This journal utilises an Online Peer Review Service (OPRS) for submissions. By clicking "Continue" you will be taken to our partner site https://www.editorialmanager.com/ashe/default.aspx. Please be aware that your Cambridge account is not valid for this OPRS and registration is required. We strongly advise you to read all "Author instructions" in the "Journal information" area prior to submitting.
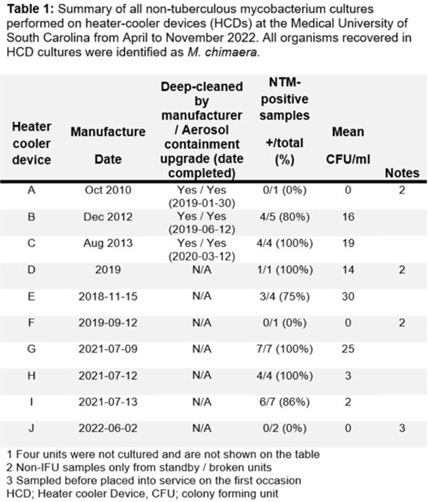
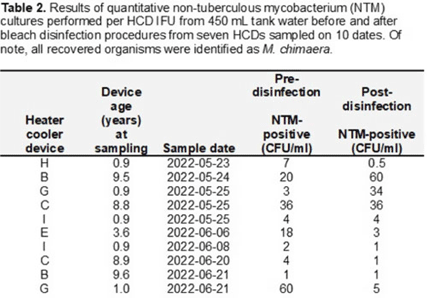
Background: The global outbreak of Mycobacterium chimaera infections associated with HCDs resulted in new maintenance recommendations. Since 2018, HCDs have been disinfected according to instructions for use (IFU), including twice-monthly bleach disinfection and monitoring hydrogen peroxide (H2O2) to maintain a minimum daily concentration of 100 ppm. In February 2020, the IFU added the recommendation to perform microbiologic surveillance of HCD tank water to ensure effectiveness of disinfection to levels of <1 colony forming unit per milliliter (CFU/mL) of nontuberculous mycobacterium (NTM). We report our experience with this microbiologic surveillance as well as that of culturing the HCD environment to investigate modes of transmission. Methods: In 2022, we began culturing tank water in 10 HCDs for NTM. For a subset of 6 HCDs, quantitative NTM culturing of tank water before and after bleach disinfection was done. After initial results indicated widespread-contamination of HCDs with M. chimaera, we performed fill water cultures from 5 sinks in 4 HCD maintenance rooms. We also conducted 20 two-hour NTM settle-plate cultures of a cardiac operating room (OR) at different sites both inside (n = 7) and outside (n = 3) the OR: 10 with the HCD (located outside the OR) turned off (controls) and 10 with HCD turned on (exposure). A paired t test was used to evaluate differences in mean recovery of NTM in tank water samples. Results: Cultures from 7 (70%) of 10 HCDs were positive, with a mean of 13.6 CFU/mL M. chimaera (Table 1). There was no significant difference between the 10 pairs of pre- and postdisinfection NTM cultures done according to the IFU from 6 HCDs: mean predisinfection cultures (15.5 CFU/mL) versus mean postdisinfection cultures (12 CFU/mL) (P = .90) (Table 2). For fill water, 1 of 7 sink samples in 1 of 4 rooms was positive for M. chimaera ( <1 CFU/mL) from a specimen from a fresh 0.2-µm filter that had been stored in the fill-sink splash zone. OR settle-plate cultures showed 0 (0%) of 10 control sites and 1 (10 %) of 10 exposure sites inside the OR positive for NTM, with a single CFU of M. avium–intracellulare complex. Conclusions: Our data cannot clearly refute either of 2 possible scenarios for HCD contamination: cross contamination during device maintenance versus at the point of manufacture. Despite the IFU guidance or disinfection being implemented, disinfection procedures failed to suppress NTM contamination, and tank water within most HCDs was contaminated with M. chimaera regardless of age or whether it was deep cleaned or upgraded with an aerosol containment device.
