



Introduction
The global labour force will age substantially over the next decades, as governments worldwide are encouraging older adults to stay longer in the labour market, in order to tackle the challenges of demographic transition for the world economy (Poplawski-Ribeiro, Reference Poplawski-Ribeiro2019). Labour force participation is not important only for the economy. One systematic review suggested that later-life paid employment has a positive effect on older adults’ mental health in high-income countries (Maimaris et al., Reference Maimaris, Hogan and Lock2010). One study in Japanese men also reported that older adults who engaged in paid work less than 35 hours per week were able to maintain their physical health (Kajitani, Reference Kajitani2011). For older adults, participating in paid employment in later life could help meet their basic needs and increase opportunities for them to develop social relationships (World Health Organization (WHO), 2015). However, the health and social benefits of working at older age depend on an individual's capacity and the suitable working conditions (International Labour Organization, 2015). Older adults in disadvantaged socio-economic status (SES) are less likely to have high levels of skills and education that provide them with desirable and flexible jobs, and they are less likely to be sufficiently healthy to perform desirable jobs (WHO, 2015). Therefore, the health and social benefits of later-life paid employment are unlikely to be universal due to disparities in labour force participation by individual capacity and SES.
Health and socio-economic determinants of later-life labour force participation
Many studies have investigated the relationship between health and later-life labour force participation. One study in London-based civil servants in the United Kingdom (UK) found that having chronic disease was associated with increased risks of all types of work exit, including ‘retirement’ (reported being retired, not on health grounds), ‘health-related exit’ (reported being long-term sick or retirement on health grounds), ‘unemployment’ (reported being unemployed) and ‘other exit’ (other reasons for work exit), and specifically the health-related work exit (Fleischmann et al., Reference Fleischmann, Carr, Stansfeld, Xue and Head2018). Another UK study also suggested that poor physical and cognitive performance was associated with a lower likelihood of participating in bridge employment after retirement (Stafford et al., Reference Stafford, Cooper, Cadar, Carr, Murray, Richards, Stansfeld, Zaninotto, Head and Kuh2017). One systematic review based on 44 longitudinal studies indicated that poor health (measured by self-perceived health, mental health and chronic diseases) was associated with exiting from paid employment (van Rijn et al., Reference van Rijn, Robroek, Brouwer and Burdorf2014). All these studies were from high-income European countries and the United States of America (USA). Epidemiological evidence on health determinants of later-life labour force participation in other countries is limited.
The socio-economic determinants of later-life labour force participation have also been examined. However, findings vary between studies due to different measures of SES and later-life labour force outcomes. One study in Finland indicated that lower levels of education, occupational position and income were all associated with higher risks of disability retirement (reported receiving any form of disability pension at the end of each year) (Leinonen et al., Reference Leinonen, Martikainen and Lahelma2012). One study in the UK also found that a lower level of household wealth was related to an increased probability of leaving paid employment (McMunn et al., Reference McMunn, Nazroo, Wahrendorf, Breeze and Zaninotto2009). One study based on data of seven longitudinal studies in Finland, France, the UK and the USA suggested that lower levels of education and occupational position were associated with increased risks of health-related work exit (i.e. reported leaving work due to their own health/disability, or receiving a health-related benefit/pension one year before or one year after the date they stopped working) in most studies but any paid work exit (i.e. retirement, health-related exit, unemployment and other exits) only in some of the studies (Carr et al., Reference Carr, Fleischmann, Goldberg, Kuh, Murray, Stafford, Stansfeld, Vahtera, Xue, Zaninotto, Zins and Head2018). One study in the USA suggested that participants with a higher level of net wealth (including lifetime wealth and savings) or pension wealth were less likely to work full-time at age 62; whereas those with a higher level of income would continue working full-time at age 62 (McGarry, Reference McGarry2004). Another study in US men indicated that a higher level of net wealth was associated with an earlier retirement expectation (leave the labour market before normal pension age); however, the effect size of the net wealth was small: per US $100,000 increase in net wealth resulted in only 14 days earlier for retirement (Dwyer and Mitchell, Reference Dwyer and Mitchell1998).
Researchers also explored the joint contribution of health and SES to later-life labour force participation. One study based on two Finnish cohorts found a significant interaction between occupational position and cardiovascular disease, suggesting that compared with those with a high occupational position and no cardiovascular disease, participants with both a low occupational position and cardiovascular disease had a 4.5-fold risk of having disability retirement (Virtanen et al., Reference Virtanen, Lallukka, Ervasti, Rahkonen, Lahelma, Pentti, Pietilainen, Vahtera and Kivimaki2017). The reason behind this amplifying effect of a low occupational position on disability retirement might still relate to the universal mechanism of the socio-economic inequality in health: people with disadvantaged SES were less likely to approach/afford/accept health-care services to prevent, treat and monitor their chronic conditions, leading to a higher risk of having disability retirement (Virtanen et al., Reference Virtanen, Lallukka, Ervasti, Rahkonen, Lahelma, Pentti, Pietilainen, Vahtera and Kivimaki2017). Moreover, older adults in lower occupational positions are likely to have physically demanding jobs, which may not allow them to continue working because of their health problems. The WHO also proposed that participating in work depends on not only older adults’ intrinsic capacities – what they can do physically or mentally, but also the fit between older adults and the social environment. The supportive environment in advantaged socio-economic settings can remove barriers to compensate for the loss of mental or physical capacity, enabling those with a decrement in physical or mental health to stay in the labour market longer. This is important for both the economy and building an age-friendly world (WHO, 2015).
Dynamics of remaining in paid employment
A few studies about the health and socio-economic determinants of work exit did not consider individuals’ return to paid employment after an initial work exit (Fleischmann et al., Reference Fleischmann, Carr, Stansfeld, Xue and Head2018; Virtanen et al., Reference Virtanen, Lallukka, Ervasti, Rahkonen, Lahelma, Pentti, Pietilainen, Vahtera and Kivimaki2017; Carr et al., Reference Carr, Fleischmann, Goldberg, Kuh, Murray, Stafford, Stansfeld, Vahtera, Xue, Zaninotto, Zins and Head2018). In later life, older adults could leave work and re-enter the labour market more than once. One study in the USA found that around 50 per cent of retirees had non-traditional retirement paths which involved remaining in full and partial paid employment after normal pension age (Maestas, Reference Maestas2010). One study in the UK suggested that there was an inverted U-shaped relationship between age and unretirement; and the possibility of remaining in paid employment was the highest when an individual was in their mid- to late sixties (Kanabar, Reference Kanabar2015). Another UK study also found that among older participants aged 50–69 years, around 25 per cent of them experienced returning to paid employment after retirement (Platts et al., Reference Platts, Corna, Worts, McDonough, Price and Glaser2019). One study in Finland also indicated that, on average, older workers who were still employed at age 62 would spend another 13.5 months working before retirement during the flexible pension age range (age 63–68); and they would also return to paid employment for another 4.8 months after retirement (Leinonen et al., Reference Leinonen, Chandola, Laaksonen and Martikainen2020).
