


Introduction
Perinatal depression, also referred to as maternal depression, can occur during pregnancy or up to 1 year postpartum. It is considered the most common complication of pregnancy. In their systematic review of perinatal depression, Gavin et al.( Reference Gavin, Gaynes and Lohr 1 ) reported a pooled point prevalence of 11 % for minor depression during pregnancy and 13 % for postpartum depression in high-income countries. Early studies reported differing levels of perinatal depression in low-income and middle-income countries (LMIC), but the current literature shows that prevalence is consistently higher than in high-income countries( Reference Patel, Rahman and Jacob 2 ). This is thought to be concomitant with or exacerbated by poverty, gender inequity, anxiety, and familial and political instability( Reference Shidhaye, Mendenhall and Sumathipala 3 , Reference Lund, De Silva and Plagerson 4 ). In a systematic review focusing on LMIC, pooled prevalence for depressive symptoms was 16 % in the antenatal period (from thirteen studies), and 20 % in the postpartum period (from thirty-four studies)( Reference Fisher, Cabral de Mello and Patel 5 ).
Perinatal depression can have serious and long-term adverse effects on women and their children, and is therefore gaining attention in the international health community( Reference Patel, Rahman and Jacob 2 , Reference Walker, Wachs and Gardner 6 – Reference Howard, Piot and Stein 8 ). Consequences for women include poor self-care, compromised care-giving and increased morbidity from other causes, while for children, malnutrition, poor physical and cognitive development and increased illness have been reported( Reference Stewart 9 – Reference Stein, Malmberg and Sylva 12 ). Strategies to address perinatal depression are, however, less clear, ranging from pharmacological treatment to community-based support mechanisms and general poverty alleviation, and focus primarily on treatment, rather than on prevention( Reference Lund, De Silva and Plagerson 4 , Reference Rahman, Fisher and Bower 13 ).
Various biologically plausible pathways between nutrient levels and depression have been suggested( Reference Kaplan, Crawford and Field 14 ). Many essential nutrients, or compounds derived from such nutrients, are required for the synthesis of neurotransmitters and their modulation, and may therefore be involved in mood regulation( Reference Rechenberg and Humphries 15 , Reference Bodnar and Wisner 16 ). The biochemical role of nutrients in the nervous system is described in detail elsewhere( Reference Kaplan, Crawford and Field 14 , Reference Rechenberg and Humphries 15 , Reference Leung and Kaplan 17 ). Pregnancy and lactation place additional demands on a woman's body, and therefore nutrient deficiencies arise more easily during this time. Deficiency of nutrients during this critical period therefore may contribute to the increased risk of depression during the perinatal period. Hormonal shifts and lifestyle changes may in themselves increase the risk of perinatal depression, but may also contribute to changes in nutrient levels and could thus act through that pathway( Reference Burt and Stein 18 ).
Previous reviews limited the measures of nutritional status to one specific nutrient or class of nutrients, such as PUFA( Reference Freeman, Hibbeln and Wisner 19 ). Some explored depression in general (not limited to the perinatal period), and others were not systematic( Reference Leung and Kaplan 17 , Reference Makrides 20 ). One review on nutrient supplementation mixed prevention (in previously undiagnosed women) and treatment (in women already diagnosed with depression)( Reference Jans, Giltay and Van der Does 21 ). The present review includes published evidence on any nutrient, but the available studies focus on only a few out of the many important nutrients and phytochemicals that may be associated with perinatal depression.
Objective
We initially designed the present review to summarise the existing evidence from all analytical studies available on the association between nutritional status and perinatal depression in women. The results of the search highlighted two main ways to capture nutritional status: through blood levels (i.e. biomarkers) and through dietary intake measures, each with their particular strengths. Biomarkers are a precise, direct measure of nutritional status that account for bioavailability, while dietary intake data can easily capture a larger panel of nutrients and study the effect of whole diets, thus considering complex food interactions. Studies measuring dietary intake have been published in a separate review( Reference Sparling, Henschke and Nesbitt 22 ). The present review focuses on nutritional biomarkers and their link to perinatal depression.
Methods
Search strategy
We searched PubMed, EMBASE and CINAHL databases from 1966 to 1 June 2016 for publications in English. We used both medical subject heading terms and free text keywords in two separate searches to identify all relevant studies. The first search combined nutrition terms with maternal depression terms, while the second combined nutrition terms with depression terms and maternity terms separately (Fig. 1). All titles and abstracts identified by the search were screened by two independent researchers who then reviewed the full text of potentially eligible articles for inclusion.

Fig. 1. Search strategy. MeSH, medical subject headings; ti/ab, title or abstract.
Eligibility
We considered articles eligible if they were peer-reviewed and presented measures of association between nutritional biomarkers during or after pregnancy, and depression during pregnancy or up to 1 year postpartum. Analytical studies of any design were eligible for inclusion.
We included studies that evaluated nutritional biomarker levels using blood analysis. We excluded supplementation studies unless blood levels of nutrients were directly compared against perinatal depression. Studies that assessed hormones or other compounds synthesised by the body but not directly affected by dietary intake were not included.
