



Dementia and minor cognitive impairment prevalence
Globally, 46.8 million people live with dementia, and this is expected to increase to 115.4 million by 2050.Reference Prince, Wimo, Guerchet, Ali, Wu and Prina1,2 Minor cognitive impairment (MCI), which may later develop into dementia, is also prevalent in up to 42% of the global population over 60 years of age.Reference Hu, Yu, Sun, Zhang, Wang and Qin3
Within the UK alone, there are over 850 000 people with dementia and it has become the leading cause of death.Reference Prince, Knapp, Guerchet, McCrone, Prina and Comas-Herrera4,5 By 2025, this number is expected to rise to 1 million.Reference Prince, Wimo, Guerchet, Ali, Wu and Prina1 MCI is also estimated in between 5 and 20% of people over 65 years of age in the UK,6 with one in ten having a chance of developing further dementia.7
Dementia and MCI in minority populations
Because of the impact of globalisation, many Western countries, including the UK, have formed significant ethnic minority populations; currently 14% of the UK population identify as an ethnic minority,8 and this is estimated to increase to 20% by 2051.Reference Lievesley9 This includes non-English speakers. Currently, there are an estimated 88 languages other than English spoken in the UK, with over 8% of the population not having English as a first language, and over 864 000 people struggling or unable to speak it.8
In countries such as the UK, there is also a growing ageing ethnic minority population.Reference Richards, Brayne, Dening, Abas, Carter and Price10 Whereas previously many ethnic minorities would return to their home country as they grew older, many people from minority backgrounds who migrated in between the 1950s and 1970s as young adults are now choosing to permanently reside in the UK in their old age.Reference Mukadam, Cooper and Livingston11
These older ethnic minorities are at particularly high risk for receiving a diagnosis of dementia.Reference Richards, Brayne, Dening, Abas, Carter and Price10,Reference Chui and Gatz12 They are highly susceptible to risk factors known to increase the likelihood of dementia, showing higher prevalence for diseases and conditions such as diabetes, heart disease, hypertension and obesity.Reference Adelman, Blanchard, Rait, Leavey and Livingston13–Reference Seabrooke and Milne15 Furthermore, ethnic minorities are more likely to come from low socioeconomic backgrounds, which is associated with their likelihood of developing dementia.Reference Yaffe, Falvey, Harris, Newman, Satterfield and Koster16,Reference Fischer, Yeung, Hansen, Gibbons, Fornazzari and Ringer17
Cognitive testing in ethnic minorities
For an early and accurate diagnosis of dementia, the use of cognitive tests in the diagnostic process is vital.Reference Panegyres, Berry and Burchell18 However, a key limitation of cognitive tests available to us is that they are designed for people from European cultures, fluent in the English language.Reference Tuerk and Sauer19,Reference Fillenbaum, Heyman, Williams, Prosnitz and Burchett20
Therefore, when administering cognitive tests to ethnic minorities, there is reduced sensitivity and specificity; we see higher instances of false positive scores (where dementia or MCI is incorrectly detected by the test in a cognitively healthy person) and false negative scores (where a person's dementia or MCI is not detected by the test) within ethnic minorities compared with their English-speaking European counterparts.Reference Regan21–Reference Khan and Tadros24
To overcome this issues, cognitive tests are often translated into target languages. However, translation alone does not address these increased rates of false positive and false negative scores that may also arise from cultural differences. Ethnic minorities may not be familiar with Western concepts such as questions about the Western calendar, Western names or Western historical and general knowledge, which are used for assessing cognitive domains such as orientation, language and memory tasks.Reference Parker and Philp23 Therefore, when assessing for dementia, cultural bias can significantly affect the validity of these cognitive tests.Reference van de Vijver and Tanzer25,Reference Van De Vijver26
Flaherty et alReference Flaherty, Moises Gaviria, Pathak, Mitchell, Wintrob and Richman27 explored this in their research on the five dimensions of cross-cultural equivalence that can be used to minimise cultural bias and measurement errors in cross-cultural testing.Reference Flaherty, Moises Gaviria, Pathak, Mitchell, Wintrob and Richman27 These dimensions are content, conceptual, criterion, semantic and technical equivalence, and should be maintained by tests when they are adapted for different language and culture backgrounds.Reference Flaherty, Moises Gaviria, Pathak, Mitchell, Wintrob and Richman27
In the context of cognitive tests for dementia and MCI technical equivalence (how the test is administered is culturally appropriate for the person being assessed, e.g. language the test is administered in) and semantic equivalence (once translated, the meanings of the test questions are the same as the original test questions, e.g. accurate translation of questions) are retained through simply translating the cognitive test into a target language.Reference Flaherty, Moises Gaviria, Pathak, Mitchell, Wintrob and Richman27
However, without accounting for cultural differences as well, there is still a loss of three of the five dimensions. These are content equivalence (the questions of the test are culturally relevant to the cultural context of the person being assessed), criterion equivalence (after accounting for culture, the test as a whole still assesses for dementia and MCI) and conceptual equivalence (after accounting for culture, the individual test questions still accurately assess the cognitive domains they were meant to at the original level of difficulty).Reference Flaherty, Moises Gaviria, Pathak, Mitchell, Wintrob and Richman27
To ensure that all five dimensions of cross-cultural equivalence are maintained, solutions such as altering cut-off scores of cognitive tests for different ethnic minorities and non-English-speaking groups has been suggested.Reference Bohnstedt, Fox and Kohatsu28,Reference Milani, Marsiske, Cottler, Chen and Striley29 However, this has still been shown to reduce the sensitivity and specificity.Reference Bohnstedt, Fox and Kohatsu28,Reference Milani, Marsiske, Cottler, Chen and Striley29 With developing and piloting new cognitive tests not being the most feasible solution, adapting existing cognitive tests for different languages and cultures has been proposed.Reference van de Vijver and Tanzer25,Reference Van De Vijver26,Reference Guillemin, Bombardier and Beaton30
The Montreal Cognitive Assessment
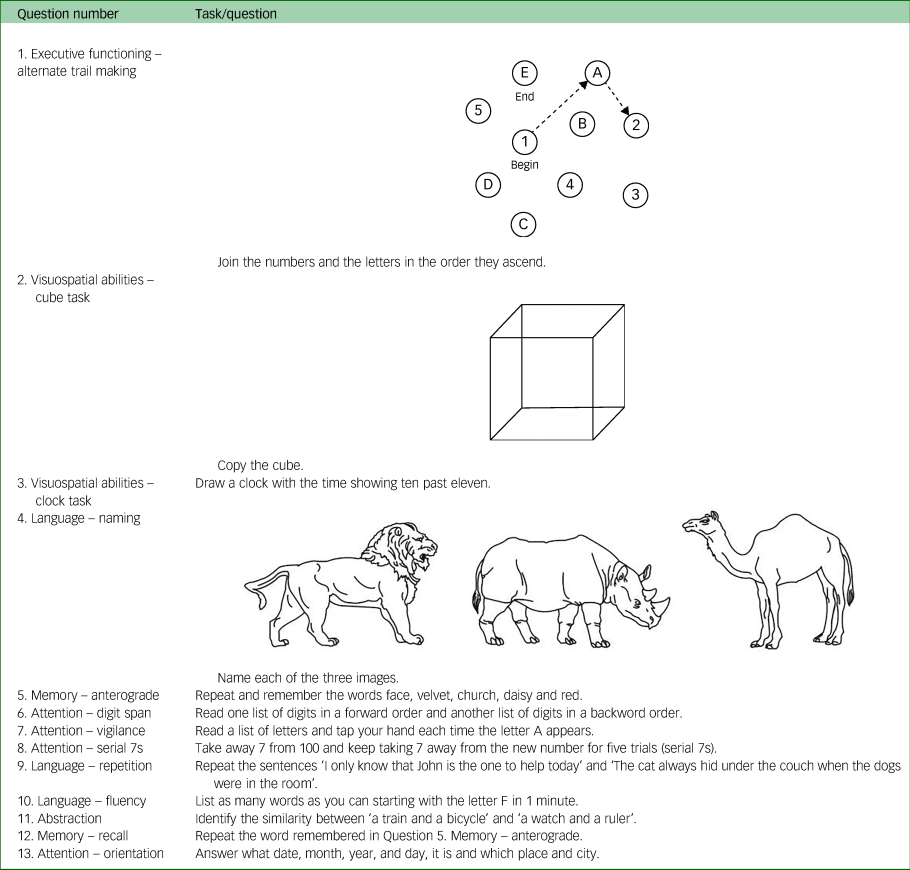
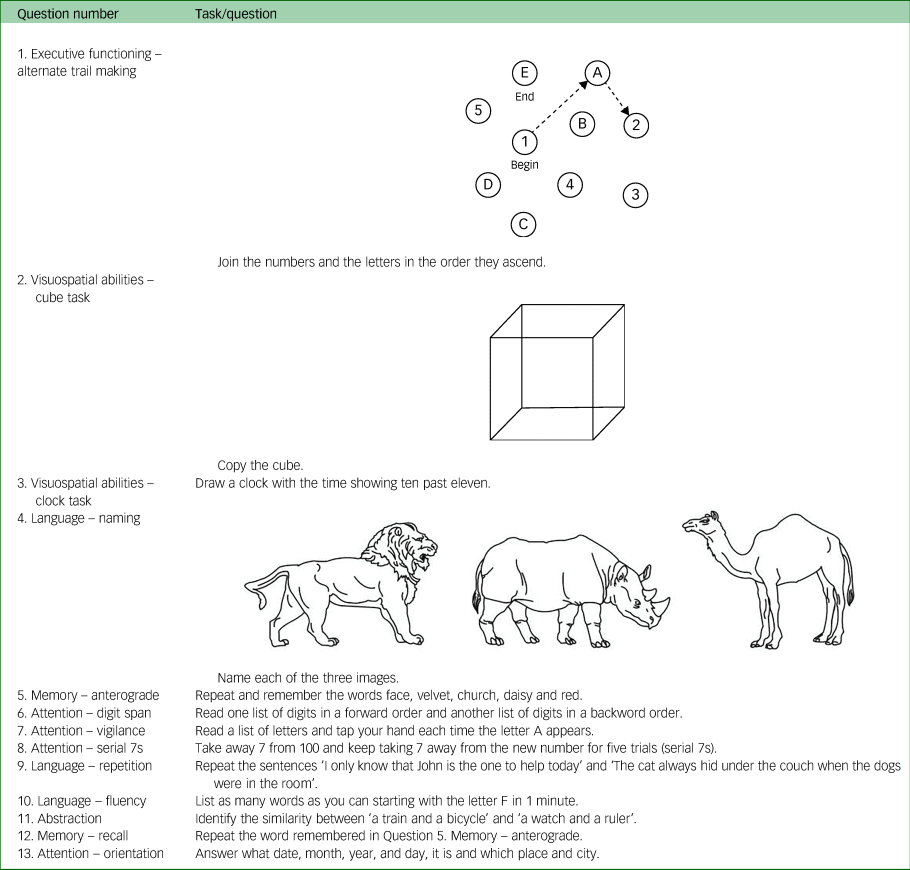
