coercion as necessary for treatment. A French translation of the instrument was made for this study using a back-translation method. The original scale showed good psychometric properties.Reference Husum, Finset and Ruud22 Internal consistency as assessed for each dimension by Cronbach's alpha coefficient was 0.70 for critical attitude, 0.73 for pragmatic attitude and 0.69 for positive attitude. For our study, these coefficients were 0.78, 0.81 and 0.68, respectively.
Symptoms of burnout
To assess the presence and intensity of burnout symptoms, we used the French version of the Oldenburg Burnout Inventory (OLBI).Reference Demerouti, Bakker, Vardakou and Kantas23,Reference Chevrier24 The OLBI is a 16-item self-rating instrument that assesses two core dimensions of burnout, namely exhaustion and disengagement. Each dimension comprises eight items whose ratings range from 1 (strongly agree) to 5 (strongly disagree). Negatively worded items (four in each dimension) are reversed-scored so that higher scores for each item correspond to more negative responses. Hence, higher scores indicate higher levels of exhaustion and disengagement, respectively. The score range of each dimension is from 8 to 32 The French version showed good psychometric properties, with Cronbach's alpha of 0.81 for the exhaustion subscale and 0.69 for the disengagement subscale.Reference Chevrier24 In the current study, the Cronbach's alpha coefficients were 0.86 and 0.73, respectively.
Statistical analyses
Descriptive statistics such as mean and standard deviation or percentages were computed to summarise participants’ characteristics.
We addressed the research question by fitting a multivariate multiple linear regression, a statistical method used to assess the effects of a set of covariates on more than one dependent variable. The Pillai's trace statistic, known for its robustness to departure from normality and adequate power to detect true differences in a variety of situations, was used to test the hypothesis that the explanatory variables have a significant effect on the dependent variables.Reference Olson25,Reference Pituch and Stevens26 The overall null hypothesis test for the multivariate model is H 0: B = 0. Its values range from 0 to 1, and increasing values mean that effects are significant, rejecting the null hypothesis that the coefficients are 0. Beforehand, the modelling of separate regressions with the same regressors was deemed necessary. As we had multiple responses, the assumption of multivariate normality of the residuals was also assessed through the Shapiro–Wilk test.
Hence, the three SACS subscale scores (critical, pragmatic and positive attitudes), used as dependent variables, were modelled as functions of age (≤29 years v. 30–39 years, v. 40–49 years v. ≥50 years); gender (female v. male); job position (nursing assistant/nurse v. medical doctor v. occupational therapist/psychologist); experience of violent events during the past 12 months (yes v. no); feeling of insecurity, exhaustion or disengagement (OLBI scores); experience with coercion during the past 12 months (yes v. no); years of professional experience; work setting (in-patient v. out-patient); and emotional burden of coercive measures as covariates. The choice of explanatory variables was determined by previous scientific findings and driven by our main hypothesis.Reference Husum, Siqveland, Ruud and Lickiewicz4 Categorical variables with k categories were transformed into k − 1 dummy variables to be considered in the regression, the k th being set aside as the reference category against which all other categories were compared. These were younger age, male gender, nursing assistant/nurse position, out-patient setting, absence of a violent event and no use of coercion. When performing multivariate multiple linear regressions, the same covariates and the same reference category must hold during the phase of the multiple regression procedure for the overall multivariate test to be valid.
The core assumptions made by multiple linear regression (normality, linearity, homoscedasticity and independence of residuals) were assessed through plots of residuals in routine pre-analysis screening.Reference Tabachnick, Fidell and Ullman27 In cases of multicollinearity, any value of the variance inflation factor greater than 5 should be a matter for concern.Reference Sheather28
Missing values
Four-hundred and seventy-seven records were extracted from the REDCap platform. After exclusion of those who did not consent to participate, we were left with a sample of 468 respondents, with incomplete data up to 8%. Missingness was dealt with using the expectation-maximisation algorithm, a single-imputation simulation technique which imputes missing values by an iterative procedure. Missingness by design, i.e. when responses are not expected for respondents who do not experience a particular event, was not imputed.
