



Introduction
Clark and Wells’ (Clark and Wells, Reference Clark, Wells, Heimberg, Liebowitz, Hope and Schneier1995) prominent cognitive model of social anxiety disorder (SAD) continues to be the basis for many therapies treating social anxiety disorder. This model assumes that social anxiety is maintained by self-focused attention (SFA) and a negative representation of the self. When socially anxious individuals enter a feared social situation, negative automatic thoughts lead to a shift in attention towards self-processing, and the individuals take an observer perspective. To create an image of themselves, how they appear to others, they use self-referred information (such as anxiety symptoms). In line with the model, socially anxious individuals report experiencing spontaneously occurring self-images during social situations (Hackmann et al., Reference Hackmann, Surawy and Clark1998). According to Hackmann et al. (Reference Hackmann, Clark and McManus2000), these self-images are mostly linked to specific memories about negative social situations that accumulated in time around the onset of the social anxiety disorder. Indeed, the literature suggests that negative self-image has a disadvantageous effect on anxiety, for both socially anxious and non-clinical participants (Ng et al., Reference Ng, Abbott and Hunt2014).
Studies that manipulated self-image (negative, positive, or relaxed) by instructing participants to keep the self-image in mind before (and during) a social task, conducted with high and low socially anxious participants, found an association between a negative self-image and heightened anxiety during a conversation with a stranger (Hirsch et al., Reference Hirsch, Meynen and Clark2004). Similar results were found also in patients with social anxiety disorder (Hirsch et al., Reference Hirsch, Clark, Mathews and Williams2003a) and in confident public speakers (Hirsch et al., Reference Hirsch, Mathews, Clark, Williams and Morrison2006). These results were consistent with performance during another social situation, namely making a speech in front of a camera (in high and low socially anxious participants; Vassilopoulos, Reference Vassilopoulos2005). In line with these findings on self-image, recent studies (Lee and Kwon, Reference Lee and Kwon2013; McEvoy and Saulsman, Reference McEvoy and Saulsman2014; Nilsson et al., Reference Nilsson, Lundh and Viborg2012; Wild et al., Reference Wild, Hackmann and Clark2007; Wild and Clark, Reference Wild and Clark2011) investigated modifying self-imagery in SAD by using an imagery rescripting technique, which aims to update the meaning of distressing memories and images in SAD. Wild et al. (Reference Wild, Hackmann and Clark2007, Reference Wild, Hackmann and Clark2008) found a significant decrease in negative beliefs, image distress, fear of negative evaluation, and anxiety in social situations within a single imagery rescripting session. Similar results were found in the study of Nilsson et al. (Reference Nilsson, Lundh and Viborg2012) after one session imagery rescripting, and in Lee and Kwon (Reference Lee and Kwon2013) at post-treatment and 3-month follow-up after three sessions. McManus et al. (Reference McManus, Clark, Grey, Wild, Hirsch, Fennell, Hackmann, Waddington, Liness and Manley2009) and Warnock-Parkes et al. (Reference Warnock-Parkes, Wild, Stott, Grey, Ehlers and Clark2017) used video feedback in the treatment of SAD to modify clients’ negative self-images by showing them how they actually appear on the video. The results showed that participants with SAD predicted an excessive negative impression of themselves about how they came across. Thus, the video feedback helped participants to gain a more realistic impression of themselves, which was associated with an improvement in their social anxiety. In sum, research indicates that self-image plays an important role in the maintenance, and consequently, in the treatment of SAD, highlighting that negative self-image may have input from autobiographic memory (Hackmann et al., Reference Hackmann, Clark and McManus2000).
The association between SFA and social anxiety has also been proven in many investigations showing that high socially anxious individuals or patients with SAD are more self-focused in social situations (for reviews, see: Bögels and Mansell, Reference Bögels and Mansell2004; Morrison and Heimberg, Reference Morrison and Heimberg2013). Although SFA is often defined as a state condition, the study of Vriends et al. (Reference Vriends, Meral, Bargas-Avila, Stadler and Bögels2017) showed that SFA varied significantly according to the tasks at hand: during a conversation (with a confederate) including different phases, they measured SFA continuously with an eye-tracker in high versus low socially anxious participants (experiment 1), and in clinical and control samples (experiment 2). SFA was defined as eye-tracked gaze duration at their own image relative to the confederates’ video image and other places on the computer screen. The results showed that, especially during the critical phase (when the confederate was critical of the participants), SFA increased in high socially anxious participants, both compared with the other phases, and compared with low socially anxious participants. While SFA varied according to the task at hand, the clinical sample showed heightened SFA throughout the conversation compared with the control sample (Vriends et al., Reference Vriends, Meral, Bargas-Avila, Stadler and Bögels2017).
