



Borderline personality disorder (BPD) is a debilitating mental health disorder characterized by patterns of instability across emotional, behavioral, cognitive, and interpersonal domains (Courtney-Seidler et al., Reference Crowley, Wu, Molfese and Mayes2013; Lieb et al., Reference Lieb, Zanarini, Schmahl, Linehan and Bohus2004). Epidemiological studies have found that BPD can affect approximately 0.5 to almost 6% of the general adult population, with 1-2% being more commonly reported (Crowell et al., Reference Crowell, Beauchaine and Linehan2009; Leichsenring, et al., Reference Leichsenring, Leibing, Kruse, New and Leweke2011; Lieb et al., Reference Lieb, Zanarini, Schmahl, Linehan and Bohus2004). Historically, BPD was not diagnosed in individuals under 18 years of age. However, the DSM-5, and national treatment guidelines in the United Kingdom and Australia, have legitimized the diagnosis of BPD in adolescents by removing the previous age requirement (of 18+ years) (American Psychiatric Association, 2013; Chanen et al., Reference Chanen, Sharp and Hoffman2017; Sharp & Wall, Reference Sharp and Wall2018). Previous research illustrates that BPD symptoms typically peak in late adolescence at around 14 to 17 years of age (Courtney-Seidler et al., Reference Crowley, Wu, Molfese and Mayes2013; Paris, Reference Paris2014). As well, the presence of BPD symptoms in middle adolescence have been shown to be predictive of a BPD diagnosis later in middle adulthood (Winograd et al., Reference Winograd, Cohen and Chen2008).
BPD in Adolescents
Prevalence rates of BPD in adolescent samples approximate that of the adult literature, ranging from 1-3% (Kaess et al., Reference Kaess, Brunner and Chanen2014; Sharp & Wall, Reference Sharp and Wall2018). Although clinical studies report higher prevalence rates of female vs. male individuals with BPD (approximately 3:1), epidemiological and community studies do not show substantial sex differences in the prevalence of BPD in adult or child–adolescent populations (Kaess et al., Reference Kaess, Brunner and Chanen2014; Zanarini et al., Reference Zanarini, Horwood, Wolke, Waylen, Fitzmaurice and Grant2011). The clinical presentation of BPD is similar in adolescents and adults, with both being highly comorbid with disorders like major depressive disorder (Bradley et al., Reference Bradley, Zittel Conklin and Westen2005; Zanarini et al., Reference Zanarini, Frankenburg, Dubo, Sickel, Trikha, Levin and Reynolds1998). The stability of adolescent BPD is similar to that of adults as well, showing moderate consistency of symptoms over time, with substantial fluctuations in response to situational factors, and a gradual reduction in symptoms over time (Bornovalova et al., Reference Bornovalova, Hicks, Iacono and McGue2009; Chanen et al., Reference Chanen, Jackson, McGorry, Allot, Clarkson and Yuen2004; Conway et al., Reference Conway, Hipwell and Stepp2017; Sharp & Wall, Reference Sharp and Wall2018). Although similar in symptom trajectory to adults, findings indicate adolescents with BPD are more likely to present with “acute” BPD symptomatology, such as recurrent self-injury, suicidal ideation, impulsive and self-damaging behaviors (e.g., substance use is a major concern in adolescent BPD samples), and inappropriate anger compared to their adult BPD counterparts (Kaess et al., Reference Kaess, Brunner and Chanen2014; Stead et al., Reference Stead, Boylan and Schmidt2019). Due to the gravity of these consequences associated with the adolescent presentation of the disorder, adolescent BPD has been acknowledged as being a serious public health concern (Chanen et al., Reference Chanen, Sharp and Hoffman2017).
Biosocial Developmental Model of BPD
A biosocial developmental model has been used to describe the developmental pathway of BPD, incorporating biological and environmental aspects of human development (Crowell et al., Reference Crowell, Beauchaine and Linehan2009; Leichsenring et al., Reference Leichsenring, Leibing, Kruse, New and Leweke2011; Linehan, Reference Linehan1993; Stepp, et al., Reference Stepp, Burke, Hipwell and Loeber2012; Winsper, Reference Winsper2018). The biosocial developmental model posits that individuals with BPD are born with an emotional vulnerability (biological risk factor). BPD develops, though, from a combination of this emotional vulnerability and chronic exposure to invalidating environmental conditions. BPD is a product of not only the interaction of the biological predisposition with the dysfunctional, invalidating environments, but also the internalization of the invalidation, and the interaction and transactions of these two systems over time (Crowell et al., Reference Crowell, Beauchaine and Linehan2009; Linehan, Reference Linehan1993; Stepp et al., Reference Stepp, Burke, Hipwell and Loeber2012). An invalidating environment is one where expressions of emotions are met by erratic, unfitting, and/or extreme responses by others. Therefore, it is important to note that invalidating environments can be quite different; for example, experiencing physical/emotional abuse, experiencing peer bullying, frequently being told one’s feelings do not make sense, etc. (Leichsenring et al., Reference Leichsenring, Leibing, Kruse, New and Leweke2011; Paris, Reference Paris2014; Selby & Joiner, Reference Selby and Joiner2009). The central premise from this theoretical framework is that both biological and environmental contexts are important to consider in the development of BPD symptoms.