Sample size estimate
Based on a previous study conducted in the Department of Psychiatry, a response rate of about 30% (or 300 participants) was expected.Reference Bartolomei, Baeriswyl-Cottin, Framorando, Kasina, Premand and Eytan29 Referring to Green, the common rule-of-thumb sample size calculation for univariate multiple regression models is N ≥ 50 + 8 m, where m is the number of predictors.Reference Green30 Adapting this rule for the multivariate case (N ≥ 3 × 50 + 8 m) led to a minimum sample of 270 people (three dependent variables and 15 common predictors). Of note, the 45 administrative and cleaning staff who were part of the survey were excluded from the regression analyses as they had no direct contact with coercive measures, unlike the health professionals. Thus, the sample of 423 participants was sufficient to address the research questions.
For all analyses, significance was set at P < 0.05. We used IBM SPSS for estimation of missing values and R to conduct the multivariate procedures, in particular, the ‘car’ and ‘mvnormtest’ packages.31,32
Results
Descriptive analysis
Descriptive statistics are summarised in Table 1. Overall, 468 participants responded to the survey (response rate: 53.1%). Participants were predominantly women (63.9%), nursing assistant/nurses (56.6%) and worked in an in-patient setting (64.1%). A majority had used or witnessed coercive measures during the past 12 months (67.5%), 27.1% had experienced physical assault at the workplace during the same period, and 71.6% were victims of verbal assault. Only 34.6% of the participants had received violence prevention training over the past 3 years.
Table 1 Characteristics of surveyed participants

OLBI, Oldenburg Burnout Inventory; SACS, Staff Attitude to Coercion Scale.
a. Only variables in the regression models and auxiliary variables that may have contained information about the missing data were imputed.
Regression analysis
No violations of key assumptions for conducting multiple regression were detected. There was no multicollinearity between the covariates, as evidenced by the variance inflation factor (no value exceeding 5).
The results of three separate standard multiple linear regressions with (a) critical attitude, (b) pragmatic attitude and (c) positive attitude subscores as dependent variables are given in Table 2. The adjusted R-squared values were 20% for SACS critical attitude, 12% for SACS pragmatic attitude and 14% for SACS positive attitude.
Table 2 Multiple regression estimates for SACS critical, pragmatic and positive attitudes