We excluded studies in women who were already diagnosed with depressive symptoms or had other underlying health problems (e.g. HIV). Studies had to assess perinatal depression through a validated depression screening tool (i.e. Edinburgh Postpartum Depression Scale (EPDS); Center for Epidemiologic Studies Depression Scale (CES-D); Beck Depression Inventory; Mini International Neuropsychiatric Interview; twenty-item Self-Reporting Questionnaire; ten-item Kessler Psychological Distress Scale; Goldberg's Depression Scale; Symptom Checklist-90-R, or Kitgum Maternal Mood Scale; Postpartum Depression Screening Scale) or through clinical diagnosis from a trained interviewer; though we also allowed prescription of antidepressants as a proxy for a clinical diagnosis. Two common tools used to screen for depression, the CES-D and the Beck Depression Inventory, have often been used in pregnancy and postpartum as they do not emphasise somatic symptoms such as appetite changes and sleep disturbance. They have been found accurate in screening for both minor and major depression( Reference Tandon, Cluxton-Keller and Leis 23 ). The only screening tools that totally exclude somatic symptoms and are technically validated for the pregnancy and postpartum period are the EPDS and the Postpartum Depression Screening Scale. These have higher sensitivity than other tools( Reference Gaynes, Gavin and Meltzer-Brody 24 , Reference Beck and Gable 25 ) and we therefore assigned a lower risk of bias to studies using these tools.
Risk of bias assessment
In order to assess the methodological quality of each study, the Cochrane Collaboration tool( Reference Higgins, Altman and Gotzsche 26 ) was used to evaluate the risk of bias in the randomised controlled trials (RCT), while observational studies were evaluated using a modified version of the Quality in Prognostic Studies (QUIPS) tool( Reference Hayden, van der Windt and Cartwright 27 ). Two reviewers independently ranked each study as having high, medium/unclear or low risk of bias in each domain of the respective tools. The reviewers compared scores, disagreements were discussed and a consensus reached.
The Cochrane tool comprises the following six domains: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), and selective reporting (reporting bias).
While the QUIPS tool is designed to evaluate bias in prognostic studies, ‘risks’ in epidemiology are similar to ‘prognoses’. It comprises six domains: study participation, study attrition (replaced by response in cross-sectional studies and by selection of controls in the two case–control studies), prognostic factor (exposure) measurement, outcome measurement, confounding, and statistical analysis and reporting. Further details are provided in Supplementary Appendix S1.
Data extraction and synthesis
We used a standard form to extract characteristics and overall results from all included studies (Table 1). We also extracted information on the type of analysis performed and detailed results for all studies (Supplementary Appendix 2, Tables S1–S4). Studies that examined both B vitamins and Fe biomarkers are described in the two respective categories in the text, but presented as their own group in the tables in order to avoid duplication. Studies examined many different nutrients and their timing of exposure and outcome assessment varied widely. More importantly, several studies only reported linear depression outcomes (as opposed to the appropriate categorical outcome for screening tools), which precluded performing a meta-analysis of associations between nutritional biomarkers and perinatal depression without access to the original data. We therefore present a descriptive summary of the results and methodological quality of all included studies.
Table 1. Summary of studies evaluating associations between nutrients and perinatal depression*†‡§||
* Statistical terms: Adj. model, statistical analysis adjusted for potential confounding factors; N/A, not applicable; PCA, principal components analysis; RCT, randomised control trial.
† Depression terms: BDI, Beck Depression Inventory; CES-D, Center for Epidemiological Studies Depression Scale; DASS-21, Depression, Anxiety, and Stress Scales; EPDS, Edinburgh Postpartum Depression Scale; K-10, Kessler Depression Scale; PHQ-9, Patient Health Questionnaire Depression Module; PP, postpartum; preg, pregnancy; SCID-CV, Structured Clinical Interview; SCL-90-R, Symptom Checklist-90-Revised.
‡ Fe and blood terms: AGP, inflammatory marker 1-acid glycoprotein; CRP, inflammatory marker C-reactive protein; DW, distribution width; Fer, ferritin; Hct, haematocrit; MCH, mean corpuscular Hb; MCHC, mean corpuscular Hb concentration; MCV, mean corpuscular volume; MPV, mean platelet volume; PDW, platelet distribution width; sTfR, soluble transferrin receptors; TfS, free Fe and transferrin saturation.
§ Vitamins and minerals: A, retinol; B12, cobalamin; C, ascorbic acid; D, serum 25-hydroxyvitamin D; EFA, essential fatty acids; Hcy, homocysteine; MMA, methylmalonic acid.
ǁ Fatty acid terms: AA, arachidonic acid; ALA, α-linolenic acid; EDA, eicosadienoic acid; ETE, eicosatrienoic acid; HUFA, highly unsaturated fatty acids; LA, linolenic acid.
Results
Study inclusion and characteristics
From three databases, 5544 articles were identified after removing duplicates. Titles and abstracts were screened and 178 full-text articles were retrieved and checked against inclusion criteria. A total of thirty-five articles that used diet or intake measures to assess nutritional status were reviewed separately( Reference Sparling, Henschke and Nesbitt 22 ), while four articles fit inclusion criteria and were included in both reviews. We finally included twenty-four articles in this review, representing 14 262 participants from sixteen mainly high-income countries (Fig. 2).
