



SARS-CoV-2 (COVID-19) has posed an unprecedented and major public health emergency throughout the world, and India is no exception to that. By the end of July 2021, about 32 million individuals have acquired the infection in the country, including about half a million active cases and 0.4 million fatalities. 1 Health care workers (HCWs) have contributed substantially to address this health crisis, often working beyond their usual physiological and psychological capacities, which have predisposed them to various psychological problems apart from contracting the COVID-19 infection. Reference Iyengar, Jain and Vaishya2,Reference Misra3
Literature from India from the first wave of the pandemic (2020) suggests that at least one-third to half of HCWs suffered from at least a moderate level of anxiety, depression, stress, and posttraumatic stress symptoms or event-related stress symptoms (ERSS). Reference Biswas and Biswas4,Reference Gupta, Prasad and Dixit5 Our previous work has also found that a sizeable proportion of the HCWs during the first wave suffered from psychological problems, namely depression (39.01%), anxiety (38.03%), stress (24.61%), and Event Related Stress Symptoms or post-traumatic stress symptoms (refers to ERSS/PTSS) (n = 69, 27.54%) during the first wave (April–July 2020).Reference Purwar, Jahan and Gautam 6 Furthermore, as high as one-third of the HCWs had negative attitudes toward the COVID-19 pandemic like reporting considerable levels of work-related stigma, lacking reliance on the personal protective equipment (PPE), and negative beliefs like uncontrollability over the patient’s condition.Reference Purwar, Jahan and Gautam 6 Additionally, regression analysis showed that being female, married, working as junior doctors, or supporting staff (vs nursing staff), and a higher level of perceived stigma, lesser reliance on PPE, and belief of uncontrollability over the patients’ condition had a higher likelihood of experiencing psychological problems.Reference Purwar, Jahan and Gautam 6
Research from various pandemics (SARS, 2003; Middle East respiratory syndrome, 2012; Swine flu, 2009, etc) suggests that HCWs are at higher risk for various psychological problems, which are determined by their level of knowledge and attitude toward the pandemic (perceived stigma, vigor, etc), ongoing socio-economical upheavals, Reference Gupta and Sahoo7–Reference Maunder, Hunter and Vincent9 and their coping methods. Reference Aguilera and Messick10,Reference Greenglass11
Furthermore, research suggests that nurses and allied staff (or supporting staff) experience greater psychological problems during a pandemic as compared to the clinicians; this has been attributed to a greater level of knowledge, clinical skills, and sense of controllability over the situation, and so forth, among the clinicians. Reference Purwar, Jahan and Gautam6–Reference Tan, Chew and Lee13 Literature pertaining to the pandemic (including emerging literature on COVID-19) highlights the awareness program about the psychological problems among the HCWs, better communication/support system in the hospital, including mental health support system, rotation-wise duties ward/intensive care units, tele-counseling services, peer-support system, and so forth, have a positive effect on the mental health of the HCWs. Reference Gupta and Sahoo7 Literature from Asia-Pacific nations and Canada, especially during the SARS (2003), has revealed that, with time, the level of psychological problems among the HCWs comes down due to acquisition of adaptive coping, better awareness about the condition, greater support from the authorities as well as from society and family, and so forth. Reference Maunder14–Reference Su, Lien and Yang16
The severity and course of the COVID-19 infection have differed substantially across the two waves (first wave, 2020; the second wave, 2021) of the pandemic in India. Reference Jain, Iyengar Karthikeyan and Vaishya17 Similarly, socio-political situations and health system preparedness of the country also varied across the two waves of the pandemic. For instance, during the first wave, the public, as well as HCWs, had lesser awareness about the course and outcome of the pandemic. Also, HCWs had lesser technical skills in dealing with the condition. These could be attributed to the evolving nature of the infection, lack of evidence-based treatment, constraints about availability of PPE, unavailability of vaccinations, and so forth. COVID-19-related morbidity and mortality were lesser during the first wave. In contrast, the second wave resulted in greater infliction of young-middle adults, higher rate of secondary infection, greater hospitalizations, and limited availability of the hospital beds and oxygen cylinders. Reference Jain, Iyengar Karthikeyan and Vaishya17
The government’s preparedness and response also accordingly varied across the two waves. Reference Jain, Iyengar Karthikeyan and Vaishya17 For instance, during the first wave, the government focused more on increasing awareness among the public through the digital platform, including providing self-help tools; arranging PPE and preparing COVID-19 management guidelines; providing financial or health-related benefits to the HCWs; and exploring options for the vaccine, and so forth. Reference Maunder14,Reference Su, Lien and Yang16,Reference Busch, Moretti and Mazzi18–Reference Koh, Lim and Chia20 In contrast, the second wave being more catastrophic necessitated the government to deploy greater HCWs and hospital resources in COVID-19 care, upscaling hospital beds and vaccination drive, arranging lifesaving medications and oxygen, and so forth.
