This journal utilises an Online Peer Review Service (OPRS) for submissions. By clicking "Continue" you will be taken to our partner site https://www.editorialmanager.com/ashe/default.aspx. Please be aware that your Cambridge account is not valid for this OPRS and registration is required. We strongly advise you to read all "Author instructions" in the "Journal information" area prior to submitting.
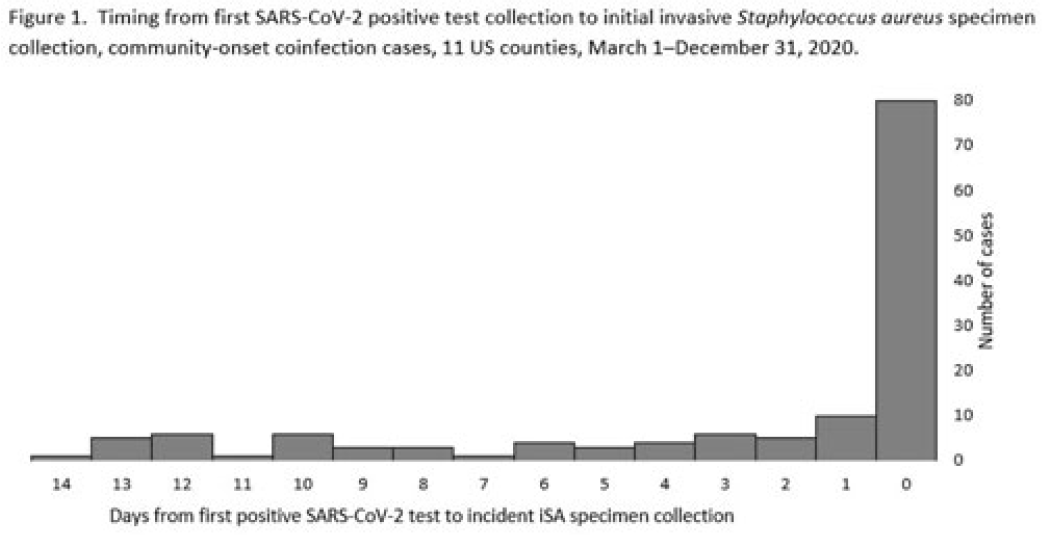
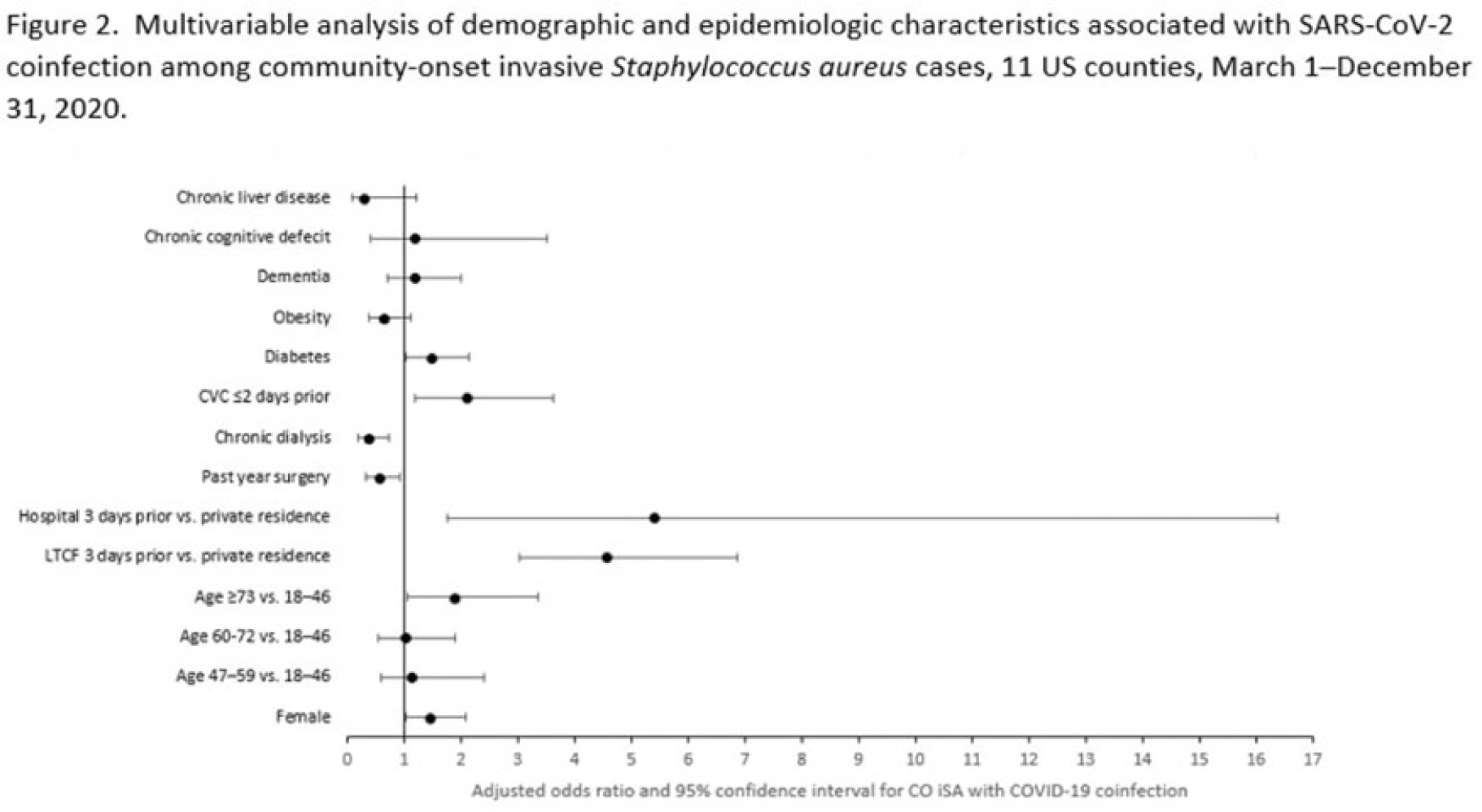
Background: Previous analyses describing the relationship between SARS-CoV-2 infection and Staphylococcus aureus have focused on hospital-onset S. aureus infections occurring during COVID-19 hospitalizations. Because most invasive S. aureus (iSA) infections are community-onset (CO), we characterized CO iSA cases with a recent positive SARS-CoV-2 test (coinfection). Methods: We analyzed CDC Emerging Infections Program active, population- and laboratory-based iSA surveillance data among adults during March 1–December 31, 2020, from 11 counties in 7 states. The iSA cases (S. aureus isolation from a normally sterile site in a surveillance area resident) were considered CO if culture was obtained <3 days after hospital admission. Coinfection was defined as first positive SARS-CoV-2 test ≤14 days before the initial iSA culture. We explored factors independently associated with SARS-CoV-2 coinfection versus no prior positive SARS-CoV-2 test among CO iSA cases through a multivariable logistic regression model (using demographic, healthcare exposure, and underlying condition variables with P<0.25 in univariate analysis) and examined differences in outcomes through descriptive