



Introduction
Long-term care (LTC) is crucial to the wellbeing of older people. It refers to the activities undertaken by care-givers which help to compensate for care recipients' loss of functional capability and enable them to live a comfortable life with dignity consistent with their human rights (World Health Organization (WHO), 2015). In response to population ageing and the mounting demand for LTC, most high-income economies have established an independent and comprehensive LTC system where trained staff (formal care) and informal care-givers (including family members, friends, volunteers or neighbours) work together to meet older people's care needs (Ikegami and Campbell, Reference Ikegami and Campbell2002).
Access to affordable LTC is a key principle of the European Pillar of Social Rights (European Commission, 2017). Ideally, LTC resources are provided to those who need them regardless of care recipients' financial capacity and affordability. This underlies the principle of horizontal equity, namely equal care for equal needs. In reality, care distribution may deviate from this ideal for various reasons. Older people without adequate support experience unmet care needs, which in the long run have a wide range of negative consequences, such as an accelerated decline in functional limitation, mental health problems and a higher mortality rate (He et al., Reference He, Craig, Xu, Covinsky, Stallard, Thomas, Hass and Sands2015; Stein et al., Reference Stein, Pabst, Weyerer, Werle, Maier, Heilmann, Scherer, Stark, Kaduszkiewicz and Wiese2016; Hu and Li, Reference Hu and Li2020). It is therefore important to understand the extent and drivers of care inequality so that policies can respond effectively to any distributive injustice in the LTC system.
Unlike health care, long-term formal care in the United Kingdom (UK) is not free of charge at the point of use. Financial support from the government is only available to people with eligible care needs. Formal care is predominantly provided by independent-sector providers, and there is a market where care can be purchased from a large number of care providers. For community-based care services, local authorities may purchase care from care providers on behalf of users, or users may employ a personal assistant or purchase care through a direct payment.
Eligibility for government support is further subject to a financial assessment. The ‘means test’ takes account of both income and savings. People with savings above an upper capital limit (currently £23,250) are not eligible for publicly funded care. While savings below a lower capital limit (currently £12,250) are ignored, savings between the upper and lower capital limits are considered on a sliding scale (Hancock et al., Reference Hancock, Pujol, Morciano, Wittenberg, Hu, King, Adams, Curry, Luheshi and Pike2019). The government recently announced the introduction of a lifetime £86,000 cap on liability to meet care costs and an increase in the lower and upper capital limits in the means test to £20,000 and £100,000, respectively. These reforms will be implemented in October 2023 (HM Government, 2021). In the current LTC system, affordability can be a major barrier to care access, raising concern about socioeconomic inequality in care utilisation.
Older people with dementia are among the most intensive users of LTC. Wittenberg et al. (Reference Wittenberg, Hu, Jagger, Kingston, Knapp, Comas-Herrera, King, Rehill and Banerjee2020) projected that the annual costs of LTC for older people with dementia will rise by 170 per cent, from £14.5 billion in 2020 to £39.2 billion in 2040 at constant prices. This will outpace the projected rise of 106 per cent in the LTC costs for the older population in general (Hu et al., Reference Hu, Hancock and Wittenberg2020a). Older people with dementia have a higher level of care needs (Østbye et al., Reference Østbye, Tyas, McDonwell and Koval1997; Giebel et al., Reference Giebel, Sutcliffe and Challis2015) and a lower socioeconomic status than those without dementia (Cha et al., Reference Cha, Farina and Hayward2021). This means that people with dementia have limited financial resources to meet their needs through privately funded care and may be especially vulnerable to unequal distribution of LTC. Therefore, it is important that the existing system provides sufficient support to people with dementia and protects them from heightened care inequalities. Reducing inequalities in dementia care is a key priority of the WHO Global Action Plan on the public health response to dementia (WHO, 2017). However, very little is known about the socioeconomic inequalities of LTC for older people with dementia.
This study investigates the distribution of LTC resources in community-dwelling older people with and without dementia in England. The focus is upon how the distribution of care varies according to people's socioeconomic status. Nested within the DETERMIND (DETERMinants of quality of life, care and costs, and consequences of INequalities in people with Dementia and their carers) programme (Farina et al., Reference Farina, Hicks, Baxter, Birks, Brayne, Dangoor, Dixon, Harris, Hu and Knapp2020), it calculates the concentration index and inequity index to gauge the magnitude of socioeconomic inequality and inequality of LTC, respectively.
Literature review
The literature makes a conceptual distinction between socioeconomic inequality and inequity in care utilisation. To investigate socioeconomic inequality, studies have mapped out the distribution of care according to a particular socioeconomic indicator such as income or wealth in the population. In comparison, socioeconomic inequity in care utilisation focuses on socioeconomic inequality for people with a similar level of care needs. Investigation into socioeconomic inequity involves classifying the drivers of care utilisation into need and non-need factors and controlling for the impacts of need factors on care utilisation (for details, see the Methods section).