To cater to the needs of the public and respond to the government’s call, the services of our institute also differed across the two waves of the pandemic (likewise of other tertiary-care hospitals across the country). During the first wave, our hospital was providing regular services alongside the COVID-19 services and not all HCWs were deployed in COVID-19 care; however, during the second wave, the hospital was converted into a dedicated COVID-19 treatment center and all HCWs were deployed in COVID-19 care.
Despite literature suggesting the COVID-19 pandemic had different attributes across the two waves (2020, first wave; 2021, second wave), little is known about its impact on the attitude and level of psychological problems among the HCWs. Reference Jain, Iyengar Karthikeyan and Vaishya17,Reference Asrani, Eapen, Hassan and Sohal21 Investigating these changes can help the public health experts, hospital infection control and disaster management committee, and policy-makers to come up with specific measures that would be customized to the different cadre of HCWs and contextually robust (eg, attitudinal factors like stigma, uncontrollability about the situation, helplessness).
Therefore, the current study was aimed to compare the level of psychological problems among the HCWs across two waves of the COVID-19 pandemic.
The primary objective of the study was to compare the level of depression, anxiety, stress, and posttraumatic stress symptoms/event-related stress symptoms (PTSS/ERSS) among the HCWs and their attitudes toward work and COVID-19 across the two waves of the COVID-19 pandemic. Additionally, it investigates the change in their psychological problems across the two waves based on their job profile.
Materials and Methods
Study Design and Setting
The current study was a comparative cross-sectional observational study that was carried out at a government-funded, tertiary care teaching hospital in central India. Participants were recruited during two separate waves of the COVID-19 pandemic (first wave: April–July 2020; second wave: April–July 2021) when the country was confronting the COVID-19 pandemic and the health care system was overwhelmed. 22
Study Participants and Selection
All the HCWs (doctors and nurses, henceforth, frontline HCWs), and the allied staff/supporting (henceforth, allied HCWs) who were working in the hospital and were willing to provide informed consent were eligible for the study. However, those not on hospital duty during the study periods, and who had known psychiatric diagnoses were excluded from the study. It must be highlighted here that for the current study, it was not mandatory that only those participants who participated in the first wave of the pandemic be recruited as participants in the second wave. Therefore, the participants across the two waves may differ.
Data Collection
The study was conducted through a hybrid model (online survey using Google Forms as well as offline). Invitations for participation in the study were sent through email and WhatsApp to all the HCWs of the hospital. Participant information sheets and informed consent forms were appended in the invitation.
However, in a subset of the participants (mainly allied staff) who were not comfortable with the online responses, information was collected through in-person interviews (offline) by one of the co-investigators (DG), and the same was filled in Google Forms. It usually required 5–7 minutes for the participants to respond to the survey questionnaire.
Ethical Considerations
The anonymity and confidentiality of participants were assured; the data was kept secured and only the investigators had access to it. Further, their participation in the study was purely voluntary, and they had all the rights to withdraw from the study at any time without fear of retribution. Also, it had been ensured that those who were later found to have significant psychological problems were intimated about it and offered mental health support. The study has the approval of the research review board and institutes’ human ethics committee (LOP IM026).
Outcome Measures
A semi-structured questionnaire
It inquired about age, gender, marital status, current living arrangements, professional details (experience, designation), COVID-19 work-related details (work area, level of involvement in patient care [screening or treatment], days since last COVID-19 duty), and presence of any psychiatric illness, or other condition, of the participants.
