



Introduction
The coronavirus (severe acute respiratory syndrome coronavirus-2; SARS-CoV-2) pandemic has resulted in an increased incidence of acute respiratory distress syndrome in the adult population, with around a third of patients admitted to intensive care in 2020.Reference Abate, Ahmed Ali, Mantfardo and Basu1 These patients often require long admissions, with high ventilatory requirements. Mean length of stay was up to 16 days in England in the early stages of the pandemic.Reference Shryane, Pampaka, Aparicio-Castro, Ahmad, Elliot and Kim2 Subsequently, intensive care units have faced higher than usual demand for extended periods of mechanical ventilation.Reference Meister, Pandian, Hillel, Walsh, Brodsky and Balakrishnan3 Prolonged mechanical ventilation is associated with a high risk of ventilator-acquired pneumonia, a requirement for high-dose intravenous sedation, neuromuscular deconditioning, subglottic stenosis, longer intensive care stays and increased mortality.Reference Young, Harrison, Cuthbertson and Rowan4
Tracheostomy can be performed to aid in ventilator weaning. This decreases airway dead space, reduces airway resistance and lessens the work of breathing, resulting in more rapid ventilator weaning.Reference Añón, Araujo, Escuela and González-Higueras5 Further advantages include improved tracheobronchial toilet, reduced sedative requirements and a lower frequency of subglottic stenosis, all of which contribute to a shorter intensive care unit stay.Reference Livneh, Mansour, Kassif Lerner, Feinmesser and Alon6–Reference Gosling, Bose, Gomez, Parikh, Cook and Sarge9 The insertion of a tracheostomy can be performed via a percutaneous or open surgical approach. The optimal timing for tracheostomy in coronavirus disease 2019 (Covid-19) patients remains a matter of debate.Reference Polok, Fronczek, van Heerden, Flaatten, Guidet and De Lange10
The rise in numbers of critically ill Covid-19 patients requiring prolonged ventilation has resulted in a proportional increase in tracheostomy procedures.Reference Meister, Pandian, Hillel, Walsh, Brodsky and Balakrishnan3,11 A recent review reports an increase in the tracheostomy rate from 8–13 per cent to 16–61 per cent.Reference Williams and McGrath12
Despite the benefits, tracheostomy can be a high-risk procedure. Coronavirus disease 2019 patients are often too unstable to tolerate a tracheostomy until weeks into their illness because of acute respiratory distress syndrome. Proning, along with high fraction of inspired oxygen and high positive end expiratory pressure requirements, mean that tracheostomy may be relatively contraindicated early in a patient's disease course. Thus, the procedure often may not be performed until 15 days or more following intubation, which itself may be almost 2 weeks into the patient's illness.Reference Battaglini, Missale, Schiavetti, Filauro, Iannuzzi and Ascoli13
During the first wave of the pandemic, concerns over exposing staff to aerosolised Covid-19 particles through tracheostomy insertion further delayed the procedure until viral load in secretions had decreased.Reference Gosling, Bose, Gomez, Parikh, Cook and Sarge9,Reference Al Omari, Al-Ashqar, Alabd Alrhman, Nuseir, Allan and Alzoubi14 The percutaneous technique is thought to reduce aerosolisation; however, open surgical tracheostomy may be required in light of anatomical considerations, staff availability or failure of the percutaneous procedure.Reference Schultz, Morvan, Fakhry, Morinière, Vergez and Lacroix15
Additionally, given the increased risk of thromboembolic phenomena in Covid-19, patients often receive high doses of anti-coagulation, putting them at further risk of complications.Reference Gosling, Bose, Gomez, Parikh, Cook and Sarge9 Patients have also been noted to have a high secretion burden with acute respiratory distress syndrome in Covid-19, with viscous secretions putting them at risk of ‘plugging off’ with subsequent tracheostomy obstruction.Reference Gosling, Bose, Gomez, Parikh, Cook and Sarge9
To the authors’ knowledge, an in-depth review of tracheostomy complications in Covid-19 has not yet been conducted. This scoping review therefore aimed to summarise the existing literature surrounding complications from tracheostomy insertion in these patients.
Research question
What are the complications encountered when performing tracheostomy in Covid-19 patients, and how might these differ from those in non-coronavirus patients?
Aims
These are: (1) to evaluate tracheostomy complications in Covid-19 patients, through a review of existing literature; (2) to compare complication rates between percutaneous and open surgical tracheostomies, and perform meta-analysis if adequate data are collected; and (3) to assess the availability of literature comparing Covid-19 with non-coronavirus tracheostomy complications.