The Montreal Cognitive Assessment (MoCA) is a cognitive test, developed to screen and assess for dementia and MCI.Reference Nasreddine, Phillips, Bédirian, Charbonneau, Whitehead and Collin31 This tool was developed by Nasreddine et al,Reference Nasreddine, Phillips, Bédirian, Charbonneau, Whitehead and Collin31 and is currently used to aid physicians primarily in detecting MCI, a state that can progress to dementia. The test lasts 10 minutes and is given a score out of 30. There are 13 questions that assess the cognitive domains attention, fluency, memory, language, orientation, visuospatial abilities and executive functioning (see Table 1).
Table 1 Questions of the Montreal Cognitive Assessment
A validation study conducted in 2005 found that the MoCA is a better substitute for the assessment of MCI and dementia than the Mini-Mental State Examination (MMSE).Reference Nasreddine, Phillips, Bédirian, Charbonneau, Whitehead and Collin31 Since its inception, the MoCA has been used to assess for several variations of dementia and associated diseases such as Parkinson's disease, vascular dementia and Huntington's disease.Reference Dalrymple-Alford, MacAskill, Nakas, Livingston, Graham and Crucian32–Reference Videnovic, Bernard, Jaglin, Shannon, Fan and Jaglin34
A recent systematic review of cross-cultural applicability of the MoCA investigated the effect language and cultural diversity have on assessing for MCI, using this cognitive screening tool.Reference O'Driscoll and Shaikh35 The review reported a wide range of cut-off scores cross-culturally (both across countries and within regions), making it difficult to identify cut-off scores to differentiate between cognitively healthy individuals and those with MCI, as scores could be considered either cognitively healthy or indicative of MCI depending on which cut-offs are used. Furthermore, the review indicates very few studies having conducted validation studies on their adapted measures, meaning sensitivity and high false positive rates. Thus, the review highlights how it can be difficult to identify recommended adjusted cut-offs according to culture, age and education level.Reference O'Driscoll and Shaikh35
Therefore, as suggested, culturally adapting the existing MoCA would be the best approach to make it suitable for different languages and cultural contexts. In fact, the MoCA is currently widespread in use across over 50 different language and cultural versions.Reference O'Driscoll and Shaikh35 Yet, despite there being literature present that highlights the various adaptations of the MoCA and their development, using methods such as the use of global guidelines or the involvement of experts, there is no consensus on which questions must be culturally adapted and why.Reference Mirza, Panagioti, Waheed and Waheed36,Reference Maneesriwongul and Dixon37 There is also a lack of standard steps and procedures that can be undertaken to translate and culturally adapt the MoCA.
Culturally adapting cognitive tests
Waheed et alReference Waheed, Mirza, Waheed, Malik and Panagioti38 proposed that every cognitive test should have its own set of specific guidelines on culturally adapting each of its questions. These would be developed through an incorporation of previous literature and feedback from those who have previously adapted it.Reference Waheed, Mirza, Waheed, Malik and Panagioti38
At present, there are only one set of guidelines that have been developed for the cultural adaptation of a specific cognitive test.Reference Waheed, Mirza, Waheed, Malik and Panagioti38 These are for the Addenbrooke's Cognitive Examination Version III (ACE-III), a gold standard for the diagnostic accuracy of cognitive impairment and dementia.Reference Hsieh, Schubert, Hoon, Mioshi and Hodges39,Reference Cheung, Clugston, Croucher, Malone, Mau and Sims40 These guidelines were developed through a multi-stage qualitative study combining findings from a systematic review on the translation and cultural adaptations of the ACE-III with feedback received via questionnaires from previous adaptors of the ACE-III.Reference Mirza, Panagioti, Waheed and Waheed36,Reference Waheed, Mirza, Waheed, Malik and Panagioti38,Reference Mirza, Panagioti and Waheed41
The findings identified how adaptors of the ACE-III had adapted each test question for their culture, and their rationale for how they applied changes to test questions based on cultural differences. Through these findings, steps were identified for the cultural adaptation of each ACE-III test question, and these were formatted into a set of guidelines that stated which questions of the ACE-III required cultural adaptation and how they had been adapted, with justification for the adaptation process.Reference Waheed, Mirza, Waheed, Malik and Panagioti38 As a demonstration of their applicability, these guidelines were then implemented, with input from focus groups, to develop an Urdu version of the ACE-III.Reference Waheed, Mirza, Waheed, Malik and Panagioti38
This Urdu version of the ACE-III was then culturally validated by administering it to 25 cognitively health Urdu speakers, who were then interviewed to determine if the test questions matched their language and cultural context.Reference Mirza, Panagioti and Waheed41 Waheed et alReference Waheed, Mirza, Waheed, Malik and Panagioti38 determined that when translating and culturally adapting a test, particularly cognitive tests that are heavily reliant on language and culture, developing cultural adaptation guidelines for the test, implementing them to create a culturally appropriate version of the test and culturally validating the test are all steps that should precede a psychometric validation of the new version of the test.Reference Waheed, Mirza, Waheed, Malik and Panagioti38
Aims
In this paper, we will describe undertaking the initial portion of this methodology to develop guidelines, this time specifically for translating and culturally adapting the MoCA. Because of the widespread availability of its existing adapted versions, it was a suitable cognitive test to develop guidelines for. The research team also consisted of two of the original developers of the ACE-III guidelines (N.M. and W.W.).
We developed the guidelines for culturally adapting the MoCA through a scoping review of the literature, using a systematic search strategy and utilising feedback from those who had adapted the MoCA for their respective cultures and languages. By developing these guidelines, we endeavoured to provide a series of evidence-based instructions that future adaptors of the MoCA can incorporate into their culturally adapted protocols, with evidence to allow for the maintaining of content, criterion and conceptual equivalence.Reference Flaherty, Moises Gaviria, Pathak, Mitchell, Wintrob and Richman27
Method
A multi-stage qualitative approach was undertaken to develop guidelines for translating and culturally adapting the MoCA. Step 1 was a scoping review of publications on translated and culturally adapted versions of the MoCA. Step 2 involved collecting feedback from previous MoCA adaptors. Finally, in step 3, data was collated from steps 1 and 2 to form the guidelines.