Attitude Toward COVID-19 Questionnaire (ATCQ)
The attitude and psychological attributes of the HCWs toward the COVID-19 pandemic were assessed using five items that were derived from the available literature, the current context of the COVID-19 pandemic in the country, including those locally relevant, and the experiences of the authors who were part of the hospital COVID-19 support system (ARR and MK) and infection control board (SP). Reference Gupta and Sahoo7,Reference Maunder14,Reference Rajkumar23 The questionnaire items related to: (1) working as HCW during COVID-19 causing stress, (2) preoccupation with COVID-19 outside the workplace, (3) perceived stigma (being treated differently by society because of the nature of the job), (4) decreased reliance over the PPE (fear of contracting COVID-19 despite working with the adequate PPE gears), and (5) uncontrollability over the patients’ clinical condition (feeling that patients’ current medical condition and the outcome are beyond one’s control; applied only for frontline HCWs). The questionnaire, however, has been developed for the current study during the first wave of the pandemic and was not validated in the study population.
Depression, Anxiety, and Stress Scale—21 Items (DASS-21)
It is a self-reported instrument (21 items) that comprises three subscales: depression, anxiety, and stress, each having seven items. The scoring for each item ranges from 0 (does not apply to me at all) to 3 (applied to me very much or most of the time). The score for each item is multiplied by 2 to get the final score for each sub-scale (total score range: 0–42). The scores are categorized into “normal,” “mild,” “moderate,” “severe,” and “very severe.” Its Hindi version is also available, which was used among the supporting staff. Reference Lovibond and Lovibond24
Impact of Event Scale-Revised (IES-R)
It is a short, self-administered tool whose score correlates better with the Diagnostic and Statistical Manual (DSM) criteria for Post-Traumatic Stress Disorders (PTSD). It has 22 items that assess the events of the past week (recent period). It also has Likert scoring: 0 = Not at all; 1 = A little bit; 2 = Moderately; 3 = Quite a bit; 4 = Extremely. A score > 24 represents PTSS/ERSS of clinical concern. Reference Beck, Grant and Read25
Statistical Analysis
Descriptive statistics were used to describe participants’ demographic and professional characteristics. Continuous data were represented by mean (standard deviation) or median (interquartile range), while categorical variables were represented as percentages (frequencies). The comparison between the participants of two groups (first and second wave, representing independent variables) was performed by a chi-square test and unpaired t-test for the categorical (including variables of outcome measures) and continuous variables, respectively. A two-sided (P < 0.05) was considered statistically significant. Polytomous variables were dichotomized if the groups were too heterogeneous for comparison (eg, categories of depression sub-scale of DASS-21 have been dichotomized into normal/absence of depression and presence of depression). The statistical analyses were carried out using the licensed Statistical Package for the Social Sciences (SPSS), version 21 (IBM Corp, Armonk, NY). 26
This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline. Reference Benchimol, Smeeth and Guttmann27
Results
A total of 322 of 1720 HCWs in the first wave (response rate = 18.7%) and 345 of 2009 HCWs in the second wave (response rate = 17.1%) responded to the survey invitations. However, only 305 and 325 respondents in the first and second waves, respectively, were found to be eligible for the study (details of participants recruitment depicted in Figure 1).