Multimethod Models for Studying BPD
Abundant theoretical work accompanied by empirical research encourages the use of holistic modeling for optimally understanding psychopathology. Researchers argue for the application of multilevel measurement (i.e., biological, psychological, social, etc.) to enhance our knowledge of the complex systems important in the development of psychopathology (Cicchetti & Dawson, Reference Cicchetti and Dawson2002). Additionally, multilevel models allow us to better understand both risk and resiliency factors associated with psychopathology (Beauchaine et al., Reference Beauchaine, Neuhaus, Brenner and Gatzke-Kopp2008; Burt et al., Reference Burt, Whelan, Conrod, Banaschewski, Barker, Bokde, Bromberg, Büchel, Fauth-Bühler, Flor, Galinowski, Gallinat, Gowland, Heinz, Ittermann, Mann, Nees, Papadopoulos-Orfanos, Paus, Pausova, Poustka, Rietschel, Robbins, Smolka, Ströhle, Schumann and Garavan2016; Cacioppo et al., Reference Cacioppo, Berntson, Sheridan and McClintock2000; Cicchetti & Dawson, Reference Cicchetti and Dawson2002; Miskovic et al., Reference Miskovic, Schmidt, Georgiades, Boyle and MacMillan2010). Inclusion of multiple levels of analysis (from biological to psychological) in a theoretical framework, and one that gives equal weight to domains in the model, provides a more useful and accurate representation of developmental psychopathology than single levels (Cicchetti & Tucker, Reference Cicchetti and Tucker1994; Miskovic et al., Reference Miskovic, Schmidt, Georgiades, Boyle and MacMillan2010; Rutter & Sroufe, Reference Rutter and Sroufe2000).
Frontal EEG Asymmetry and BPD
At present, the extant literature has focused on examining neurobiological correlates of resilience and emotion-based disorders (Burt et al., Reference Burt, Whelan, Conrod, Banaschewski, Barker, Bokde, Bromberg, Büchel, Fauth-Bühler, Flor, Galinowski, Gallinat, Gowland, Heinz, Ittermann, Mann, Nees, Papadopoulos-Orfanos, Paus, Pausova, Poustka, Rietschel, Robbins, Smolka, Ströhle, Schumann and Garavan2016). For example, individual differences in resting frontal EEG alpha asymmetry (FAA) have been considered a plausible neurobiological correlate in the study of resilience and psychopathology. Specifically, FAA is considered a salient candidate due to the role of the prefrontal cortex in both higher-order cognitive processes and the mediation and regulation of emotional processes (Burt et al., Reference Burt, Whelan, Conrod, Banaschewski, Barker, Bokde, Bromberg, Büchel, Fauth-Bühler, Flor, Galinowski, Gallinat, Gowland, Heinz, Ittermann, Mann, Nees, Papadopoulos-Orfanos, Paus, Pausova, Poustka, Rietschel, Robbins, Smolka, Ströhle, Schumann and Garavan2016; Coan & Allen, Reference Coan and Allen2004; Smith et al., Reference Smith, Reznik, Stewart and Allen2017). Empirical work examining hemispheric asymmetries in EEG activity illustrate that the two hemispheres of the cerebral cortex are differentially involved in emotion and motivation tendencies (Davidson, Reference Davidson2000; Fox, Reference Fox1994). The right frontal brain region has shown to be involved in the experience of withdrawal-related negative emotions (e.g., sadness, fear, anxiety), and greater relative right activity is associated with the tendency to withdrawal and disengage from a stimulus (Coan & Allen, Reference Coan and Allen2004; Davidson, Reference Davidson2000; Fox, Reference Fox1991, Reference Fox1994). Furthermore, greater relative right FAA has been well supported as a potential marker of depression vulnerability (see Reznik & Allen, Reference Reznik and Allen2018 for a review). This is an important consideration given the high comorbidity of depression and BPD (Bradley et al., Reference Bradley, Zittel Conklin and Westen2005; Zanarini et al., Reference Zanarini, Frankenburg, Dubo, Sickel, Trikha, Levin and Reynolds1998). Conversely, greater relative left frontal activity is associated with the propensity to approach and engage with a stimulus. Both negative and positive emotional outcomes (e.g., anger, joy) have been both shown to be associated with greater relative left frontal activity (Davidson, Reference Davidson2000; Fox, Reference Fox1994; Harmon-Jones et al., Reference Harmon-Jones, Harmon-Jones and Price2013; Keune et al, Reference Keune, van der Heiden, Várkuti, Konicar, Veit and Birbaumer2012). Moreover, this approach motivation pattern has been shown to be associated with attention deficit hyperactivity disorder (ADHD), which is particularly relevant to the study of BPD, given the symptom overlap between ADHD and BPD (Hale et al., Reference Hale, Smalley, Hanada, Macion, McCracken, McGough and Loo2009; Keune et al, Reference Keune, Wiedemann, Schneidt and Schönenberg2015; Stepp et al. Reference Stepp, Burke, Hipwell and Loeber2012). Overall, the strong association between FAA with emotion, emotion regulation, and psychopathologies that overlap in symptom presentations with BPD (i.e., depression and ADHD), in conjunction with emotion dysregulation being considered a core feature of BPD, makes FAA a particularly salient measure in the study of BPD.
Given the disposition for individuals with BPD to exhibit both approach and withdrawal motivational tendencies (e.g., approach due to heightened anger and impulsive states and withdrawal due to fear and depression), FAA could be an especially important biological correlate to investigate in the context of BPD and social behavior (Beeney et al. Reference Beeney, Levy, Gatzke-Kopp and Hallquist2014; Coan & Allen, Reference Coan and Allen2004; Flasbeck et al. Reference Flasbeck, Popkirov and Brüne2017; Gunderson, & Lyons-Ruth, Reference Gunderson and Lyons-Ruth2008; Popkirov et al., Reference Popkirov, Flasbeck, Schlegel, Juckel and Brüne2019). However, research examining FAA in BPD is sparse, and the studies available employ vastly different methodologies (see, e.g., Beeney et al. Reference Beeney, Levy, Gatzke-Kopp and Hallquist2014; Flasbeck et al., Reference Flasbeck, Popkirov and Brüne2017; Popkirov et al., Reference Popkirov, Flasbeck, Schlegel, Juckel and Brüne2019). Given that the pattern of resting FAA is linked to the experience and regulation of positive and negative emotions, it is possible that individual differences in resting FAA may help to explain different outcomes in BPD, such as interpersonal functioning and emotion dysregulation (Beeney et al. Reference Beeney, Levy, Gatzke-Kopp and Hallquist2014; Coan & Allen, Reference Coan and Allen2004; Flasbeck et al., Reference Flasbeck, Popkirov and Brüne2017; Popkirov et al., Reference Popkirov, Flasbeck, Schlegel, Juckel and Brüne2019).