Materials and methods
Medline and Embase databases were searched in November 2021. The Medical Subject Headings (used for Medline) were: ‘Tracheostomy’, ‘Postoperative Complications’, ‘COVID-19’ and ‘SARS-CoV-2’. The Emtree headings (used for Embase) were: ‘Tracheostomy’, ‘Postoperative Complication’, ‘Coronavirus Disease 2019’ and ‘Severe Acute Respiratory Syndrome Coronavirus 2’ (Table 1).
Table 1. Breakdown of literature search
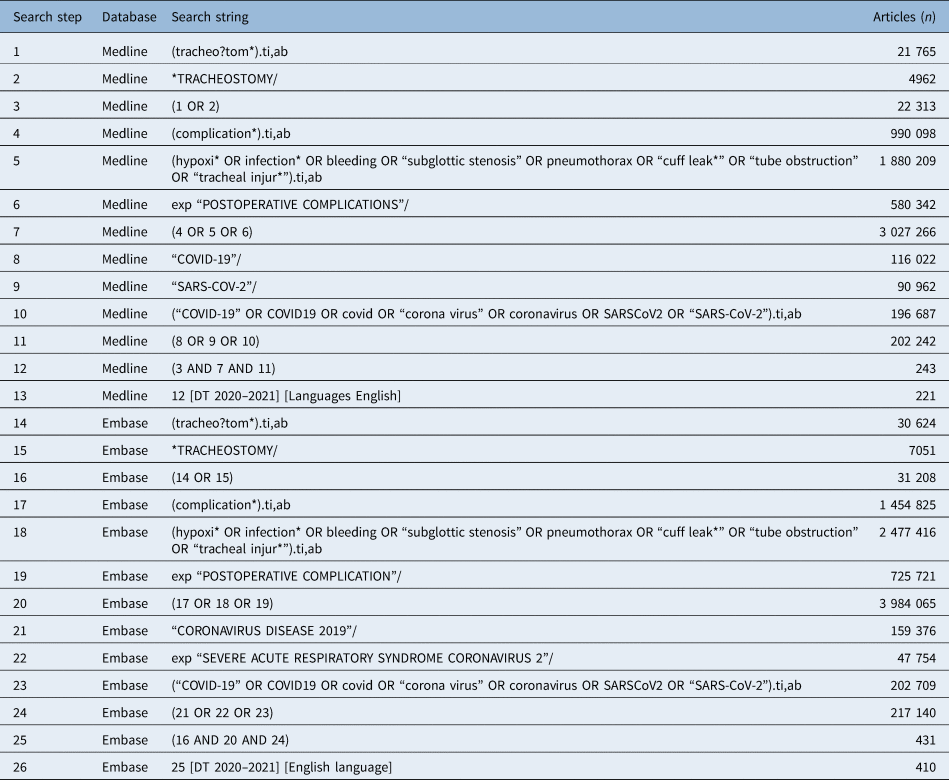
The Medical Subject Headings (used for Medline) were: ‘Tracheostomy’, ‘Postoperative Complications’, ‘COVID-19’ and ‘SARS-CoV-2’. The Emtree headings (used for Embase) were: ‘Tracheostomy’, ‘Postoperative Complication’, ‘Coronavirus Disease 2019’ and ‘Severe Acute Respiratory Syndrome Coronavirus 2’.
Duplicate results and conference abstracts were removed. Results were limited to English-language papers and to articles published during the height of the Covid-19 pandemic (November 2019 to December 2021). Papers were subsequently removed by screening the abstracts; studies were excluded if they included paediatric patients, if Covid-19 was not the primary reason for admission and if tracheostomy was performed for other indications than to facilitate ventilatory weaning (e.g. in acute airway obstruction). Case reports were excluded. The full texts of remaining papers were screened prior to analysis for the review, and were excluded if they did not comment on complications of tracheostomy procedures. Systematic reviews and guidelines were excluded from the analysis, but utilised for background information. Reference lists of included studies were used for background information. Figure 1 shows the article search breakdown.

Fig. 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (‘PRISMA’) diagram.
Following full-text screening, data were extracted into a dedicated Microsoft™ Excel® spreadsheet to record: date of publication, country of publication, time from intubation to tracheostomy, type of tracheostomy performed and complications resulting from the tracheostomy procedure.