In sum, studies have shown direct associations between a negative self-image and social anxiety, and between SFA and social anxiety. However, until now, the majority of studies did not assess this interactional association. A small number of studies investigated how SFA varies under different conditions of self-images during a social situation. Makkar and Grisham (Reference Makkar and Grisham2011) showed that high socially anxious participants holding a negative self-image in mind reported more SFA, felt more anxious, and evaluated their performance less well than those holding a control image in mind during a videotaped speech. Ng and Abbott (Reference Ng and Abbott2016) examining the effects of negative, positive and neutral self-image during a speech task on cognitive and attentional processes in clinical and non-clinical sample, found that individuals with SAD reported higher overall ratings on social anxiety symptoms, SFA and greater under-estimation of social performance compared with the control group. However, in contrast to the cognitive model, no differences for the three self-image conditions were observed, showing that a negative self-image had no effect on state anxiety, SFA or performance. The explanation for these unexpected results was that the speech task was threatening and anxiety-inducing for patients with SAD to the extent that anxiety over-ruled the effect of self-image type (positive, negative or neutral).
Taken together, the effect of self-image on SFA and how self-image and SFA interact within patients with social anxiety still remain unclear and need to be further investigated. In addition, current research in this field shows some limitations. Lee et al. (Reference Lee, Ahn and Kwon2019) astutely point out that current research usually compares negative self-image and neutral self-image, neglecting potential benefits of positive self-image. Even when positive self-images were considered in studies (Hirsch et al., Reference Hirsch, Mathews, Clark, Williams and Morrison2003b; Ng and Abbott, Reference Ng and Abbott2016; Vassilopoulos, Reference Vassilopoulos2005) baseline measurements (pre-manipulation of self-image) were neglected. Therefore, it is unclear how far the outcome results stem from the self-image manipulation. Furthermore, even though the current literature highlights that negative self-image increases social anxiety, there is a lack of clarity over direction of the relationship between self-image and SFA. Clark (Reference Clark, Crozier and Alden2001) assumes that a negative self-image can be generated in three different ways. Namely, by a marked distortion in how they perceive others see how they feel, by spontaneously occurring images in which they see themselves as if viewed from an observer’s perspective, and by a more diffuse types of ‘felt sense’.
In response to these limitations in the current literature, the present study investigates the interaction between self-image and social anxiety on SFA and state anxiety during a social interaction situation. High and low socially anxious participants with an activated negative versus positive self-image had a real-time video conversation with an instructed confederate.
According to Clark and Wells’ (Reference Clark, Wells, Heimberg, Liebowitz, Hope and Schneier1995) model, it is expected that high socially anxious participants in general would report more SFA and higher state anxiety than low socially anxious participants. Moreover, an interaction effect is expected, namely that high socially anxious participants with a negative self-image will report higher SFA and higher state anxiety during the conversation compared with those with a positive self-image, and to low socially anxious participants with a negative self-image. According to the reviews of Ng and Abbott (Reference Ng and Abbott2014) and Ng et al. (Reference Ng, Abbott and Hunt2014), self-image seems to have per se an adverse effect on state anxiety. Therefore, the present study explores the effect of self-image on state anxiety and on SFA, controlled for social anxiety.
Method
Participants
The sample was recruited from an online advertisement on the university homepage, and informative flyers were distributed in university buildings, coffee shops and libraries. Individuals aged between 18 and 30 years, fluent in German, and not consuming any drugs (substances or psychopharmacological medication) participated in our experiment. Using the scores of the Social Phobia Scale (SPS: Mattick and Clarke, Reference Mattick and Clarke1998; German version: Stangier et al., Reference Stangier, Heidenreich, Berardi, Golbs and Hoyer1999), we divided participants ad hoc into two groups. The high social anxiety (HSA) group included 27 participants (scores of 20 or more), and the low social anxiety (LSA) group included 36 participants (scores below 20). A score above the cut-off score of 20 indicates social phobia (Stangier et al., Reference Stangier, Heidenreich, Berardi, Golbs and Hoyer1999). The sample details are presented in Table 1.