Social Rejection and BPD
Extreme difficulty in interpersonal functioning is a core domain of BPD. It is hypothesized that interpersonal difficulties in BPD may be largely due to an emotional vulnerability that includes fears of abandonment, rejection sensitivity, and intolerance of aloneness (Gunderson, & Lyons-Ruth, Reference Gunderson and Lyons-Ruth2008). Previous research illustrates that instability in interpersonal functioning is often a core feature in both adults and adolescents with BPD, with these individuals often reporting greater interpersonal conflict and termination of relationships (Lazarus et al., Reference Lazarus, Cheavens, Festa and Rosenthal2014; Sharp, Reference Sharp2014; Stepp et al., Reference Stepp, Hallquist, Morse and Pilkonis2011; Wright et al., Reference Wright, Zalewski, Hallquist, Hipwell and Stepp2016). Additionally, significant interpersonal difficulties, for individuals with BPD, have been shown to remain even after treatment and remission of the disorder (Gratz et al., Reference Gratz, Dixon-Gordon, Breetz and Tull2013; Gunderson & Lyons-Ruth, Reference Gunderson and Lyons-Ruth2008; Stepp et al., Reference Stepp, Hallquist, Morse and Pilkonis2011; Wright et al., Reference Wright, Zalewski, Hallquist, Hipwell and Stepp2016). Despite the obvious importance of understanding interpersonal functioning (i.e., an environmental context) for both the development and maintenance of BPD, these data are also limited (Lazarus et al., Reference Lazarus, Cheavens, Festa and Rosenthal2014; Sharp, Reference Sharp2014; Stepp et al., Reference Stepp, Hallquist, Morse and Pilkonis2011).
Interpersonal dysfunction, though posited as a core feature of BPD, is relatively less well understood (Foxhall et al., Reference Foxhall, Hamilton-Giachritsis and Button2019). In the adult literature, there is evidence that supports a strong relation between rejection sensitivity and BPD symptomatology (Berenson et al., Reference Berenson, Downey, Rafaeli, Coifman and Paquin2011; Dixon-Gordon et al., Reference Dixon-Gordon, Chapman, Lovasz and Walters2011; Foxhall et al., Reference Foxhall, Hamilton-Giachritsis and Button2019; Gratz et al., Reference Gratz, Dixon-Gordon, Breetz and Tull2013; Sadikaj et al., Reference Sadikaj, Moskowitz, Russell, Zuroff and Paris2013; Tragesser, et al., Reference Tragesser, Lippman, Trull and Barrett2008). In order for us to better understand interpersonal dysfunction in individuals with BPD (or otherwise), it is likely important for studies to employ measures that simulate real-world conditions/situations (Cicchetti, Reference Cicchetti2014; Gratz et al., Reference Gratz, Dixon-Gordon, Breetz and Tull2013). Because Cyberball involves experimentally excluding (implicitly rejecting) the participant, it is an ideal approach for studying potential social and psychological vulnerabilities in BPD (Scheithauer, et al., Reference Scheithauer, Alsaker, Wölfer and Ruggieri2013; Williams & Jarvis, Reference Williams and Jarvis2006). Cyberball is a validated computer task designed to elicit feelings of social rejection, social exclusion, and ostracism (Crowley, et al., Reference Crowley, Wu, Molfese and Mayes2010; Jamieson et al., Reference Jamieson, Harkins and Williams2010; Tang et al., Reference Tang, Lahat, Crowley, Wu and Schmidt2019; Williams & Jarvis, Reference Williams and Jarvis2006). It is an online virtual ball-toss game that sets up participants to believe they are playing the game with other participants over the internet (Williams & Jarvis, Reference Williams and Jarvis2006).
Previous work illustrates that Cyberball-induced distress (as evoked by not being tossed the ball in the game) is associated with diminished feelings of belonging, lower self-esteem, less control, and a sense of meaninglessness and invisibility (Crowley et al., Reference Crowley, Wu, Molfese and Mayes2010; Gratz, et al., Reference Gratz, Dixon-Gordon, Breetz and Tull2013; Tang, et al., Reference Tang, Lahat, Crowley, Wu and Schmidt2019; Williams & Jarvis, Reference Williams and Jarvis2006). Adults (aged 18-60 years) with BPD have been shown to report greater feelings of social rejection, distress, and/or negative emotions following the Cyberball task compared to healthy controls and/or other clinically impaired individuals (e.g., depression and social anxiety) (Beeney, et al.; Reference Beeney, Levy, Gatzke-Kopp and Hallquist2014; Ernst et al., Reference Ellis, Boyce, Belsky, Bakermans-Kranenburg and Van IJzendoorn2018; Euler et al., Reference Euler, Wrege, Busmann, Lindenmeyer, Sollberger, Lang and Walter2018; Gratz et al., Reference Gratz, Dixon-Gordon, Breetz and Tull2013; Gutz et al., Reference Gutz, Roepke and Renneberg2016; Renneberg et al., Reference Renneberg, Herm, Hahn, Staebler, Lammers and Roepke2012; Seidl et al., Reference Seidl, Padberg, Bauriedl-Schmidt, Albert, Daltrozzo, Hall, Renneberg, Seidl and Jobst2020; Staebler et al., Reference Staebler, Helbing, Rosenbach and Renneberg2011; Weinbrecht et al., Reference Weinbrecht, Niedeggen, Roepke and Renneberg2018). Similar findings were found in youth (aged 15-24 years) with BPD who reported greater feelings of rejection than healthy controls before, during and following the Cyberball task (Lawrence et al., Reference Lawrence, Chanen and Allen2011).