It is important to note that steps 1 and 2 are mutually exclusive, and can be conducted independently. However, both steps must be complete to allow for step 3, the collation of their findings. This research took place at the Centre for Primary Care and Health Services Research, The University of Manchester.
Step 1: scoping review
We conducted a scoping review with a systematic search of all primary publications of translations and cultural adaptations of the MoCA. The methods of this review followed a similar systematic review of the ACE-III conducted by Mirza et al.Reference Mirza, Panagioti, Waheed and Waheed36
Search strategy
Because of the nature of the review, the search was conducted with healthcare-based electronic databases EMBASE, Medline and PsycINFO. The search terms were ‘Montreal cognitive assessment OR MoCA’ AND ‘dementia’ OR ‘Alzheimer*’ OR ‘cognitive’. A broad search was conducted to yield the maximum number of papers. Furthermore, a filter was applied to restrict the search period from April 2005 (as that was when the first paper on the MoCA was published) to July 2020.Reference Nasreddine, Phillips, Bédirian, Charbonneau, Whitehead and Collin31 In addition, we utilised Web of Science and Scopus to see if there were any publications that cited the original paper by Nasreddine et al.Reference Nasreddine, Phillips, Bédirian, Charbonneau, Whitehead and Collin31
Inclusion and exclusion criteria
Papers that mentioned a translated and/or culturally adapted version of the MoCA and were the original paper to have reported that adaptation were included. This included but were not limited to validation studies.
Papers that did not mention a translated or culturally adapted version of the MoCA were excluded.
Study selection
The results of the searches in each database were exported to Endnote (Endnote Basic for Clarivate, The Endnote Team, Philadelphia, USA; see https://endnote.com/downloads) and duplicates were removed. The selection of studies was conducted in two steps. First, the titles and abstracts were screened, and following this, the full texts of selected papers were accessed and compared against the eligibility criteria.
When the full texts were unavailable, the authors of the publications were contacted to provide additional information. A final attempt to obtain the publications was made by contacting the respective journals and putting in a request.
In addition, when requesting data from adaptors of the MoCA in step 2, we enquired whether their adapted MoCAs were mentioned in any earlier publications, and as a result, we were able to attain further sources.
Data extraction
The following data was extracted from the full text versions of the selected papers: authors, year of publication, country and language the MoCA was adapted for, and any text that described how they translated and adapted test questions for cultural differences (translation and cultural adaptation procedures).
The reported translation procedures of each paper were broken down into mutually exclusive steps. The translation steps of all papers were then merged, and duplicates were removed, to create a list of all potential steps on translating the MoCA.
The reported cultural adaptation procedures of each paper were reviewed to identify which questions of the MoCA had been culturally adapted and how. The cultural adaptation procedures for each question across papers were merged and duplicates were removed. This created a list of mutually exclusive steps for each question of the MoCA on how to culturally adapt it, along with the accompanying rationale.
Reporting of the cultural adaptation and translation procedures, and quality assessment
Two authors (G.K. and N.M.) assessed the quality of the reported translation and cultural adaptation procedures of the papers by using the Manchester Translation Reporting Questionnaire (MTRQ) and the Manchester Cultural Adaptation Reporting Questionnaire (MCAR) (see Fig. 1). These scales were initially used to assess the reported adaptations procedures of publications on the ACE-III by Mirza et al.Reference Mirza, Panagioti, Waheed and Waheed36,Reference Waheed, Mirza, Waheed, Malik and Panagioti38 These scales help display which papers reported their translation and cultural adaptation procedures in sufficient detail to be replicated by future adaptors.
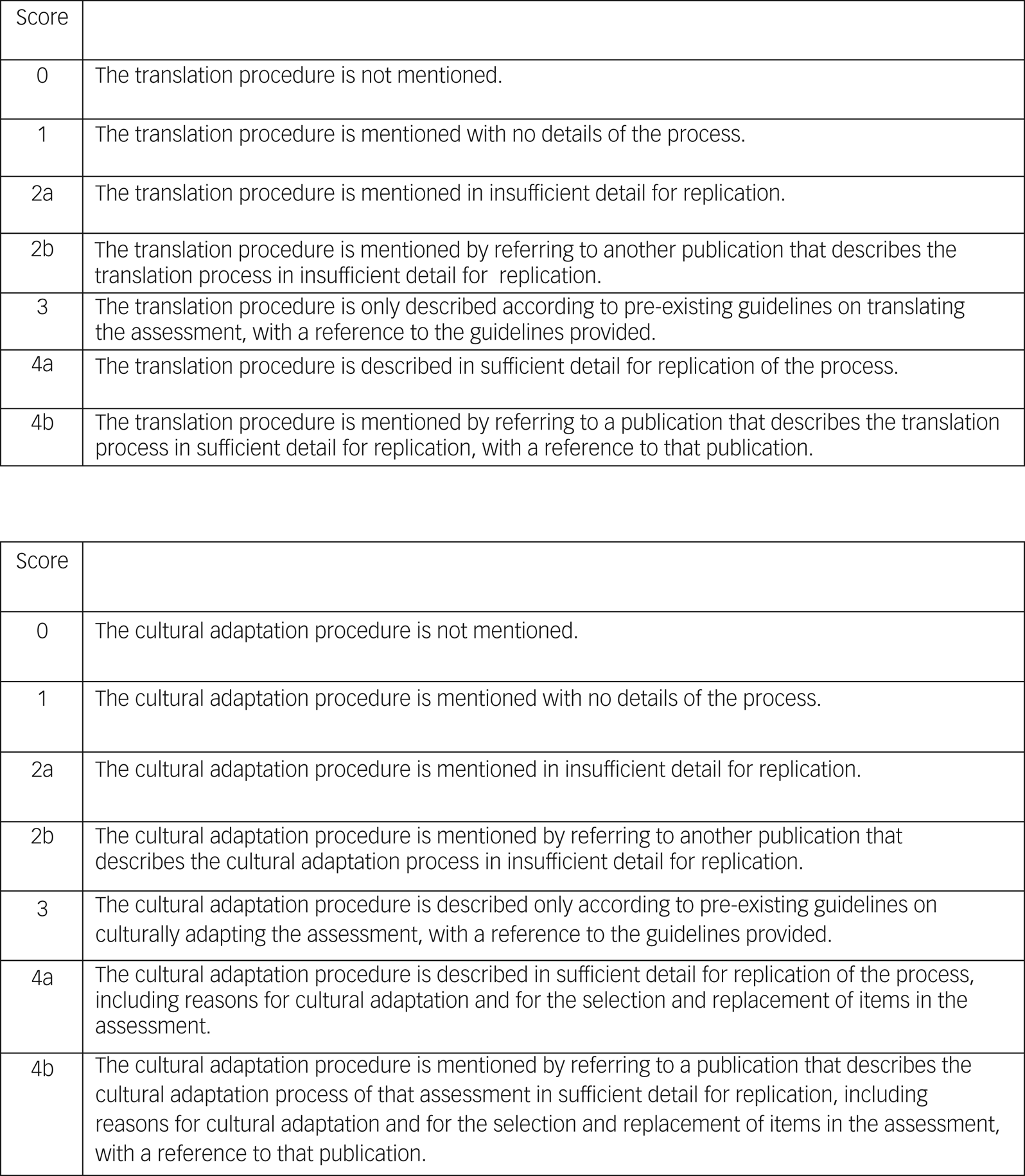
Fig. 1 The Manchester Translation Reporting Questionnaire and the Manchester Cultural Adaptation Reporting Questionnaire.
Each questionnaire is a seven-point rating scale that quantifies the quality of the reporting of the translation and cultural adaptation of a health measure, particularly cognitive tests. A score of 0 means that translation or cultural adaptation was not mentioned; 1 means that it was mentioned but with no details of the process; 2a or 2b means that a description of translation or cultural adaptation was mentioned either in the paper or referring to another paper, respectively, but the description was in insufficient detail for replication; 3 means that the translation or cultural adaptation described according to pre-existing guidelines, with a reference provided; and 4a or 4b means that a description of translation or cultural adaptation was mentioned either in the paper or referring to another paper, respectively, and the description was in sufficient detail for replication.
It is important to note that the MTRQ and MCAR do not assess the quality of the actual translation and cultural adaptation, as papers may not always report in detail what procedures they undertook. Instead, rating is based on the extent to which translation and cultural adaptation can be replicated from the information reported.
Step 2: feedback from previous MoCA adaptors
We aimed to gather a description of the cultural adaptation procedures and associated rationale from previous adaptors of the MoCA, who had translated and culturally adapted it for their respective language and culture.