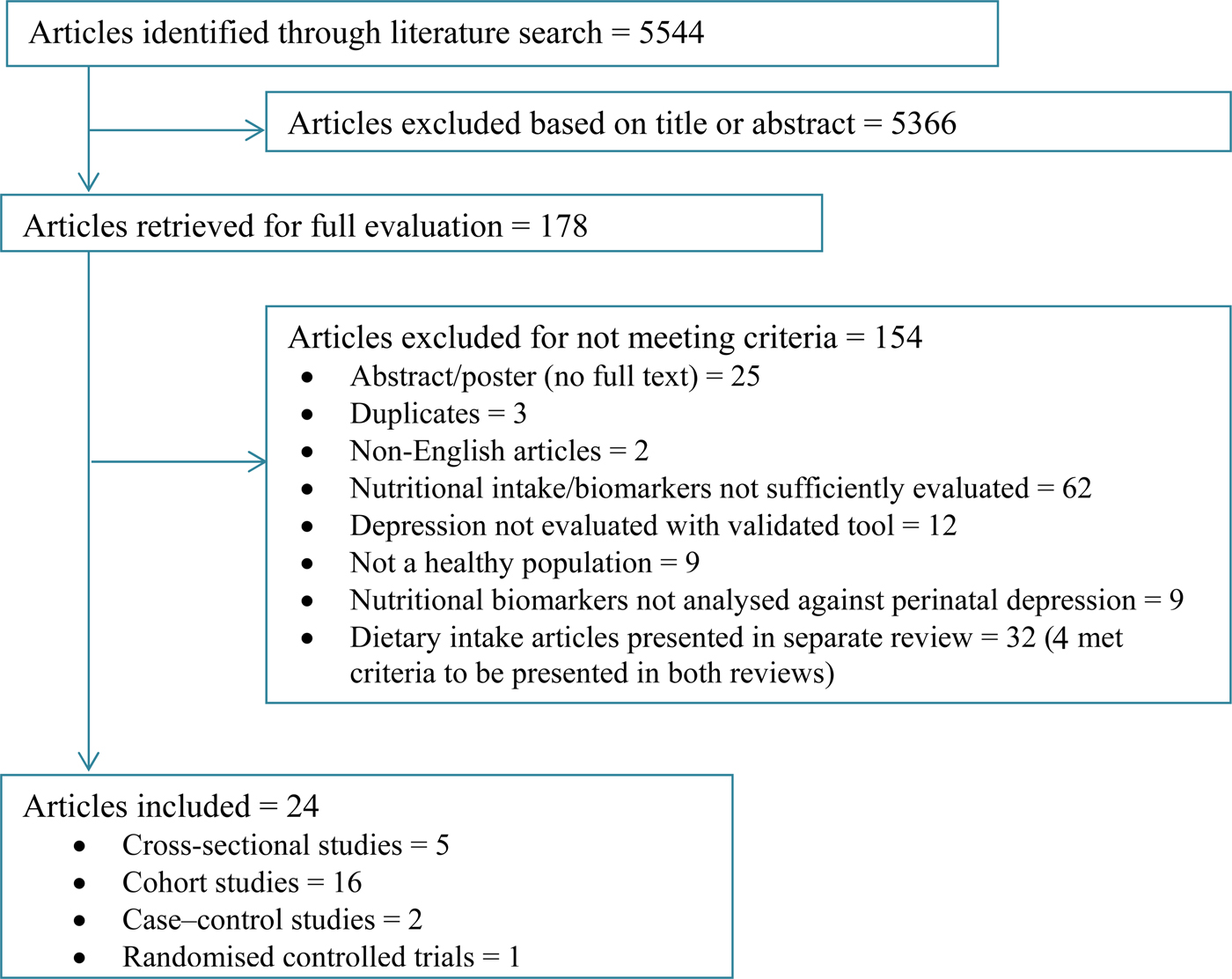
Fig. 2. Flowchart for inclusion of studies.
Studies were grouped in four categories according to the nutrients measured: (1) vitamins (four B vitamin studies – two of which also included Fe and are presented in that category as well, and ten vitamin D studies); (2) minerals (five Fe studies, one Se study and one Zn and Mg study); (3) fat and fatty acids (three studies assessing PUFA and one assessing lipoproteins and cholesterol); and (4) several essential nutrients (one study assessing major essential nutrients grouped by principal components analysis). In terms of study population, five studies used population-based prospective cohorts, seventeen recruited participants from hospitals or clinics, one was a population-based convenience sample( Reference Aubuchon-Endsley, Thomas and Kennedy 28 ), and one was a baseline assessment of an RCT( Reference Lukose, Ramthal and Thomas 29 ).
Of the studies, three used the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) Diagnoses (SCID-CV), and twenty used a screening tool, most commonly the EPDS (fifteen studies) or the CES-D (three studies). One study used filling a prescription for antidepressants as a proxy for clinical diagnosis. Most studies reported a prevalence of perinatal depression between 10 and 30 %, consistent with literature reviews( Reference Bennett, Einarson and Taddio 10 , Reference O'Hara and Wisner 30 ). Five studies found a depression prevalence over 30 % in their populations, of which three over 40 %( Reference Bae, Kim and Ahnv 31 – Reference Cassidy-Bushrow, Peters and Johnson 33 ), while three studies reported prevalences lower than 10 %( Reference Chong, Wong and Colega 34 – Reference Albacar, Sans and Martin-Santos 36 ). Two studies failed to report depression prevalence and another two could not estimate it as they used a case–control design( Reference Aubuchon-Endsley, Thomas and Kennedy 28 , Reference Mokhber, Namjoo and Tara 37 – Reference Rees, Austin and Owen 39 ).
Of the twenty-four included studies, sixteen reported the prevalence of nutrient deficiency for their nutrient of interest. Five reported that either none or a very small percentage (<5 %) of their study population was deficient( Reference Aubuchon-Endsley, Thomas and Kennedy 28 , Reference Bae, Kim and Ahnv 31 , Reference Bodnar, Wisner and Luther 40 – Reference Huang, Arnold and Qiu 42 ). Interestingly, the eight studies that found no association between nutritional biomarkers and perinatal depression included those five, and one further study that did not report its nutrient deficiency prevalence( Reference Watanabe, Suganuma and Hayashi 32 ).