Remaining in paid employment after normal pension age might be due to failures in planning, low wealth accumulations or financial shocks, but might also be due to a more complicated retirement process. In a dynamic model of retirement, older adults’ expectations could be updated and reoptimised by their health conditions, finances and life satisfaction after retirement; and their psychological ‘burnout’ caused by the long-term employment during earlier adulthood could also recede after retirement. These transitions could render work relatively attractive again, making older adults return to the labour market (Maestas, Reference Maestas2010). There have been studies examining dynamic changes in later-life labour force participation. For example, one longitudinal study in the USA identified five work–retirement patterns including full retiree, partial retiree or part-time worker, full-time worker, work-disabled and homemaker in each wave of data collection (1998–2004). This study suggested that both older men and women could experience multiple transitions across waves (e.g. transiting from full-time worker to work-disabled, partial retiree or full retiree in older men; or transiting full retiree to partial retiree or part-time worker in older women) (Tang and Burr, Reference Tang and Burr2015). Instead of identifying work–retirement patterns in each wave, another longitudinal study summarised four patterns of labour force activities over eight interviews during 28 months of follow-up in US older men. The four patterns were no transitions–working, no transitions–non-working, transitions–crisp exit and transitions–blurred exit (Mutchler et al., Reference Mutchler, Burr, Pienta and Massagli1997).
Health and SES can determine older adults’ return to paid employment after retirement, as well as dynamic changes in later-life labour force status. For example, older adults with poor self-rated health were more likely to be in the work-disabled status (Tang and Burr, Reference Tang and Burr2015), have no return to paid employment after retirement (Platts et al., Reference Platts, Corna, Worts, McDonough, Price and Glaser2019) and experience crisp exit from paid employment (Mutchler et al., Reference Mutchler, Burr, Pienta and Massagli1997). Returning to paid employment after retirement was more common among older adults who were more educated (Platts et al., Reference Platts, Corna, Worts, McDonough, Price and Glaser2019) or had a higher occupational position (Leinonen et al., Reference Leinonen, Chandola, Laaksonen and Martikainen2020). However, for economic-related factors, findings were mixed. For example, in the Finnish study, high household income seemed to encourage later retirement and participation in post-retirement employment (Leinonen et al., Reference Leinonen, Chandola, Laaksonen and Martikainen2020); while in the US study, having more non-housing economic resources was associated with a higher probability of becoming a full retiree in older men (Tang and Burr, Reference Tang and Burr2015). Another US study also suggested that older male workers with high non-wage income and pension availability tended to transit from full-time working to blurred exit from the labour market (Mutchler et al., Reference Mutchler, Burr, Pienta and Massagli1997). The UK study found no association between income and post-retirement employment after controlling for a wide range of confounders (Platts et al., Reference Platts, Corna, Worts, McDonough, Price and Glaser2019).
Limitations in methodology still existed in these studies. Only time-invariant variables for health and socio-economic factors were used in these studies (Mutchler et al., Reference Mutchler, Burr, Pienta and Massagli1997; Tang and Burr, Reference Tang and Burr2015; Platts et al., Reference Platts, Corna, Worts, McDonough, Price and Glaser2019; Leinonen et al., Reference Leinonen, Chandola, Laaksonen and Martikainen2020). Participants may experience more than one work exit/return event; but in these studies, only the first-time work exit was considered (Platts et al., Reference Platts, Corna, Worts, McDonough, Price and Glaser2019; Leinonen et al., Reference Leinonen, Chandola, Laaksonen and Martikainen2020). Although dynamic changes in later-life labour force status across waves were identified, determinants of these dynamic changes were not examined; instead, only associations between health/socio-economic factors and fixed patterns of labour force status at baseline were examined (Tang and Burr, Reference Tang and Burr2015). Moreover, there were no statistical approaches to handling missingness in covariates when testing these associations (Tang and Burr, Reference Tang and Burr2015). Therefore, when identifying determinants of later-life labour force participation, choosing time-varying covariates and considering repeatable events of labour force participation in later life are needed. Furthermore, appropriate analytical methods to handle missing data could be applied.
Research gap, aim, objectives and hypotheses
In summary, previous studies about health and socio-economic determinants of later-life labour force participation have been mainly from high-income European countries and the USA. Evidence from other countries is limited. Findings vary between studies due to different measures of SES and later-life labour force outcomes. Additionally, appropriate analytical methods for the inclusion of time-varying covariates and repeatable events of labour force participation in later life is needed.
We aimed to investigate the associations of older adults’ intrinsic capacity and SES with participating in work in later life in countries of different regions, using the harmonised measures of SES and later-life labour force outcomes. The Ageing Trajectories of Health – Longitudinal Opportunities and Synergies (ATHLOS) consortium (Sanchez-Niubo et al., Reference Sanchez-Niubo, Egea-Cortés, Olaya, Caballero, Ayuso-Mateos, Prina, Bobak, Arndt, Tobiasz-Adamczyk, Pająk, Leonardi, Koupil, Panagiotakos, Tamosiunas, Scherbov, Sanderson, Koskinen, Chatterji and Haro2019) harmonised 17 ageing cohorts worldwide, providing an opportunity for us to look into this research question cross-nationally. Five cohort studies were selected including the US Health and Retirement Study (HRS) (Sonnega et al., Reference Sonnega, Faul, Ofstedal, Langa, Phillips and Weir2014), the English Longitudinal Study of Ageing (ELSA) (Steptoe et al., Reference Steptoe, Breeze, Banks and Nazroo2013), the Japanese Study of Aging and Retirement (JSTAR) (Hidehiko et al., Reference Hidehiko, Satoshi and Hideki2010), the Mexican Health and Aging Study (MHAS) (Wong et al., Reference Wong, Michaels-Obregon and Palloni2017) and the China Health and Retirement Longitudinal Study (CHARLS) (Zhao et al., Reference Zhao, Hu, Smith, Strauss and Yang2014). These countries are all major economies in their regions and account for approximately 50 per cent of the global economy and 40 per cent of the world population aged 65 and over; while they also represent diverse economic, social, cultural and epidemiological contexts (World Bank, 2015; International Monetary Fund, 2019). The five cohorts all have at least three waves of data collection and available variables in labour force participation, SES and intrinsic capacity, which are ideal for investigating our main research question using time-varying variables for covariates and labour force outcomes (considering the repeatable events of labour force outcomes, which can be recurrent and collected repeatedly over time). Exploring differences and similarities in the associations of older adults’ intrinsic capacity and SES with participating in work in later life within and across countries will be instructive for setting common and country-specific strategies to promote healthy labour force participation and healthy ageing in later life.