Table 1. Characteristics of the participants in the high and low social anxiety group
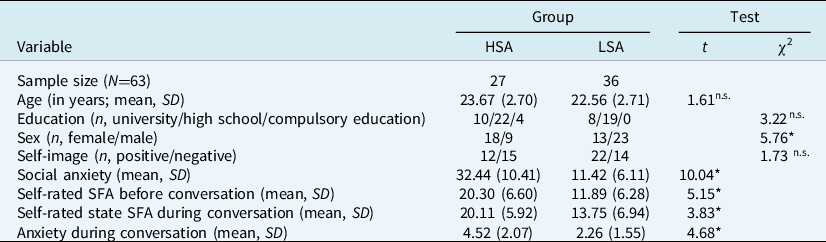
HSA, high social anxiety; LSA, low social anxiety; SD, standard deviation; SFA, self-focused attention. Social anxiety was measured with the Social Phobia Scale. Anxiety during conversation was measured with a visual analogue scale. *p<.05; n.s.not significant.
Materials and procedure
Imagery task
We activated a negative or a positive self-image with an imagery task (e.g. Hulme et al., Reference Hulme, Hirsch and Stopa2012; Vassilopoulos, Reference Vassilopoulos2005). High and low socially anxious participants were instructed to vividly recall either a previously experienced negative social situation (in which they felt anxious) or a positive social situation (in which they felt relaxed and well). Participants were randomly allocated to the negative or positive self-image condition. The literature shows that the negative self-images may come from autobiographical memory (Hackmann et al., Reference Hackmann, Clark and McManus2000). Therefore, we did not instruct participants to hold a specific image in mind chosen by us. Once a memory was brought to mind, participants closed their eyes and were asked a series of questions to elicit details about the situation (e.g. Where are you right now? What do you see in your environment? Who is also present in this situation? What is going on in this scene?) and how they appeared, sounded, and felt (e.g. How do you feel in this situation? What physical sensations do you have in this situation? What is going through your mind? What are you doing right now? How do you see yourself?), in order to help them to visualize the situation. At the end of the imagery task, participants were not specifically instructed to hold the image in mind during the conversation, but the task ended with ‘capture the moment and let it sink in’. The imagery task was delivered through an audio file to ensure standardization for all participants.
Manipulation check
For the manipulation check, we asked participants open-ended questions about their emotions during the imagery task, whether they could recall the image, and what they sensed and felt during the imagery task. On a 10-point scale (ranging from not at all to extremely), participants rated the intensity of their feelings and sensations. Participants who were not able to recall a negative or positive social situation (e.g. when a participant in the negative self-image condition was not able to recall a social situation in which she/he felt anxious) were excluded from the analysis.
Video conversation with a confederate
The participants had a video conversation Footnote 1 with a confederate, believing them to be another study participant. The video conversation lasted for eight minutes on average. Three male and three female confederates were involved in this study. They were briefly informed about the study (they were told that our study is about attention processes during a conversation) and were blind to the condition to which they had been assigned (positive versus negative self-image, high versus low social anxiety group). Confederates were gender matched to the participants (opposite sex). Before the start of the study, the confederates received several hours of training, and instructed to make the conversation as similar as possible for all participants by following scripted questions (e.g. What is your name? Do you study or do you work? What kind of music do you like?).
Social anxiety
Social anxiety was measured with the SPS (SPS: Mattick and Clarke, Reference Mattick and Clarke1998; German version: Stangier et al., Reference Stangier, Heidenreich, Berardi, Golbs and Hoyer1999), which includes 20 items on a 5-point scale ranging from 0 (not at all) to 4 (extremely). A score above the cut-off score of 20 indicates social phobia (Stangier et al., Reference Stangier, Heidenreich, Berardi, Golbs and Hoyer1999). The SPS had high internal consistency in the present study with a Cronbach’s alpha of .91.
Anxiety during the conversation
A visual analogue scale (VAS) was developed to measure anxiety during the conversation. Participants could specify their level of agreement by indicating a position along a continuous line (100 mm) between the two poles (not at all anxious and extremely anxious). The VAS was used three times, at the beginning as baseline, before the conversation, and again immediately after.