The reported prevalence of nutrient deficiency was highest in the ten vitamin D studies. Using a common cut-off for vitamin D deficiency of 20 ng/ml and converting nmol/l to ng/ml, deficiency in the study populations ranged from 24 %( Reference Robinson, Whitehouse and Newnham 43 ) to 85 %( Reference Accortt, Schetter and Peters 44 ). In five studies examining Fe and Fe-deficiency anaemia, two (one American and one Korean) reported no deficiency or anaemia( Reference Aubuchon-Endsley, Thomas and Kennedy 28 , Reference Bae, Kim and Ahnv 31 ), while a study from India reported 30 % anaemia prevalence, based on Hb concentrations, without assessing ferritin concentrations or other markers that differentiate Fe-deficiency anaemia from other forms( Reference Lukose, Ramthal and Thomas 29 ). Another found 14 % Fe deficiency and 25 % Fe depletion in a Spanish population( Reference Albacar, Sans and Martin-Santos 36 ). One Japanese study on Fe did not present the prevalence of deficiency( Reference Watanabe, Suganuma and Hayashi 32 ). A Norwegian group suggested that being at <5 % of the omega-3 PUFA index could be indicative of a biological deficiency. Their population was categorised into percentiles, and 28 % (12/43) subjects were at or below 5·1 % of the PUFA index, which they hypothesise indicates deficiency in fatty acids( Reference Markhus, Skotheim and Graff 35 ). Eight studies did not report whether there were nutritional deficiencies in their populations.
Risk of bias assessment
All studies had potential sources of bias in at least one domain. We present the risk of bias of the five cross-sectional and two case–control studies in Fig. 3, and of the sixteen cohort studies in Fig. 4. Since there was only one RCT, we describe it in the text.

Fig. 3. Risk of bias assessment results for cross-sectional studies and case–control studies. * Case–control studies; +, low risk of bias; ?, unclear risk of bias; –, high risk of bias.

Fig. 4. Risk of bias assessment results for cohort studies. +, Low risk of bias; ?, unclear risk of bias; –, high risk of bias.
All of the cross-sectional and case–control studies had unclear or medium to high risk of bias in at least two domains, often because they failed to report crucial information. The domains ‘exposure measurement’ and ‘statistical analysis and reporting’ were those with the lowest risk of bias. Outcome measurement and confounding were most problematic, with only one study considered at low risk of bias in each of these domains. Even in adjusted models, four out of seven studies did not include important confounders.
The sixteen cohort studies had low risk of bias in exposure measurement, with one study using umbilical cord blood instead of maternal venous blood( Reference Gould, Anderson and Yelland 45 ). Outcome measurement introduced little bias for this study design; only two studies had medium risk of bias for using the CES-D as a screening tool( Reference Cassidy-Bushrow, Peters and Johnson 33 , Reference Brandenbarg, Vrijkotte and Goedhart 46 ). Eleven out of sixteen cohort studies had a low risk of bias in study participation, whereas five studies had potential bias in their sampling and selection of participants. Study attrition was the domain with the highest risk of bias, with only three studies having low risk of bias. Three cohort studies lost about half of their study population to follow-up( Reference Markhus, Skotheim and Graff 35 , Reference Mokhber, Namjoo and Tara 37 , Reference Accortt, Schetter and Peters 44 , Reference Wójcik, Dudek and Schlegel-Zawadzka 47 ). Of the eleven studies with over 10 % loss to follow-up, six failed to analyse differences between completers and non-completers, which meant they had high risk of bias in this domain. Only eight of sixteen studies adequately adjusted for confounders, while the remainder had a medium or high risk of bias due to their failure to account for variables such as history of depression, social or marital support, or basic demographic factors. Finally, in the domain of statistical analysis and reporting, twelve of the sixteen cohort studies had a low risk of bias as they clearly presented adjusted models with effect estimates, two studies had medium risk of bias for unclear reporting, and two others were considered at high risk of bias for failure to present adjusted models. The RCT by Mokhber et al.( Reference Mokhber, Namjoo and Tara 37 ) had low performance and detection bias, medium risk of selection and reporting bias, and high risk of attrition bias, with only 51 % of participants completing the trial.
Results from studies
Fourteen studies reported protective effects from higher (v. lower) nutrient levels (B vitamins, vitamin D, Fe, Se, Zn and PUFA): one cross-sectional study, one case–control study, eleven cohort studies and one RCT (see Table 1), three of which did not present an adjusted analysis( Reference Markhus, Skotheim and Graff 35 , Reference Wójcik, Dudek and Schlegel-Zawadzka 47 , Reference Gur, Gokduman and Turan 48 ). Two studies found that higher nutrient levels were associated with higher risk of depression( Reference Lukose, Ramthal and Thomas 29 , Reference Nielsen, Strom and Boyd 38 ). Eight studies, four cohort and four cross-sectional, found no statistically significant association between nutrient levels studied and perinatal depression in their main analysis (Table 1). All studies are described below in four categories, according to the nutrient groups examined.
Vitamins (Supplementary Appendix S2, Table S1)
There was little evidence for any association between folate or vitamin B12 and perinatal depression from the four included studies. Of the four studies, three had low risk of bias in at least three of the six domains( Reference Lukose, Ramthal and Thomas 29 , Reference Chong, Wong and Colega 34 , Reference Blunden, Inskip and Robinson 41 ). Chong et al.( Reference Chong, Wong and Colega 34 ) examined folate and vitamin B12 in a cohort in Singapore in the third trimester of pregnancy and measured depression at baseline and at 3 months postpartum. Vitamin B12 was not associated with depression at either time point. Increased folate levels were protective against depression in the antenatal assessment (OR 0·69 per standard deviation increase (95 % CI 0·52, 0·94); P = 0·02). However, at 3 months postpartum when including the antenatal depression score in the model, the relationship was weaker and no longer significant (OR 0·84 (95 % CI 0·62, 1·12); P = 0·25). An English cohort study assessed whether folate levels in the first trimester were related to depression at 6 and 12 months postpartum and found no association at either time point( Reference Blunden, Inskip and Robinson 41 ). In two cross-sectional studies, one from India and one from Japan, researchers found no association between B vitamins and perinatal depression( Reference Lukose, Ramthal and Thomas 29 , Reference Watanabe, Suganuma and Hayashi 32 ).