Specifically, our objectives were to (a) examine the longitudinal association of physical incapacity (measured by a mobility score as well as three levels of this score) and SES (measured by quintiles of wealth) with remaining in paid employment (a subset of labour force participation) in older adults in each country; (b) test whether wealth moderated the association between physical incapacity and remaining in paid employment in each country; and (c) compare inequalities in probabilities of remaining in paid employment by physical incapacity and wealth across countries.
We hypothesised that:
(1) Older adults with a higher level of physical incapacity are less likely to remain in paid employment than those without physical incapacity in each country.
(2) Wealth is a moderator for the relationship between physical incapacity and remaining in paid employment in each country (i.e. although the odds of remaining in paid employment decreases with increasing physical incapacity among both socio-economically advantaged and disadvantaged older adults, the decreasing rate in odds is slower among socio-economically advantaged individuals than disadvantaged individuals).
Methods
Sample
We included 8,003 (HRS Waves 6–11, 2002–2013) US participants, 7,225 (ELSA Waves 1–7, 2002–2015) English participants, 2,163 (JSTAR Waves 1–3, 2007–2011) Japanese participants, 7,374 (MHAS Waves 1–3, 2001–2013) Mexican participants and 7,367 (CHARLS Waves 1, 2 and 4, 2011–2016) Chinese participants. Wave 6 (2002) rather than Wave 1 (1992) of HRS was used as the baseline wave, to minimise the variations in period effect on the age-cohort model for the longitudinal analysis across countries (Fannon and Nielsen, Reference Fannon and Nielsen2018). In each country, samples whose individual-level weights at baseline were missing or zero, and samples aged less than 60 years old at baseline were excluded. Figure S1 in the online supplementary material illustrates the procedure of sample selection.
Physical incapacity
Physical incapacity (time-varying) was measured as the sum score (range 0–7) of seven self-reported indicators of mobility (yes/no) in each wave, including difficulties for walking without equipment, sitting for long periods, climbing stairs, stooping/kneeling/crouching, reaching/extending arms, lifting/carrying weights and picking up coins. A higher score indicates higher incapacity. The internal consistency of the sum score was ⩾0.7, in an acceptable range (Price et al., Reference Price, Jhangiani, Chiang, Price, Jhangiani and Chiang2015). The predictive validity of the score for mortality was similar to or better than that by the scales of (instrumental) activities of daily living (Hajian-Tilaki, Reference Hajian-Tilaki2013) (see Table S1 and Figure S2 in the online supplementary material). We also re-categorised the sum score into three levels in each country (0 = none, 1–2 = middle, ⩾3 = highest).
Socio-economic status (SES)
The SES was assessed by household wealth (time-varying) in each wave. Household wealth was the sum of all wealth components minus the sum of all debts. All wealth components included net values of primary and second residence and other real estates, vehicles, business, stocks, mutual funds and investment trusts, checking, savings and money market accounts, governmental savings bonds, T-bills and certificates of deposit, bonds and bond funds, and others. All debts included first and second mortgages, other home loans and other debts.
For each continuous wealth variable in each wave of each country, we firstly applied the inflation adjustment using the consumer price index provided by the World Bank (2017). Secondly, all continuous wealth variables across waves in each country were organised into quintiles based on the analytical sample size at baseline, ranging from the highest to the lowest levels.
Paid employment
Paid employment (time-varying) was measured by asking participants whether they were currently in paid employment (yes or no) in each wave. Paid employment was one of the elements of labour force participation. Through using time-varying variables for remaining in paid employment, we captured the dynamics of remaining in paid employment before and after normal retirement age during follow-up.
Confounding factors
Time-varying age, marital status, smoking, the eligibility for full retirement and long-term conditions, and time-invariant gender, birth cohort group and education, were included as confounders. The long-term conditions included diabetes, respiratory diseases, joint disorders, cancer, hypertension and stroke. The time-varying variable for the eligibility for full retirement was created based on every participant's age in each wave and also normal pension age in each country, namely 65 years for all US participants (born in/before 1942), 65 years for English male participants and 60 years for English female participants (born in/before 1943), 65 years for all Japanese participants (born in/before 1947), 65 years for all Mexican participants (born in/before 1941) and 60 years for Chinese male participants and 55/50 years for Chinese female participants (born in/before 1952) in our study (Social Security Administration, 2018–2019).
Missing data
Table S2 in the online supplementary material shows percentages of non-respondents and non-responding items for all variables in each wave of each country. During follow-up, around 31 per cent of US participants, 65 per cent of English participants, 41 per cent of Japanese participants, 18 per cent of Mexican participants and 21 per cent of Chinese participants became non-respondents. JSTAR, MHAS and CHARLS have more missing data than the HRS and ELSA, particularly for wealth, physical incapacity, smoking and long-term conditions. For example, percentages of missing data for baseline wealth in JSTAR, MHAS and CHARLS were around 56, 17 and 10 per cent, respectively. While there was no missing data for baseline wealth in HRS, in ELSA the percentage of missing data for baseline wealth was around 1 per cent. Due to larger missingness in JSTAR, MHAS and CHARLS, conducting complete case analyses might exclude a large number of valid samples in the three countries, resulting in a decreased power of analysis. Results based on complete case analyses thus might not be representative in the three countries.