Disclosures: None
Background: Aeromonas is a gram-negative rod known to be present in water, sewage and soil which may cause infections especially in immunocompromised hosts. Cases of Aeromonas gastroenteritis have been associated with warmer weather. In total, 3 patients with extensively drug resistant (XDR) Aeromonas were identified at our facility between August and September 2022 on 2 intensive care units (ICUs). Our infection prevention, microbiology, and facility teams investigated these cases to determine whether a common source could be the mode of transmission. Methods: To first determine whether patients’ Aeromonas specimens were related, whole-genome sequencing (WGS) of the clinical isolates from 3 patients was performed using the Illumina DNA Prep Kit and Illumina MiSeq. Sequencing analysis was performed using CLC Genomics Workbench for de novo assembly, single-nucleotide polymorphisms (SNP) calling, and tree generation, Geneious Prime for reference-based assembly, annotation, and quality assessment, KmerFinder for reference identification, and the Comprehensive Antibiotic Resistance Database for resistance gene detection via protein homology. Chart review revealed that patients occupied multiple rooms between 2 ICUs (Fig. 1). Because water is a known source of Aeromonas, facility records were reviewed for water intrusion events. This analysis identified several cases in the affected patient and surrounding rooms. Sinks and faucets from 10 rooms were swabbed followed by direct plating on blood, MacConkey agar, and Aeromonas-selective cefsulodin-Irgasan-novobiocin (CIN) agar plates. Lastly, the city temperatures before and after positive cases were reviewed to identify whether any correlation could be shown between temperature and timing of infection. Results: WGS analysis revealed that the 3 Aeromonas isolates (all identified as A. hydrophila) were not directly related (minimum distance, 934 SNPs) and harbored between 4 and 19 unique antimicrobial resistance genes, including co-occurring carbapenemases VIM-2 and KPC-3 in 1 isolate and OXA-232 in another. Of the 20 environmental samples, few gram-negative nonfermenting bacteria and no Aeromonas isolates were detected (Fig. 1). Elevated city did loosely proceed patient cases of Aeromonas, suggesting a possible role of higher temperature, which may have promoted the growth of Aeromonas during the periods of the 3 cases and thus may contribute to the nosocomial infections (Fig. 2). Conclusions: Although our investigation did not reveal a definitive cause for the Aeromonas cases, it did show the importance prompt identification and investigation can have on mitigating the spread of a cluster. Our facility has not identified any additional nosocomial cases. Monitoring water intrusion events and plans for remediation continue to be a priority.


Disclosures: None
Background: Burkholderia cepacia complex is an opportunistic environmental pathogen that has been linked to nosocomial outbreaks. We describe an outbreak of bacteremia caused by Burkholderia cenocepacia from a contaminated chlorhexidine gluconate solution. Methods: The hospital infection control team carried out an outbreak investigation on February 21, 2021, when 3 adult hemodialysis patients developed B. cenocepacia bacteremia. Patient demographics and clinical profile were reviewed retrospectively. Potential sources of infection were identified, and environmental screening was performed in several units. Processes of catheter care in the hemodialysis unit were reviewed. Water samples from the hemodialysis unit, and samples of solutions used in patient care were sent for culture. Isolates from patients and from environmental samples were sent for 16S rRNA gene sequencing to determine genetic relatedness. Results: In total, 16 patients, 8 of whom were male, developed B. cenocepacia bacteremia during the investigated period. The median age was 68 years (range, 19–83), and 15 of 16 had at least 1 comorbidity. All patients used a central venous catheter (CVC) for hemodialysis, and 11 (70%) of these 16 were temporary. Chlorhexidine gluconate solution was routinely used as part of CVC care and 1 bottle was shared among 4 hemodialysis stations. On suspicion of contamination, all identified chlorhexidine bottles were recalled on February 26, 2021, and random samples from 15 opened and 19 unopened bottles were sent for culture from the following units: hemodialysis (n = 2), ICU (n = 14), wards (n = 6), and 4 each from transplant surgery, and delivery suites. O0f 34 sampled bottles, 17 grew B. cenocepacia: 8 opened and 9 unopened bottles. The Bayesian inference tree (Fig. 1) supports the hypothesis that patient samples and the samples from the chlorhexidine solutions were most probably related to each other based on the 16S rRNA sequences. However, the individual identities of the specific sample sequences could not be determined using the analyzed region of the gene, possibly due to low quality of the sequences received. No new cases of B. cenocepacia were identified after recall of the chlorhexidine solution, and the outbreak was deemed resolved on March 24, 2021. Conclusions: Medical solutions routinely used in patient care can cause outbreaks and should be suspected as a potential source of infection by infection control teams.