Rationale for the Present Study in Adolescence
Adolescence has been conceptualized as the “storm and stress” period of development when rejection sensitivity is heightened (Arnett, Reference Arnett1999; Paris, Reference Paris2014; Tang et al., Reference Tang, Lahat, Crowley, Wu and Schmidt2019; Wright et al., Reference Wright, Zalewski, Hallquist, Hipwell and Stepp2016). Studies examining age differences in response to social exclusion and social evaluation across interviews (O’Brien & Bierman, Reference O’Brien and Bierman1988) and experiments (Abrams et al., Reference Abrams, Weick, Thomas, Colbe and Franklin2011; Gunther Moor et al., Reference Gunther Moor, Bos, Crone and van der Molen2014; Sebastian et al., Reference Sebastian, Viding, Williams and Blakemore2010; Stroud et al., Reference Stroud, Foster, Papandonatos, Handwerger, Granger, Kivlighan and Niaura2009; Tang et al., Reference Tang, Lahat, Crowley, Wu and Schmidt2019; Van den bos et al., Reference van den Bos, De Rooij, Miers, Bokhorst and Westenberg2014; Westenberg et al., Reference Westenberg, Drewes, Goedhart, Siebelink and Treffers2004) illustrate that adolescents experience greater emotional distress from social exclusion, compared to both children and adults. Adolescence is also a period when the environmental context changes and individuals start spending more time outside of their homes and with peers (Arnett, Reference Arnett1999; Brown et al., Reference Brown, Laitner, Saxe, Lerner and Steinberg2004; Harris, Reference Harris1995). As more value is placed on peer relationships, there becomes a greater demand for social inclusion and acceptance from one’s peers. This social demand is also met with greater instances of risk-taking behaviors and the emergence of many psychiatric disorders (Ahmed et al., Reference Ahmed, Bittencourt-Hewitt and Sebastian2015). It is hypothesized that these problematic outcomes arise at this developmental stage due to the intricate interaction between the developing adolescent brain (especially the development of the prefrontal cortex) coupled with this new social demand (Ahmed et al., Reference Ahmed, Bittencourt-Hewitt and Sebastian2015; Guyer et al., Reference Guyer, Silk and Nelson2016; Kessler et al., Reference Kessler, Berglund, Demler, Jin, Merikangas and Walters2005; Lamblin et al., Reference Lamblin, Murawski, Whittle and Fornito2017; Steinberg, Reference Steinberg2008). The adolescents of today have even greater exposure to their peers through social media, and thus have an increased chance for repeatedly experiencing perceived and objective social rejection (Brown et al., Reference Brown, Laitner, Saxe, Lerner and Steinberg2004; Lenhart et al., Reference Lenhart, Ling, Campbell and Purcell2010; O’Keeffe & Clarke-Pearson, Reference O’Keeffe and Clarke-Pearson2011). The presence of BPD, then, could place adolescents at an increased risk for experiencing heightened sensitivity to perceived rejection (Guyer et al., Reference Guyer, Silk and Nelson2016; Sharp, Reference Sharp2014; Wright et al., Reference Wright, Zalewski, Hallquist, Hipwell and Stepp2016). Given the developmental nature of BPD, and the importance of understanding the environmental context (i.e., invalidating environment), adolescence is an ideal period for us to study the etiology of BPD.
As illustrated above, there are studies supporting the relation between BPD and feelings of social rejection and distress following a social rejection paradigm in adult (18-60 years) and youth (15-24 years) samples (Beeney, et al.; Reference Beeney, Levy, Gatzke-Kopp and Hallquist2014; Ernst et al., Reference Ellis, Boyce, Belsky, Bakermans-Kranenburg and Van IJzendoorn2018; Euler et al., Reference Euler, Wrege, Busmann, Lindenmeyer, Sollberger, Lang and Walter2018; Gratz et al., Reference Gratz, Dixon-Gordon, Breetz and Tull2013; Gutz et al., Reference Gutz, Roepke and Renneberg2016; Lawrence et al., Reference Lawrence, Chanen and Allen2011; Renneberg et al., Reference Renneberg, Herm, Hahn, Staebler, Lammers and Roepke2012; Seidl et al., Reference Seidl, Padberg, Bauriedl-Schmidt, Albert, Daltrozzo, Hall, Renneberg, Seidl and Jobst2020; Staebler et al., Reference Staebler, Helbing, Rosenbach and Renneberg2011; Weinbrecht et al., Reference Weinbrecht, Niedeggen, Roepke and Renneberg2018). However, there are limited data on adolescent BPD and social rejection, with no studies, to our knowledge, having implemented Cyberball or similar paradigms to examine these relations across the full adolescent age range.
Using a biosocial developmental model, and a multi-level approach, here we sought to extend the extant empirical research on brain–behavior relations in adolescent BPD. Our overall aim was to examine whether individual differences in frontal brain activity at rest moderated the relation between BPD and self-reported feelings of social rejection following a laboratory-based social rejection task among a mixed, clinical-community adolescent (ages 11 to 17 years) sample that included individuals with and without a BPD diagnosis. Due to the lack of empirically supported evidence of BPD-specific patterns of FAA (i.e., the paucity of research on FAA in BPD samples, the inconsistency of these findings, and the absence of any previous studies examining FAA in adolescent BPD samples), we did not speculate on an expected direction of FAA patterns (i.e., greater relative right vs left FAA) (Beeney et al. Reference Beeney, Levy, Gatzke-Kopp and Hallquist2014; Coan & Allen, Reference Coan and Allen2004; Flasbeck et al., Reference Flasbeck, Popkirov and Brüne2017; Gunderson & Lyons-Ruth, Reference Gunderson and Lyons-Ruth2008; Popkirov et al., Reference Popkirov, Flasbeck, Schlegel, Juckel and Brüne2019). Rather, we postulated that since both approach and withdrawal motivations are related to interpersonal dysfunction associated with BPD, both a greater relative right (withdrawal) or left (approach) FAA pattern for individuals scoring high on self-reported BPD features would exhibit heightened scores on self-reported feelings of social rejection, following Cyberball (Beeney et al. Reference Beeney, Levy, Gatzke-Kopp and Hallquist2014; Coan & Allen, Reference Coan and Allen2004; Flasbeck et al., Reference Flasbeck, Popkirov and Brüne2017; Gunderson & Lyons-Ruth, Reference Gunderson and Lyons-Ruth2008; Popkirov et al., Reference Popkirov, Flasbeck, Schlegel, Juckel and Brüne2019).