analysis. Results: Overall, 3,908 CO iSA cases were reported, including 138 SARS-CoV-2 coinfections (3.5%); 58.0% of coinfections had iSA culture and the first positive SARS-CoV-2 test on the same day (Fig. 1). In univariate analysis, neither methicillin resistance (44.2% with coinfection vs 36.5% without; P = .06) nor race and ethnicity differed significantly between iSA cases with and without SARS-CoV-2 coinfection (P = .93 for any association between race and ethnicity and coinfection), although iSA cases with coinfection were older (median age, 72 vs 60 years , P<0.01) and more often female (46.7% vs 36.3%, P=0.01). In multivariable analysis, significant associations with SARS-CoV-2 coinfection included older age, female sex, previous location in a long-term care facility (LTCF) or hospital, presence of a central venous catheter (CVC), and diabetes (Figure 2). Two-thirds of co-infection cases had ≥1 of the following characteristics: age > 73 years, LTCF residence 3 days before iSA culture, and/or CVC present any time during the 2 days before iSA culture. More often, iSA cases with SARS-CoV-2 coinfection were admitted to the intensive care unit ≤2 days after iSA culture (37.7% vs 23.3%, P<0.01) and died (33.3% vs 11.3%, P<0.01). Conclusions: CO iSA patients with SARS-CoV-2 coinfection represent a small proportion of CO iSA cases and mostly involve a limited number of factors related to likelihood of acquiring SARS-CoV-2 and iSA. Although CO iSA patients with SARS-CoV-2 coinfection had more severe outcomes, additional research is needed to understand how much of this difference is related to differences in patient characteristics.