While there is a well-established body of literature on socioeconomic inequality and inequity in health-care utilisation (Allin et al., Reference Allin, Masseria and Mossialos2011; Pulok et al., Reference Pulok, van Gool, Hajizadeh, Allin and Hall2020), the evidence base for LTC is much smaller. Analyses of socioeconomic inequality and inequity of LTC have been conducted in a limited number of countries. García-Gómez et al. (Reference García-Gómez, Hernández-Quevedo, Jiménez-Rubio and Oliva-Moreno2015) found that both formal and informal care were more concentrated among poorer people in Spain. After care needs were controlled for, however, formal care was more concentrated among people with higher income, while intensive informal care was more concentrated among those with lower income. Tenand et al. (Reference Tenand, Bakx and van Doorslaer2020) reported that the distribution of formal home care and institutional care in the Netherlands was significantly in favour of poorer people, with this pattern of care distribution remaining after care needs were controlled for. Wang et al. (Reference Wang, Yang and Chen2022) focused on the socioeconomic inequality of LTC for older people in China where the availability of formal care is much more limited than that in high-income countries. They found that the distribution of home-based care favoured the poor and that of institutional care favoured the rich.
Unmet LTC needs refer to the situation where care is needed but is either non-existent or insufficient (Williams et al., Reference Williams, Lyons and Rowland1997). This concept enables researchers to look at care utilisation from an alternative angle. Absolute unmet needs are defined as having a care need but not receiving any help at all, whereas relative unmet needs are defined as the situation where care users are not satisfied with the help or need more help (Vlachantoni, Reference Vlachantoni2019). García-Gómez et al. (Reference García-Gómez, Hernández-Quevedo, Jiménez-Rubio and Oliva-Moreno2015) found that absolute unmet needs in Spain are more concentrated among people with a lower level of income. Studies in the United States of America (USA) show that a lower income was associated with a higher level of unmet needs in people with dementia (Black et al., Reference Black, Johnston, Rabins, Morrison, Lyketsos and Samus2013, Reference Black, Johnston, Leoutsakos, Reuland, Kelly, Amjad, Davis, Willink, Sloan and Lyketsos2019).
There is an ongoing debate in the inequity analysis community about the best approach to executing the classification between need and non-need factors, as there is no single, agreed-upon definition of care needs. In the health economics literature, age and gender are often treated as need factors (O'Donnell et al., Reference O'Donnell, van Doorslaer, Wagstaff and Lindelow2008), whereas the behavioural model of care utilisation classifies them as predisposing factors that affect care utilisation prior to the onset of care needs (Anderson and Newman, Reference Anderson and Newman2005). This often results in debatable conclusions about socioeconomic inequity in care utilisation. An equitable distribution of care resources in the context of one conceptual framework is not necessarily considered equitable in another. Ilinca et al. (Reference Ilinca, Rodrigues and Schmidt2017) have demonstrated that the results in European countries are sensitive to the treatment of the living arrangement variable (i.e. who older people live with in the same household); treating it as a need factor led to a higher level of pro-rich inequity in the use of formal home care than otherwise.
Some studies have focused on cross-national comparisons of socioeconomic inequality of care utilisation. Rodrigues et al. (Reference Rodrigues, Ilinca and Schmidt2018) analysed socioeconomic inequity in 14 European countries. They found that the distribution of informal care and home care was pro-poor. After adjusting for care needs, the distribution of home care was pro-poor in Denmark and Estonia but pro-rich in Spain and Italy. Carrieri et al. (Reference Carrieri, Di Novi and Orso2017) clustered European countries into three regions: Northern Europe, Continental Europe and Southern Europe. This clustering is motivated by the widely used classification of welfare states into social democratic (Northern Europe), conservative (Continental Europe) and Mediterranean (Southern Europe) welfare-state regimes where the state, family and market play different roles in welfare provision (Esping-Andersen, Reference Esping-Andersen1989, Reference Esping-Andersen2000; Ferrera, Reference Ferrera1996). They found that while inequity in paid domestic help and home-based nursing care favours the rich in Southern and Continental Europe, countries in Northern Europe do not demonstrate significant care inequity. These differences are broadly consistent with the clustering of welfare states where the social democratic regime is characterised by more state involvement in welfare provision and correspondingly more progress in the reduction of inequity than in the other regimes (Aspalter, Reference Aspalter and Aspalter2017). So far, little attention has been devoted to LTC inequality and inequity in liberal welfare-state regimes, such as the USA and the UK.
Socioeconomic inequality and inequity in LTC are a highly country-specific issue. The existing LTC policies in different countries vary markedly in terms of the sources of funding for care (tax or national insurance), eligibility criteria for public support (means-testing or universal entitlement) and the types of support available to informal care-givers. All of these factors affect how care resources are distributed in the older population (Ikegami and Campbell, Reference Ikegami and Campbell2002). Furthermore, all existing studies have focused on the general older population, so there is little comparable evidence on people with dementia. In the English context, the means-tested system is intended to make the distribution of care more equitable. However, whether such a system is generous enough to guarantee care equity is an empirical question that we aim to answer in this study. People with dementia have a higher level of care needs and a lower socioeconomic status than those without dementia (Østbye et al., Reference Østbye, Tyas, McDonwell and Koval1997; Giebel et al., Reference Giebel, Sutcliffe and Challis2015; Cha et al., Reference Cha, Farina and Hayward2021). If the means-tested system is highly restrictive so that many people have no access to government support, it is expected that, for people with a similar level of care needs, the distribution of formal care will be in favour of richer people and that poorer people either rely more on informal care or are more likely to have unmet care needs.