Multiple imputation (using 50 datasets) was used to address missing data for covariates and outcome variables across waves in the five countries. Imputation models were built using the twofold fully conditional specification (FCS) algorithm (Welch et al., Reference Welch, Bartlett and Petersen2014), by including all covariates, outcome variables and individual-level weights. Imputed covariates and outcome variables were used for data analysis. Age in each wave was used as the timing variable. Compared with the wave number, which assumes that every respondent is measured at the same time-point, age is more accurate in measuring changes in paid employment status over time, as it specifies an entry and exit time for each individual differently. With the twofold FCS algorithm, interactions between age and other variables were automatically considered in the imputation model. Records with imputed values for non-respondents in each wave were automatically excluded, as the twofold FCS algorithm only imputed non-responding items within each wave, rather than non-responders (attrition/wave non-response) in that wave. For each country, 50 imputed datasets were created.
Statistical analyses
We applied multilevel mixed-effects logistic regression to estimate the association of physical incapacity (categorical) and wealth (quintiles) with remaining in paid employment in each country, allowing for random intercepts for each participant (Sommet and Morselli, Reference Sommet and Morselli2017). In longitudinal data, the multilevel logistic model is suitable for the repeatable events of paid employment, which can be recurrent and collected repeatedly over time, allowing for the correlation between durations to events experienced by the same individual, or individuals who are clustered into the higher-level units (Steele, Reference Steele2008). Age was the timing metric and centred on 60 to aid interpretation. In each country, we built both basic and fully adjusted models. The basic model was controlled for gender and linear and quadratic terms of age. The fully adjusted model was additionally controlled for cohort group, marital status, education, smoking, long-term conditions and eligibility for a full retirement pension. We also tested the multiplicative interactions between physical incapacity and wealth. The Wald test (Rodríguez, Reference Rodríguez2007) was applied to compare the difference between a model with interaction and a model without interaction. Odds ratios with 95 per cent confidence intervals (CIs) were calculated.
In the next step, we quantified cross-country inequalities in the probability of remaining in paid employment by physical incapacity (continuous) and wealth (quintiles) with increasing age. We combined country-specific data into one pooled dataset and generated a country variable (0 = USA (reference category), 1 = England, 2 = Japan, 3 = Mexico, 4 = China). This allowed us to test whether the cross-country differences in age-related probabilities of remaining in paid employment by physical incapacity and wealth were statistically significant, through including the multiplicative interaction terms among country, physical incapacity and wealth. Both linear and quadratic terms of the physical incapacity score were included in the model. The model was additionally adjusted for linear and quadratic terms of age, cohort group, gender, marital status, education, smoking, long-term conditions and eligibility for a full retirement pension. The Wald test helped build the final model. Probabilities of remaining in paid employment by physical incapacity and wealth at age 60, 65 and 70 years across countries were predicted using marginal effects with 95 per cent CIs (Norton et al., Reference Norton, Dowd and Maciejewski2019), to aid interpretations for comparing inequalities in the probability of remaining in paid employment between countries.
Finally, we conducted sensitivity analyses. Firstly, we used time-varying continuous scores of physical incapacities to examine the main association of physical incapacity and wealth with remaining in paid employment in each country, adjusting for all confounding factors. Secondly, since agricultural work in China was not considered as paid employment during data harmonisation, we identified persons who mainly worked on farmland (around 70% of the Chinese sample) as having paid employment and re-ran multilevel analysis in China. The reason is that agricultural employment in China is associated with an increased opportunity for rural older workers to continue working in later life (Clark et al., Reference Clark, York and Anker1999).
All analyses were performed using Stata MP 16.1 (StataCorp, 2017).
Results
Baseline sample characteristics
Table 1 shows sample characteristics at baseline. US, Japanese and Chinese participants were younger than English and Mexican participants. All countries had more women than men except for China. English, Mexican and Chinese participants were more likely to be widowed but have a lower level of educational attainment than their US and Japanese counterparts. Remaining in paid employment was more common in the USA, Japan and Mexico than in England and China. Japanese and Mexican participants had the lowest (0) and the highest (2) median value of the sum score of physical incapacity, respectively. Around 80 per cent of Japanese participants had no physical incapacity, whereas in other countries proportions were less than 50 per cent. China had the highest proportion of smokers. Long-term conditions were common in all countries but more so in the USA. The majority of participants had been eligible for full retirement pension in each country.
Table 1. Sample characteristics at baseline in the United States of America (USA), England, Japan, Mexico and China

Notes: 1. A higher score indicates higher incapacity. SD: standard deviation.
Within-country analyses
Table 2 presents results of basic models for the within-country association of physical incapacity and wealth with remaining in paid employment. In all countries, compared to those without physical incapacity, participants in the highest level of physical incapacity had significantly lower odds of remaining in paid employment, with odds ratios ranging between 0.07 (95% CI = 0.03–0.16) in Japan to 0.36 (95% CI = 0.23–0.58) in China. Compared with participants with the highest level of wealth, those with the lowest level of wealth had significantly lower odds of remaining in paid employment in the USA, England and China; in Japan, the odds of remaining in paid employment was the lowest among participants with the second-lowest level of wealth; but the relationship between wealth and remaining in paid employment was non-significant in Mexico. The multiplicative interactions between physical incapacity and wealth were non-significant in all countries. In each country, the Wald test suggested that model fitness did not increase significantly by adding this multiplicative interaction (p > 0.05). After full adjustment, results for main associations shown in Table 3 remained similar to the basic models shown in Table 2. Models in Tables 2 and 3 did not include the multiplicative interactions between physical incapacity and wealth.
Table 2. Results of basic multilevel models for associations between physical incapacity, wealth and paid employment in the five countries

Notes: Each model was adjusted for age, age-squared and gender only. USA: United States of America. Ref.: reference category.
Significance levels: * p < 0.05, ** p < 0.01, *** p < 0.001.
Table 3. Results of fully adjusted multilevel models for associations between physical incapacity, wealth and paid employment in the five countries

Notes: Each model was adjusted for age, age-squared, gender, cohort group, education, smoking, marital status, long-term conditions and eligibility for full retirement pension. USA: United States of America. Ref.: reference category.
Significance levels: * p < 0.05, ** p < 0.01, *** p < 0.001.