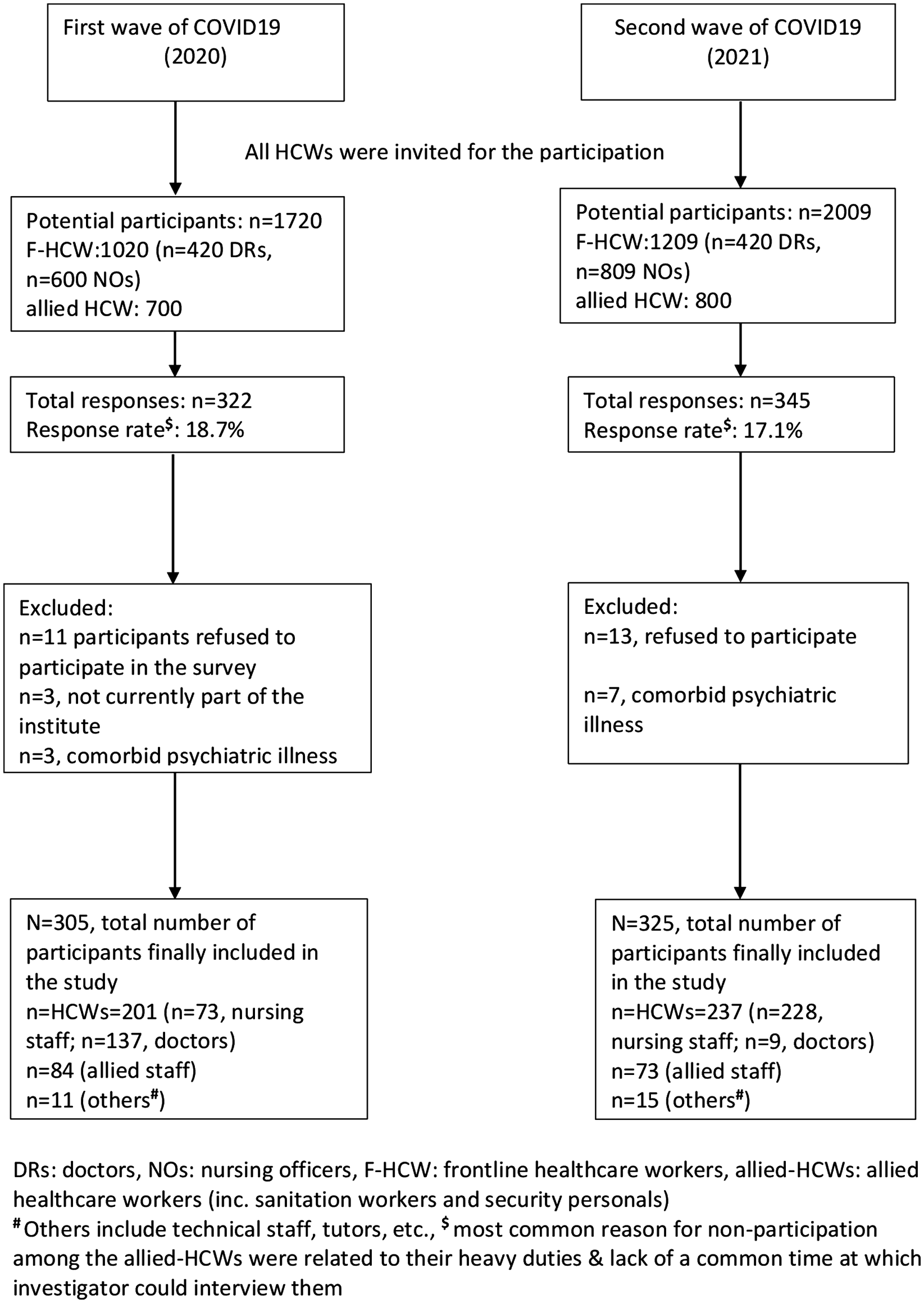
Figure 1. Flow chart depicting process of participant recruitment.
Sociodemographic and Professional Characteristics of the Participants
More than half of the participants were of age < 30 years across both the waves (first vs second wave: 187 [61.3%] vs 191 [55.8%]), with a slight male preponderance (174 [57%] vs 167 [51.4%]). A significantly higher proportion of participants in the second wave compared to the first wave was married (210 [64.6%] vs 150 [49.2%], P < 0.01) and staying with their family members (193 [59.9%] vs 146 [49.9%], P = 0.04). Similarly, participants of the second wave have greater professional experience (2.0 [1.0, 4.9] vs 3.0 [2.0, 5.0], P < 0.01), lesser duration of duty off since their last COVID-19 duty (20.0 [6.0, 99.0] vs 2.0 [1.0, 30.0], P < 0.01), and proportionally higher active involvement in patients care (244 [75.1] vs 87 [27.6], P < 0.01) compared to the first wave (Table 1). Furthermore, the proportion of the frontline HCW (doctors and nurses) did not differ across the two study periods (237 [72.9%] vs 87 [68.4%], P = 0.26); however, the relative proportion of the nurses in the second wave versus the first wave was much higher (166 [69.9%] vs 42 [20.0%], P < 0.01).