Evidence of a protective effect on perinatal depression was stronger for vitamin D, but not entirely consistent. Out of ten studies on the topic, four did not find a significant protective association in their main analysis (one had high risk of bias in several domains, one had medium risk of bias in several domains and one had low risk of bias in most domains). One study found no association( Reference Huang, Arnold and Qiu 42 ) and a small cohort study with high loss to follow-up found a borderline protective association (log-transformed continuous vitamin D levels, per unit: β = −0·21; P = 0·06)( Reference Accortt, Schetter and Peters 44 ). A large Australian study, within a PUFA trial, found no association overall, but within the control group at 6 weeks postpartum, vitamin D levels in cord blood were protective against depression (reference: <10 ng/ml; 10·1–20 ng/ml: risk ratio 0·35 (95 % CI 0·17, 0·69); >20 ng/ml: risk ratio 0·24 (95 % CI 0·12, 0·51)), with strong evidence for the interaction with treatment (P = 0·006)( Reference Gould, Anderson and Yelland 45 ). A Danish case–control study with low risk of bias reported that higher levels of vitamin D were associated with more depression( Reference Nielsen, Strom and Boyd 38 ).
The other six vitamin D studies not only reported protective associations but found linear trends between vitamin D concentrations and depression. A study from the Netherlands reported that for each 10 nm decrease in vitamin D concentration, there was a 5 % increase in risk of depressive symptoms, and for the most deficient category (≤29·9 nmol/l; ≤11·9 ng/ml), the adjusted OR was 1·48 (95 % CI 1·13, 1·95)( Reference Brandenbarg, Vrijkotte and Goedhart 46 ). This study had moderate risk of bias in three domains and low risk of bias in three domains. A Chinese cohort study with low risk of bias in five of six domains found a protective effect of vitamin D levels on postpartum depression (OR 0·81 (95 % CI 0·70, 0·92); P < 0·001)( Reference Fu, Liu and Tu 49 ). Two small studies, one Turkish and one American, both with high risk of bias in at least one domain, found higher vitamin D levels to be protective against depression( Reference Gur, Gokduman and Turan 48 , Reference Murphy, Mueller and Hulsey 50 ). Lastly, Robinson et al.( Reference Robinson, Whitehouse and Newnham 43 ) in an Australian cohort used a shortened EPDS and found that women in the lowest quartile of vitamin D levels (<18·8 ng/ml, similar to the deficiency level of<20 ng/ml) were at higher risk of depression at 3 d postpartum (OR 2·19 (95 % CI 1·26, 3·78); P = 0·006). This study ranked as having low risk of bias in five of six domains.
Minerals (Supplementary Appendix S2, Table S2)
Only one study assessed the relationship between Fe biomarkers and perinatal depression longitudinally. In a Spanish cohort with low risk of bias, Albacar et al.( Reference Albacar, Sans and Martin-Santos 36 ) showed that Fe deficiency (ferritin <7·26 µg/l) and Fe depletion (ferritin <12 µg/l) were both associated with higher odds of developing postpartum depression at 32 weeks (Fe deficiency: OR 3·73 (95 % CI 1·84, 7·56), P < 0·001; Fe depletion: OR 2·30 (95 % CI 1·29, 4·10), P = 0·005).
An American study and a Korean study examined Fe biomarkers and perinatal depression using cross-sectional designs and both generally had a high risk of bias. Neither study found protective associations of Fe (the first did not report deficiencies and the latter found no clinical anaemia) or presented an adjusted model( Reference Aubuchon-Endsley, Thomas and Kennedy 28 , Reference Bae, Kim and Ahnv 31 ). Two further cross-sectional studies examined Fe levels and depression in the first trimester (and also included B vitamin biomarkers). Watanabe et al.( Reference Watanabe, Suganuma and Hayashi 32 ) in Japan found no associations, and Lukose et al.( Reference Lukose, Ramthal and Thomas 29 ) in India found that anaemia was protective against depression in the first trimester (adjusted prevalence ratio 0·67 (95 % CI 0·47, 0·96); P = 0·03). The study by Lukose et al.( Reference Lukose, Ramthal and Thomas 29 ) was considered as having moderate risk of bias in three domains and low risk of bias in three domains, and Watanabe et al.( Reference Watanabe, Suganuma and Hayashi 32 ) only achieved a low risk of bias score in two of six domains.
A research team from Iran conducted a randomised trial supplementing women daily with Se for 6 months of pregnancy. They showed significantly higher Se blood levels and on average two points lower EPDS scores in the supplementation group (supplementation mean EPDS score: 8·8 (sd 5·1) v. placebo EPDS score: 10·7 (sd 4·4); P < 0·05)( Reference Mokhber, Namjoo and Tara 37 ). This study, however, had a high risk of bias due to incomplete outcome data (51 % completion) and unclear risk of bias in three other domains. Lastly, a team in Poland enrolled a small cohort of pregnant women (n 66), supplemented them with Zn and Mg and found a weak linear correlation between EPDS scores and Zn blood levels (r –0·2968; P = 0·01), but not Mg blood levels( Reference Wójcik, Dudek and Schlegel-Zawadzka 47 ). No adjusted model or effect size was reported and the study had high risk of bias in four out of six domains.