Inequalities in the probability of remaining in paid employment by physical incapacity and wealth
Figure 1 shows predicted probabilities of remaining in paid employment by wealth and physical incapacity at age 60, 65 and 70 in each country, based on the estimation of the fully adjusted model shown in Table S3 in the online supplementary material. Generally, probabilities of remaining in paid employment decreased with the increase of age and with the increase of the score of physical incapacity. Patterns of the probability of remaining in paid employment by wealth were not uniform across countries. Wealth gradients in remaining in paid employment were clearer in the USA, England and Japan than in Mexico and China. Particularly in the USA, when having no physical incapacity (sum score = 0), the absolute differences in the probability of remaining in paid employment between the richest and the poorest groups were approximately 60, 50 and 40 per cent at age 60, 65 and 70, respectively, which were greater than that in any other country at the same age. The multiplicative interaction between wealth and physical incapacity was not statistically significant: as the score of physical incapacity increased from 0 to 7, the probability of remaining in paid employment declined by half in each wealth group. However, in the USA, England and Japan, the absolute decline in the probability of remaining in paid employment with increasing physical incapacity was the largest in the richest group, due to a distinctly higher probability of remaining in paid employment in the richest group when having no physical incapacity (sum score = 0). Thus, the absolute inequality in the probability of remaining in paid employment by wealth was large when physical incapacity was low, but small when physical incapacity was high in the USA, England and Japan. Probabilities of remaining in paid employment were high in all wealth groups in Mexico (e.g. approximately 40–60% at age 65), but low in all wealth groups in China (e.g. less than 5% at age 65). With increasing physical incapacity, compared to the USA, trajectories of the probability of remaining in paid employment declined faster in England and Japan, but slower in China and Mexico. This was due to a significant interaction between physical incapacity and country (see Table S3 in the online supplementary material).
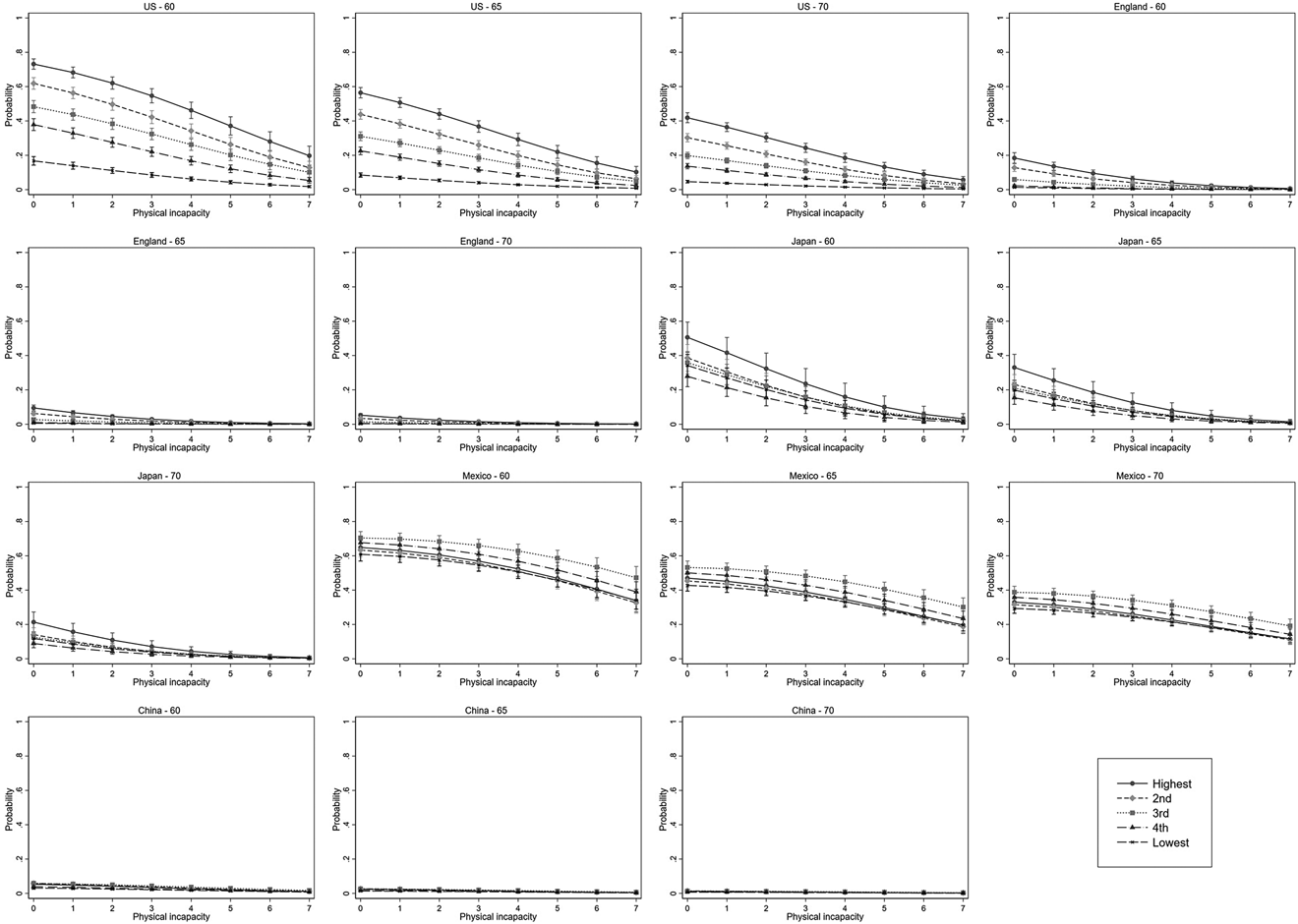
Figure 1. Marginal effects of changes in probability of remaining in paid employment by quintiles of wealth with increasing physical incapacity at 60, 65 and 70 years old.
Note: US: United States of America.
Sensitivity analyses
Table S4 in the online supplementary material shows the association of continuous physical incapacity score and wealth with remaining in paid employment in each country. Results were identical to the results of our main analyses. In each country, the increased score of physical incapacity was associated with decreased odds of remaining in paid employment in later life. A higher level of wealth was associated with higher odds of remaining in paid employment in the USA, England, Japan and China, but not Mexico.
Table S5 in the online supplementary material presents results for the main association in China when re-categorising the participation of agricultural work into the group of remaining in paid employment. Different from the main results shown in Tables 2 and 3, less-wealthy participants had higher odds of remaining in employment than their richest counterparts in China.
Discussion
In summary, in all countries, increased physical incapacity was associated with lower odds of remaining in employment (confirming Hypothesis 1). Older adults with lower levels of wealth were less likely to remain in paid employment than those with the highest level of wealth in the USA, England and Japan, but not in Mexico. Wealth was not a moderator for the relationship between physical incapacity and remaining in paid employment in any country (rejecting Hypothesis 2). We also found that the absolute inequality in the probability of remaining in paid employment by wealth was large when physical incapacity was low, but small when physical incapacity was high in the USA, England and Japan; and probabilities of remaining in paid employment were high and low in all wealth groups in Mexico and China, respectively.