Method
Participants and Sample Overview
The present study was part of a larger study which recruited different diagnostic groups, all with underlying emotion dysregulation problems (e.g., depression, disruptive behavior disorders, and disruptive mood dysregulation disorder). A healthy control group was also recruited from the community, as a comparison group for the clinical groupings within the larger study. These controls were enrolled in the larger study if they had not been previously diagnosed with or received treatment for a psychiatric condition.
In total, the larger study included 88 adolescents (female = 54; 61% of sample; Mage = 14.59 years; SD = 1.69; range = 11 to 18 years) who were referred from a tertiary mental health hospital and the community (n = 19). Adolescents and their caregivers were recruited by referral from a mental health clinician or by a research assistant who obtained their contact information through a clinic database of all consecutively referred patients who also consented to be contacted for research. Community individuals (n = 19) were recruited from the community through word of mouth.
All clinic participants had one or more psychiatric disorders, and each of them had one of either major depressive disorder, BPD, or both conditions. Participants were excluded if they had an IQ of less than 70, a history of diagnosed head injury (e.g., concussion), epilepsy, psychotic or bipolar depression disorders, or autism spectrum disorder. Of the sample who reported on their ethnicity, 86.4% were White, 3.4 % Hispanic/Latino, 1.1% Indigenous, 1.1% Asian, 1.1% Black/West Indian, 4.5% Multi-Ethnic, and 2.3% Other (those with White and either Indigenous or Latino ancestry). Fourteen participants did not report on their ethnicity. The adolescent and caregiver consented to participate in the research study after meeting with the research assistant.
Procedures
All procedures were approved by the Hamilton Health Sciences Research Ethics Board, and all participants tested gave their consent to participant. The study comprised two laboratory visits. The first visit (Time 1) included administering all psychiatric interviews and measures (reported by both adolescent and caregiver). Participants returned two weeks later for a baseline EEG recording and to complete the Cyberball task (Time 2). At the end of the first visit, participants were informed that, when they came back for their second visit, they would be completing the EEG recording and playing an online game with similar-aged peers.
Clinical Interviews
All participants (irrespective of their previous diagnostic history) were assessed for the presence of psychiatric disorders at Time 1 using The Mini-International Neuropsychiatric Interview for Children and Adolescents (MINI-KID; Sheehan et al., Reference Sheehan, Sheehan, Shytle, Janavs, Bannon and Rogers2010) with both the adolescent and parent versions, and The Childhood Interview for Borderline Personality Disorder (CI-BPD; Sharp et al., Reference Sharp, Ha, Michonski, Venta and Carbone2012). Two doctoral-level students conducted the clinical evaluations on the adolescents, while a trained research assistant collected parent reports. Final diagnoses were established using a combination of parent and adolescent reports at an evaluation meeting supervised by a licensed psychiatrist (see below for specific procedures).
Clinical Psychiatric Interview
MINI-KID is a standardized diagnostic interview that assess DSM-IV-TR disorders in individuals aged six to 17 years. We used this interview to assess for lifetime and present prevalence of depression, and present social anxiety, separation anxiety, generalized anxiety, ADHD, oppositional defiant disorder, and conduct disorder within our sample. The MINI-KID has demonstrated good test–retest reliability (k = 0.56 to 0.87) for mood, anxiety, ADHD, and behavioral disorders based on joint caregiver–child interviews and adequate agreement with another diagnostic interview (Sheehan et al., Reference Sheehan, Sheehan, Shytle, Janavs, Bannon and Rogers2010). It was administered to both the adolescent and one of their caregivers by separate research assistants, and inter-rater reliability was deemed excellent (k = .83 to 1.0). Discrepant ratings by informants were discussed in team meetings with the lead child psychiatrist. Internalizing problems (i.e., mood and anxiety) were most often scored in favor of the adolescents’ reports and externalizing behaviors were most often scored in favor of the caregivers’ reports, as research has illustrated utilizing this method when faced with discrepant reports (Duncan et al., Reference Duncan, Georgiades, Wang, Van Lieshout, MacMillan, Ferro, Lipman, Szatmari, Bennett, Kata, Janus and Boyle2018).
Clinical Interview for BPD
The CI-BPD; Zanarini, Reference Zanarini2003) is a semi-structured interview that was adapted from the adult Diagnostic Interview for Personality Disorders (DIPD-IV; Zanarini et al., Reference Zanarini, Frankenburg, Sickel and Yong1996), and is specifically for child and adolescent BPD presentations. A total of nine items (sections) are included on the CI-BPD that reflect the nine diagnostic criteria of BPD. The interviewer codes the items as not present (coded as 0), probably present (coded as 1), and definitely present (coded as 2). A minimum of five items coded as “2” are required for a BPD diagnosis, and three items indicate “probable” BPD pathology. Overall, the CI-BPD shows good reliability and validity (Sharp et al., Reference Sharp, Ha, Michonski, Venta and Carbone2012). Confirmatory factor analysis also supported a unidimensional factor, which is consistent with previous research in adult and adolescent samples (Kaess et al., Reference Kaess, Brunner and Chanen2014; Miller et al., Reference Miller, Muehlenkamp and Jacobson2008; Sharp et al., Reference Sharp, Ha, Michonski, Venta and Carbone2012; Yen et al., Reference Yen, Gagnon and Spirito2013). The CI-BPD was administered solely to adolescents aged 12 years and over, as research has illustrated the validity of this measure in adolescents this young in an American sample (Sharp et al., Reference Sharp, Ha, Michonski, Venta and Carbone2012). Graduate student research assistants were the ones who administered the CI-BPD, following an extensive training by a child psychiatrist. Inter-rater reliability for the CI-BPD was excellent (k = .913) in this sample. Discrepancy or uncertainty about ratings were resolved during a supervision meeting with a child psychiatrist with expertise in adolescent BPD.