Research methods
Data
The data for this study come from the English Longitudinal Study of Ageing (ELSA), a national survey that collected ageing and health-related information from a nationally representative sample of individuals aged over 50 in England. The baseline survey of ELSA was conducted in 2002, with the same sample being interviewed every two years. The sample has been regularly refreshed to maintain its representativeness of the older population. We used data from the pooled sample for older people aged 65 and over from Waves 6, 7 and 8 of the survey, conducted in 2012, 2014 and 2016, respectively (N = 17,248). This ensured that we had a sufficiently large sample size of older people with dementia. We did not include respondents in the earlier waves because the questions relating to LTC utilisation in Waves 1–5 were different from those in Waves 6–8. We did not include respondents in care homes because only core members in the first wave of ELSA or in the refreshment samples who later moved into a care home were interviewed. The number of people in this group was small, and they did not represent the population of interest.
Among the 17,248 older people in the pooled sample, 361 people did not report their socioeconomic status (i.e. income or wealth) and 439 people did not report their cognitive functioning status. Our analyses focused on the 16,458 older people aged 65 and over who participated in any of the three waves of the ELSA survey and provided information on both cognitive functioning status and socioeconomic characteristics. The same respondents may be included in multiple waves. A total of 4 per cent (N = 656) of the interviews were conducted by proxies. Following the method of Davies et al. (Reference Davies, Cadar, Herbert, Orrell and Steptoe2017), we identified 412 older people who had dementia. This group includes: (a) interviewees or informants who reported a diagnosis of dementia by a physician and (b) interviewees who were rated to have a score higher than 3.5 in the short-form Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE). A systematic review conducted by Quinn et al. (Reference Quinn, Fearon, Noel-Storr, Young, McShane and Stott2014) shows that using the cut-off point of 3.5 in the IOCODE has high sensitivity (0.82) and specificity (0.84) to identify cases of dementia. Among the 412 people with dementia, 39 per cent of the interviews (N = 160) were conducted by proxies.
Measurements
Care utilisation is the focus of analysis in this study. Following García-Gómez et al. (Reference García-Gómez, Hernández-Quevedo, Jiménez-Rubio and Oliva-Moreno2015), we investigated three variables relating to care utilisation: receipt of informal care, receipt of formal care and number of unmet needs. The respondents were asked whether or not they had difficulties in performing six activities of daily living (ADLs; dressing, walking across the room, bathing, eating, getting in and out of bed, using the toilet), four instrumental activities of daily living (IADLs; shopping, taking medications, working around the house and managing money) and three mobility tasks (walking 100 yards, climbing several flights of stairs without rest and climbing one flight of stairs without rest). To ensure that the difficulties in performing these tasks related to LTC needs, the ELSA questionnaire emphasised to survey participants that they should only answer affirmatively if the issues arose because of physical, mental, emotional or memory problems and were expected to last more than three months.
Survey participants were further asked whether they received help to perform the aforementioned activities and, if so, who helped them. The ELSA questionnaire defined help from a spouse, adult children, relatives, neighbours or friends as informal care and help from a home care worker, personal assistant, member of a reablement/immediate care team, shelter housing manager, council handyman or cleaner as formal care. We followed the same definitions in this study. We created two variables to indicate whether people received informal care and formal care, respectively. They were both dichotomised (0 = no, 1 = yes).
We created two unmet LTC needs variables, the first including all measured needs and the second focusing on ADLs only. If a person reported difficulties in performing any of the ADL, IADL or mobility activities, but did not receive formal or informal care for this activity, we treated it as a case of an unmet need. For people who reported difficulties in performing those activities, we created a count variable by adding up the number of unmet needs. This variable had a value ranging from 0 (no unmet needs) to 13 (needs not met at all). Our second unmet needs variable focused on older people who reported difficulties in ADL activities but did not receive any help. The value of this variable ranged from 0 (no unmet ADL care needs) to 6 (ADL care needs not met at all). It can be noted that both variables capture absolute unmet LTC needs.
Regarding determinants of care utilisation, a distinction was made between need and non-need factors. Following García-Gómez et al. (Reference García-Gómez, Hernández-Quevedo, Jiménez-Rubio and Oliva-Moreno2015) and Rodrigues et al. (Reference Rodrigues, Ilinca and Schmidt2018), we included age, gender, functional capability, depressive symptoms, self-reported health and long-term illness as need factors. Functional capability was measured by the number of difficulties in performing ADL, IADL and mobility tasks. A higher number of difficulties indicates more severe functional limitations or lower functional capability. Such a measurement was created based on theories that functional capability has a single latent dimension and the loss of ability to perform daily activities follows a hierarchical sequence (Spector and Fleishman, Reference Spector and Fleishman1998; Kingston et al., Reference Kingston, Collerton, Davies, Bond, Robinson and Jagger2012).