Consistent with previous work (van Rijn et al., Reference van Rijn, Robroek, Brouwer and Burdorf2014; Stafford et al., Reference Stafford, Cooper, Cadar, Carr, Murray, Richards, Stansfeld, Zaninotto, Head and Kuh2017; Fleischmann et al., Reference Fleischmann, Carr, Stansfeld, Xue and Head2018), we found that physical incapacity, as an indicator of individual health, was a predictor of remaining in paid employment in later life in each country. We also found that compared to US participants, with increasing physical incapacity, trajectories of the probability of remaining in paid employment declined faster in England and Japan, but slower in Mexico and China. One potential explanation is that England and Japan have had free or low-cost national health care for the long term. Without salary income and sufficient wealth in later life, English and Japanese older adults could still have protection against the major health-care costs that go beyond income level. This might encourage them to quit the labour market, especially when having more illness or increased incapacity (Reich and Shibuya, Reference Reich and Shibuya2015; National Health Service, 2018). Countries including the USA, Mexico and China are making progress to achieve universal health coverage under new health-care programmes, such as the Medicaid expansion (including Affordable Care Act) in the USA (Barnett and Sommers, Reference Barnett and Sommers2017), Seguro Popular in Mexico (King et al., Reference King, Gakidou, Imai, Lakin, Moore, Nall, Ravishankar, Vargas, Tellez-Rojo, Avila, Avila and Llamas2009), and the New Cooperative Medical Scheme in China (Zhang et al., Reference Zhang, Dong, Xu, Miao, Mao, Sloan and Tang2021). However, there is heterogeneity in actual health-care reimbursements and changes in health-care policies across regions within countries; and the overall out-of-pocket spending on health services in the general population is still high (King et al., Reference King, Gakidou, Imai, Lakin, Moore, Nall, Ravishankar, Vargas, Tellez-Rojo, Avila, Avila and Llamas2009; Hero et al., Reference Hero, Zaslavsky and Blendon2017; Zhang et al., Reference Zhang, Dong, Xu, Miao, Mao, Sloan and Tang2021). These issues might discourage older adults to leave the labour market, particularly if they have catastrophic spending on health services for themselves and their families.
Significant wealth inequalities in remaining in paid employment were found in countries including the USA, England and Japan. This finding supported the notion that older adults in socio-economically disadvantaged settings were more likely to leave paid employment (Leinonen et al., Reference Leinonen, Martikainen and Lahelma2012; Carr et al., Reference Carr, Fleischmann, Goldberg, Kuh, Murray, Stafford, Stansfeld, Vahtera, Xue, Zaninotto, Zins and Head2018; Fleischmann et al., Reference Fleischmann, Carr, Stansfeld, Xue and Head2018). This finding could be potentially explained by several reasons. Compared with socio-economically advantaged older adults, socio-economically disadvantaged older adults are more likely to have unskilled or manual jobs, making them suffer from health problems in earlier older ages (Padilla, Reference Padilla2011). From the supply side, socio-economically disadvantaged older adults at an older age might not be healthy enough to work even if they need or want to; from the demand side, employers might be reluctant to employ older workers for manual jobs, particularly if companies need to cover older workers’ health insurance, making them have a high risk of layoffs and a low possibility of finding a new job in later life (Staudinger et al., Reference Staudinger, Finkelstein, Calvo and Sivaramakrishnan2016). Other structural factors such as pension and public benefits can also influence older adults’ labour force participation in these countries. Researchers have found that public benefits for US older adults have been largely protected over the past decades, especially for those in disadvantaged socio-economic settings; compared with the working-age population, government transfers have been more equally distributed among the ageing population in the USA (Bosworth et al., Reference Bosworth, Burtless and Zhang2016). In the UK, the pension system is also effective in preventing the ‘very bottom’ poverty although compared with the USA, the average pension income of older adults in the UK is lower (Sefton et al., Reference Sefton, Evandrou and Falkingham2007). Some researchers suggested that greater public pension entitlement is still important for reducing inequalities in unmet medical needs among older adults in the UK (Reeves et al., Reference Reeves, McKee, Mackenbach, Whitehead and Stuckler2017). Therefore, stable pension and public benefits might encourage socio-economically disadvantaged older adults to leave paid employment in the USA and England. Differently, the public pension scheme in Japan seemed unlikely to encourage older adults to leave paid employment, as Japan has both stringent minimum earnings and working-time requirements for pension entitlement, while over half of Organisation for Economic Co-operation and Development (OECD, 2019) countries have no such requirements. In Figure 1, we also notice that for participants within the same level of wealth, the probability of remaining in paid employment was always higher in Japan than in England and the USA.
Wealth can be both an indicator of SES and a measure of economic hardship in later life. Previous evidence suggested that a low level of wealth could be associated with continued employment in later life since older adults may not be able to afford retirement due to economic constraints (Dwyer and Mitchell, Reference Dwyer and Mitchell1998; McGarry, Reference McGarry2004; Tang and Burr, Reference Tang and Burr2015; Leinonen et al., Reference Leinonen, Chandola, Laaksonen and Martikainen2020). This could potentially explain the non-significant association between wealth and remaining in paid employment in Mexico in our study. Similar to older adults in the USA, England and Japan, socio-economically advantaged older Mexicans would have continued employment probably due to better job opportunities and working conditions in later life. However, socio-economically disadvantaged older Mexican workers might be forced to stay in the labour market for a longer-term because of poverty. In OECD countries, Mexico ranked third for the labour force participation rate of people aged 65 years and over in 2015 (OECD, 2015). Due to low levels of education and skills, socio-economically disadvantaged older workers in Mexico are mainly employed in informal sectors, resulting in earning insufficient income and having no pension through social security schemes in later life (AARP and Foreign Policy Analytics, 2017). A lack of economic security for daily living and health care might make Mexican workers continue to stay in the labour market during older age. Although the introduction of Seguro Popular in Mexico has largely improved citizens’ access to quality health care, health-care services are provided by many social security institutes which are not well connected. Mexicans may have to switch doctors when quitting from their work, leading to disruption of their continuous health care (King et al., Reference King, Gakidou, Imai, Lakin, Moore, Nall, Ravishankar, Vargas, Tellez-Rojo, Avila, Avila and Llamas2009). Therefore, older Mexicans, particularly those with financial constraints, would remain in paid employment, to maintain their stable access to quality health care. In summary, probabilities of remaining in paid employment were high in Mexican participants with both high and low levels of wealth; but reasons for remaining in paid employment between rich and poor Mexican participants could be different (i.e. choices related to socio-economic advantage versus necessities related to economic disadvantage).