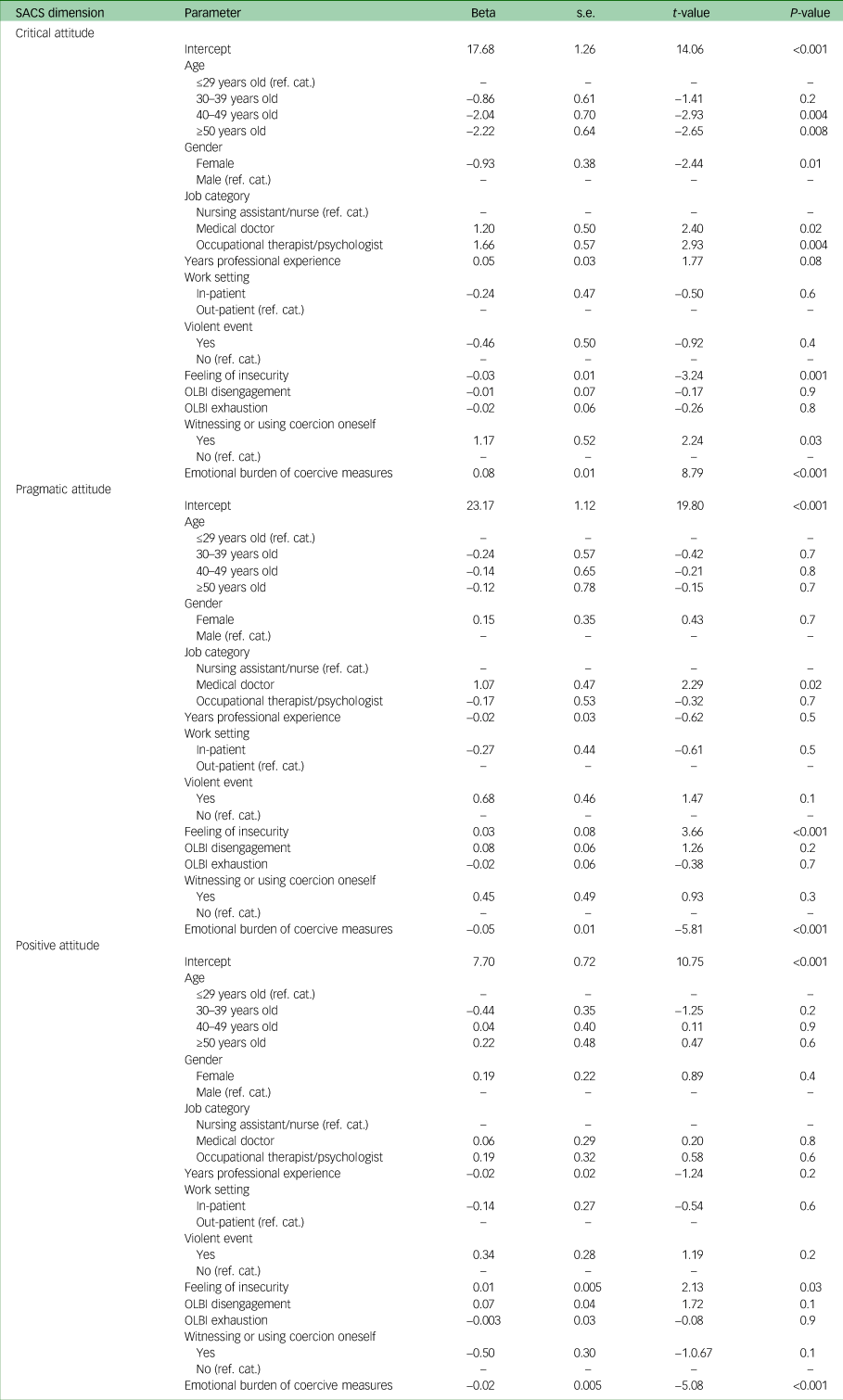
SACS, Staff Attitude to Coercion Scale; ref. cat., reference category; OLBI, Oldenburg Burnout Inventory.
Critical attitude
Considering SACS critical attitude, age, gender, job category, feeling of insecurity, using or witnessing coercion, and emotional burden of coercive measures were significantly associated with the dependent variable. Older age was negatively associated with critical attitudes (P = 0.004 and P = 0.008 for 40–49 and 50+ years, respectively). In other words, older staff members were less likely to perceive coercion as offending patients compared with the ≤29-year-old category. Similarly, gender and feeling of insecurity were negatively associated with the dependent variable (P = 0.01 and P = 0.001, respectively). Compared with males, females perceived coercion as less offending. Likewise, staff members showing higher levels of insecurity were less critical towards coercion. Conversely, job category, witnessing or using coercion, and the emotional burden associated with coercive measures were all positively associated with the dependent variable. Compared with nursing assistants/nurses, psychiatrists and occupational therapists/psychologists were more likely to score high on this scale (P = 0.02, P = 0.004). The same was true for participants having witnessed or used coercion compared with those who did not (P = 0.03). Likewise, the level of emotional burden was positively associated with critical attitude scores (P < 0.001). Experience of violent events in the past 12 months was not significantly associated with critical attitude subscale scores (P = 0.4).
Pragmatic attitude
Regarding the SACS pragmatic attitude subscale, job category, feeling of insecurity and emotional burden of coercive measures all had significant effects on the dependent variable. Compared with nursing assistants/nurses, being a medical doctor had a positive association with the dependent variable. In other words, medical doctors viewed coercion as necessary for safety and security reasons more than nurses (P = 0.02). Higher levels of perceived insecurity were also associated with higher subscale scores (P < 0.001). For the emotional burden, a negative association was observed. Reporting of high levels of emotional burden associated with the use of coercive measures was correlated with lower appraisal of coercion as necessary for safety reasons (P < 0.001). There was no association with experience of violent events (P = 0.1).