PUFA and fat (Supplementary Appendix S2, Table S3)
Three studies examined relationships between PUFA biomarkers and perinatal depression. A Brazilian cohort study showed that high v. low n-3 PUFA markers and low v. high n-6:n-3 ratios were protective against depression (EPA: OR 0·92 (95 % CI 0·86, 0·99); DHA: OR 0·96 (95 % CI 0·93, 0·99); DPA: OR 0·87 (95 % CI 0·77, 0·99); total n-3: OR 0·98 (95 % CI 0·96, 0·99); total n-6:n-3: OR 1·40 (95 % CI 1·09, 1·79)( Reference Pinto, Vilela and Farias 51 ). This study received a high risk of bias score in the study attrition domain due to high loss to follow-up with differences shown on baseline characteristics. They had low risk of bias in all other domains. Rees et al.( Reference Rees, Austin and Owen 39 ) in their case–control study with moderate to low risk of bias found that among many PUFA biomarkers, high DHA, high total n-3 PUFA and a low n-6:n-3 PUFA ratio were protective against depression (total n-3: OR 0·21 (95 % CI 0·05, 0·99, P = 0·05); DHA: OR 0·18 (95 % CI 0·04, 0·88, P = 0·03); n-6:n-3 ratio: OR 4·69 (95 % CI 1·00, 22·0, P = 0·05). Markhus et al.( Reference Markhus, Skotheim and Graff 35 ) in Norway examined a range of PUFA markers in a small cohort study (n 42) that had high risk of bias in three domains and low risk of bias in the other three. Using linear regression, they found an association between a low omega-3 index in pregnancy and EPDS score postpartum (β = 0·39; P < 0·01). In their Brazilian cohort, Teofilo et al.( Reference Teofilo, Farias and Pinto 52 ) measured both mean TAG and cholesterol levels (total cholesterol, LDL and HDL) and EPDS scores each trimester of pregnancy and found that higher HDL concentration was significantly associated with lower risk of antenatal depression in a linear mixed-effects model (β = −0·08 (95 % CI −0·157, −0·002); P = 0·04).
Multiple nutrients (Supplementary Appendix S2, Table S4)
The study by Bodnar et al.( Reference Bodnar, Wisner and Luther 40 ) was the only one to examine a number of major nutrients simultaneously, and used principal components analysis to create nutrient groups, or factors, in an American cohort. They identified three factors in women less than 20 weeks pregnant: essential fatty acids, micronutrients and carotenoids, and used a robust clinical diagnosis of depression in the second and third trimesters of pregnancy. They did not find statistically significant results after adjustment for covariates, but did find a crude association between carotenoids and depression (unadjusted: OR 0·40 (95 % CI 0·20, 0·90), P = 0·02; adjusted: OR 0·80 (95 % CI 0·30, 2·10), P = 0·67). Other micronutrients and essential fatty acids were not protective. This study had a low risk of bias in all domains except for study attrition and confounding, due to only 73 % of participants having full assessment data and not fully accounting for history of depression. Two other studies examining multiple micronutrients included Fe and B vitamins, and their results are thus discussed in their respective nutrient categories.
Discussion
Overall, there is inconsistent evidence for an influence of nutritional biomarker levels on perinatal depressive symptoms, with stronger evidence for certain nutrients. There is also not enough evidence to conclude that there is no link between nutrients and perinatal depression. Of twenty-four studies included, fourteen found protective effects of higher nutrient levels on perinatal depression, two studies reported higher nutrient levels were associated with a higher risk of perinatal depression, and the remaining eight studies found no association.
For vitamin D, there was inconsistent but stronger evidence for a protective effect, coming from more and higher-quality studies. Of ten studies on vitamin D, eight were prospective cohort studies, six showed significant protective effects, six had sample sizes over 200, and only two were of overall high risk of bias, one of which did not show any association. (Risk of bias scores are not meant to be collapsed, as heavy bias in even one domain can change study results. However, in the interest of interpretability, the risk of bias scores were combined into an overall bias assessment for the discussion. Any studies with high risk of bias in at least one domain were considered generally high risk of bias, if studies had low risk of bias in at least three domains with no high risk of bias scores, they were considered to have medium risk of bias, and studies with low risk of bias in four to six domains with no high risk of bias scores were considered to have overall low risk of bias.) For fats and PUFA there was some evidence for a protective effect, coming from one low risk of bias, medium-sized cohort study (n 238) examining HDL concentrations, and three high risk of bias studies addressing PUFA levels. Although only one of five studies examining Fe and perinatal depression reported a protective association, it was the only low risk of bias study in the group, a prospective cohort with sufficient power to detect an association (n 729). The remaining four studies on Fe were cross-sectional or case–control studies; one with medium sample size (n 365) and medium overall risk of bias and three with low sample sizes (<200) and high overall risk of bias.
Evidence on other minerals is weak due to single studies examining each distinct exposure. Three studies examined Se, Zn and Mg and found protective associations from higher nutrient levels and perinatal depression despite small sample sizes, but were of overall high risk of bias. One study with low risk of bias grouped many nutrients into factors and did not find any effect in adjusted analysis.
The evidence for a link between B vitamins and perinatal depression is also weak. However, the population source and/or methodology of studies may not have been suitable for detecting associations. Three of the four studies on B vitamins did not report the prevalence of nutrient deficiency and the fourth reported a low prevalence (<5 %). Two were cohort studies with overall low risk of bias, and two were cross-sectional and had medium or high risk of bias, one of which surprisingly found that anaemia protected from depression.
The weakness of the evidence base on this topic may thus be attributable to a paucity of studies and to methodological limitations of existing studies rather than an absence of true associations. We outline several methodological issues below which may offer some guidance for undertaking higher-quality studies in the future. Some practical methodological recommendations for future studies are presented in Table 2.
Table 2. Methodological recommendations for future studies
Exposure measurement
All studies measured nutrient biomarkers in the blood. While this can only capture a few biomarkers, it is generally a precise indicator of recent bioavailability. FFQ, on the other hand, measure whole diets and can thus capture complex synergies of ingested foods, but are imprecise and suffer from reporting bias( Reference Ioannidis 53 ). Studies using FFQ were reviewed separately( Reference Sparling, Henschke and Nesbitt 22 ). Four of the studies included in this review used both biomarkers and FFQ( Reference Lukose, Ramthal and Thomas 29 , Reference Bae, Kim and Ahnv 31 , Reference Watanabe, Suganuma and Hayashi 32 , Reference Blunden, Inskip and Robinson 41 ), which can potentially provide a more complete picture of nutritional status. However, only one of these four studies was of high quality and linked diets to blood levels. The population of this study showed no nutrient deficiency and the authors found no association with perinatal depression( Reference Blunden, Inskip and Robinson 41 ). More high-quality longitudinal studies on perinatal depression that measure both specific nutritional biomarkers and overall diets are needed.