For the participants retained in the present analyses, eight of them (13% of the final sample) did not meet diagnostic criteria for any mental health disorder. Thirty-five of the participants (55% of the total sample) had any combination of mental health diagnosis, including mood, anxiety, and disruptive behavior disorders, but did not have 3 or more symptoms of BPD. Finally, sixteen participants met diagnostic criteria for BPD (i.e., “definite” diagnosis), and five met diagnostic criteria for a “probable” diagnosis (i.e., meeting three to four out of the nine diagnostic criteria for BPD), together accounting for 33% of the overall sample. The developmental stage and clinical characteristics of this sample places these individuals at a heightened susceptibility for emotion dysregulation, a core feature of BPD. We did not examine all of these diagnostic classifications within our analyses, but we controlled for BPD diagnosis status.
Self-reported Measures
Symptoms of Depression
Depressive symptoms were assessed using the Depressive Problems Subscale of the Child Behavior Checklist (CBCL; Achenbach & Edelbrock, Reference Achenbach and Edelbrock1983; Achenbach & Rescorla, Reference Achenbach and Rescorla2001). The CBCL contains 113 problem items rated as: 0, not true; 1, somewhat or sometimes true; and 2, very true or often true. (Achenbach & Rescorla, Reference Achenbach and Rescorla2001; Achenbach & Ruffle, Reference Achenbach and Ruffle2000). For the analyses in this study, we used the total depressive problems score, which is a continuous measure that totals all items that comprise the DSM-oriented depressive problems subscale.
Self-reported BPD Features
The Borderline Personality Features Scale for Children – 11-item (BPFSC-11) was used to assess self-reported BPD symptoms (Sharp et al., Reference Sharp, Steinberg, Temple and Newlin2014). This measure was modified from the original 24-item BPFSC measure, which was adapted from the Personality Assessment Inventory – Borderline scale (PAI-BOR), an adult measure. The BPFSC differs from the PAI-BOR to include more age-appropriate language but retains the four domains of BPD, including affective instability, identity problems, negative relationships, and self-harm. Previous psychometric analysis revealed that the BPFSC-11 is comparable to the original BPFSC and supported a unidimensional factor of BPD (Sharp et al., Reference Sharp, Steinberg, Temple and Newlin2014). In the present study, we used this scale as our continuous measure of BPD in our analyses.
Social Exclusion Task: Procedures and Measures
Procedures
At the start of the second visit, participants were re-informed that, following their EEG recording, they would be playing a game over the Internet with other study participants. They were led to believe that they would play an online ball-toss game, Cyberball, with two other same-aged peers who were playing in other laboratories within the building. However, the experimenters pre-matched the participants for age range and identified gender to a selection bank of stock photos of “opponent players”. Participants were also told that they would be able to see pictures of these “opponent players” (i.e., the stock photos), and that the research assistants for the other laboratories took the photos for these opponents. Study participants were asked, even though they would not be able to see their own picture in the same way during the game, if they consented to having their picture taken so that the opponents would believe that they were truly playing with them. Following consent from the participants, the experimenter pretended to take the participant’s picture and upload it to the “game’s server,” while the other experimenter pretended to telephone call the other laboratories to determine if they were ready to start the online game.
The participants were then informed that they were to play a virtual ball-toss game with these “opponent players” over the Internet. They were instructed to try their best to visualize playing ball toss with the other players, as if it was in real life. Participants were told that they could throw to whomever they wanted, and that the “opponent players” could do so as well. However, in reality, the other two “opponent players” were completely computerized. When the game began, participants would receive a visual “Connecting to Other Players” notification on the computer screen. Then, the screen would change and switch to the game, which included the participant’s online player (without a picture) at the bottom center of the screen, with the other two virtual players at the top left and right corners of the screen center. The stock photos and names appeared next to the respective virtual players. Participants were instructed to use their right index and middle fingers on a keyboard to respond by pressing computer keys 1 and 4 to pass to the opponent players on the right and left side, respectively. When the participant understood how to respond, the experimenters left the room. Each trial began with the ball in the glove of one of the two virtual opponents for 500 to 2500 ms. Fifty total trials were divided into fair play and exclusion blocks. The fair play block consisted of 30 trials divided and included the virtual opponent throwing the ball at each other but not to the participant (10 times), the virtual opponents throwing the ball to the participant (10 times), and the participant throwing the ball to the opponents (10 times). The frequency with which the ball was thrown to the participant was pseudorandom and predetermined, such that the participant waited zero to three throws between the opponents before receiving the ball again. The fair play block transitioned to the exclusion block after 30 trials. During the exclusion block, the virtual opponents solely passed the ball to each other and not to the participant for 20 trials. After this procedure, the game was finished, and a visual notification appeared on the screen informing the participant to call the experimenter back to the room.