Depressive symptoms were measured by the eight-item Center for Epidemiologic Studies Depression Scale (CES-D). Interviewees were asked to evaluate six negative statements about their feelings in the past week (e.g. I felt depressed) and two positive statements (e.g. I enjoyed life). A variable was coded as 1 if an interviewee reported ‘yes’ to a negative statement and 0 otherwise. The positive statements were reverse coded. Adding up the scores of these variables, we created a variable which has a value ranging from 0 (no depressive symptoms) to 8 (severe depressive symptoms). Interviewees were asked to evaluate their own health on a five-point Likert scale: excellent, very good, good, fair or poor. We combined them into three categories: 0 = excellent, very good or good, 1 = fair, 2 = poor. Interviewees were asked whether they had any long-term illness, disability or infirmity. Based on the answer to this question, we created a dichotomised variable (0 = no, 1 = yes).
For the non-need variables, we investigated marital status, living with children in the same household, level of education, equivalised income and total net wealth. The marital status variable has two categories: 0 = never married, widowed, separated or divorced and 1 = married or co-habiting with a partner. The co-residence variable indicated whether an older person was living with his or her children in the same household (0 = no, 1 = yes). The education variable has three categories: no educational qualifications, primary or secondary education and higher education.
Income and wealth were both continuous variables which came from the ELSA dataset of financial-derived variables. We used the equivalised income which accounts for the size and composition of a household and thus better reflects an individual's living standards and costs than individual income (Barr, Reference Barr2004). The variable in the ELSA dataset used an Organisation for Economic Co-operation and Development equivalence scale which assigned a weight of 0.5 to second adults and dependent children aged 14 and over and a weight of 0.3 to children under 14 years of age (Institute for Fiscal Studies, 2011). The wealth variable measures total non-pension wealth. This variable included net financial wealth, net physical wealth and housing wealth. We logarithmically transformed these two variables prior to the data analyses so that they both had an approximately normal distribution. For people with zero income or wealth, we recoded their income or wealth as £1 so that those observations could be retained in the process of logarithmic transformation. A small number of observations with negative income (N = 6) or wealth (N = 351) were dropped in the transformation process.
All of the need and non-need factors in the dataset had less than 1 per cent missing values, except for the CES-D scores (missingness = 7%), self-reported health (4%) and education (2%). Multiple imputation was used to impute the missing values in those three variables. All of the other variables in our dataset were used as predictors to make the imputation. The three variables were imputed by chained equations (Stata syntax: mi impute chained).
Data analysis
We calculated the concentration index (CI) to measure the socioeconomic inequality of care utilisation in the ELSA sample. We used equivalised individual income and total (non-pension) wealth as two separate socioeconomic indicators. There were different ways to calculate the CI. Our starting point was the convenience formula of CI, which can be expressed as follows:

where $\bar{h}$ is the mean of care utilisation across all people in the sample, h i denotes care utilisation of person i, r i is the person's rank in the distribution of the socioeconomic indicator and cov(.) denotes the co-variance of h i and r i. All three care utilisation variables in our study are bounded variables. In this case, the corrected concentration index (CCI) is more commonly used (Erreygers, Reference Erreygers2009) and can be calculated as follows:
is the mean of care utilisation across all people in the sample, h i denotes care utilisation of person i, r i is the person's rank in the distribution of the socioeconomic indicator and cov(.) denotes the co-variance of h i and r i. All three care utilisation variables in our study are bounded variables. In this case, the corrected concentration index (CCI) is more commonly used (Erreygers, Reference Erreygers2009) and can be calculated as follows:

The value of the CCI ranges between −1 and 1. A positive value indicates that the distribution of LTC resources is more concentrated among the better-off, whereas a negative value means that care resources are distributed in favour of poorer people. A higher absolute value indicates a more pro-rich or pro-poor distribution of care resources. Equality is achieved when the CCI equals zero. It should be noted that the CI calculated in our study provides a measure of the relative differences in care utilisation between different income or wealth groups. It stands in contrast to measures of absolute inequality which quantify the absolute differences between different socioeconomic groups.
Socioeconomic inequity in care utilisation, also known as horizontal inequity (HI), is a measure of socioeconomic inequality which accounts for the contributions of need factors to care utilisation. If care utilisation is assumed to be a linear and additively separable function of the need and non-need factors, the relationships between these variables can be estimated by the following regression model:

where x k and z p denote the need and non-need factors, respectively, and β and γ are their respective coefficients. ɛ i is the error term. Using the regression coefficients from Equation 3 as the input, Wagstaff et al. (Reference Wagstaff, van Doorslaer and Watanabe2003) showed that the CI in Equation 1 can be decomposed into the weighted sum of the CIs for the need and non-need factors:

where $\overline {x_k}$ and $\overline {z_p}$
and $\overline {z_p}$ denote the mean of the need and non-need factors, respectively, and CIk and CIp denote the CI for these variables. $GC_\varepsilon$
denote the mean of the need and non-need factors, respectively, and CIk and CIp denote the CI for these variables. $GC_\varepsilon$ is the generalised CI for the error term. Combining Equations 2 and 4, we have:
is the generalised CI for the error term. Combining Equations 2 and 4, we have:

Then the HI can be calculated by subtracting the contributions of the need factors from the CCI:

A positive (negative) value of HI indicates a pro-rich (pro-poor) distribution of care resources standardised by care needs. The standard errors of CIs and HIs were calculated using the bootstrap method with 1,000 repetitions of re-sampling. The principle of horizontal equity assumes that vertical equity, namely unequal treatment for unequal needs, is justifiable (O'Donnell et al., Reference O'Donnell, van Doorslaer, Wagstaff and Lindelow2008). Such an assumption does not hold for unmet needs. No government policies or interventions would aim to achieve graded unmet needs for people with varied needs. We could split the CI of unmet needs into the contributions of need and non-need factors, but there is no conceptual basis to interpret the contribution of non-need factors as HI (García-Gómez et al., Reference García-Gómez, Hernández-Quevedo, Jiménez-Rubio and Oliva-Moreno2015).