Self-focused attention
The 11-item Self-Focused Attention Scale (SFAS: Bögels et al., Reference Bögels, Alberts and de Jong1996) was translated into German (translation and re-translation). Using a 5-point scale from 0 (never) to 4 (very often), participants filled out five items referring to SFA related to arousal, and six items referring to SFA related to interpersonal behavior. Total scores range from 0 to 44, with higher scores indicating increased SFA. The SFAS was used twice: at the beginning of the experiment before the imagery task, to measure trait SFA, and then a slightly adapted version after the conversation that referred to SFA during the video conversation, to measure state SFA. The internal consistency in this study was high, with Cronbach’s alpha of .89 for trait SFAS and .85 for state SFAS.
Integrity of the confederates
At the end of data collection, two independent observers watched all videos of the confederates and rated their behaviour on three items (on a 5-point Likert scale), namely, friendliness, speech flow (clear and fluent language), and body language (open and interested behaviour).
Procedure
At the beginning, the participants were informed in detail about the course of the experiment. However, they were not informed about the confederate, but told that they would have a conversation with another participant. All of them signed an informed consent form and then completed a demographic questionnaire about age, education, sex, the SPS, the trait SFAS, and the state anxiety-VAS for the first time on the computer. Next, participants received instructions about the imagery task and the video conversation, and filled out the state anxiety-VAS twice. Then we activated a negative or a positive self-image with the imagery task, and immediately thereafter, participants had a video conversation with the confederate. During the conversation, participants observed the video image of themselves and the confederate’s image on their computer screen. After the conversation, participants again filled out the state anxiety-VAS and the state SFAS on the computer. After the manipulation check questions, the participants were debriefed about the experiment and the true identity of the confederate, thanked, and paid (40 CHF in cash).
Statistical analyses
Data preparation and data checks were conducted using SPSS 22. Differences between the HSA and LSA groups on sample characteristics were computed with t-tests and chi-square tests. To analyse baseline differences between negative and positive self-image, t-tests were conducted. Group differences regarding state anxiety and self-rated SFA during the experiment were analysed using general linear models (GLM) repeated measures, with between-subjects factors social anxiety (high versus low) and self-image (positive versus negative) and within subject factor state anxiety (baseline, before, and after conversation) respectively SFA (before and after conversation). We were interested in main effects for social anxiety and self-image as well as in their interaction. Due to technical problems, the VAS of seven participants could not be recorded (all questionnaires were conducted online). There were significant differences between the sex distribution of the high and low socially anxious groups. All analyses were controlled for sex, but it was not found to have effects on the statistical models.
The explorative analysis for group differences regarding state anxiety and self-rated SFA during the experiment were analysed using GLM repeated measures, with between-subjects factor self-image (positive versus negative), within-subject factor state anxiety (before and after conversation) respectively SFA (before and after conversation), and with social anxiety as covariate.
An alpha level of .05 was used to denote a significant result and partial eta squared was specified for effect size.
Results
Differences between HSA and LSA groups
The two experimental groups did not differ significantly in age or education (see Table 1). The HSA group included more female participants. As expected, the HSA group showed significantly higher trait SFA, higher state SFA, and higher anxiety during the conversation compared with the LSA group (see Table 1).
Baseline comparison between negative and positive self-image
Comparing the self-image groups, no baseline differences were found in social anxiety (negative self-image: mean = 21.41, SD = 12.37; positive self-image: mean = 19.59, SD = 14.15; t 61 = .54, p = .591), state anxiety (negative self-image: mean = 11.96, SD = 7.47; positive self-image: mean = 12.33, SD = 5.11; t 61 = .23, p = .816), and SFA (negative self-image: mean = 15.43, SD = 6.26; positive self-image: mean = 15.62, SD = 8.71; t 61 = .14, p = .889).
Manipulation check and integrity of the confederates
Eighty-six per cent of the participants reported having a clear recall of their image. There were no significant differences in recalling the image between positive and negative self-image condition (χ2 (1, 63) = 1.80, p = .180).
The HSA versus LSA groups did not differ in recalling the self-image (χ2 (1, 63) = .01, p = .917) or the mean intensity of their feelings (HSA: mean = 5.89, SD = 1.58 versus LSA: mean = 5.72, SD = 2.41, t 61 = –0.10, p = .919).
