

No CrossRef data available.
Article contents
Impact of different COVID-19 encounter definitions on antibiotic prescribing rates in urgent care
Published online by Cambridge University Press: 16 May 2022
Abstract
Core share and HTML view are not available for this content. However, as you have access to this content, a full PDF is available via the ‘Save PDF’ action button.
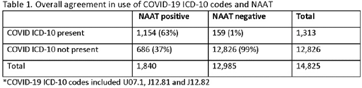
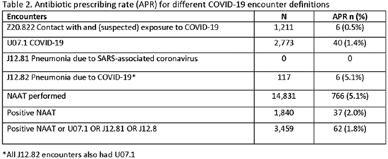
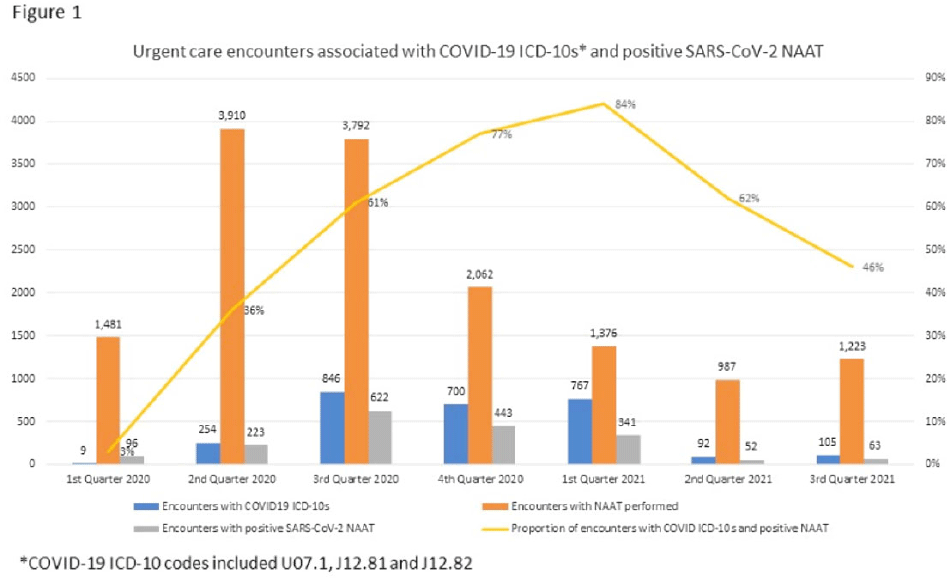
Background: Billing data have been used in the outpatient setting to identify targets for antimicrobial stewardship. However, COVID-19 ICD-10 codes are new, and the validity of using COVID-19 ICD-10 codes to accurately identify COVID-19 encounters is unknown. We investigated COVID-19 ICD-10 utilization in our urgent care clinics during the pandemic and the impact of using different COVID-19 encounter definitions on antibiotic prescribing rates (APRs). Methods: We included all telemedicine and office visits at 2 academic urgent-care clinics from January 2020 to September 2021. We extracted ICD-10 encounter codes and testing data from the electronic medical record. We compared encounters for which COVID-19 ICD-10 codes were present with encounters for which SARS-CoV-2 nucleic acid amplification testing (NAAT) was performed within 5 days of and up to 2 days after the encounter (Fig. 1). We calculated the sensitivity of the use of COVID-19 ICD-10 codes against a positive NAAT. We calculated the APR as the proportion of encounters in which an antibacterial drug was prescribed. This quality improvement project was deemed non–human-subjects research by the Stanford Panel on Human Subjects in Medical Research.
Funding: None
Disclosures: None
- Type
- Antibiotic Stewardship
- Information
- Antimicrobial Stewardship & Healthcare Epidemiology , Volume 2 , Issue S1: SHEA Spring 2022 Abstracts , July 2022 , pp. s5
- Creative Commons

 This is an Open Access article, distributed under the terms of the Creative Commons Attribution licence (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted re-use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution licence (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted re-use, distribution, and reproduction in any medium, provided the original work is properly cited.- Copyright
- © The Author(s), 2022. Published by Cambridge University Press on behalf of The Society for Healthcare Epidemiology of America
 You have
Access
You have
Access
 Open access
Open access