Results
Table 1 shows the sample characteristics of older people with and without dementia. The final column of the table reports the test of association between the sample characteristics and the dementia variable. The two groups of people differ significantly in regard to a multitude of characteristics. Seventy per cent of the older people with dementia were recipients of informal care and 32 per cent were recipients of formal care. In contrast, 18 per cent of people without dementia received informal care and 7 per cent received formal care. However, the two groups of people did not differ significantly in terms of the number of unmet needs. Compared to people without dementia, those with dementia were older, had more severe functional limitations and poorer health, and were more likely to have other long-term illness. People with dementia had a lower level of education, income and wealth than those without dementia.
Table 1. Sample characteristics of older people with and without dementia

Note: χ2 refers to the Pearson's chi-square test and ρ refers to the Spearman's rank-order correlation coefficient.
Significance level: *** p < 0.001.
Table 2 shows the income-based inequality and inequity in LTC utilisation among older people with dementia (second column). The CCI of informal care is negative but not statistically significant (p = 0.617), indicating that the distribution of informal care among older people with dementia was approximately equal. The CCIs of formal care and unmet needs are significantly negative (p < 0.05), meaning that they were more concentrated among people with lower income. Such a pattern of care distribution can be visualised using the concentration curve (Figure 1). The concentration curve of informal care sticks very close to the 45° line of equality (upper left panel), whereas that of formal care (upper right panel) and unmet needs (lower left panel) lies above the equality line. For people in the lowest income quintile, their probability of receiving formal care was on average 0.38, which stands in contrast to those in the highest income quintile, whose probability of receiving formal care was 0.24. People in the lowest income quintile had on average 2.2 unmet needs, whereas those in the highest quintile had 1.8 unmet needs. Regarding informal care recipients, people in the middle quintile had the highest probability of care utilisation (lower right panel).

Figure 1. Concentration curve and predicted probability of care utilisation among older people with dementia.
Table 2. Income-based concentration index and decomposition by need and non-need factors

Notes: Bootstrapped standard errors are in parentheses. CCI: corrected concentration index. HI: horizontal inequity.
Significance levels: * p < 0.05, ** p < 0.01, *** p < 0.001.
We split the CCI for people into the contributions of the need and non-need factors. According to Equation 5, the contribution of a factor to care inequality depends upon (a) the relationship between this factor and the care utilisation, and (b) the CI of this factor. Considering the utilisation of informal care for older people with dementia, there is a significantly positive association between the number of functional limitations and the receipt of informal care (coefficient = 0.226, p < 0.001; Table S1 in the online supplementary material), which means that those with a higher level of care needs are more likely to receive informal care. Meanwhile, the CI of functional limitations is significantly negative (CI = −0.057, p < 0.001), which means that functional limitations are more concentrated among poorer older people with dementia. The contribution of the functional limitation variable then equals −0.057 × 0.226 × 5.6 × 4 = −0.29 (p < 0.001; Table S2 in the online supplementary material), which indicates a pro-poor contribution to socioeconomic inequality in the utilisation of informal care. For the purposes of readability and interpretability, Table 2 only reports the aggregate contributions of the two broader categories of need and non-need factors. The detailed breakdown regarding each factor in these two broader categories can be found in the online supplementary material. It is important to note that people with dementia are a relatively small group in the whole older population, so the standard errors of CCI and HI tend to be larger. The effect size of CCI and HI is equally important information, and their statistical significance should be interpreted with caution.
Among older people with dementia, the contribution of need factors to the CCI was negative for all three care utilisation variables, which represents a pro-poor contribution to socioeconomic inequality (second column of Table 2). For informal care, the pro-poor contribution of need factors and the pro-rich contribution of non-need factors offset each other, which resulted in a small and statistically insignificant CCI. For formal care and unmet needs, the contribution of non-need factors was negative and thus pro-poor. Overall, 66 per cent (i.e. −0.076/−0.116) of the pro-poor inequality in the utilisation of formal care was attributable to need factors, while the remainder (34%) was contributed by non-need factors. The contribution of need factors to the pro-poor inequality of unmet needs was 10 per cent (i.e. −0.005/−0.048), and that of non-need factors was 90 per cent.