Disclosures: None
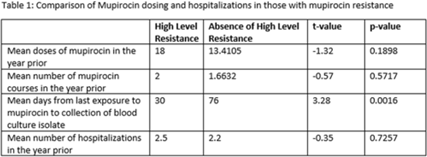
Methicillin-resistant Staphylococcus aureus (MRSA) is a common etiology of hospital-acquired infections (HAIs). One strategy to reduce HAIs due to MRSA involves a multistep decolonization process. This often involves nasal application of mupirocin 2% ointment. In our institution, when individuals meet criteria for decolonization, we recommend 5 days of treatment given twice daily. High levels of mupirocin resistance have been reported in some hospital systems, with >80% of tested isolates being resistant. To better understand our resistance levels, we selected 238 MRSA isolates from blood cultures to be tested for mupirocin resistance to correlate the presence of resistance and use of mupirocin for decolonization. We choose to assess MRSA blood isolates rather than nasal swabs given that we aim to prevent invasive MRSA infections, including blood stream infections, with decolonization. The blood cultures were collected from 11 acute-care facilities within our system from March 2021 through June 2022. High-level resistance was defined as an MIC >1,024 μg/mL according to Clinical and Laboratory Standards Institute guidelines. Of those, 7.14% showed high level resistance, and 76.47% occurred in those who were exposed to mupirocin and 23.53% occurred in those without mupirocin exposure (P = .0094). On average, those with high-level resistance had had more recent exposure to mupirocin compared to those without resistance, which was statistically significant. Also, those with high resistance, on average, received more doses of mupirocin, although this was not statistically significant. Conclusions: More recent and higher number of doses of mupirocin were associated with the development of resistance, which is consistent with what we know from pharmacodynamics of antibiotic resistance with other agents. These findings may be particularly important for those patients who have frequent hospitalizations and often require decolonization. Understanding baseline mupirocin resistance levels in an institution can assist with determining decolonization strategies.
Disclosures: None
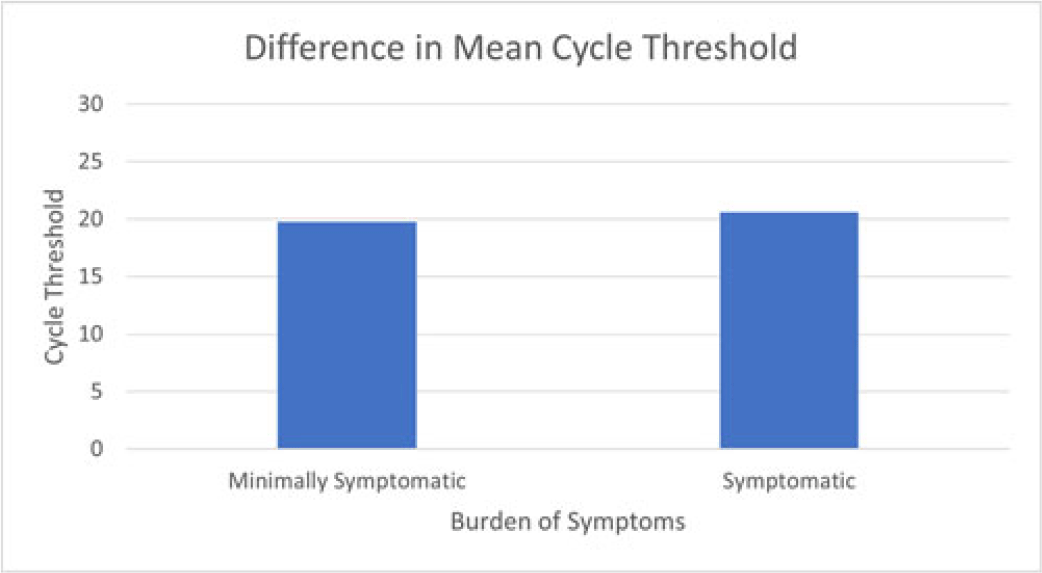