Disclosures: None
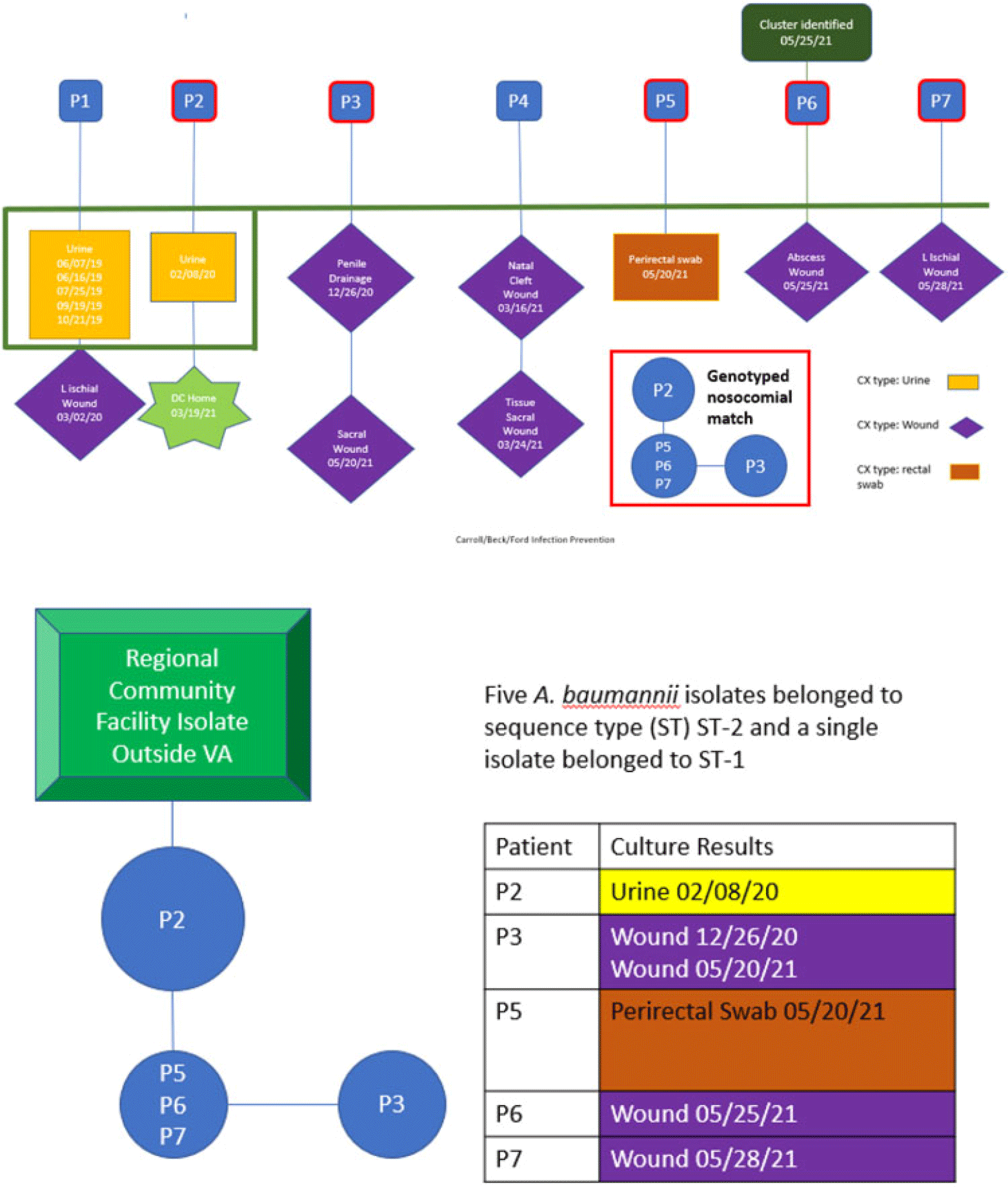
Background: Drug-resistant pathogens are a significant source of increased cost and patient complications in long-term and/or congregate care settings. Once introduced, depending on the environmental niche in which they establish and the mechanisms they employ for survival, they can be difficult to eradicate. We report the details of an epidemiologic investigation of a multidrug-resistant Acinetobacter baumannii (MDR-A) outbreak in a spinal cord intervention (SCI) unit within a Veterans Affairs facility in San Antonio, Texas, that was identified after back tracing a positive wound culture from a long-term resident. Methods: All MDR-A isolates were matched to the patients harboring them. Their clinical, epidemiologic, and geographic histories within our facility were traced. All potentially shared characteristics between cases were evaluated closely. Results: In total, 5 cases were determined to be likely connected over a period of ~18 months starting December 2020. The extant isolates underwent molecular evaluation and were genetically related. Patient activity was traced by the infection prevention team to identify potential sources of transmission. Environmental sampling after standard cleaning found a common strain on a shower trolley shared by these patients. Following focused cleaning of this and other shared locations, no new related isolates have been identified from patient or environmental samples. Conclusions: In this case, investigation by the infection prevention team of a single multidrug-resistant organism led to identification and eradication of a potential pathogen. Despite standard cleaning processes, a likely shared fomite was identified and decontaminated, thereby preventing future infections. This case exemplifies the value of thorough epidemiologic study paired with modern molecular methods of identification.
Disclosures: None
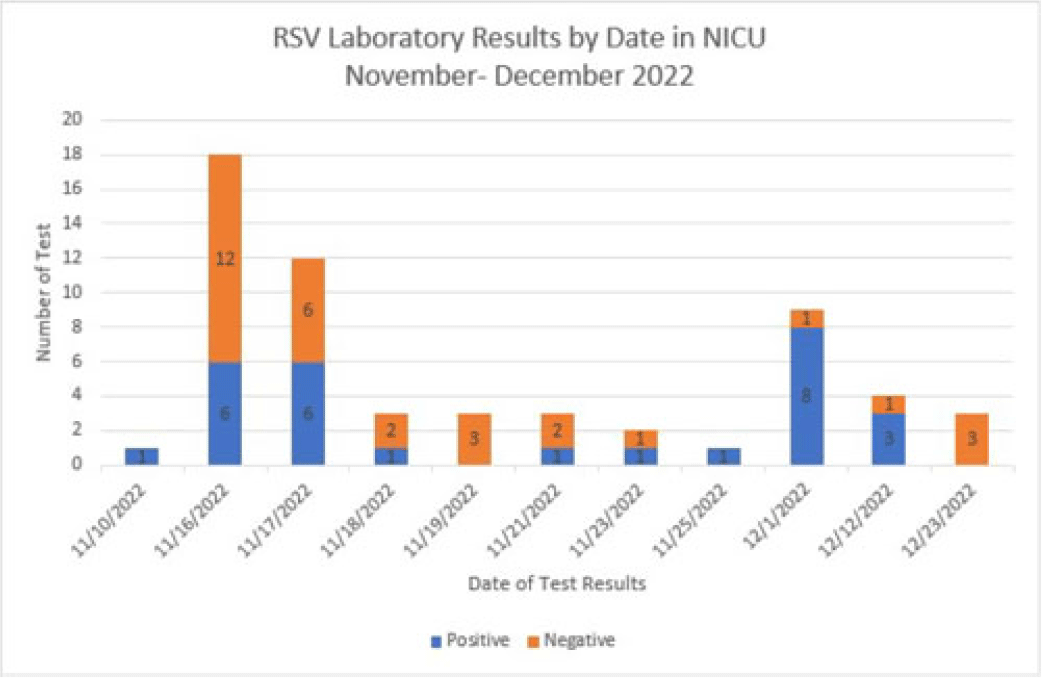
Background: Respiratory syncytial virus, RSV, is a respiratory virus that causes cold-like symptoms in adults. In infants and young children, RSV can cause severe illnesses such as bronchiolitis or pneumonia. We describe a successful response to a laboratory-confirmed RSV outbreak in a 21-bed open-pod neonatal intensive care unit (NICU) at a level 2 trauma hospital. Methods: After 2 of the 3 initial neonates were diagnosed with hospital-onset RSV, an outbreak investigation began on