Regarding integrity of the confederates, no significant differences were found in confederates’ behaviour towards the HSA versus LSA group (F 3,32 = 1.16, p = .339, η2 = .10). Inter-rater reliability was excellent, with .949 with a 95% confidence interval from .899 to .974.
The influence of social anxiety and self-image on state anxiety
Table 2 presents the main and interaction effects of social anxiety (HSA versus LSA) and self-image (positive versus negative) on state anxiety and SFA. The main effect for social anxiety was significant (p = .002); the HSA group reported more anxiety during the experiment compared with the LSA group. The main effect for self-image on state anxiety was not significant. However, a significant interaction effect between self-image and social anxiety was shown by the fact that the HSA group with a negative self-image were more anxious during and after the conversation compared with both the LSA group, and participants with a positive self-image (see Fig. 1).
Table 2. Main and interaction effects of social anxiety (high versus low) and self-image (positive versus negative) groups on state anxiety and SFA (before and during the conversation)

SA, social anxiety; SFA, self-focused attention.
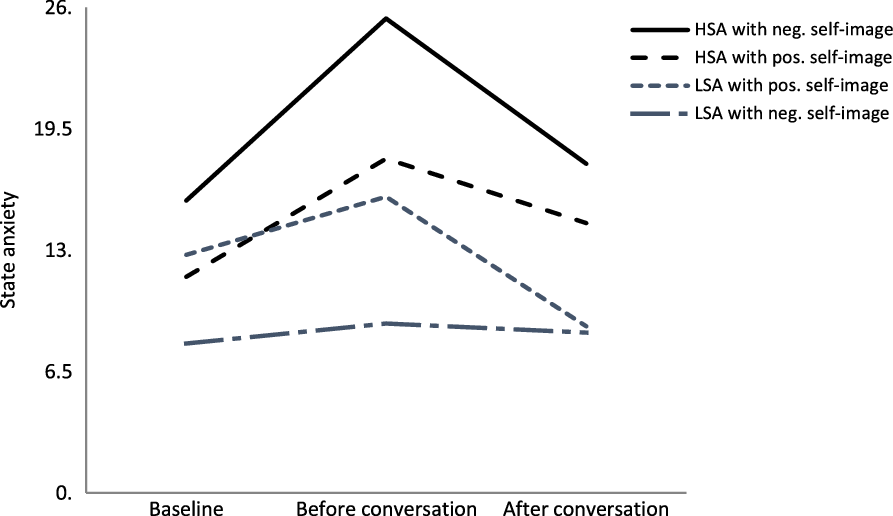
Figure 1. The interaction effect between social anxiety (high versus low social anxiety) and self-image (negative versus positive self-image) on state anxiety.
The influence of social anxiety and self-image on SFA
Main and interaction effects of the social anxiety (HSA versus LSA) and self-image (positive versus negative) on SFA are also presented in Table 2. The main effect for social anxiety was significant (p = .000); the HSA group showed increased SFA before and during the conversation compared with the LSA group. Neither a main effect of self-image nor an interaction effect between social anxiety and self-image was found for SFA.
Explorative analysis
GLM repeated measures controlled for social anxiety revealed a significant main effect for self-image on state anxiety (F 1,59 = 6.12, p = .016, η2 = .10), indicating that participants with a negative self-image reported higher state anxiety than those with a positive self-image before and during the conversation (independent of social anxiety groups). Again, self-image had no main effect on SFA (F 1,59 = .21, p = .648, η2 = .00).
Discussion
The current experiment investigated the role of self-image on self-focused attention and state anxiety in high versus low socially anxious individuals. High and low socially anxious individuals with either a negative or a positive self-image participated in a conversation with a confederate. High socially anxious participants with a negative self-image reported higher state anxiety than those with a positive self-image and compared with low socially anxious participants. In line with the model of Clark and Wells (Reference Clark, Wells, Heimberg, Liebowitz, Hope and Schneier1995), high socially anxious individuals showed higher levels of SFA and social anxiety during the conversation than low socially anxious participants. SFA, on the other hand, was only affected by social anxiety, but not by self-image. When analyses were controlled for social anxiety, a negative self-image was significantly associated with increased state anxiety; however, self-image had again no effect on SFA.