The timing of exposure measurement is important for several reasons. Pregnancy and breastfeeding will deplete nutrient levels throughout the perinatal period, and levels measured at the beginning of pregnancy may thus not be comparable with nutrient levels around birth, even in the same woman( Reference King 54 ). Measuring all study participants at a similar time during pregnancy will remove this problem. Alternatively, one could control for gestational age at nutrient measurement. Time of measurement in pregnancy may be particularly important for water-soluble nutrients as their levels fluctuate more than fat-soluble ones( Reference Marangoni, Cetin and Verduci 55 , Reference Gernand, Schulze and Stewart 56 ). At a population level, however, fluctuations should not be problematic as long as the timing of measurement is more or less the same in the comparison groups. Currently, critical times of nutrient depletion have not been defined and the possible relationship of nutrient losses with depression is unclear, and therefore it is not possible to determine whether across studies, different measurement times in the course of pregnancy and lactation would produce different results. More fundamentally, given the potential for reverse causality (depressive symptoms leading to poor self-care and poor diet, or less time outdoors for vitamin D), it is important to measure nutritional biomarkers with sufficient lead-time until depression outcome measurement.
Outcome measurement
Clinical diagnosis of depression is the ‘gold standard’, but it is time-consuming and requires a trained clinician and is thus usually not feasible in large population studies( Reference Bennett, Einarson and Taddio 10 ). Various screening tools have been developed that show good reliability, sensitivity and specificity depending on the cut-off point, and have been adapted to many different languages and cultural contexts( Reference Gibson, McKenzie-McHarg and Shakespeare 57 , Reference Hewitt, Gilbody and Brealey 58 ). For example, a cut-off point of ≥13 on the EPDS has been shown to have a sensitivity of 0·91 (95 % CI 0·84, 0·99) and a specificity of 0·91 (95 % CI 0·88, 0·94) for postpartum depression( Reference Hewitt, Gilbody and Brealey 58 ). Only two tools exclude all somatic symptoms of pregnancy and have been validated specifically for the perinatal period: the EPDS and the Postpartum Depression Screening Scale( Reference Noble 59 ). Three (15 %) of the twenty-four included studies used a clinical interview (sometimes in combination with a screening tool), and nine (45 %) used the EPDS (one a shortened version), while the remaining eight (40 %) used tools that may not produce valid results in the perinatal period.
Having a history of mental disorders (including depression) is a known risk factor for perinatal depression, and antenatal depression is a risk factor for postpartum depression( Reference Norhayati, Hazlina and Asrenee 60 ). Eleven (55 %) of the twenty-four reviewed studies failed to take baseline depression or history of depression into account in their analysis. This can potentially confound the relationship of interest since previous depressive symptoms are likely to have a negative influence on self-care and diets and thus on nutritional status( Reference Stuart-Parrigon and Stuart 61 ). Failing to account for (recent) depressive history could thus lead to spurious associations.
Other sources of bias
Many studies included in the present review suffered from weaknesses in design and reporting, often in more than one domain. Eleven (55 %) of the studies had limited power to detect an effect due to small sample size (<200), which makes null findings difficult to interpret. In the two case–control studies and one cross-sectional study that found an association (out of seven with these designs), reverse causality cannot be ruled out as a possible explanation. The same is true for some cohort studies where lag time between exposure and outcome measurement was very short, the lowest being 3 weeks( Reference Brandenbarg, Vrijkotte and Goedhart 46 ).
The large cohorts generally described enrolment and follow-up protocols in detail (such as Blunden et al.( Reference Blunden, Inskip and Robinson 41 ) and Cassidy-Bushrow et al.( Reference Cassidy-Bushrow, Peters and Johnson 33 )), but several of the other studies did not (such as Pinto et al.( Reference Pinto, Vilela and Farias 51 )), making it difficult to judge risk of bias. Thirteen studies (54 %) did not include important potential confounders, such as basic sociodemographic variables, and thus may have overestimated the strength of the association. In the special case of vitamin D, the compound can be ingested through foods or synthesised by the human body if skin is exposed to sunlight. Sunlight exposure also has a proposed direct link to depression outside the dietary intake pathway( Reference Barnard and Colón-Emeric 62 ). Hence, any nutritional analysis of vitamin D should adjust for sunlight exposure or a proxy thereof. Lastly, statistical model building and reporting was unclear in some studies, which made it difficult to interpret the results and assess the evidence.
Most of these studies were observational (since blood nutrient concentrations cannot be directly increased) and suffered from several limitations, which can explain some inconsistencies in the results. A recent review on the relationship between dietary intake and supplementation with perinatal depression similarly found that there was inconclusive evidence of an association between certain diets and foods with perinatal depression. The strongest PUFA experimental study in the previous review found no effect on depression, but other trials also on PUFA did find an association. Taken together, the evidence from both reviews suggests that, although not definitive, higher v. lower concentrations of PUFA may be protective against depression( Reference Sparling, Henschke and Nesbitt 22 ), but would require further investigation. Most trials focus on one nutrient or supplement combination, rather than diets as a whole. In the previous review on diets and supplementation, observational studies also generally found a protective effect from healthier or Mediterranean diets as a whole( Reference Sparling, Henschke and Nesbitt 22 ).