Table 1. Socio-demographic profiles of the participants

# χ 2 (df): chi-square value (degree of freedom).
Include separated, divorced, and in a live-in relationship (2020, n = 4; 2021, n = 5).
†† log10-transformation was done as the dependent variables were strongly skewed (value ranging from 2.8 to 4.4); ‘t’ indicates mean difference of the log10-transformed values.
§ Rest did not disclose their gender (2020, n = 4; 2021, n = 0).
§ § HCW: nurses, medical interns, postgraduate trainees, and trained doctors; allied HCW: Dietician, Security Guard, Housekeeping; others include technicians, research staff, other teaching staff (2020, 11 [3.7]; 2021, 15 [4.6]) who were not included in the comparative analysis.
Comparison of Attitude Toward Work and COVID-19 Pandemic, and Level of Psychological Problems Among HCWs
There were no significant differences (P = 0.14–0.40) between the two groups in terms of proportion of the participants with “considerable/large degree” of preoccupation with COVID-19 outside the workplace (72 [22.2%] vs 83 [27.2%]), fear of contracting infection despite wearing PPE (72 [22.2%] vs 90 [29.5%]), and uncontrollability over the patient’s clinical condition (70 [21.5%] vs 81 [26.6%]).
However, the proportion of the participants experiencing “considerable/large degree” work-related stigma (74 [22.8%] vs 90 [29.5], P = 0.054, marginally significant) and work-related stress (219 [76.8] vs 237 [89.8], P < 0.05) was a lesser of the second wave compared to the first wave (Table 2).
Table 2. Comparison in the scores of the health care workers (frontline and allied-HCWs combined) (2020 vs 2021) on the measures of the psychological outcomes

# χ 2(df): chi-square value (degree of freedom).
DASS21: depression, anxiety, and stress scale 21 item; IES-R: impact of event scale-revised (PTSD, reflecting event-related stress-symptoms).
† Neutral responses were not included in the analysis, hence, total n < total no. of participants.
§ For the purpose of analyses the polytomous groups have been dichotomized.
Significantly lesser proportions of participants of the second wave had depression (33 [9.6%] vs 136 [42.2%], P < 0.05), anxiety (56 [16.3%] vs 133 [41.3%], P < 0.05), stress (23 [6.7%] vs 97 [30.1%], P < 0.05), and ERSS (93 [27.0%] vs 101 [31.2%], P < 0.05) (see Table 2).
Subgroup Analysis of the Frontline HCWs and Allied HCWs
On subgroup analysis, the levels of depression, anxiety, stress, and ERSS were lower among the participants of the second wave (vs the first wave). However, there were no significant differences between the two groups concerning their attitudes toward the COVID-19 pandemic and work (Table 3).
Table 3. Subgroup analysis comparing the scores of the frontline health care workers (2020 vs 2021) on the measures of the psychological outcomes

# χ 2 (df): chi-square value (degree of freedom).
† Total n is less than the total number of the participants in the given group as remaining participants had “neutral” reply.
†† Fisher’s exact test applied.
When only allied HCWs were considered, significantly lesser proportion of the participants of second wave reported considerable/large degree of work-related stress (40 [62.5%] vs 77 [100%]), preoccupation with COVID-19 outside the workplace (28 [38.4%] vs 55 [65.5%]), and fear of contracting an infection (33 [45.2%] vs 52 [61.9%]). However, these differences were not significant concerning the work-related stigma (47 [64.4%] vs 60 [71.4%], P = 0.34) (Table 4).
Table 4. Subgroup analysis comparing the scores of the allied health care workers § (2020 vs 2021) on the measures of the psychological outcomes

# χ 2 (df): chi-square value (degree of freedom).
§ Allied HCW includes the housing staff (security guards, sanitation workers, etc).
† Total n is less than the total number of the participants in the given group as remaining participants had “neutral” reply.
Item no. 5 in attitude questionnaire is not applicable for the allied HCW.
†† Fisher’s exact test applied.
Discussion
The present study was conducted to assess and compare the level of psychological problems (depression, anxiety, stress, and ERSS) and attitudes toward work and COVID-19 among the HCWs (both frontline as well as allied HCWs) of India, across two waves of the pandemic, separated by an interval of one year (2020 and 2021). To the best of our knowledge, this is among the first studies from across the globe, including India, that have investigated the change in psychological problems and attitudinal attributes of the HCWs across the different waves of the COVID-19 pandemic and compared them.