Although a high level of wealth was significantly associated with remaining in paid employment in China in our main analyses, the probabilities of remaining in paid employment are very low in all Chinese participants. In the original composition of the CHARLS sample, those who were categorised as having paid employment in each wave were mainly officials, managers, leaders and paid workers (Lu et al., Reference Lu, Pikhart and Sacker2021). Despite inequalities in their occupational positions, all these participants can have stable and secure pension income covered by the urban pension system (Social Security Administration, 2018–2019; Hou et al., Reference Hou, Wang, Wang and Zhao2021). Thus, they might have a strong incentive to be retired after passing the eligible age. In our sensitivity analyses, socio-economically disadvantaged agricultural workers were more likely to remain in employment than others. In China, pension participation for agricultural workers is voluntary and the benefits of the rural pension system are far less generous than the urban pension system (Fjeld and Sagli, Reference Fjeld, Sagli, Eide and Ingstad2011; Hou et al., Reference Hou, Wang, Wang and Zhao2021). Therefore, rural agricultural workers would still work on farmland in a later age to accumulate savings for expenditures of daily livings and health care.
From a global perspective, two studies in the 1990s indicated that older adults from middle- and low-income countries in Africa, Asia and Latin America had significantly higher labour force participation rates than their counterparts from high-income countries in Europe and North America (Clark and Anker, Reference Clark and Anker1993; Clark et al., Reference Clark, York and Anker1999). However, neither of the two studies considered the existing socio-economic inequality in labour force participation within each country. In our study, we found clear wealth gradients in remaining in paid employment in the USA, England and Japan. Particularly in the USA, the absolute difference in the probability of remaining in paid employment between the poorest and the richest groups was daunting (Figure 1). In 2013, the United Nations projected that the gap in later-life labour force participation rate between middle-/low-income and high-income countries would decrease over the next decades, due to an increased retirement income on average among men in middle-/low-income countries, and positive attitudes towards later-life labour force participation, improved health in general, and the reduction in pension replacement rates among both men and women in high-income countries (United Nations, 2013; Staudinger et al., Reference Staudinger, Finkelstein, Calvo and Sivaramakrishnan2016). However, our results suggested that this gap might not be decreasing if considering socio-economic inequalities in labour force participation within countries. Older adults from high-income countries could still have a very low probability of remaining in paid employment in later life if they are socio-economically disadvantaged.
Regarding the absolute inequality in the probability of remaining in paid employment by wealth, we found that this absolute inequality was large when physical incapacity was low, but small when physical incapacity was high in the USA, England and Japan (Figure 1). This finding suggested that the protective effect of wealth on remaining in paid employment in the three high-income countries decreased as physical incapacity increased. The adverse effect of physical incapacity on remaining in paid employment could be compensated by wealth only when the physical incapacity was mild or moderate. Although older adults nowadays are healthier than their counterparts in previous generations, having illness or incapacity is still one of the most frequent reasons for leaving the labour market worldwide (Staudinger et al., Reference Staudinger, Finkelstein, Calvo and Sivaramakrishnan2016).
Strengths and limitations
Using harmonised data from five sister longitudinal studies of ageing worldwide, our study filled the research gap by using comparable and time-varying variables to investigate health and socio-economic determinants of remaining in paid employment in later life in both high-income and middle-income countries. We applied an advanced statistical method: multilevel mixed-effects logistic regression, considering repeated events of having paid employment over up to 14 years of follow-up. We also predicted age-related probabilities of remaining in paid employment by wealth and physical incapacity in each country.
Our study has several limitations. Firstly, data harmonisation resulted in the omission of some country-specific covariates. For example, our model did not adjust for occupational position due to disparities and missingness in occupational classifications across countries. We have the 1980 US Census Occupation in HRS (for those who had not been in work since entering the cohort, their occupational positions were not identified in the original data), the National Statistics Socio-Economic Classification in ELSA, the Japan Standard Occupational Classification in JSTAR (more than 70% of participants had unclassifiable occupations), the Mexican Classification of Occupations in MHAS, but missing occupational classifications in CHARLS. The post hoc analyses controlling for occupational position were conducted in England and Japan (see Table S6 in the online supplementary material). Findings were identical to the main findings in Table 3, suggesting that the exclusion of occupational position did not influence the direction of the main relationship. We did not consider specific types of paid employment (full-time versus part-time) due to unavailability of relevant information and/or large missingness in original variables in CHARLS, JSTAR and MHAS. Future studies exploring health and socio-economic determinants of remaining in part-time and full-time paid employment separately are needed. This is important, as many countries are encouraging bridge employment (i.e. participation in the labour force between retirement from full-time work and complete workforce withdrawal) and setting flexible pension age ranges to encourage part-time paid employment before fully leaving the labour market (Alpass, Reference Alpass and Pachana2015). Additionally, alcohol consumption was not considered in the current analysis. This is because more than 70 per cent of Mexican participants had missing data for alcohol consumption. However, alcohol consumption might be associated with physical incapacity (Hu et al., Reference Hu, Pikhart, Kubinova, Malyutina, Pajak, Besala, Bell, Peasey, Marmot and Bobak2016), SES (Collins, Reference Collins2016) and labour force participation (Jorgensen et al., Reference Jorgensen, Pedersen, Thygesen, Lau, Christensen, Becker and Tolstrup2019).
Secondly, we only imputed item non-response instead of wave non-responders in each wave. Participants who dropped out of the study after the baseline wave might be more likely to have severe illness than those who remained. Our main statistical approach, multilevel modelling, is capable of handling attrition and wave non-response, unequal time spaces, and the inclusion of time-varying and between-individual covariates that are either continuous or discrete measures (Steele, Reference Steele2008). We also created 50 imputed datasets in each country to ensure that the number of imputations was large enough not to affect the conclusions or inhibit analysis reproducibility, particularly for countries like Japan, Mexico and China, as the number of imputed datasets should be approximately equal to or larger than the percentage of incomplete cases (White et al., Reference White, Royston and Wood2011). Although statistical strategies can, to some extent, address the potential bias caused by missingness, they are not perfect. Therefore, our findings might still underestimate the adverse effect of physical incapacity on remaining in paid employment.