Participants
Previous adaptors of the MoCA were identified as those who had made their version available on the MoCA website.Reference Nasreddine42
Materials
We downloaded all adaptations of the MoCA from the website, which currently hosts the MoCA and all its versions, currently providing 62 translations and cultural adaptations of the test, across 54 languages. This included one English version for Singapore and six Chinese versions, highlighting the impact of culture beyond language differences. Using the online translation application Google Translate (Google Translate for Google, Google, California, USA; see https://translate.google.co.uk/), we translated the MoCA versions to English.43 We checked which questions had been directly translated and which questions had been culturally adapted beyond a change in language.
We developed a uniform set of questionnaires for each version of the MoCA that had culturally adapted questions. These were based on the questionnaires used to develop guidelines for culturally adapting the ACE-III.Reference Waheed, Mirza, Waheed, Malik and Panagioti38
These questionnaires asked participants to first mention if their version of the MoCA was mentioned in any publications, and to list them. Following this, it presented them with the MoCA questions they had culturally adapted along with the question's original counterpart. For each of these questions, it enquired why cultural changes were needed, and the rationale behind how they changed it from the original to their version (see Supplementary Appendix 1 available at https://doi.org/10.1192/bjo.2021.1067 for a sample questionnaire).
Questionnaires for 45 of the 62 versions were developed (72.6%). For the remaining 17 versions, we could not make questionnaires as we were unable to create back translations of the test in English. This was because of a lack of resources in terms of electronic translation applications and translators available. These were the Bengali, Kannada, Lithuanian, Malayalam, Marathi, Myanmar, Persian, Russian, Sinhalese, Slovak, Slovenian, Swahili, Tamil, Telugu, Thai, Ukrainian and Vietnamese versions. Therefore, they have been excluded from the analysis (27.4%).
Procedure
Contact information for the adaptors of the MoCA was tracked down by first checking the MoCA version, followed by contacting the MoCA website. If a name was identified, we searched PubMed, ResearchGate and LinkedIn for an active email address. We also searched respective publications on those versions of the MoCA to see if one of the authors was also the initial adaptor and could be contacted through the journal or via the corresponding author.
These questionnaires were then sent out to the adaptors via email, along with a request to check our English translation of their version. If the adaptors responded and agreed to complete the questionnaire, we sent a reminder email after 2 weeks. If the adaptors did not respond after another 2 weeks, the email request was re-sent. If no further reply was received after this, no further contact was made.
Overall, the contact information for six adaptors could not be identified (13% of questionnaires developed and 9.7% of all adaptations). Questionnaires for the remaining 39 versions were sent out. Of these, 17 were returned fully completed, including after follow-up emails (27.4% of all adaptations and 43.6% of questionnaires sent out).
Step 3: collate data from steps 1 and 2 to form the guidelines
To develop guidelines for translating and culturally adapting the MoCA, we combined data on cultural adaptation and rationale behind the adaptation from our scoping review and questionnaire feedback from MoCA adaptors.
The questionnaires sent to adaptors were already organised by question and we were able to merge all adaptors’ feedback on the cultural adaptation procedures for each question. We again removed duplicating information so that each question of the MoCA had independent steps that could be undertaken to adapt it, along with the rationale.
For each question of the MoCA, its respective data on the cultural adaption steps and rationale behind cultural adaptation from the both the scoping review and questionnaire feedback were merged. Where we saw repetition (e.g. where the same concept or method for cultural adaption was being conveyed), the duplicate information was removed.
This resulted in a final list of mutually exclusive cultural adaptation steps for each question of the MoCA, along with rationale and guidance on how to conduct those steps. The respective papers and adapted versions of the MoCA were cited, resulting in a question-by-question set of guidelines.
Results
Step 1: scoping review
Our search identified 19 768 papers on the MoCA (see Fig. 2 for the flow diagram). We then proceeded to screen the titles of the papers and excluded 14 406 papers. Following this, abstracts were screened, and this narrowed our search to 296 papers. The other 1302 papers were excluded as they only focused on the original English versions of the MoCA.

Fig. 2 Flow diagram of the scoping review results.
Full texts of the remaining 296 publications were screened and this brought the number of papers to 58. The remaining 238 papers were excluded as they were not the primary papers for their non-English version of the MoCA. For six of the papers, full-text articles could not be located despite contacting authors and the respective journals; details of these papers are available in the Supplementary Material. Therefore, we had 52 papers that were deemed suitable for analysis.
Reporting of the translation procedures and quality assessment of that reporting
The scoping review identified and considered seven discrete steps that can be undertaken in any order when translating the MoCA:
(a) Translation: The original English version is converted into the target language without any cultural adaptation. A native/fluent speaker of the language can be of help. Alternatively, an official translator may be used, e.g. ‘A Japanese geriatrician and a psychologist translated the original English version of the MoCA into Japanese’.Reference Fujiwara, Suzuki, Yasunaga, Sugiyama, Ijuin and Sakuma43
(b) Back translation: An initial translation is converted back from the target language to English, e.g. ‘The revised Cantonese MoCA was then back-translated into English by another bilingual translator’.Reference Chu, Ng, Law, Lee and Kwan44
(c) Users in co-production: Individuals selected from the target population who may use the test give feedback or information that can influence the development of the test, e.g. ‘Twenty patients with confirmed stroke who were attending the outpatient physiotherapy clinic of the Universiti Kebangsaan Malaysia Medical Centre (UKMMC) participated. After completion of the BM [Bahasa Malaysia] MoCA, participants were asked to comment on whether any parts of the test were difficult to comprehend or complete.’Reference Sahathevan, Mohd Ali, Ellery, Mohamad, Hamdan and Mohd Ibrahim45
(d) Expert recommendations: Individuals with specialist knowledge on translation, target languages or subject matters related to the test, provide information or advice that may affect how the translated test is developed, e.g. ‘The resulting revision was reviewed and amended by a translation committee, which consisted of 3 Korean psychiatrists and 2 psychologists.’Reference Lee, Dong Woo, Cho, Na, Hong Jin and Kim46
(e) Revisions based on step-by-step feedback: Changes and adaptations are made to the translated test based on suggestions that have been proposed and approved, e.g. ‘Wording was adjusted where necessary, and the process was repeated until the final MoCA-ChLA [Chinese-Language Los Angeles] was considered by the two bilingual psychologists (ELT and PL) to be linguistically and semantically equivalent to the original MoCA, unambiguous, and easily comprehensible.’Reference Zheng, Teng, Varma, Mac, Mungas and Lu47
(f) Involvement of the original authors: Authors of the original test provide information or advice that may affect how the translated test is developed; in this instance, authors of the original paper by Nasreddine et al,Reference Nasreddine, Phillips, Bédirian, Charbonneau, Whitehead and Collin31 e.g. ‘The original author (ZSN) reviewed and approved the back-translated MoCA-B [MoCA-Basic] version.’Reference Chen, Xu, Chu, Ding, Liang and Nasreddine48
(g) Pilot study: A small scale preliminary study is implemented in which the translated version of the test is administered and evaluated to see whether it is viable and suitable for the proposed users, e.g. ‘A pilot study was conducted to establish whether the new BM [Bahasa Malaysia] version of the MoCA could be understood and completed by stroke patients in Malaysia.’Reference Sahathevan, Mohd Ali, Ellery, Mohamad, Hamdan and Mohd Ibrahim45
Across the 52 papers in our scoping review, a total of 30 different languages were used, with Chinese being the most widely reported; eight papers were included that looked into the translation and cultural adaptation of the MoCA into a Chinese version. This was followed by five papers for the Turkish version, four papers for the Czech version, four papers for the Cantonese version, three papers for the Arabic version, two papers for the Finnish version, two papers for the Indonesian version, two papers for the Malay version and two papers for the Polish version. There was one paper each for the following MoCA versions; Brazilian, Chinese (Changsha), Dutch, English, Filipino, French, Georgian, German, Greek, Hebrew, Hiligaynon, Hungarian, Italian, Japanese, Kazakh, Korean, Malayalam, Persian, Portuguese, Sinhala, Slovenian and Swahili.