Positive attitude
Regarding SACS positive attitude, feeling of insecurity and emotional burden of coercive measures were the only significant covariates. Indeed, a feeling of insecurity was positively associated with the dependent variable. Higher levels of insecurity were correlated with a stronger perception of coercion as a treatment intervention (P = 0.03). On the contrary, the emotional burden of coercive measures was negatively associated with this subscale. Higher experienced emotional burden in relation to the use of coercion was associated with a less positive attitude (P < 0.001). There was no difference between nurses and medical doctors, nor between nurses and occupational therapist/psychologists (P = 0.8 and P = 0.6, respectively). There was also no influence of experience of violent events (P = 0.2).
Multivariate regression
The result of the Shapiro–Wilk test for multivariate normality of the residuals was W = 0.92 (P < 0.001).
Pillai's multivariate test of significance (F = 5.17, P < 0.001) showed that age, job category, feeling of insecurity, witnessing or using coercion, and emotional burden related to coercive measures had joint significant effects on the three dependent variables. More precisely, the null hypothesis that the coefficients for age classes 40–49 and ≥50 years, being a medical doctor or occupational therapist/psychologist, feeling of insecurity, witnessing of using coercion oneself, and emotional burden of coercive measures were zero were rejected at P < 0.05 (details are shown in Table 3). The experience of violent events had no influence on the three dependent variables (P = 0.05).
Table 3 Multivariate regression results for SACS subscores

SACS, Staff Attitude to Coercion Scale; Den, denominator; Num, numerator; OLBI, Oldenburg Burnout Inventory; ref. cat., reference category.
Sensitivity analysis
To rule out potential biases induced by including professionals not directly involved in the decision-making processes related to coercive measures, we performed a sensitivity including only nurses and psychiatrists as professional categories. The results of the multivariate regression analysis did not differ from those of the main analysis, except with respect to age. Indeed, job position, feeling of insecurity, witnessing or using coercion and emotional burden of coercive measures had joint significant (P < 0.05) effects on the three dependent variables.
Discussion
The present work investigated the determinants of the attitudes of staff members towards coercion, especially regarding the experience of violent events. The main hypothesis was that the experience of violence in the workplace would be related to a less critical attitude towards coercion.
Our results invalidate this hypothesis, as the experience of violent events in the workplace was not associated with attitudes towards coercion. However, our analysis showed that a feeling of insecurity was significantly associated with a less critical, more positive attitude. This discrepancy seems to indicate that attitudes towards coercion might be influenced not by the experience of violence but rather by the ability to handle the potential for violence and feelings of insecurity. This decisive role of insecurity confirms previous scientific findings.Reference Doedens, Vermeulen, Boyette, Latour and de Haan14,Reference Cusack, McAndrew, Cusack and Warne33,Reference Goulet and Larue34 It can be hypothesised that feeling unsafe or not in the capacity of handling violent situations might reinforce the vision of coercion as an important, positive means of protection and care. Staff members night thus use coercive measures as means of dealing with the apprehension of violence, while minimising their deleterious consequences. The fact that about two-thirds of our sample had not received any type of violence management training in the past 3 years should be regarded in the light of these results as problematic. As the literature has shown, effective and regular staff training could help to prevent the use of coercive measures and positively influence attitudes towards coercion.Reference Husum, Siqveland, Ruud and Lickiewicz4,Reference Needham, Abderhalden, Halfens, Dassen, Haug and Fischer35,Reference Price, Baker, Bee and Lovell36 Such training should provide staff members with de-escalation techniques and alternatives to coercive measures. Special institutional attention should also be paid to support of staff members regarding their feelings of safety, including regular clinical team supervision.