The cognitive model of Clark and Wells (Reference Clark, Wells, Heimberg, Liebowitz, Hope and Schneier1995) assumes that SFA and a negative self-image have an important role in developing and maintaining social anxiety. However, it is still unclear how SFA and self-image interact. In line with previous research (e.g. Hirsch et al., Reference Hirsch, Clark, Mathews and Williams2003a, b, Reference Hirsch, Meynen and Clark2004, Reference Hirsch, Mathews, Clark, Williams and Morrison2006; Vassilopoulos, Reference Vassilopoulos2005) our results showed an effect of self-image on anxiety. An interaction effect indicated that high socially anxious individuals with a negative self-image in particular were more anxious compared with those with a positive self-image and to those with low social anxiety. Controlling for social anxiety, we found again that a negative self-image enhanced state anxiety in all participants. This result is in line with Hirsch et al. (Reference Hirsch, Mathews, Clark, Williams and Morrison2006), who found that confident public speakers with a negative self-image in mind reported higher anxiety during a speech compared with speakers with a positive self-image, and to a control group with a neutral self-image. Thus, in accordance with the literature, a negative self-image seems to have a strong adverse effect on anxiety.
Regarding the path from SFA to anxiety, we could replicate the significant association between social anxiety and increased SFA proven in previous researches (e.g. Bögels and Mansell, Reference Bögels and Mansell2004; Vriends et al., Reference Vriends, Meral, Bargas-Avila, Stadler and Bögels2017; Woody and Rodriguez, Reference Woody and Rodriguez2000; Zou et al., Reference Zou, Hudson and Rapee2007). In contrast to Makkar and Grisham (Reference Makkar and Grisham2011), we found no effect of self-image on SFA. An explanation might be that in Makkar and Grisham’s study, participants held fictive self-images related to a speech situation in mind, whereas the present study allowed a freely chosen autobiographic self-image. As such, the recalled image in the present study was not by definition congruent with the task at hand, and perhaps therefore did not affect SFA. Another explanation could be a difference in the social situation that was investigated. In Makkar and Grisham, participants were involved in a performance situation – a videotaped brief speech – whereas participants in the present study were involved in a social interaction situation. Thus, a negative self-image might be more involved in performance situations compared with in social interaction situations, as in performance situations, the direction of attention is less interactive, and therefore SFA might be easier to maintain. Interaction situations, on the other hand, require more complex interpersonal social behaviours, and thus, cognitive resources for holding a self-image in mind might be more limited. Indeed, research repeatedly highlighted a positive association between social anxiety and SFA in public speaking or speech tasks (e.g. Deiters et al., Reference Deiters, Stevens, Hermann and Gerlach2013; Woody and Rodriguez, Reference Woody and Rodriguez2000) than in social interactions situations (e.g. Alden et al., Reference Alden, Teschuk and Tee1992; Bögels et al., Reference Bögels, Rijsemus and De Jong2002). Nevertheless, the missing association between self-image and SFA is in line with Ng and Abbott (Reference Ng and Abbott2016), who used a speech task with a free-chosen self-image. Taken together, the literature suggests that a negative self-image might enhance SFA in public speaking, and in conditions in which a situation-congruent self-image is chosen. Future studies should investigate these contrasts in findings. Unlike the studies of Makkar and Grisham (Reference Makkar and Grisham2011) and Ng and Abbott (Reference Ng and Abbott2016), the strength of our study is the pre- and post-conversation collection of data about state anxiety and SFA, which clarifies the influence of self-image on state anxiety and on SFA. It should also be mentioned that the link between self-image and SFA is not clearly defined in the cognitive model of Clark and Wells (Reference Clark, Wells, Heimberg, Liebowitz, Hope and Schneier1995). According to the cognitive model, when socially anxious individuals enter a feared social situation, negative automatic thoughts lead to a shift in attention towards self-processing and the individuals take an observer perspective. They use interoceptive information produced by self-focus to construct an image of themselves, which is mostly negative. This image could be experienced as a felt sense or a picture in their mind’s eye. Thus, self-image seems to be a part within SFA. On the other hand, a negative self-image can be generated in three different ways: firstly, by a marked distortion that others see them in the same way as how they feel (e.g. feeling anxious is equal to looking anxious); secondly, by spontaneously occurring images in which they see themselves as if viewed from an observer’s perspective; and finally, a more diffuse types of ‘felt sense’ (Clark, Reference Clark, Crozier and Alden2001). Thus, the place of self-image in the model remains unclear. In line with previous research, our results highlight the strong effect of self-image on social anxiety. However, our results show that SFA was not affected by self-image.