Background: Directing COVID-19 diagnostic testing to healthcare workers (HCWs) who are likely to be infected has potential to reduce staffing shortages and decrease opportunity for in-hospital transmission; however, HCWs with COVID-19 may exhibit a range of symptoms. We assessed the burden of symptoms in relation to cycle threshold (Ct) values as a surrogate for viral shedding in vaccinated healthcare workers. Methods: We retrospectively reviewed employee health records of COVID-19–vaccinated employees who tested positive for SARS-CoV-2 between December 2020 and January 2022 at 2 academic hospital systems. We reviewed demographic data, reasons for testing including symptoms, exposure history, medical history, vaccination dates, Ct values, and genotypes when available. We compared mean Ct values between symptomatic and minimally symptomatic cases using independent sample t tests. Patients were defined as minimally symptomatic if they had no symptoms or a single symptom that is not cough, fever, or anosmia at the time of testing. Patients were defined as more symptomatic if they reported >1 symptom or cough, fever, or anosmia. Results: In total, 298 HCWs tested positive for COVID-19. Most positive cases were female (73%), white (78%), and had patient-facing roles (77%). Genotypic testing (n = 109) revealed that most genotypes belonged to the SARS-CoV-2 delta variant (AY lineages, B1.617.2). More cases were minimally symptomatic (62%) than were more symptomatic (38%). None required hospitalization during the study period. Mean Ct values (n = 141) showed no significant difference between more symptomatic and minimally symptomatic cases (19.8 vs 20.6; P = .40) (Fig. 1). Also, there was no significant difference in mean Ct value, comparing those with vaccination 90 days prior to positive (20.52 vs 19.88; P = .537). Conclusions: Our study shows no significant difference in cycle threshold values between minimally symptomatic and more symptomatic infections in vaccinated HCWs. In addition, HCWs exhibit high viral load even when infected within 90 days after vaccination. When considering whether to attend work, HCWs should be aware that mild symptoms and recent vaccination do not necessarily reflect low transmissibility and that they should follow CDC guidance regarding when to return to work.