Out of 52 papers, 16 mentioned a translation process taking place but did not provide enough detail with regards to specific steps. Consequently, a score of 1 was given to these papers on the MTRQ scale. Of these, four papers were for the Turkish version,Reference Aksoy, Timer, Mumcu, Akgun, Kivrak and Necioglu Orken49–Reference Yancar Demir and Özcan52 two were for the Chinese versionReference Chang, Chang, Lin, Huang, Chang and Lui53,Reference Hu, Zhou, Hu, Huang, Wei and Qi54 and two were for the Czech version;Reference Bezdicek, Balabanova, Havrankova, Stochl, Roth and Ruzicka55,Reference Reban56 there was one paper each for the Singaporean,Reference Dong, Sharma, Chan, Venketasubramanian, Teoh and Seet57 Slovenian,Reference Potocnik, Ovcar Stante and Rakusa58 Malay,Reference Razali, Jean-Li, Jaffar, Ahmad, Shah and Ibrahim59 Italian,Reference Pirrotta, Timpano, Bonanno, Nunnari, Marino and Bramanti60 Indonesian,Reference Panentu and Irfan61 Hungarian,Reference Volosin, Janacsek and Nemeth62 HebrewReference Lifshitz, Dwolatzky and Press63 and Greek versions.Reference Konstantopoulos, Vogazianos and Doskas64
Excluding the aforementioned papers, Table 2 shows the remaining 36 papers in which individual translation steps were reported. Of these, only four papers (Chu et al,Reference Chu, Ng, Law, Lee and Kwan44 Freitas et al,Reference Freitas, Simões, Martins, Vilar and Santana90 Husein et alReference Husein, Lumempouw, Ramli and Herqutanto84 and Sahathevan et alReference Sahathevan, Mohd Ali, Ellery, Mohamad, Hamdan and Mohd Ibrahim45) reported using all of the translation steps. The remaining 32 reported to have undertaken some translation steps, in various combinations.
Table 2 All papers included in our analysis, with the reported translation steps undertaken
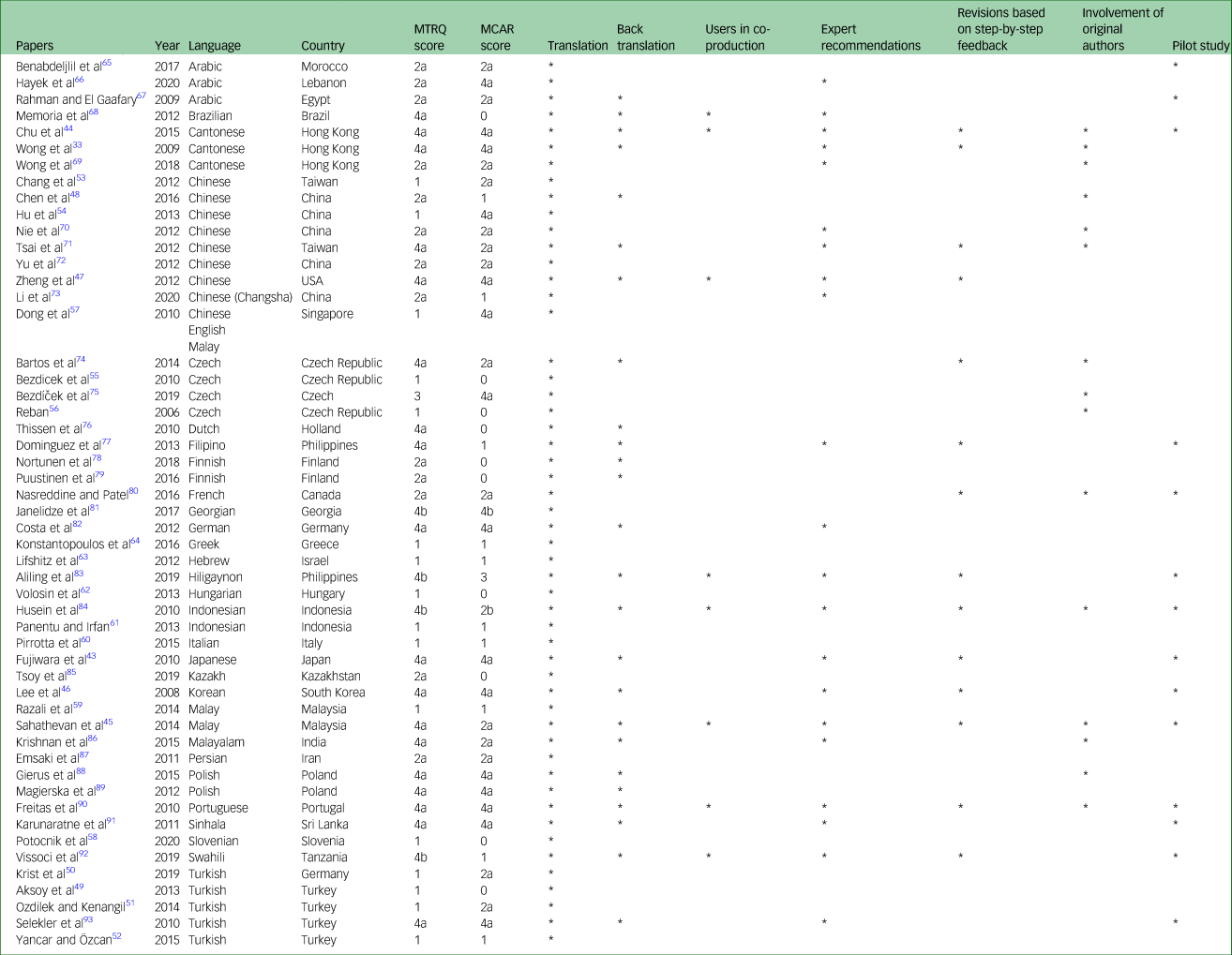
MTRQ, Manchester Translation Reporting Questionnaire; MCAR, Manchester Cultural Adaptation Reporting Questionnaire.
All of the papers reported simple translation, 25 papers undertook back translation, 21 involved the use of expert recommendations, 15 involved original authors, 14 made revisions based on step-by-step feedback, 14 directed pilot studies and eight reported users in co-production.
Reporting of the cultural adaptation procedures and quality assessment
Out of the 52 papers, ten (Aksoy et al,Reference Aksoy, Timer, Mumcu, Akgun, Kivrak and Necioglu Orken49 Bezdicek et al,Reference Bezdicek, Balabanova, Havrankova, Stochl, Roth and Ruzicka55 Memoria et al,Reference Memoria, Yassuda, Nakano and Forlenza68 Nortunen et al,Reference Nortunen, Puustinen, Luostarinen, Huhtala and Hänninen78 Potocnik et al,Reference Potocnik, Ovcar Stante and Rakusa58 Puustinen et al,Reference Puustinen, Luostarinen, Luostarinen, Pulliainen, Huhtala and Soini79 Reban,Reference Reban56 Thissen et al,Reference Thissen, Van Bergen, De Jonghe, Kessels and Dautzenberg76 Tsoy et alReference Tsoy, Turuspekova, Klipitskaya, Mereke and Cumming85 and Volosin et alReference Volosin, Janacsek and Nemeth62) did not mention any cultural adaptation that may have taken place, resulting in a score of 0 on the MCAR scale. Ten papers (Chen et al,Reference Chen, Xu, Chu, Ding, Liang and Nasreddine48 Dominguez et al,Reference Dominguez, Orquiza, Soriano, Magpantay, Esteban and Corrales77 Konstantopoulos et al,Reference Konstantopoulos, Vogazianos and Doskas64 Li et al,Reference Li, Wang, Wu, Xu, Wu and Zhou73 Lifshitz et al,Reference Lifshitz, Dwolatzky and Press63 Panentu et al,Reference Panentu and Irfan61 Pirrotta et al,Reference Pirrotta, Timpano, Bonanno, Nunnari, Marino and Bramanti60 Razali et al,Reference Razali, Jean-Li, Jaffar, Ahmad, Shah and Ibrahim59 Vissoci et alReference Vissoci, de Oliveira, Gafaar, Haglund, Mvungi and Mmbaga92 and Yancar and ÖzcanReference Yancar Demir and Özcan52) mentioned that a cultural adaptation process took place but did not describe it, scoring 1 on the MCAR.
For the remaining 32 papers, Table 3 highlights which questions were reportedly culturally adapted. Furthermore, this shows the regularity with which each question needed to be adapted across the papers. Question 10 for language was most frequently culturally adapted, in 20 out of 32 papers. This was closely followed by question 5 (in 19 out of 32 papers), and by extension, question 12. Question 9 for language was found to be culturally adapted in 15 papers.
Table 3 The frequency of cultural adaptation across questions of the Montreal Cognitive Assessment in papers

Question 1 for executive functioning was culturally adapted in 12 papers, question 7 for attention was adapted in ten papers, question 4 for language was adapted in six papers, question 13 for attention was adapted in five papers and question 11 for abstraction was adapted in three papers. Only two papers culturally adapted question 2 for visuospatial abilities, and only one paper each culturally adapted question 3 for visuospatial abilities, question 6 for attention and question 8 for attention.