Prevalence of nutritional deficiency
Sixteen of twenty-four studies included in the present review are from high-income countries where nutrient deficiencies are relatively rare( Reference Gernand, Schulze and Stewart 56 ). Three others were undertaken in Turkey, Brazil and Iran, which are upper-middle-income countries( Reference Mokhber, Namjoo and Tara 37 , Reference Gur, Gokduman and Turan 48 , Reference Teofilo, Farias and Pinto 52 ), and one study came from India, a lower-middle-income country( Reference Lukose, Ramthal and Thomas 29 ). In higher-income settings, there may be insufficient variation in nutrient levels and too few participants in the clinically deficient range to detect an association. For example, Blunden et al.( Reference Blunden, Inskip and Robinson 41 ) reported no associations with perinatal depression when examining folate in a setting where 96 % of the women reported taking folic acid supplements during pregnancy, and the prevalence of folate deficiency was below 5 %. Studies from low-income countries, where nutritional deficiencies are still widespread and more severe, would therefore have a much better chance to establish this relationship( Reference Patel, Rahman and Jacob 2 , Reference Fisher, Cabral de Mello and Patel 5 ).
Vitamin D deficiency is common in many populations around the world, including in high-income countries( Reference Holick and Chen 63 ). Insufficiency in the study populations of the reviewed articles ranged from 24 %( Reference Robinson, Whitehouse and Newnham 43 ) to 85 %( Reference Accortt, Schetter and Peters 44 ). Higher prevalence of deficiency provided more power to detect an association with perinatal depression, and indeed, for vitamin D, the evidence of an association with perinatal depression was most convincing. There is also evidence in the literature of an association between vitamin D and depression in general, i.e. not just in the perinatal period( Reference Ju, Lee and Jeong 64 ).
Practical implications
While there is an emerging body of evidence on the treatment of perinatal depression with PUFA( Reference Ellsworth-Bowers and Corwin 65 ), there has been little research so far on prevention. Prevention strategies can be broader than treatment strategies, as they work ‘upstream’ of the problem and can address several risk factors and outcomes concomitantly. The Lancet series on perinatal mental health in 2014 highlighted risk factors for perinatal depression including low socio-economic status, trauma, domestic violence, lack of support, migration status, history of psychopathology, and chronic illness and medical problems( Reference Howard, Molyneaux and Dennis 66 ). Some treatment options (and to a lesser extent prevention strategies) proposed in LMIC are embedded within complex interventions that have health and economic components related to nutrition( Reference Rahman, Fisher and Bower 13 , Reference Howard, Molyneaux and Dennis 66 ). Understanding the root causes of perinatal depression, including the role of nutrition, may encourage a shift from treatment to prevention, and targeting these root causes might simultaneously alleviate other adverse health outcomes. Developing prevention strategies could also reduce the need for treatment options, which are often inaccessible to women in LMIC( Reference Mendenhall, De Silva and Hanlon 67 ).
Strengths and limitations
We gathered all available evidence on whether blood levels of different nutrients are associated with perinatal depression. We considered both antenatal and postpartum depression, which traditionally have been separated( Reference Howard, Piot and Stein 8 , Reference O'Hara and Wisner 30 ). Previously, the focus has been on postpartum depression, but evidence is emerging that antenatal depression is both common unto itself and a risk factor for postpartum depression( Reference Patel, Rodrigues and DeSouza 68 – Reference Husain, Bevc and Husain 70 ) and should thus no longer be ignored. Because of the heterogeneity of both the exposure and the outcome classification, a meta-analysis was not possible, but we provide a narrative synthesis of evidence on the topic.
A limitation of the present review is that it may suffer from publication bias. Studies finding null results are less likely to be published in English-language scientific journals and we did not include other languages or grey literature. However, we did identify six studies that reported no significant associations (B vitamins, vitamin D, Fe, and all nutrients grouped in principal components analysis) and two studies that reported high nutrient levels (B vitamins) or anaemia as risk factors for perinatal depression, contrary to expectation. Furthermore, there may be many more unknown relationships between nutrients other than those in the present review and perinatal depression, which have yet to be examined and thus are not part of this synthesis.
Conclusions
This synthesis of available evidence suggests that blood levels of certain nutrients potentially play a role in the development of perinatal depression, but results are inconsistent and we lack confidence in effect estimates. The evidence appears to be stronger for vitamin D compared with B vitamins or minerals. However, many studies exhibited serious methodological limitations, and in several nutrient categories only one study of poor quality was available, reducing the ability to draw robust conclusions. These findings are similar to what we found when reviewing studies on the influence of dietary intake and supplementation on perinatal depression. While overall inconclusive, there was some evidence that perinatal depression is linked to certain diets and foods( Reference Sparling, Henschke and Nesbitt 22 ). To strengthen the evidence base on this topic, robust longitudinal studies are needed from settings with higher prevalence of nutritional deficiencies that ideally measure both specific nutritional biomarkers and overall diets.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/jns.2017.58
Acknowledgements
The authors are sincerely thankful to the German Ministry of Education and Research (BMBF) who supported this research. T. M. S. and S. G. are funded by a grant (award number 01ER1201) from BMBF. We acknowledge the financial support of the Deutsche Forschungsgemeinschaft and Ruprecht-Karls-Universität Heidelberg within the funding programme Open Access Publishing. The content of this publication is solely the responsibility of the authors.
T. M. S. proposed the concept and conducted the search. S. G. and N. H. advised on concept and scientific decisions. N. H., R. C. N. and T. M. S. screened titles, abstracts and full-text articles for inclusion, and each participated in the risk of bias assessment. T. M. S. led the review process and the writing of the manuscript. S. G. led the editing process, and all authors read, edited and approved the final manuscript.
There were no conflicts of interest.









 Open access
Open access