Our results also show that psychiatrists and psychologists/occupational therapists have more critical attitudes towards coercion than nursing staff. This confirms previous literature findings.Reference Steinert, Lepping, Baranyai, Hoffmann and Leherr10,Reference Krieger, Moritz, Lincoln, Fischer and Nagel12 These results should be carefully considered and discussed. There are major differences between professions in terms of responsibilities regarding coercive measures, as psychiatrists hold the power to decide to use such measures, even if the situation is discussed with other professionals. Psychologists and occupational therapists are normally not directly involved in the decision-making process but rather witness coercive measures being used. It can thus be hypothesised that the influence of job position on attitudes towards coercion is mediated by the role of professionals regarding coercive measures.
As Morandi et al have shown, psychiatrists tend to experience more external pressures (issues that drive the use of coercive measures) and internal pressures (ethical conflicts).Reference Morandi, Silva, Mendez Rubio, Bonsack and Golay8 Differences are also notable in the daily activities of health professionals regarding patient contact, with nursing staff engaging in much closer and intensive contact with patients in hospital. The frequency and intensity of these contacts might thus affect the experience of insecurity or the appraisal of a patient's clinical state, in turn influencing one's appraisal of coercion.
Having used or witnessed a coercive measure during the past 12 months was associated with a more critical attitude. This finding should be carefully interpreted as it seems to be in contradiction with previous findings.Reference Morandi, Silva, Mendez Rubio, Bonsack and Golay8,Reference van Doeselaar, Sleegers and Hutschemaekers37–Reference Molewijk, Kok, Husum, Pedersen and Aasland39 However, most of these previous studies used instruments and scales other than the SACS, limiting the comparability of results. A study by Molewijk et al using the SACS showed that staff members who experienced coercion at least weekly were more likely to have a pragmatic attitude compared with those who never or rarely experienced it.Reference Molewijk, Kok, Husum, Pedersen and Aasland39 Regarding interpretation of our finding, it must be mentioned that our Department has been progressively implementing a broad coercion reduction programme over the past years. Thus, staff members were probably already influenced in their perceptions of the more negative aspects of coercive interventions. Furthermore, although a large proportion of staff members took part in the study, we cannot exclude an influence of selection bias, as the staff members most engaged in the matter of coercion reduction could have been more likely to answer the survey. Further qualitative distinctions should also be made in future research to understand potential differences between using or witnessing coercive measures regarding staff members’ attitudes. As discussed above, these differences might reflect different intensities and frequencies of patient contact. The frequency of experiences with coercion and more or less active roles in decision-making could also be interesting variables for a future analysis.
Notably, the emotional burden associated with the use of coercive measures was associated with less positive, more critical attitudes towards coercion, a result in line with previous findings by Krieger and colleagues, who completed the SACS by adding new items to assess staff members’ views and emotions about coercion.Reference Krieger, Moritz, Lincoln, Fischer and Nagel12 As the SACS assesses mostly cognitive aspects of attitudes towards coercion, assessment of the emotional burden associated with coercion sheds important light on the determinants of these attitudes.Reference Efkemann, Scholten, Bottlender, Juckel and Gather40 This emotional burden might be linked to past professional or personal experiences and reflect internal conflicts or perceptions directly related to the way patients experience coercion, often marked by feelings of humiliation, shame and dehumanisation.