Feelings of Social Rejection
Immediately following the Cyberball game, the participants were informed that they were to complete a questionnaire, the Need Threat Scale (NTS), regarding how they felt during the Cyberball game (Jaimison et al., Reference Henriques and Davidson2010; van Beest & Williams, Reference Tragesser, Lippman, Trull and Barrett2006). The NTS is a valid and reliable measure of ostracism distress that includes 20 items to evaluate feelings of distress following being rejected during the Cyberball game (Crowley et al., Reference Crowley, Wu, Molfese and Mayes2010). It consists of four, dimensional subscales: belonging, control, meaningful existence, and self-esteem, and these items include statements like “I felt rejected” and “I felt invisible.” (Crowley et al., Reference Crowley, Wu, Molfese and Mayes2010; Jamieson et al., Reference Henriques and Davidson2010; van Beest & Williams, Reference Tragesser, Lippman, Trull and Barrett2006). Items are rated on a 5-point scale ranging from 1 (not at all) to 5 (extremely/a lot). A total score is calculated by summing the four scales to provide an index of overall ostracism distress during Cyberball. However, given that ostracism and rejection are related constructs (Williams, Reference Williams2007), and rejection sensitivity is more often the term associated with BPD (Foxhall et al., Reference Foxhall, Hamilton-Giachritsis and Button2019; Gunderson & Lyons-Ruth, Reference Gunderson and Lyons-Ruth2008), we considered our total NTS score as a proxy for rejection sensitivity and refer to scores on the NTS as total social rejection scores from here on.
Debrief
Following completion of the NTS, the participants were asked open-ended questions about how they felt about the game, what they liked or did not like about it, and if they felt anything was off (i.e., suspicious). Following this questioning, experimenters informed the participants that they were actually playing with a computer, and not real people. The experimenter then made a rating based on the debrief as to whether they believed the participants were deceived by this information or not during the game.
EEG Data Collection and Reduction
EEG Data Collection
Continuous EEG was collected using a high-density 128 electrode Hydrocel net (Electrical Geodesics Incorporated [EGI], Inc., Eugene, Oregon) with Netstation (EGI, Inc.) and a high impedance amplifier, sampled at 250 Hz (.1 Hz high pass, 100 Hz low pass). All electrodes were referenced to the central (Cz) scalp site for recording. Before beginning, impedances at or below 40 K-Ohms were considered acceptable. Participants were informed before the recording started that they would be instructed to sit with their hands in their lap, feet flat on the floor, and their eyes open staring straight ahead for three minutes, and then a research assistant would inform the participant to close their eyes and the recording would last for another three minutes. EEG data were preprocessed offline in Netstation through a 0.1 Hz first order high-pass filter and a 50 Hz low-pass filter.
EEG Data Reduction and Quantification
EEG data were visually scored and edited using BrainVision Analyzer (Brain Products GmbH, Gilching, Germany). Only channels selected a priori were isolated to be processed. Continuous EEG data, of approximately six minutes in length, were segmented into two sections; eyes open and eyes closed, which included a buffer of segmented data between the end of eyes open and start of eyes closed that was eliminated from analyses. Eye blinks were removed using Independent Components Analysis. All other artifacts were visually edited. Segments were further segmented into 1s epochs with 0.5s overlap. Artifact-free epochs were extracted using a Hamming window. Data were subjected to a Fast Fourier Transform and spectral power density (μV2/Hz) was extracted in the alpha band (8 to 13 Hz).
For our present analyses, we were particularly interested in examining F3 and F4, due to a priori hypotheses (Beeney et al., Reference Beeney, Levy, Gatzke-Kopp and Hallquist2014; Flasbeck et al., Reference Flasbeck, Popkirov and Brüne2017; Fox, Reference Fox1994; Popkirov et al., Reference Popkirov, Flasbeck, Schlegel, Juckel and Brüne2019; Schmidt et al., Reference Schmidt, Santesso, Miskovic, Mathewson, McCabe, Antony and Moscovitch2012), and these two sites were used for the calculation of the frontal asymmetry metric. All power density values were transformed using the natural log to normalize the data distribution. The eyes-open and eyes-closed conditions were correlated (r’s = .80 to .86, p<0.05), so we combined these conditions separately for each hemisphere site (i.e., F3 and F4). Next, asymmetry scores were calculated by subtracting the natural log-transformed scores (ln[right]-ln[left]). Thus, asymmetry scores were based on the following homologous pair: F4 minus F3 (Flasbeck et al., Reference Flasbeck, Popkirov and Brüne2017; Popkirov et al., Reference Popkirov, Flasbeck, Schlegel, Juckel and Brüne2019; Schmidt et al., Reference Schmidt, Santesso, Miskovic, Mathewson, McCabe, Antony and Moscovitch2012). Because EEG power is inversely related to activity, higher scores on this asymmetry metric reflect greater relative left frontal activity (Tomarken et al., Reference Tomarken, Davidson, Wheeler and Kinney1992).
It is also important to point out that we examined EEG power in the left (P3) and right (P4) parietal sites and computed a parietal asymmetry score (ln[right]-ln[left]) and examined this posterior asymmetry in relation to the main study measures to ensure that the effects were specific to the frontal region. We did not find any statistically significant correlations between the parietal asymmetry score and the two other primary study measures, i.e., continuous BPFSC scores (p > .05) and total social rejection scores (p > .05), so the parietal data were not discussed below.
Missing Data
Of the 88 participants who participated in the first visit, two participants (both male) declined to participate in the second visit (one clinical and one control). We only included individuals who had complete data for both time points in our analyses. Sixty-five participants had complete EEG data. Of these 65, one participant did not complete the Cyberball task at Time 2, due to technical issues. This resulted in the final sample for our analyses below comprising of 64 participants (females = 62.5%; Mage = 14.45 years; SD = 1.6; range = 11-17 years). There were no differences between participants who were included in our final analyses and those who were not (including those who declined the second visit, were unable to complete the Cyberball task, and did not have complete EEG data) on age, sex, sociodemographic measures (i.e., household income and mother’s education level), BPD scores, and total social rejection scores.