Differences in complication rates between percutaneous and open surgical tracheostomy were analysed using a significance level of 95 per cent. Data for each complication were expressed in a 2 × 2 contingency table, in which rows indicated percutaneous or open surgical approaches, and columns indicated whether a complication occurred or did not occur. Pearson's chi-square test of independence was performed to examine the relation between each complication and tracheostomy method for those studies that reported complications by tracheostomy type.
Reporting is in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (‘PRISMA’) extension for scoping reviews 2018. A scoping review approach was selected given the novelty of this area, and the lack of randomised, controlled trials to date. An outline of the literature has been presented, to identify key areas for future research.
Results
Of 85 papers for which full texts were screened, 61 were included in the review (Figure 1). All papers were published between April 2020 and December 2021, and were either prospective or retrospective observational studies, with a combination of single- and multi-centre studies. The majority of studies were from Europe or the USA; a breakdown is shown in Table 2. The studies included in the analysis are shown in Table 3. A meta-analysis was not performed as there were no randomised, controlled trials identified in the search.
Table 2. Breakdown of studies by continent

Table 3. Studies included in review

Fifty-six studies (91.8 per cent) reported the average time of intubation prior to tracheostomy, either mean or median. For the 30 papers (49.2 per cent) reporting the mean, time from intubation to tracheostomy was 18 ± 6 days.
In total, 7117 tracheostomies were performed. One large study did not report tracheostomy technique. In the remaining 60 studies (98.3 per cent), 2979 percutaneous or hybrid tracheostomies, and 3442 open surgical tracheostomies, were performed. From the 7117 tracheostomy procedures, a total of 1330 procedure-related complications were reported (18.7 per cent of procedures). Eleven studies (18.0 per cent) did not specify tracheostomy type when reporting complications. The summary of reported complications is shown in Table 4. Table 5 shows the rate of complications for percutaneous and open surgical tracheostomies for those studies that reported complications by tracheostomy technique.
Table 4. Complications by tracheostomy type

Table 5. Complication rates by type of procedure performed

*P-value attained following Pearson's chi-square analysis. n/a = not applicable
Analysis revealed that percutaneous tracheostomy was higher risk than open surgical tracheostomy with respect to post-operative bleeding, false passage and pneumothorax; however, open surgical tracheostomy carried a higher risk for peri-operative hypoxia. The remaining complications demonstrated no difference between percutaneous and open surgical techniques.
Three studies (4.9 per cent) compared tracheostomy in Covid-19 patients to a control group without Covid-19. One of these studies found an increased incidence of tracheal injuries in Covid-19 patients.Reference Bertini, Forfori, Bruschini, Corradi, Ribechini and Brogi16 The second of these studies found a significantly increased risk of bleeding in Covid-19 patients (20.3 per cent vs 5.97 per cent), but with no difference in length of hospital stay.Reference Mesalles-Ruiz, Hamdan, Huguet-Llull, Penella, Portillo and Bagudà17 The final of these studies reported an increased time from intubation to tracheostomy in Covid-19 patients (25.4 days vs 22.9 days).Reference Reis, Castelhano, Gani, Almeida and Escada7
Discussion
This review identified bleeding as the most common complication in Covid-19 tracheostomies, occurring in 9.2 per cent of all procedures. This is higher than the 6 per cent rate demonstrated prior to Covid-19, as reported in the 2014 National Confidential Enquiry into Patient Outcome and Death report on tracheostomy patient outcomes.Reference Wilkinson, Freeth and Kelly18 This report accounted for both surgical and percutaneous tracheostomies.
Bleeding accounted for 658 of the total complications (49.5 per cent) in this review. Post-operative bleeding was approximately five times more common than peri-operative bleeding. This is reasonably consistent with a 2021 systematic review of 31 studies encompassing 3479 Covid-19 tracheostomies, which found bleeding to account for 52.5 per cent of procedure-related complications.Reference Ferro, Kotecha, Auzinger, Yeung and Fan19 This paper was not a dedicated study of complications, and therefore the complication frequency was not discussed extensively. In addition, this study did not compare bleeding risk of percutaneous versus open surgical tracheostomies, and did not compare with procedures performed in non-coronavirus groups.