The integration of patients’ perspectives into staff training regarding the management of violence and the use of coercion could be, in this context, a possible way to influence staff's views about coercive measures. The post-coercion review could prove to be an essential instrument to yield this perspective.Reference Wullschleger, Vandamme, Mielau, Stoll, Heinz and Bermpohl41 The systematic use of advance statements could also be an important way of carrying the experiences of patients, increasing staff members’ awareness of the consequences of coercive measures and identifying possible alternatives. Furthermore, the involvement of peer workers, whose key role in the facilitation of advanced directives has recently been shown, should be reinforced.Reference Tinland, Loubière, Mougeot, Jouet, Pontier and Baumstarck42
With respect to other influencing factors, our results indicate that gender and age are significantly associated with critical attitudes towards coercion. Past research has yielded mixed and partly contradictory results regarding the role of gender.Reference Husum, Bjørngaard, Finset and Ruud43,Reference Wynn44 In our sample, women tended to show slightly less critical attitudes towards the use of coercion. A possible explanation could be that women might perceive insecurity and the risk of violence differently from men and thus be more likely to validate the use of coercion as a means of protection. Qualitative analyses would be very helpful to understand better this association in our context. Similarly, the role of age could not clearly be identified in the literature. Older participants in our sample tended to have less critical attitudes towards coercion. The evolution of psychiatric practices, as well as nursing and medical education, with a stronger focus on issues related to coercion and patients’ rights could explain the tendency of younger, newly trained staff members to be more critical towards coercive practices that might have been more accepted in the past. Younger staff members might thus be more inclined to question coercive practices that do not match their personal ideal representation of their work and to perceive their negative consequences in a more acute way.
Regarding limitations, it must be considered that attitudes towards coercion represent a complex phenomenon linked not only to staff-related variables but also to institutional and organisational factors that were not investigated in the present survey. Existing policies, institutional culture, and architectural and environmental factors all influence attitudes towards coercion.Reference Doedens, Vermeulen, Boyette, Latour and de Haan14 This wide range of potential influencing factors probably explains the somehow low R-squared values of the regressions. The SACS surely also only captures some aspects of attitudes towards coercion, as acknowledged by the authors of the scale.Reference Husum, Bjørngaard, Finset and Ruud3 To the best of our knowledge, the SACS is the only evaluated instrument for assessment of staff attitudes towards coercion. Newer instruments capturing a broader spectrum of dimensions related to attitudes towards coercion are needed to investigate further this outcome. Social desirability might also have influenced the results, considering the efforts made over the past years to address the issue of coercion in the Department. Last, the relationship between attitude towards coercion and the use of coercive measures remains an unresolved question that could not be addressed in the present study.
However, the fact that the regression models included staff members not involved in decisions relating to coercive measures or in the application of such measures may have biased the results. We chose to include staff members not directly involved in decision-making processes surrounding coercion, as their views might reflect a general institutional perception of coercion. As these professionals are also exposed to violence, it seemed important to include their perceptions in the analysis. Furthermore, most studies investigating attitudes towards coercion also included all professional categories in contact with patients.Reference Krieger, Moritz, Lincoln, Fischer and Nagel12,Reference Husum, Finset and Ruud22,Reference Molewijk, Kok, Husum, Pedersen and Aasland39 The results of the sensitivity analysis we performed did not differ greatly from those of the main analysis, showing that the inclusion of these groups of professionals did not influence the core results.
Another strength of this work is the large, representative sample of staff members working at our Department, spanning across all professional categories. This large sample, as well as the wide range of investigated variables allowed us to produce important results shedding new light on the issue of the attitude towards coercion.
In conclusion, our results indicate that experience of violent events at the workplace does not influence staff members’ attitudes towards coercion. However, feeling of insecurity and the burden of coercive measures both, although in opposite directions, influence the way staff members perceive coercive measures. Even if the link between attitude and use of coercion remains unclear, institutional coercion reduction policies should focus on changing the perception of coercion by staff members, as their perspectives probably have an impact on the way coercion is applied in psychiatric services. Such coercion reduction programmes should include thorough and regular staff training, including post-coercion review techniques. These training programmes should also have a strong focus on the lived experience of patients who have faced coercive measures.
Data availability
The data that support the findings of this study are available from the corresponding author, A.W., upon reasonable request.
Author contributions
A.W. actively took part in study design, data collection and analysis, as well as drafting and revision of the manuscript. A.C. was involved in data analysis, manuscript drafting and revision. S.K. was involved in study design and manuscript revision. R.B., N.K. and J.B. were all involved in study design, data collection and manuscript revision.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.




 Open access
Open access
eLetters
No eLetters have been published for this article.