We found a significant decline in all the parameters of psychological problems (depression, anxiety, stress, ERSS) among the HCWs during the second wave of the pandemic (vs first wave). This observation persisted across a different cadre of HCWs, both the frontline as well as allied HCWs, who were equally, if not more, prone to various psychological problems due to limited knowledge about the pandemic and various psycho-social vulnerabilities. These findings are consistent with the literature on previous pandemics. Reference McAlonan, Lee and Cheung15,Reference Li, Ge and Yang28,Reference Wu, Fang and Guan29 Literature suggests psychological problems of HCWs during the pandemic improve over time; these are attributed to adaptive coping skills, better family and social support, Reference Su, Lien and Yang16 greater awareness about the pandemic, tangible support from the hospital authorities, availability of the standard infection control and treatment protocol, availability of vaccines, and so forth. Reference Busch, Moretti and Mazzi18 In the present study, the improvement in psychological problems and attitudes toward work and the COVID-19 pandemic among the HCWs in the second wave could be understood considering the greater awareness among the HCWs about the COVID-19 pandemic, greater family supports (significantly higher proportions of the participants of the second wave were staying with their family members). Similarly, the availability of standard infection control and treatment protocols, greater professional experience of the HCWs, and positive impact of getting vaccinated (which were available at large in the second wave) might have contributed to lessening the psychological problems among the HCWs. However, more research, particularly of a qualitative nature, is required to assess the nuances associated with this change.
Although we found a significant reduction in the work-related stress (item 1. Working as HCW during COVID-19 causes stress) and stigma (item 4. I am treated differently because of my work), as assessed on the ATCQ, among the participants of the second wave, their other attitudinal attributes remained the same.
The improvement in work-related stress and stigma shows that HCWs, in general, might have developed better coping skills to deal with the ongoing stress. Moreover, greater awareness about the problems, tangible support at the workplace, both from colleagues and higher authorities, and support from the government in the form of various health insurances, advance payment of salary, and so forth, might also have contributed to these improvements. However, these findings require further exploration.
In contrast, non-significant improvement in attitudes of the HCWs like preoccupation with COVID-19, fear of contracting infection, and uncontrollability over the patients’ conditions, could be understood in the light of a greater number of HCWs being actively involved in providing COVID-19 care and had lesser days since last post-duty offs. Thus, HCWs may fear acquiring and transmitting the infection to their family members, getting overwhelmed by the higher COVID-19 positivity rate and mortality rate, compounded by the scarcity of the hospital beds and lifesaving medications, thereby, maintaining a negative attitude on these domains. Reference Jain, Iyengar Karthikeyan and Vaishya17,Reference Asrani, Eapen, Hassan and Sohal21
On subgroup analysis, however, the attitudinal attributes of the frontline HCWs (doctors and nurses), as per the responses on ATCQ, remained the same across the two waves. These reflect that frontline HCWs might have experienced greater work-related stress and fear of acquiring infection and transmitting it to others. These factors may likely have contributed to maintaining stigma. Furthermore, the sense of uncontrollability over the patients’ conditions can be understood in light of higher COVID-19-related complications and mortality. Reference Imad and Kwatra30–Reference Schmidt-Sane32 Moreover, in this study, the differential proportions of the nurses and doctors across the two waves might have resulted in this observation. Literature suggests that nurses experience a greater level of psychological problems as compared to doctors, who might have greater awareness, technical skills, and a higher sense of controllability over their work and patients’ condition. Reference Gupta and Sahoo7,Reference Su, Lien and Yang16,Reference Kang, Ma and Chen33 However, the cross-sectional nature of the study precludes us from drawing any firm conclusion. Thus, more studies, especially of qualitative nature, are required to investigate the nuances behind it.