It is likely that high-dose prophylactic or treatment dose anti-coagulant medications received by Covid-19 patients contributed to the higher risk of bleeding.Reference Carfora, Spiniello, Ricciolino, Di Mauro, Migliaccio and Mottola20 Coronavirus disease 2019 patients are at high risk of thromboembolic disease because of immobility, increased levels of clotting factors and endothelial dysfunction. The incidence of venous thromboembolism in Covid-19 intensive care patients has been reported as up to 28 per cent.Reference Jiménez, García-Sanchez, Rali, Muriel, Bikdeli and Ruiz-Artacho21
Despite this, recent literature suggests that the benefits of therapeutic level anti-coagulation in hospitalised patients with severe Covid-19 are outweighed by risk of bleeding. Therefore, therapeutic dose anti-coagulation could be avoided in Covid-19 intensive care patients, which would potentially decrease the risk of tracheostomy related bleeding.Reference Wahid and Ortel22,23 The UK's National Institute for Health and Care Excellence currently recommends above prophylactic dose low molecular weight heparin only in patients with a low oxygen requirement, unless as part of a research trial.24
Another potential reason for increased bleeding risk in Covid-19 patients is frequent suction due to high secretion load, which increases the risk of mucosal bleeding.Reference Gosling, Bose, Gomez, Parikh, Cook and Sarge9
Somewhat surprisingly, this review found that Covid-19 patients undergoing percutaneous tracheostomy are at higher risk of bleeding than those undergoing an open surgical procedure. Literature prior to the pandemic demonstrates no difference in bleeding rates between percutaneous and surgical tracheostomies.Reference Johnson-Obaseki, Veljkovic and Javidnia25,Reference Brass, Hellmich, Kullmer, Ladra and Ladra26 This includes a 2016 Cochrane review, albeit acknowledging low quality of evidence.Reference Brass, Hellmich, Kullmer, Ladra and Ladra26
It is unclear why the contradiction observed in this review is demonstrated in patients with Covid-19. It is possible that the availability of electrocautery in open surgical procedures reduces the probability of bleeding in a high-risk population. Furthermore, in the preliminary months of the pandemic, open surgical tracheostomies were commonly performed by senior surgeons, given concerns about the aerosolisation risk to staff.Reference Broderick, Kyzas, Sanders, Sawyerr, Katre and Vassiliou27 As a result, it is possible that more meticulous haemostasis was ensured, in comparison to the non-coronavirus literature, where tracheostomies are performed by operators with varied levels of experience. Finally, anti-coagulation is commonly suspended prior to surgical tracheostomy to reduce risk of bleeding.
The second most common complication identified in this review was peri-operative hypoxia, occurring in 123 out of 7117 patients (1.73 per cent). There was discrepancy in the studies in terms of hypoxia definition, with most defining it as oxygen saturations below 80 per cent or 90 per cent for a specified time period of up to 5 minutes. This is almost three times the rate found in a pre-coronavirus multi-institutional analysis from 2012,Reference Halum, Ting, Plowman, Belafsky, Harbarger and Postma28 and twice that found in the previously mentioned National Confidential Enquiry into Patient Outcome and Death report.Reference Wilkinson, Freeth and Kelly18 The higher baseline rate of complications may be partially the result of patients with higher body mass index in intensive care unit during the Covid-19 pandemic, and an increased risk of hypoxia in this cohort.Reference Cordes, Best and Hiatt29
Several causes of hypoxaemia have been described in Covid-19 cases. These include intrapulmonary shunting, reduced regulation of lung perfusion, pulmonary intravascular microthrombi and poor diffusion capacity, all contributing to higher oxygen requirements and the risk of peri-procedural desaturation.Reference Dhont, Derom, Van Braeckel, Depuydt and Lambrecht30
Furthermore, in light of the difficulty in reducing ventilatory requirements to a desirable level, some institutions were keen to perform a tracheostomy when ventilatory requirements were higher than perhaps would normally be accepted in a non-coronavirus patient. This resulted in episodes of decompensation during the apnoeic period, when the ventilator was paused to facilitate the creation of a tracheal window, and subsequent desaturation. In order to address this, some authors have suggested a trial of apnoea in the intensive care unit after pre-oxygenation with fraction of inspired oxygen of 100 per cent. In the absence of being able to tolerate such a trial, it can be argued that tracheostomy should be deferred until the patient's ventilatory requirements have reduced.Reference McGrath, Brenner, Warrillow, Pandian, Arora and Cameron31
This review demonstrated a higher risk of hypoxia when an open surgical technique was used. Over the course of the pandemic, various consensus guidelines have been released for the provision of safe surgical tracheostomy in Covid-19.Reference Schultz, Morvan, Fakhry, Morinière, Vergez and Lacroix15,Reference Jones, Gendre, Walshe, Walsh, Glynn and Lacy32,Reference Shivnani, Raman and Amle33 Such protocols have all shared the recommendation to pause ventilation during the creation of the tracheal window, to minimise aerosolisation during this high-risk step of the procedure. This may explain the difference found in this review, reflecting a higher risk of hypoxia during open surgical tracheostomies than during percutaneous tracheostomies. This is not consistent with the 2016 Cochrane review in non-coronavirus patients, which demonstrated no difference.Reference Brass, Hellmich, Kullmer, Ladra and Ladra26