The third and fourth columns of Table 2 show the income-based inequality in care utilisation among people without dementia and the two groups of people combined together. For people without dementia, the distribution of informal care was significantly in favour of people with lower income. As with people with dementia, this reflected a higher level of care needs amongst people with lower income. The pro-poor distribution of informal care is illustrated in Figure 2 where the concentration curve for informal care lies above the equality line (upper left panel). Older people in the lowest income quintile had a probability of 0.21 of using informal care, while the probability for those in the highest income quintile was reduced to 0.10 (lower right panel of Figure 2). The contribution of non-need factors to the CI, namely HI, was small and statistically insignificant (HI = 0.008, p = 0.146).
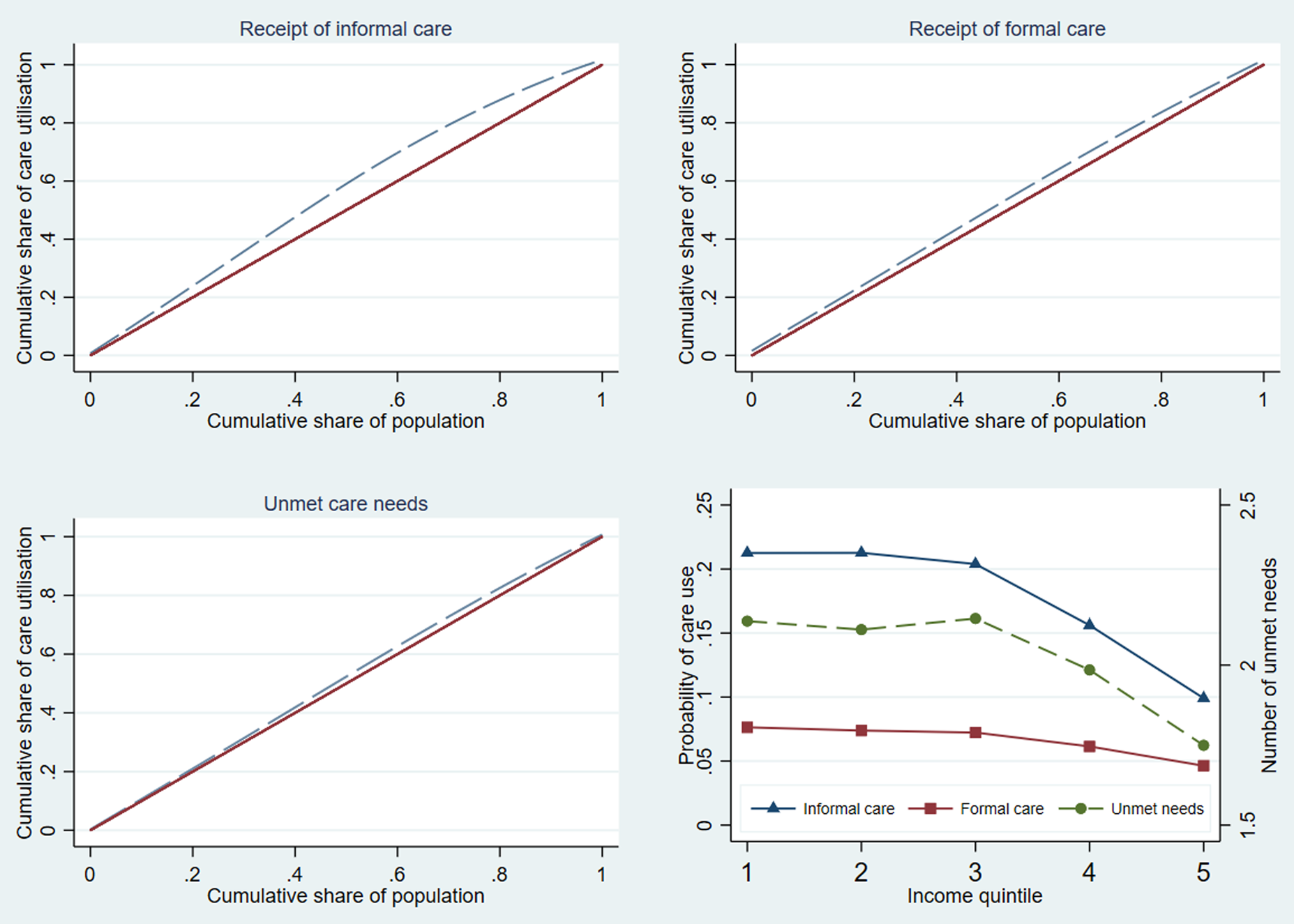
Figure 2. Concentration curve and predicted probability of care utilisation among older people without dementia.
The distribution of formal care for older people without dementia was also in favour of those with lower income (CCI = −0.017, p < 0.001), but less so than for people with dementia. The probability of using formal care decreased from 0.08 to 0.05 between older people in the lowest and higher income quintiles (lower right panel of Figure 2). The HI index of formal care was positive and statistically significant (HI = 0.026, p < 0.001). This means that for older people with similar care needs, formal care was more concentrated among people with higher income. The distribution of unmet needs was significantly more concentrated among those with a lower level of income (CCI = −0.24, p < 0.001). Older people in the lowest income quintile on average had 2.1 unmet needs, in contrast to 1.7 unmet needs among those in the highest income quintile (lower right panel of Figure 2). The contributions of the need factors and non-need factors to the pro-poor distribution of unmet needs were 46 and 54 per cent, respectively.