November 16, 2022. Following the results, testing was expanded to all neonates in the NICU. The clinical case was defined as a hospitalized neonate with laboratory confirmation of RSV by RSV antigen screen or polymerase chain reaction (PCR) detection on the Biofire respiratory panel. Outbreak resolution was determined by utilizing a viral test for the remaining positive neonates after the 2-week incubation period from the last identified positive neonate. Results: On day 1 of the investigation, 6 of 18 neonates were identified as positive for RSV. The initial 12 negative neonates received a prophylactic dose of palivizumab. Due to the increase in positive neonates, enhanced infection prevention and control measures were immediately implemented. These measures included the immediate closure of the NICU for new transfers, placing all positive neonates in a single-bay cohort in the NICU, implementing contact and droplet precautions, minimizing shared staff, increasing environmental cleaning, and using dedicated equipment. With awareness of the increased community occurrence of RSV, additional measures were taken to monitor adherence to infection prevention and control measures by staff and visitors entering the NICU, including daily symptom screening. Visitation was restricted to block scheduling to monitor the number of individuals in the NICU. Once we obtained the complete conversion of the initial neonate cohort, the additional focus shifted to maintaining the enhanced precautions until all neonate laboratory tests were negative. The NICU was successfully reopened once the remaining 3 positive neonates received no growth on their viral culture. Conclusions: The quick and effective response from a multidisciplinary team allowed a successful intervention to mitigate the identified outbreak. This investigation highlights the importance of enhanced infection prevention and control practices during increased community spread. Future efforts focus on educating staff and visitors on appropriate measures to decrease transmission risks.
Disclosures: None
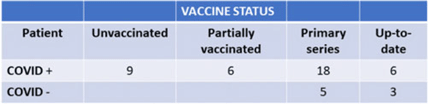