Thirdly, we excluded those aged less than 60 years at baseline, limiting the generalisability of our findings to individuals aged 60 years and older. Previous studies on health and socio-economic determinants of remaining in paid employment have largely focused on younger age groups (participants were mainly aged 60 years or less) (Dwyer and Mitchell, Reference Dwyer and Mitchell1998; Carr et al., Reference Carr, Fleischmann, Goldberg, Kuh, Murray, Stafford, Stansfeld, Vahtera, Xue, Zaninotto, Zins and Head2018; Fleischmann et al., Reference Fleischmann, Carr, Stansfeld, Xue and Head2018; McGarry, Reference McGarry2004; van Rijn et al., Reference van Rijn, Robroek, Brouwer and Burdorf2014; Stafford et al., Reference Stafford, Cooper, Cadar, Carr, Murray, Richards, Stansfeld, Zaninotto, Head and Kuh2017). However, currently, many adults aged 65 or more remain active, healthy and refuse to accept that they are old. The United Nations has not adopted a standard cut-off to define old age globally either (British Geriatrics Society, 2017). Our study would therefore provide evidence on determinants of remaining in paid employment after age 60. Nevertheless, distributions of some covariates among participants might be altered and variations in risk factors might also be reduced due to survival selection. Our study might underestimate the association of physical incapacity and wealth with remaining in paid employment.
Policy implications
Health is still a vital predictor of remaining in paid employment in later life. More efforts should be made to achieve universal health coverage in the USA, Mexico and China. National policies should consider older adults’ changing capacities in older age for job placement and prioritise the provision of supportive services for less-wealthy older adults to avoid premature loss of function and institutionalisation, to reduce the socio-economic gap in later-life labour force participation. Reasonable adjustments in the workplace for older adults with disabilities and health conditions could also maintain the rate of remaining in paid employment and decrease the rate of unemployment due to disability (Office of Disability Employment Policy, 2018).
Countries such as Mexico and China have not had adequate old-age income support for older adults, particularly for those in socio-economically disadvantaged settings (e.g. informal workers in Mexico or agricultural workers in China). Their high probabilities of remaining in paid employment in our study might not be an optimistic phenomenon since the hardship could be entailed in working until death. However, informal work (including agricultural work) has represented a substantial part of the labour market in some middle- and low-income countries. The development of pathways for informal workers to access different forms of social security and pension coverage in middle-/low-income countries like Mexico and China is needed (Staudinger et al., Reference Staudinger, Finkelstein, Calvo and Sivaramakrishnan2016). Additionally, we found very low probabilities of remaining in paid employment for Chinese participants who were officials, managers, leaders and paid workers. One study based on CHARLS also reported that the additional work capacity among age groups 60–64 and 65–69 was 42.4 and 38.3 per cent, respectively, for men and 37.6 and 37.7 per cent, respectively, for women in urban China; and in the post-retirement age cohorts, there was more excess work capacity among the better-educated older adults (Hou et al., Reference Hou, Wang, Wang and Zhao2021). Therefore, improvements in retirement policies to encourage older adults’ later-life labour force participation in urban China are needed. A waste of more-educated human resources caused by retirement age policies should be avoid (Hou et al., Reference Hou, Wang, Wang and Zhao2021).
Countries such as the USA, England and Japan have comprehensive old-age income support for older adults. To help less-wealthy older adults remain in paid employment for a longer term, apart from raising normal pension age and incentivising later retirement, policies for encouraging employers to hire socio-economically disadvantaged older workers (e.g. monetary incentives and anti-age discrimination policies) and enhancing older workers’ employability (e.g. vocational training) could also be facilitated (Staudinger et al., Reference Staudinger, Finkelstein, Calvo and Sivaramakrishnan2016).
Conclusions
Physical capacity was a predictor of remaining in paid employment in each country. Wealthier older adults were more likely to remain in paid employment in the USA, England, Japan but not in Mexico. Probabilities of remaining in paid employment were generally high in Mexico but very low in China. The absolute difference in the probability of remaining in paid employment between the richest and the poorest groups was greater in the USA than in any other country. The inverse association between physical incapacity and remaining in paid employment could be partially compensated by wealth only when physical incapacity was not severe in the USA, England and Japan.
Data
The HRS (http://hrsonline.isr.umich.edu/) was developed by a team of researchers based at the University of Michigan, supported by the National Institute on Aging and the Social Security Administration. ELSA (http://www.data-archive.ac.uk/) was developed by a team of researchers based at NatCen Social Research, University College London and the Institute for Fiscal Studies. CHARLS (http://charls.pku.edu.cn/en) was supported by the Behavioural and Social Research division of the National Institute on Aging, the Natural Science Foundation of China, the World Bank, the China Medical Board and Peking University. JSTAR (https://www.rieti.go.jp/en/projects/jstar/) was conducted by the Research Institute of Economy, Trade and Industry (RIETI), Hitotsubashi University and the University of Tokyo. MHAS (http://www.mhasweb.org/index.aspx) is a collaborative effort among researchers from the University of Texas Medical Branch (UTMB), the Instituto Nacional de Estadística y Geografía (INEGI, Mexico), the University of Wisconsin, the Instituto Nacional de Geriatría (INGER, Mexico), the Instituto Nacional de Salud Pública (INSP, Mexico) and the University of California Los Angeles (UCLA). Harmonised datasets from the Ageing Trajectories of Health – Longitudinal Opportunities and Synergies (ATHLOS) project (http://athlosproject.eu/) were used where possible.
Acknowledgements
We thank the developers, funders and archives of HRS, ELSA, JSTAR, MHAS and CHARLS, and the ATHLOS. We also thank all participants in the five cohort studies. All of them bear no responsibility for the analyses or interpretations presented here.
Author contributions
WL and MB designed the study. WL performed the statistical analysis and wrote the first draft of the article. ASN organised data harmonisation and management. MB, DS and MM assisted WL with refining the analysis and interpreting results. All authors contributed to drafting, revision and approval of the article.
Financial support
This work was supported by the European Union's Horizon 2020 Research and Innovation Programme (635316); the CETOCOEN Excellence (857560); and the R-Exposome Chair (857487).
Conflict of interest
The authors declare no conflicts of interest.
Ethical standards
We used secondary data. Ethical approval is not required.





 Open access
Open access