Other complications found to significantly differ in rate between percutaneous and open surgical tracheostomy techniques were false passage and pneumothorax. Both of these were more common using the percutaneous technique. However, overall rates of these complications were low, at 0.08 per cent and 0.2 per cent respectively. Pneumothorax in itself appears to be high risk in Covid-19 patients, but is not necessarily linked to poor prognosis.Reference Martinelli, Ingle, Newman, Nadeem, Jackson and Lane34 Other complications with very low numbers were subglottic stenosis and fistula. Most studies did not follow up subjects for long enough to determine the true rate of subglottic stenosis, and this is anticipated to be a phenomenon described in forthcoming studies.Reference Scholfield, Warner, Ahmed and Ghufoor35
The expected increase in tracheostomy tube obstruction due to mucus plugging in Covid-19 patients was not demonstrated in this review, with a rate of only 0.18 per cent. This is much lower than the rate of 2.5 per cent reported in the National Confidential Enquiry into Patient Outcome and Death tracheostomy report.Reference Wilkinson, Freeth and Kelly18 This report included late obstruction occurring on the critical care unit or the ward in this figure, which may partially account for the discrepancy. The same is true for displacement, with a rate of 0.59 per cent here versus 4.1 per cent in the report.
This review has several limitations. Most importantly, all of the studies identified by the search are retrospective or prospective observational studies. The lack of randomised, controlled trials means that meta-analysis was not possible, and the heterogeneity of the studies makes statistical analysis difficult to interpret.
Additionally, it is difficult to comment on long-term complications of tracheostomy, as most studies did not include long-term follow up after the study period, with the total study period usually being between one and two months. Only one study specifically assessed the airway at the follow-up clinic. This means that the true numbers of long-term complications, such as subglottic stenosis and granulomas, are likely to be higher than reported here.
A third limitation is the failure of some studies to break down complications by tracheostomy technique. This potentially skews the analysis comparing complications of percutaneous tracheostomy with those of an open surgical approach. In addition, some studies only reported specific complications, such as bleeding and hypoxia, and there may have been other complications not reported in the write-up.
Finally, there is difficulty in locating matched studies involving non-coronavirus patients, in order to compare Covid-19 and non-coronavirus complication rates. Since the start of the pandemic, the vast majority of tracheostomy research has pertained only to patients with Covid-19, with a paucity of comparative studies published.
Further research is required to fully investigate the increased risk of tracheostomy complications in Covid-19 patients, and to determine the validity of the observed differences between percutaneous and open surgical tracheostomy procedures.
An accurate meta-analysis of complications requires randomised, controlled trials. This is not necessarily practical in this cohort, as choice of tracheostomy technique is often precluded by the availability of qualified staff and other factors such as anatomical considerations. In order to obviate this, a large, multi-centre cohort study comparing matched intensive care unit patients with and without Covid-19 would be useful, that more precisely delineates factors associated with complications in patients undergoing tracheostomy.
Conclusion
Several complications are observed following open surgical and percutaneous tracheostomy in Covid-19 patients. The overall rates of these complications appear to be increased, as compared to non-coronavirus patients, particularly with regard to post-operative bleeding and peri-operative hypoxia. There are also differences between open surgical and percutaneous complication rates that are not seen in non-coronavirus patients.
There are a paucity of high-quality, randomised, controlled trials required to draw these conclusions. Further research is needed to fully investigate the increased risk of tracheostomy complications in Covid-19 patients, in order to determine the true risk of complications. Authors should routinely report tracheostomy technique, anti-coagulation status and rates of all the complications discussed in this review. It would be helpful to include long-term follow up and airway assessment of tracheostomy patients, to accurately determine the risk of these complications.
Specific considerations must be made when considering Covid-19 patients for tracheostomy, and awareness of the commonly seen complications is an important factor in this decision.
Acknowledgement
Thanks are extended to Ms C Goodin, National Health Service Support Librarian at Charing Cross Campus Library, for her valuable assistance with the literature search.
Competing interests
None declared