Disclosures: None
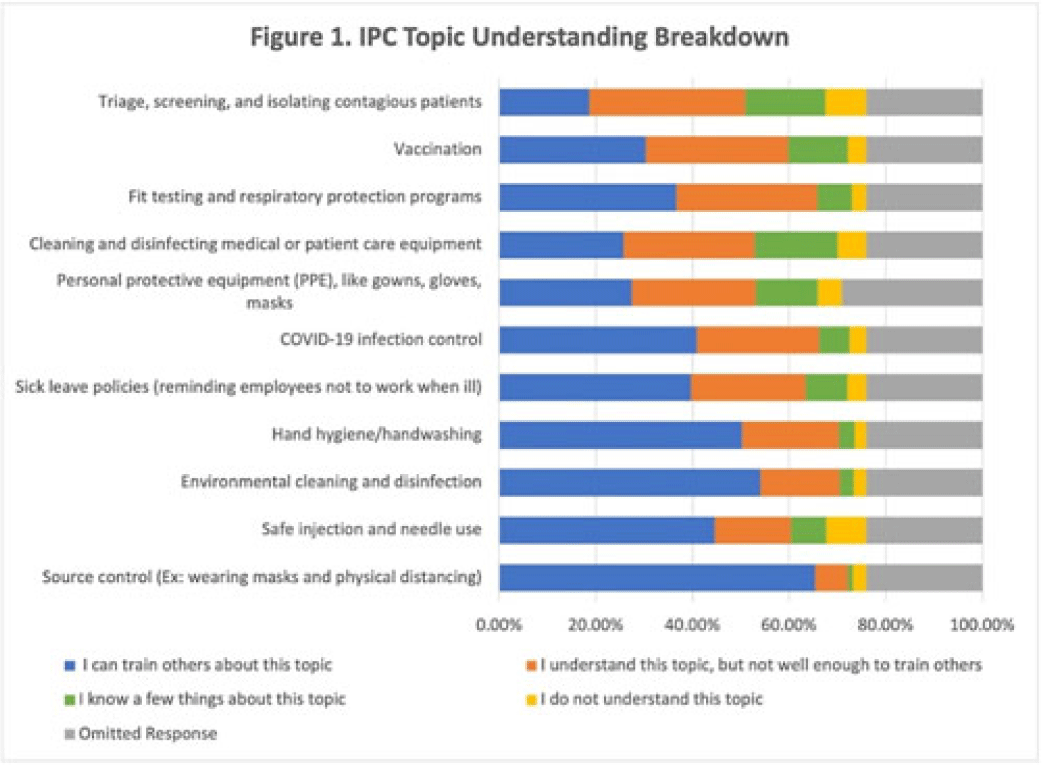
Background: Infection prevention and control (IPC) competency is critical for healthcare personnel (HCP) and patient safety. In collaboration with the CDC new national IPC training collaborative called Project Firstline, the Oregon Health Authority’s (OHA) Healthcare Associated Infection (HAI) Program established a state-level program in 2021. The goal of Oregon Project Firstline is to provide relevant, accessible, and engaging IPC training materials for our state’s HCP. We assessed the IPC learning needs of Oregon’s healthcare workforce, and to understand the preferred methods and formats of training across the various HCP roles. Methods: OHA’s HAI program recruited HCP by distributing electronic surveys through multiple healthcare, regulatory, and public health partners’ email listservs and HCP-targeted newsletters. Survey responses were recorded from September 23 to December 10, 2021. The HAI program assessed respondents’ IPC knowledge, online and in-person job training preferences, frequently used training devices, and trusted sources for IPC information. An individual’s understanding of an IPC topic was categorized based on their self-assessed confidence in their knowledge and ability to teach the topic to others. In total, 6,382 surveyed responses were analyzed. Results: The average understanding among HCP was lowest in IPC topics relating to triage and isolation of contagious patients and fit testing of respiratory protection devices. For these topics, 3,208 HCP (66.21%) and 3,657 HCP (75.48%) HCP, respectively, did not understand the topic well enough to teach others (Fig. 1). The highest number of HCP (n = 2,512, 39.36%) requested additional training in methods on how to educate others about IPC topics (ie, “train the trainer”). Surveyed respondents most frequently used personal computers for job trainings in both work and at-home settings (n = 4,603, 72.12%) and 3,437 HCP (53.85%) were open to either in-person or remote formats for job education. The CDC and OHA were the most frequented and trusted IPC sources among surveyed HCP: 4,124 HCP (64.62%) and 3,584 HCP (56.16%), respectively. Conclusions: IPC is a critical topic in HCP training across all healthcare facility types and employee roles. Effective educational planning includes understanding the learners’ knowledge needs and preferred methods of learning. Our learning needs assessment identified important IPC knowledge gaps and will help ensure that our training courses will be offered in effective educational formats for Oregon’s diverse HCP. Future training will include appropriate triage of potentially infectious patients, respiratory fit testing, and general IPC “train the trainer” sessions. Additionally, we will offer both in-person and remote options.
Disclosures: None