This highlights which cognitive domains, and their respective questions, are dependent on cultural knowledge, and which rely on a simple translation.
Individuals involved in translation and cultural adaptation
Of the 52 papers that mentioned translation and cultural adaptation processes in some level of detail, 21 publications elaborated further the individuals involved in the translation and cultural adaptation process (see Table 4).
Table 4 Reported individuals involved in translation and cultural adaptation
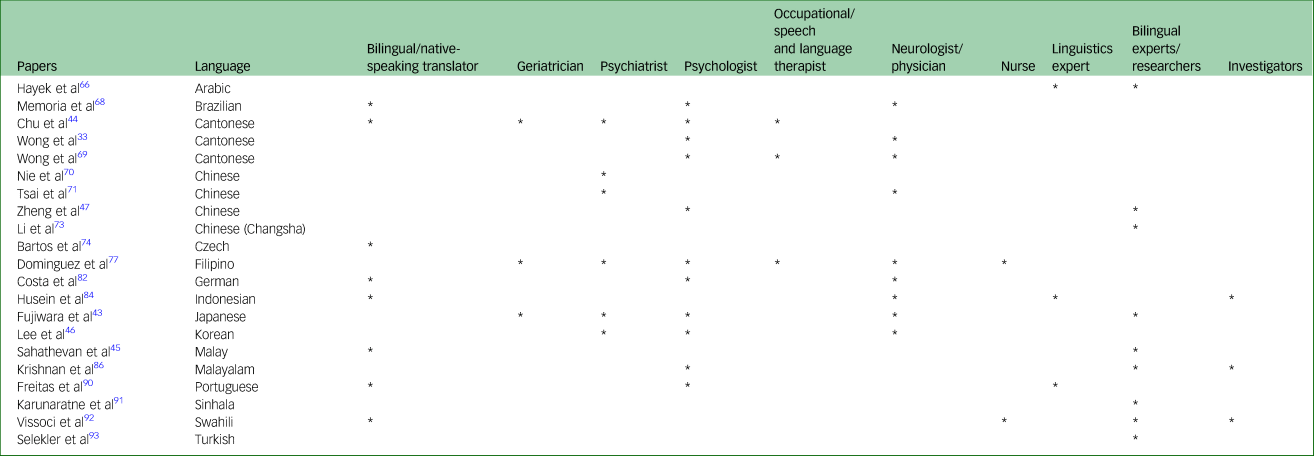
Of these, 11 mentioned psychologists, nine mentioned neurologists/physicians, eight mentioned bilingual experts/researchers, eight referred to bilingual/native-speaking translators and six referred to psychiatrists. Three papers mentioned geriatricians, three mentioned occupational/speech and language therapists, three referred to a linguistics expert and three mentioned the use of an investigator. Only two papers mentioned nurses.
Step 2: feedback from previous MoCA adaptors
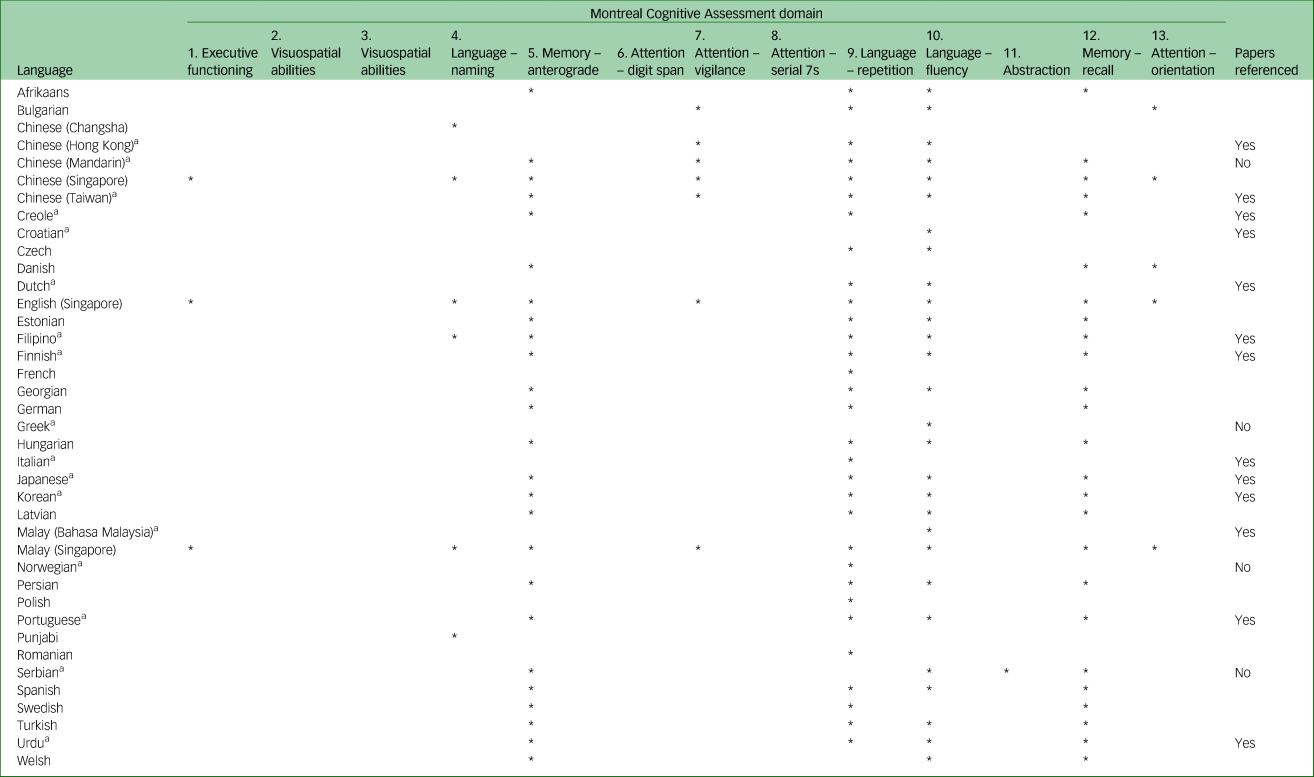
Table 5 summarises which questions of the MoCA were culturally adapted by adaptors, thus showing the frequency of cultural adaptation undertaken for each question. The table also highlights which adaptors returned feedback that provided rationale for their cultural adaptation.
Table 5 Questionnaires distributed to adaptors of the Montreal Cognitive Assessment
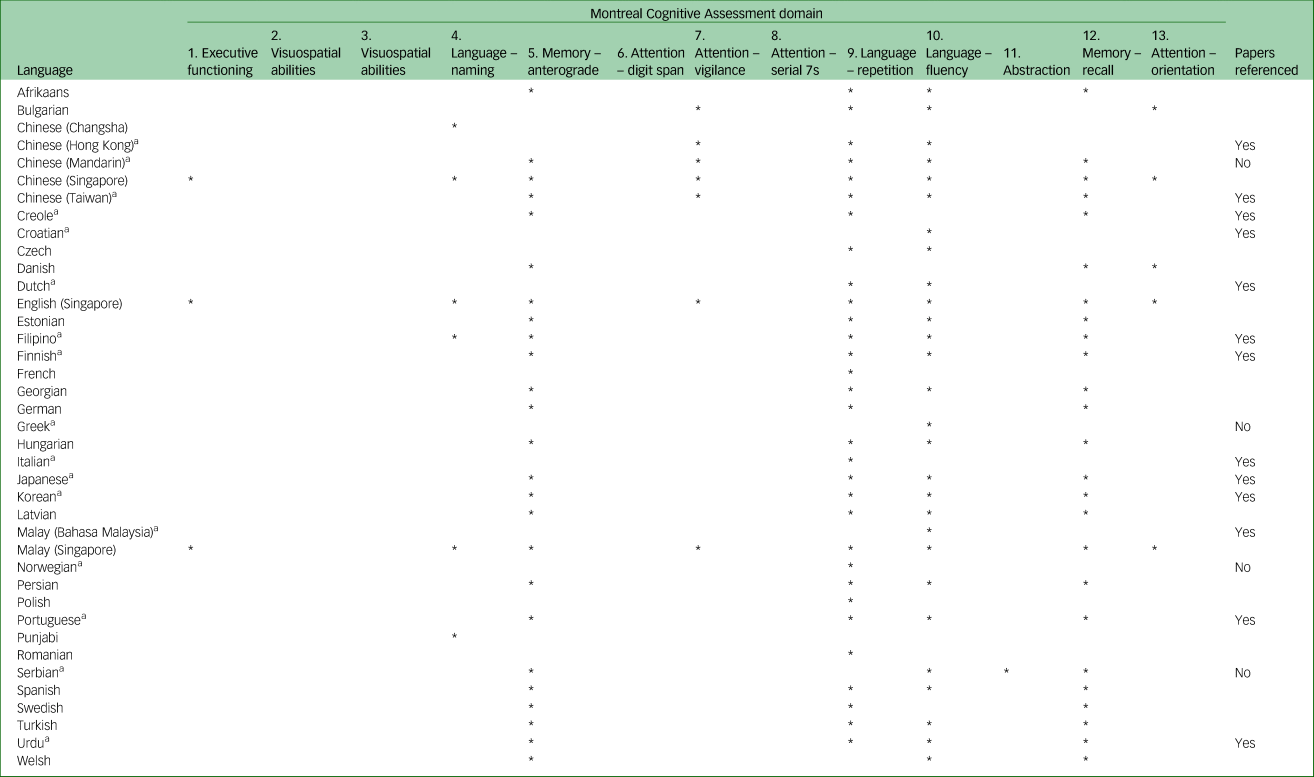
* Question was culturally adapted.
a. Questionnaire was returned.