The present study has the following limitations. Although the HSA group in the present study had social anxiety scores comparable to those of clinical samples (Berger et al., Reference Berger, Hohl and Caspar2009), this was not a clinical patient sample diagnosed with SAD. Thus, our results cannot be generalized to patients with SAD. Furthermore, the current study did not include a control condition without self-image manipulation, leaving open the hypothesis that having any self-image in mind (positive or negative) affects SFA in social situations. We did not control the content of the free-chosen self-image, thus, it leaves open to question whether we captured a typical self-image for this person, or if the self-image matched the task at hand. In addition, we did not instruct participants specifically to hold the self-image in mind during the conversation, with the intention of measuring the effect of self-image on SFA in a more subtle way. For the manipulation check, we asked participants to rate the intensity of their emotions during the imagery task, but not how positive or negative the recalled self-image was. We also did not enquire if the recalled self-image was situation congruent. Finally, we do not know exactly how the participants use their own video image. Observing their own video image might have manipulated SFA, increasing the perception of their own SFA. On the other hand, the video image might have been less anxiety-creating for low socially anxious individuals or might even have helped to correct their distorted self-view, as seen in the study of McManus et al. (Reference McManus, Clark, Grey, Wild, Hirsch, Fennell, Hackmann, Waddington, Liness and Manley2009) and Warnock-Parkes et al. (Reference Warnock-Parkes, Wild, Stott, Grey, Ehlers and Clark2017).
The present study underlines the following research implications. Future research should include a clinical sample to investigate the differences between social anxiety and SAD. Furthermore, several self-image conditions (negative, positive, neutral) and a condition with no self-image manipulation would be important to clarify the effect of self-image. To investigate the specificity of self-image, future studies should incorporate different social situations, such as a brief speech and conversation. Moreover, it is important to investigate whether the influence of self-image is more effective when an individual holds in mind congruent images related to the social interaction task. Thus, self-image manipulation with congruent and incongruent images could be conducted in future research. A control group without participants’ own video display should be added to investigate the manipulation of SFA. Further studies could also include safety behaviours, which play an important role in maintaining social anxiety too. It would be very informative to examine how much participants take part in the conversations and if there would be any differences between socially anxious and non-anxious individuals. Results regarding the relationship between self-image, SFA and safety behaviours would deliver a clearer understanding of the cognitive model of social anxiety.
In conclusion, the present study confirms once again the strong influence of negative self-image and increased SFA on social anxiety. Moreover, the present study highlights that a negative self-image has an adverse effect on anxiety for all participants, but especially for those with social anxiety. As described in the cognitive model of Clark and Wells (Reference Clark, Wells, Heimberg, Liebowitz, Hope and Schneier1995), increased SFA is associated with heightened anxiety during social interactions. However, the present results do not show a direct link between self-image and SFA, namely that SFA was not affected by a negative self-image. If the present results can be replicated in further research with clinical samples, greater clarity might be achieved regarding the place of self-image in the cognitive model of Clark and Wells (Reference Clark, Wells, Heimberg, Liebowitz, Hope and Schneier1995). Furthermore, as our results highlight the crucial role of SFA and self-image on social anxiety, it would be important to update the role of self-image in treatments for social anxiety.
Acknowledgements
None.
Financial support
This study was supported by grant 100014_135331 from the Swiss National Science Foundation.
Conflicts of interest
The authors declare none.
Ethics statements
The experiment took place at the Department of Psychology, University of Basel and was reviewed and approved by the local ethics committee (Ethikkommission beider Basel 338/08). All authors have abided by the Ethical Principles of Psychologists and Code of Conduct.
Data availability
Data are available on request due to privacy/ethical restrictions.
Author contributions
Yasemin Meral: conceptualization (equal), data curation (lead), formal analysis (lead), investigation (equal), methodology (equal), project administration (supporting), writing – original draft (lead); writing – review and editing (lead); Noortje Vriends: conceptualization (equal), formal analysis (equal), funding acquisition (lead), investigation (equal), methodology (equal), project administration (lead), writing – original draft (equal).




 Open access
Open access
Comments
No Comments have been published for this article.