On subgroup analysis involving the allied staff, a significant positive attitudinal change (on ATCQ) was seen except in work-related stigma. These findings highlight that the positive impact of COVID-19-related awareness and standard operating protocols, family support, vaccination, and so forth, was greater among allied HCWs compared to the frontline HCWs. It must be underscored here that allied HCWs, who mainly represent contractual and low-paid workers in India, were harder hit by the COVID-19 pandemic and experienced various adverse socio-economic consequences due to job losses of their family members and out-of-pocket expenses for the treatment of the COVID-19 infection and its complications. Reference Gupta and Sahoo7,Reference Cabarkapa, Nadjidai, Murgier and Ng34 This calls for a tailored support system, including mental health interventions to address the attitudinal issues of the allied staff, which often gets overlooked. However, as mentioned above, these nuances need to be further explored to draw any firm conclusion.
Surprisingly, we found that likewise of the frontline HCWs, allied HCWs did not report any significant change in their levels of work-related stigma. A similar mechanism as highlighted for the frontline HCWs (higher COVID-19 positivity and mortality rate, fear of transmitting the infection to others, etc) might have contributed to this. Reference Imad and Kwatra30,31 Such mechanism needs to be investigated further.
Limitations of the Study
First and foremost, the participants of the two waves were not the same. This acts as a major limitation as different participant populations at different points of time may have different concerns, hence likely to have a different psychopathologies. Therefore, the findings on the current study may be influenced by this difference. A future study must explore the difference in psychological concerns of the participants using the same set of participants.
Second, the heterogeneity in the proportions of the doctors and nurses, representing the frontline HCWs, across the two waves, might have affected some of the study findings. Therefore, clubbing them under the category of frontline HCWs rather than independently assessing their psychological problems and attitudinal attributes might have confounded some of the results. Third, there were some differences in the socio-demographic (gender, age, staying with family, etc) and clinical profiles (professional experience, days since last COVID-19 duty, etc) of the participants across the two waves. However, we did not systematically analyze the interaction of these variables with other independent variables on the outcome measures. The survey was based on the self-reporting on part of the participants, which has the potential to color the actual differences, for which a clinical interview-based assessment might have been more useful. Also, the dichotomization (into normal/absence or presence) of multi-nominal (normal, mild, moderate, severe, very severe level of psychological problems) outcome variables of DASS-21 AND IES-R might have missed the important ordinal aspects of the psychological problems and attitudinal attributes. Furthermore, the questionnaire used to assess the attitude of the participants was not validated in the target population; therefore, its findings could raise concerns.
Conclusion
The present study found that as compared to the first wave of the COVID-19 pandemic, HCWs in the second wave of the pandemic experienced a lesser level of depression, anxiety, stress, and event-related stress symptoms. Furthermore, HCWs during the second wave experienced lesser work-related stress and stigma. However, these findings slightly differed on sub-group analysis with no significant attitudinal difference across the two waves in the frontline HCWs and a more positive attitudinal change among the allied HCWs. The better psychological profile of the HCWs for the second wave can be an outcome of higher professional experience of the HCWs of the second wave, greater awareness about the illness and its treatment, tangible support from the authorities, impact of vaccination, greater family support, support from the society, and better coping skills. The above findings highlight the positive impact of better administrative, familial, and social support on the psychological health of the HCWs. Moreover, there could be a subset (cadre) of the health care workforce who need tailored occupational and mental health supports to cope with the psychosocial stress put forth by such a pandemic. More research, particularly of qualitative nature, interview-based, and employing validated instruments for assessing the attitudes of the HCWs, is warranted to investigate the nuances and determinants of change in the psychological and attitudinal attributes of the HCWs across different waves of the COVID-19 pandemic and to make suitable organizational and mental health support system changes in the hospital.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/dmp.2022.192
Data availability statement
The data associated with the current research can be obtained from the corresponding author (SP) upon reasonable request.
Author contributions
All the authors have contributed significantly to the research work that has resulted in this paper. They all have contributed significantly to preparing this manuscript and taking responsibility for the content of the manuscript.
SG: Methodology, analysis, draft preparation
DB: Draft preparation
SP: Study methodology, draft review
LP: Data collection and draft review
ARR: Study methodology, draft review
MK: Study methodology, draft review
RJ: First draft preparation
DG: Data collection
Conflict(s) of interest
None of the authors has any association with any commercial sector or any agency that could be construed as a potential conflict of interest regarding the current research work. Authors declare no conflicts of interest pertaining to this research work.