Background: We describe the management of a major COVID-19 outbreak in January 2022 during the SARS-CoV-2 omicron-variant winter surge involving the only inpatient psychiatric facility of Santa Clara County, California, which serves a population of 1.9 million. Methods: On January 14, 2022, infection prevention staff were notified of a symptomatic COVID-19 case in our locked inpatient psychiatric unit who had been admitted since October 2021. The index patient had no visitors or transfers outside the unit. The patients in this unit were noncompliant with masking and mingled with each other during meals. Initial testing identified 23 positive cases among 47 patients and 12 staff cases. Mitigating actions included closing the unit to new admissions, creating alternate care areas in the emergency psychiatric unit, and separating patients into “exposed but negative” and “infected” cohorts and housing them in “red,” and “yellow” zones, respectively. A “green” zone was created by clearance of positive cases. For the cohort exposed to COVID-19, masking was enforced by supervision, dining was scheduled in batches, and daily symptom screening and antigen testing were performed in addition to standard postexposure RT-PCR testing on day 4 and day 7. Mandatory N95 respirators and eye protection were implemented for staff on unit entry. Exposed staff followed employee health protocols for postexposure testing. Enhanced environmental control measures included terminal cleaning and UV-C disinfection of common areas and patient rooms and a thorough investigation of airflow. Discharged patients were contacted if they were residing in congregate facilities. Results: Of 47 patients, 39 (83%) tested positive for COVID-19. However, 8 patients remained negative; all 8 had received at least their primary vaccine series (Table 1). In total, 16 HCWs were SARS-CoV-2 positive in this outbreak. The outbreak officially ended 25 days after the first case. All SARS-CoV-2–positive patients had mild illness, not requiring treatment or hospitalization. We identified vaccine immune escape, staff presenteeism, patient noncompliance with masking, and comingling as major causes of transmission. We determined through contact tracing and temporality that the outbreak likely started from a positive staff member or visitor because most patients had been long-term residents. Conclusions: This outbreak was challenging due to the specialized behavioral needs of the involved patients. It was imperative to reopen this unit quickly and safely to provide psychiatric care to our county’s most vulnerable patients. Ongoing PPE education, repeated reinforcement, engagement in staff wellness to combat pandemic fatigue, and aggressive vaccination are all crucial to minimizing the impact of future outbreaks.
Disclosures: None