We can see that the majority of adaptors culturally adapted question 5, and by extension question 12, for memory, and questions 9 and 10 for language. We can also see that some adaptors culturally adapted question 4 for language, question 7 for attention and question 13 for orientation. Only three adaptors culturally adapted question 1 for executive functioning, and only one adapted question 11 for abstraction.
In contrast, none of the adaptors had culturally adapted questions 2 and 3 for visuospatial abilities, and questions 6 and 8 for attention that pertains to numbers.
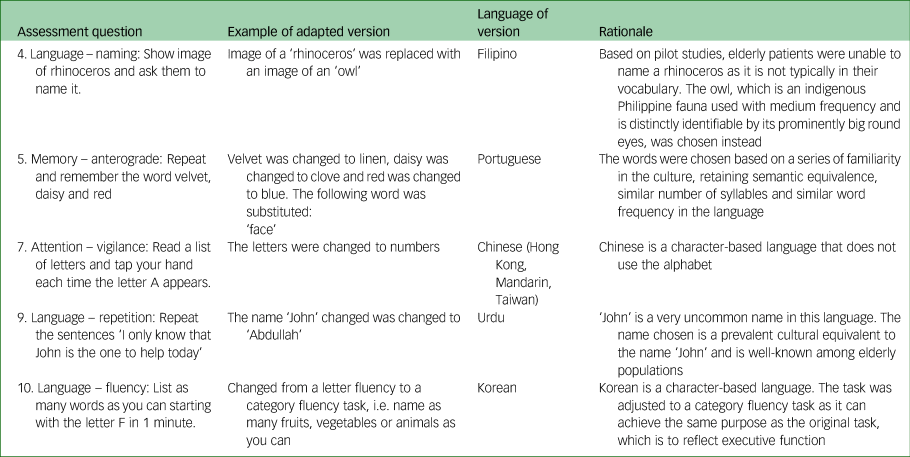
Table 6 provides examples of some of the modifications adaptors reported back in the questionnaires along with the rationale they provided for some of these questions.
Table 6 Cultural adaptation of Montreal Cognitive Assessment items from feedback provided through questionnaires
As with our scoping review, this has highlighted cognitive domains, and their respective questions, dependent on cultural knowledge.
We also found that of the 17 returned questionnaires, 13 of the adaptors mentioned their adapted MoCAs being mentioned in publication; these were screened and added to the scoping review retroactively.
Step 3: collate data from steps 1 and 2 to form the guidelines
For each question of the MoCA, the individual cultural adaptation steps identified from our scoping review and from adaptors’ feedback, along with the rationale for undertaking cultural adaptation, were tabulated to form the guidelines. Figure 3 summarises the steps and processes we undertook to synthesise the data into guidelines for the adaptation of the MoCA.
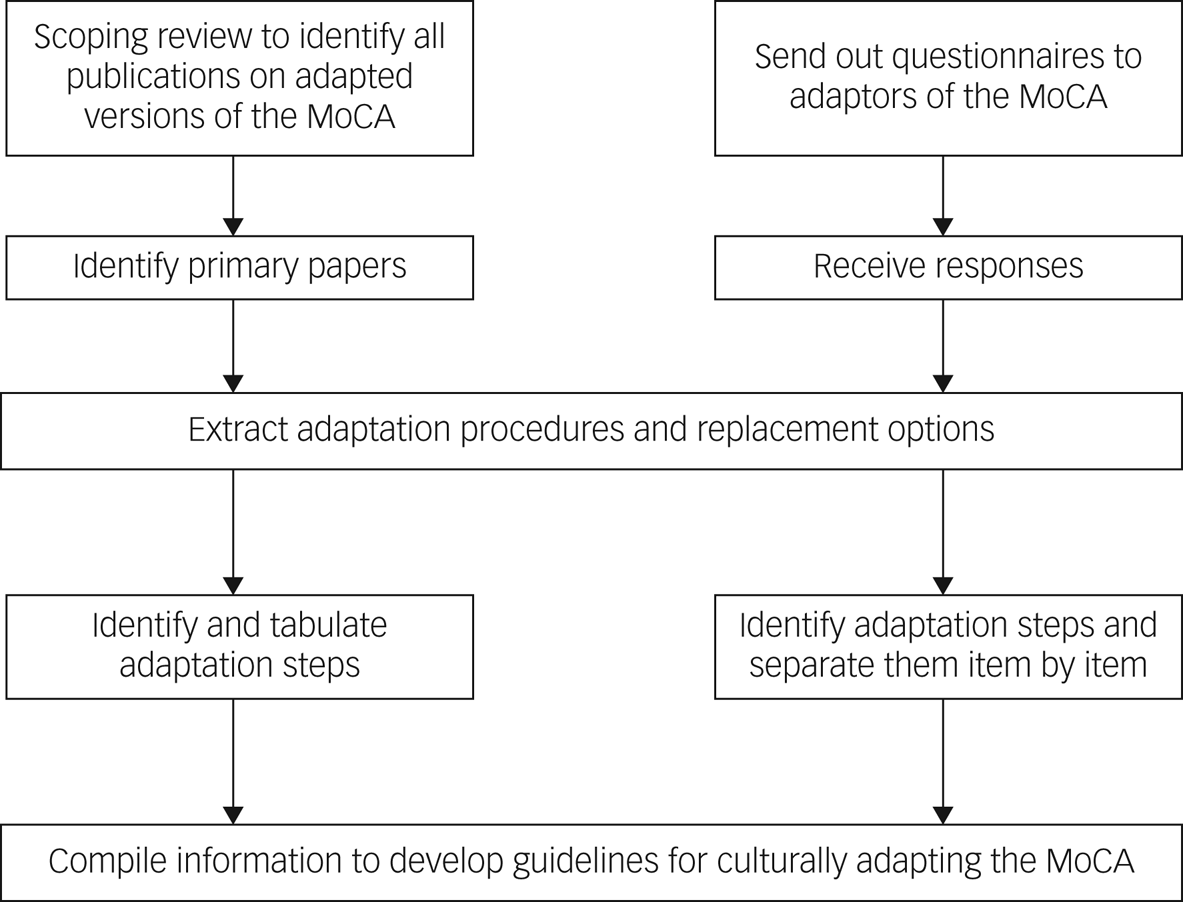
Fig. 3 Development process of the guidelines.
For each question, the following was presented:
(a) How the questions have been previously culturally adapted, with steps undertaken.
(b) Citing of the respective languages and adaptors that used these steps.
(c) The rationale behind adapting the question with these steps and the replacement chosen.
Figure 4 shows an excerpt from the guidelines, providing examples of these.

Fig. 4 Example from the guidelines.
The full guidelines are 29 pages providing data and guidance on the translation and cultural adaptation of the MoCA. These guidelines display information spanning 32 languages and 38 countries (see Supplementary Appendix 2 for a copy of the guidelines).
Discussion
The diagnosis of dementia and MCI within elderly ethnic minority populations is currently compromised because of the lack of cognitive tests that account for the language and culture of individuals from these populations.Reference Tuerk and Sauer19,Reference Fillenbaum, Heyman, Williams, Prosnitz and Burchett20 The current breadth of cognitive tests are susceptible to cultural bias and require an extensive cultural adaptation beyond a translation verbatim.Reference van de Vijver and Tanzer25,Reference Van De Vijver26,Reference Guillemin, Bombardier and Beaton30
One solution to this is to produce individual guidelines for the cultural adaptation of various cognitive tests, as has been previously done for the ACE-III.Reference Mirza, Panagioti, Waheed and Waheed36,Reference Waheed, Mirza, Waheed, Malik and Panagioti38 We aimed to replicate these methods for the MoCA, a popular cognitive test used to screen and diagnose for dementia and MCI. Through the combination of a scoping review and questionnaire feedback from adaptors of the MoCA, we were able to successfully develop guidelines on translating and culturally adapting the MoCA.