Table 3 shows the wealth-based inequality and inequity of LTC utilisation. We found a similar pattern of care distribution when wealth was used as the socioeconomic indicator. There was a pro-poor distribution in the utilisation of informal and formal care. Unmet care needs were also more concentrated among people with a lower level of wealth. Wealth-based inequity in the utilisation of formal care was significantly pro-poor among older people (HI = −0.13, p < 0.001) with dementia but significantly pro-rich among those without dementia (HI = 0.023, p < 0.001).
Table 3. Wealth-based concentration index and decomposition by need and non-need factors

Notes: Bootstrapped standard errors are in parentheses. CCI: corrected concentration index. HI: horizontal inequity.
Significance levels: * p < 0.05, ** p < 0.01, *** p < 0.001.
Table 4 shows the results of socioeconomic inequality of unmet ADL care needs. In this analysis, we focused on older people with difficulties in performing ADL tasks. The pro-poor distribution of unmet needs remains strong, even though the magnitude of inequality seems to be lower in comparison to results in Tables 2 and 3 where we focused on older people with difficulties in performing ADL, IADL and mobility tasks. When income was used as the socioeconomic indicator, unmet ADL care needs were more concentrated in poor people without dementia (CI = −0.018, p < 0.01). When wealth was used as the socioeconomic indicator, unmet ADL care needs were more concentrated in poor people with dementia (CI = −0.054, p < 0.05).
Table 4. Concentration index of unmet activities of daily living care needs

Notes: Bootstrapped standard errors are in parentheses. CCI: corrected concentration index.
Significance levels: * p < 0.05, ** p < 0.01, *** p < 0.001.
Discussion
Using equivalised income and wealth as two separate socioeconomic indicators, this paper investigated socioeconomic inequality and inequity in the utilisation of LTC for older people with and without dementia in England. Previous studies have shown that the provision of health care in the UK is largely equitable, thanks to a universal health system where the majority of services are free of charge at the point of use (Allin et al., Reference Allin, Masseria and Mossialos2011). This is not the case for LTC. Wittenberg et al. (Reference Wittenberg, Hu and Hancock2018) estimated that one-third of older home care recipients are self-funded, raising concerns about the affordability and adequacy of care in the older population. These issues are even more acute in the case of people with dementia because they have a higher level of care needs and a lower socioeconomic status than those without dementia, as demonstrated in Table 1. The distribution of informal care in the older population is strongly pro-poor. Socioeconomic stratification of care needs plays a dominant role: older people with lower income or wealth have more care needs, which in turn drives the utilisation of care. These results are consistent with findings reported in other European countries (García-Gómez et al., Reference García-Gómez, Hernández-Quevedo, Jiménez-Rubio and Oliva-Moreno2015; Carrieri et al., Reference Carrieri, Di Novi and Orso2017; Ilinca et al., Reference Ilinca, Rodrigues and Schmidt2017; Rodrigues et al., Reference Rodrigues, Ilinca and Schmidt2018; Tenand et al., Reference Tenand, Bakx and van Doorslaer2020).
The distribution of formal care is also pro-poor. Apart from the income-based stratification of care needs, another contributing factor is the availability of government support. In England, older people with eligible care needs and lower financial means are entitled to in-kind services funded by the government or cash-for-care benefits (Comas-Herrera et al., Reference Comas-Herrera, Wittenberg and Pickard2010; Rodrigues and Glendinning, Reference Rodrigues and Glendinning2015). This helps people with substantial care needs to access formal care even though they may lack the financial capacity to purchase it for themselves on the private market. The evidence reported in our study suggests that the pro-poor distribution of formal care is a pattern shared by older people with and without dementia.
However, the inequity of formal care presents a different picture. Existing studies show varied results across countries, with the need-standardised distribution of formal care ranging from being in favour of richer people, being in favour of poorer people, to being mostly equitable (Rodrigues et al., Reference Rodrigues, Ilinca and Schmidt2018). Our findings suggest that such heterogeneity not only exists across countries but can also exist across different groups of older people. On the one hand, we did not find evidence of significant income-based inequity among older people with dementia, and the inequity of formal care was found to be pro-poor when wealth was used as the socioeconomic indicator. People with dementia tend to have less financial means than those in the general older population and arguably need more government support as a group. It appears that the current means-testing system in England recognises older people with dementia as a vulnerable group and plays a meaningful role in compensating for their financial disadvantages and promoting equitable utilisation of formal care.
On the other hand, we have found a significant pro-rich inequity in formal care utilisation among older people without dementia or older people as a whole. This implies that people without dementia are qualitatively different from those with dementia in terms of care needs and socioeconomic status such that the equitable distribution of formal care cannot be guaranteed by the existing means-testing rules. The pattern of LTC inequality and inequity in England resembles that in Italy and Spain where government support for LTC is also based on means tests. Carrieri et al. (Reference Carrieri, Di Novi and Orso2017) observed that the level of government support is positively correlated with equitable access to formal care. Compared with the LTC systems with universal benefits or more generous entitlements, a means-testing system has the advantage of targeting services at older people who need them and containing care costs. However, when the entitlement to government support is over-restrictive or eligible care needs are narrowly defined, such a system can give rise to an unfair distribution of formal care in favour of the rich, as evidenced in our study. In developing countries, it is common that care needs of older people are predominantly met by family care-givers. However, against the backdrop of global population ageing, recent years have seen some countries devoting more public resources to expanding the capacity of formal care and ramping up financial support for care recipients (Hu et al., Reference Hu, Li, Wang and Shi2020b). Our study suggests that, in the course of designing and reforming the LTC system, it is important that the governments carefully consider the implications for care equity regarding different models of LTC financing.