The scoping review was able to list all papers on existing translations and cultural adaptation of the MoCA and through the MTRQ and MCAR ratings, highlight which papers provide the most replicable data on translating and culturally adapting the MoCA for future adaptors to consider.
Through our review, a full list of independent translation steps that can be undertaken by future adaptors was identified along with the frequency of their occurrence. This allows future adaptors to make judgement calls regarding which steps they may endeavour to undertake, based on what previous adaptors followed. Naturally, some approaches such as simply having a native speaker back-translate a measure would be problematic from a clinical or psychometric standpoint.Reference Reynolds, Suzuki and IB94 A native speaker is not necessarily someone qualified or informed about the nuances of cognitive tests, thus an additional expert in this field of study would be desirable to help form a cultural adaptation or accurate translation.
We can see that direct translation was the most common step, undertaken by all of the publications, followed by back translation, expert recommendations, the involvement of original authors, revisions based on step-by-step feedback, pilot studies and finally, users in co-production. Across the same language versions, although there is some overlap of translation steps undertaken, there is no consistency. For example, in one Indonesian version all of the translation steps were undertaken,Reference Husein, Lumempouw, Ramli and Herqutanto84 whereas in the other only one step was.Reference Panentu and Irfan61 This would suggest that translation steps were undertaken on the basis of convenience and resources, as opposed to the best fit for different language and cultural groups.
We also identified which cognitive domains and their respective questions were considered to be dependent on culture and therefore most likely to be culturally adapted. Question 10 for language, which focused on verbal fluency, was culturally adapted the most, followed by further questions for language and memory. On the other hand, questions for attention based on numbers (i.e. serial 7s and digit span) and visuospatial abilities had not been reportedly culturally adapted as much in any of the papers.
Thus, we have identified which possible domains of the MoCA display significant cultural reliance. It is important to note that although cognitive domains such as attention and visuospatial abilities were not frequently adapted in our findings, this does not necessarily mean that they cannot be influenced by culture in other cases.
Through our questionnaires we were able to acquire additional and far richer data on the cultural adaptation of the MoCA, including rationale behind changes made. As with our scoping review, this feedback from adaptors showed which questions were most likely to require cultural adaptation, indicating their cultural dependence.
Findings from the questionnaires mirrored those from our review: question 10 for language was once again the most culturally adapted, followed by the same questions for language and memory. Similarly, questions for attention based on numbers, executive functioning and visuospatial abilities received little to no cultural adaptation by adaptors.
The previous systematic review of adaptations of the ACE-III reported similar findings across cognitive domains and their questions. Reasoning behind these findings in both our scoping review and across questionnaires is that executive functioning, visuospatial abilities and number-based tasks are not associated with culture. This indicates to future adaptors which questions should be prioritised for cultural adaptation.
Across the same language versions there was little overlap, suggesting that different cultures may have different needs with regards to cultural adaptation, even if they share a language. Interestingly, however, within the Cantonese and Chinese versions there was consistency across the versions in requiring cultural adaptation for question 1 for executive functioning and question 7 for attention – questions that typically do not require adaptation. This is because they rely specifically on the alphabet, in contrast to Cantonese and Chinese characters. In this instance, language and culture played a dual role and required the cultural adaptation of these questions for these specific language versions, irrespective of which country the version was for.
Our scoping review was restricted in several ways that prevented the incorporation of some language and cultures. First, it was restricted by what was reported in the papers. Further and additional adaptation procedures that may have been undertaken by adaptors but were not mentioned in their respective papers still resulted in scores of 1 and 0 on the MTRQ and MCAR. The scales also cannot guarantee the quality of those processes, and whether they resulted in robustly adapted versions of the MoCA.
Second, regarding our questionnaires sent to adaptors, we were limited by resources and translators available to us, and therefore unable to produce and distribute questionnaires for all 62 versions of the MoCA. The relatively poor return rate of 17 out of 62 questionnaires reduced the amount of additional information we could have included in the guidelines.
This highlights the significance of conducting the scoping review and questionnaires in tandem, and combining the findings to allow for the incorporation of as much information as possible. The guidelines are not restricted to information available in published literature, and incorporate primary experiences of cultural adaptation by existing adaptors of the MoCA, which accounted for adaptations that may not have had corresponding papers.
Additionally, the adaptations reported were culturally skewed favouring primarily MoCA versions from Asia (mainly China) and Europe. However, the guidelines are designed in such a way that they can be used to culturally adapt the MoCA in countries such as those from Africa or South America.
If a language in these countries is not letter-based but character-based, then it may be more appropriate to use a category fluency task rather than a letter fluency task, as it has been shown to be just as effective. Similarly, if the images of animals that have to be recognised are not animals familiar in certain countries, native animals knowledgeable to older groups should be selected. Words that have to be remembered should not just be directly translated into the corresponding language; a word that represents the same concept but also has the same fluency in the target language and, ideally, the same number of syllables should be used instead.
Examples and associated rationale like this within the guidelines can help support and guide adaptors who want to adapt the MoCA for their respective language and culture, regardless of where they are from.
Overall, we replicated a novel approach that has only previously been done once before. However, unlike the ACE-III guidelines, for the MoCA we were able to gain more data as the MoCA originated earlier, with far more translated and culturally adapted versions. Although the ACE-III guidelines compiled data from 22 languages and cultural contexts,Reference Waheed, Mirza, Waheed, Malik and Panagioti38 the guidelines for the MoCA compiled data for 32 languages across 38 countries. Additionally, the ACE-III review found 32 papers and only six completed questionnaires from adaptors of the ACE-III were received.Reference Mirza, Panagioti, Waheed and Waheed36 In comparison, the MoCA guidelines are composed of far richer and extensive data.
The implications of this methodology, and the findings regarding questions pertaining to specific cognitive domains, can be replicated further to develop guidelines in the same manner for other cognitive tests. Furthermore, these particular methods allow for familiarity with a chosen test.
However, although we have demonstrated that these set of guidelines can assist future adaptors in creating their own version of the MoCA, it does not obviate the need to conduct a formal cultural and psychometric validation within a target population. These are essential steps that should follow the development and utilisation of guidelines to produce a culturally adapted version of a test.
Naturally, other factors beyond culture, such as age and education level, can also influence sensitivity. Therefore, it may also be appropriate to use cut-offs and point adjustments for these factors once translation and cultural adaptation has occurred for a test, and future researchers should endeavour to establish what these might be during psychometric validation in large clinical populations.
Overall, these guidelines can act as a starting point for future adaptors of the MoCA, and have been designed so that necessary updates and further information on cultural adaptation can continue to be added to them. The next step would be to implement these guidelines to develop an adaptation of the MoCA for a particular language and cultural context, as was done for the ACE-III, to demonstrate usability and cultural validity.
Supplementary material
Supplementary material is available online at https://doi.org/10.1192/bjo.2021.1067
Data availability
The data that support the findings of this study are available from the corresponding author, N.M., upon reasonable request.
Acknowledgements
We thank Kathleen Gallant and Ziad Nasreddine from mocatest.org for providing access to the MoCA, rights to conduct research with the MoCA, and information and support for contacting adaptors of the MoCA. We also thank Adrian Wong, Christina Agogiatou, Magda Tsolaki, Alessandro Pirani, Elaine Chan, Farrukh Habib, Hiroyuki Suzuki, Momoko Kobayashi, Yoshinori Fujiwara, Irena Martinic Popovic, Jacqueline C. Dominguez, Jeannette Moreira, Luis Faisca, Jos F. M. de Jonghe, Jukka Puustinen, Jun-Young Lee, Marleen Regina van Walsem, Pengxu Wei, Ramesh Sahathevan, Sandra Freitas and Vanja Kljajevic, for completing and returning questionnaires.
Author contributions
The research question was formulated and the study was designed by W.W. and N.M. The study was carried out by N.M. and G.K., supervised by W.W. The qualitative data analysis was conducted by N.M. and G.K., supervised by W.W. N.M. and G.K. contributed to the writing of the article, and this was reviewed by W.W.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
None.











 Open access
Open access
eLetters
No eLetters have been published for this article.