A pro-poor distribution of care does not mean that the care needs of poorer people are fully met. Indeed, we have found that unmet needs for LTC are more concentrated among poorer people, both for those with and without dementia. As pointed out above, people with lower income tend also to have more care needs. Meanwhile, there is a positive correlation between the number of care needs and the number of unmet needs. In our sample, older people who had difficulties in performing fewer than five daily tasks had on average 1.6 unmet needs, whereas those experiencing difficulties in more than five tasks had on average 3.8 unmet needs. As the level (or number) of care needs increases, it is more difficult for existing care resources to meet them fully. Care resources are stretched thin among older people with substantial care needs, which results in a disproportionate concentration of unmet needs among the poor. This once again points to the inadequacy of government support for the financially disadvantaged older people.
The concentration of unmet needs among poorer people has profound implications. Older people with unmet needs are reported to experience a range of difficulties in life such as wetting or soiling themselves, going without eating, taking the wrong medication or lacking exercise, all of which pose a threat to their health (Allen et al., Reference Allen, Piette and Mor2014; Hu and Li, Reference Hu and Li2020). This suggests that poorer people are more exposed to unmet needs than their richer peers, which in turn can result in expanded health inequality. Two points are worth mentioning here. First, inadequate care leads to the progression of care needs, which suggests the existence of reverse causality. Second, such a causal pathway has a different timing. Care provision responds to changes in care needs, which have swift consequences for care utilisation and care adequacy. In comparison, the progression of care needs is a developmental process that takes shape over the lifecourse. It is possible that unmet needs do not have a notable effect on health in the short term, but the concern is that sustained exposure to unmet needs and the progression of care needs may reinforce each other in a vicious circle in the long run.
This study has important limitations. First, due to the relatively small number of care recipients who have dementia, we were not able to calculate the socioeconomic inequality and inequity in the intensity of care (i.e. care hours) received by this group of people and compare it with the general older population. This limitation, however, was at least partially mitigated by our analysis of unmet care needs because the number of unmet needs arguably captures the level of care which people needed but was left unfulfilled. Second, the ELSA sample did not include older people living in a care home, where around 70 per cent of residents are estimated to have dementia and where a third of people with dementia reside. The proportion of self-funded care recipients is markedly higher in care homes than in the community (Wittenberg et al., Reference Wittenberg, Hu and Hancock2018). We expect that the pro-rich inequity in the utilisation of formal care is even stronger in care homes. Third, a limitation shared with other studies using the ELSA sample is that the cases of dementia may be underestimated due to the sampling bias in this group of older people (Davies et al., Reference Davies, Cadar, Herbert, Orrell and Steptoe2017). It would be useful to check whether the pattern of care inequality and inequity among older people with dementia in this study can be replicated from analyses of data in other national surveys where dementia is ascertained by different means. Finally, when logarithmically transforming the wealth variable, we dropped 2 per cent of the sample with negative values. It would be useful in future analysis to explore and adopt transformation methods that can retain negative values. The inverse hyperbolic sine transformation approach (Bellemare and Wichman, Reference Bellemare and Wichman2020), which has gained increasing popularity in more recent empirical studies, holds great promise for this purpose.
Conclusions
Driven by the socioeconomic stratification of care needs, the utilisation of LTC in England is strongly pro-poor. There is a largely equitable distribution of informal care for community-dwelling older people and of formal care for older people with dementia. Government support in the formal care sector plays a constructive role in protecting older people with a lower level of income or wealth, and there is no evidence to suggest that older people with dementia are further affected by an unfair distribution of LTC. However, the pro-rich inequity of formal care for people without dementia and the concentration of unmet needs among poorer people with and without dementia is a clear indication that the existing care resources in England remain insufficient for those from a financially disadvantaged background and with substantial and complex care needs. Any countries that have in place a means-tested LTC system or plan to develop such a system may want to consider how to strike a balance between economic efficiency and care equity. Our analyses of care receipt and unmet needs lead to opposing results, which underscores the importance of looking at ‘both sides of the coin’ when the policy goal of a country is to promote distributive fairness in the LTC system. Sufficient support from the government helps to prevent the mutual reinforcement between health and LTC inequality in the older population.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0144686X22000885.
Financial support
This study is part of the DETERMIND project (DETERMinants of quality of life, care and costs, and consequences of INequalities in people with Dementia and their carers), which was supported by the Economic and Social Research Council (UK) and the National Institute for Health Research (UK) (grant number ES/S010351/1).
Conflict of interest
The authors declare no conflicts of interest.
Ethical standards
This study uses secondary data from the English Longitudinal Study of Ageing (ELSA). Ethical approval for ELSA was given by the London Multicentre Research Ethics Committee.









 Open access
Open access