Data Analyses
All continuous scores were evaluated for the normality of their distributions (see Table 1 for descriptive statistics of study measures). Outliers (for all continuous variables) were assessed using the conventional criteria of z-scores greater than +/- 3.29 (p < .001, two-tailed test) (Tabachnick & Fidell, Reference Tabachnick and Fidell2013). No outliers were identified. All continuous predictor and covariate variables were centered at their means to reduce multicollinearity and more easily facilitate interpretation of the results (see Table 2 for difference in correlations between centered and non-centered predictor variables). All data transformations and statistical analyses were conducted using the SPSS (version 27) software (IBM Corp., Armonk, New York: IBM Corp.).
Table 1. Descriptive Statistics for the Study Measures (N = 64)

Table 2. Correlations among Study Measures

*p < .05. **p < .01.
Considering that BPD is theoretically associated (and correlated within our sample) with social rejection (see Table 2), a hierarchical regression model was performed to assess the robustness of this association within our sample, and to determine if FAA (a biological proxy of emotion regulation) strengthened the association between BPD and feelings of social rejection. We also wanted to test whether BPD and FAA predicted feelings of social rejection above and beyond other associated factors inherent in our sample. To do this, we included age, sex, gender identity, depression scores, and BPD diagnosis status into the first step of our model.
Age was included since our sample spans the developmental stage associated with heightened feelings of social rejection (Arnett, Reference Arnett1999; Paris, Reference Paris2014; Tang et al., Reference Tang, Lahat, Crowley, Wu and Schmidt2019). Biological sex was included, as research illustrates differences in sex on patterns of FAA (Cave & Barry, Reference Cave and Barry2021; Davidson et al., Reference Davidson, Schwartz, Pugash and Bromfield1976). Gender identity was also included in addition to biological sex for four important reasons: 1) theoretically, gender socialization is bound within a social task like Cyberball; 2) research illustrates that adolescent males report heightened levels of rejection sensitivity compared to their female counterparts (this is considered to be due, in part, to socialization); 3) we had four transgender individuals in our sample that we wanted to more appropriately represent; and 4) we matched the Cyberball task demographic (i.e., the “opponent players”) to the participants’ identified gender. We then controlled for depression in our first step, because 42% of our overall sample met diagnostic criteria for major depressive disorder (past and current episodes), and because depression is associated with feelings of social rejection (Arnett, Reference Arnett1999; Paris, Reference Paris2014; Tang et al., Reference Tang, Lahat, Crowley, Wu and Schmidt2019), and patterns of frontal brain activity (Henriques & Davidson, Reference Henriques and Davidson1990, Reference Henriques and Davidson1991). BPD diagnosis status was also included because 21 individuals met diagnostic criteria for “definite” or “probable” BPD. Multicollinearity and singularity of our BPD grouping variable were considered; however, since our independent (continuous) variable of BPD and our diagnostic grouping variable were not deemed multicollinear (r<0.9), and these measures are not singular in measure (one measures symptom range and the other is a dichotomous grouping), we deemed this grouping variable appropriate to include (Tabachnick & Fidell, Reference Tabachnick and Fidell2013).
In the second step, we included our independent variables (BPD and FAA), separately, to examine their overall contribution to the variance. The last step (third step) included the addition of the interaction term of BPD (Time 1) x FAA (Time 2). This third step, our main research question, examined whether the combination of BPD and FAA increased the proportion of explained variance in feelings of social rejection following the Cyberball task, and thus, whether FAA moderated the relation between symptoms of BPD and feelings of social rejection within our sample.
Results
Descriptive Statistics
Tables 1 and 2 present the descriptive statistics for the demographic measures and the correlations among the study measures, respectively.
Regression Analyses
Results from the regression analyses are presented in Table 3. In the first step of the regression analysis predicting feelings of social rejection, our controlling variables explained a statistically significant proportion of the variance (R 2 = 0.21; p<0.05). In this step, depression scores significantly predicted feelings of social rejection (β = -.50, t(59) = -2.88, p < .01). When we included BPD and FAA scores in our second step, the overall model was statistically significant (p<.05); however, these variables did not explain a significant proportion of variance (R 2 = 0.23; ns). Finally, after including our interaction term of self-reported BPD scores (Time 1) and FAA scores (Time 2), our overall model was statistically significant (F(8, 55) = 3.18, p<.01). In particular, the interaction of BPD x FAA emerged as the only significant predictor within this model (β = -.31; p< 0.01). This final model, with all three steps, accounted for 32% of the variance in overall self-reported feelings of social rejection following Cyberball.
Table 3. Summary of Hierarchical Regression Analysis for Variables Predicting Feelings of Social Rejection following Cyberball (N = 64) – Models 1-3

Note: BPFSC and FAA were centered at their means; BPFSC = borderline personality feature scale for children; FAA = frontal alpha asymmetry.
**p < .01.
In order to decompose this effect, the sample was evenly split into right frontal (bottom 33%), middle frontal (middle 33%), and left frontal (upper 33%) groups on their overall resting FAA scores (see Figure 1; Gelman & Park, Reference Gelman and Park2009). The first third of the sample (n = 21) with the lowest FAA scores (M = -.48; SD = .33; range = -1.61 to -.21), indicative of greater relative right frontal FAA, comprised the right frontal group. The second third of the sample (n = 22), with moderate FAA scores (M = -.04; SD = .11; range = -.19 to .16), comprised the middle group. Finally, the last third of the sample (n = 21), with the highest FAA scores (M = .56; SD = .30; range = .17 to 1.54), indicative of greater relative left frontal FAA, comprised the left frontal group.

Figure 1. BPD x FAA Interaction Effect on Overall Scores of Social Rejection. Note: BPFSC = BPD symptoms; Total Social Rejection Scores = Total NTS score (higher scores less feelings of rejection); FAA = Frontal Alpha Asymmetry.
Examination of the interaction plot revealed that those adolescents with greater relative left FAA at rest showed a differential effect for social rejection, depending on the total number of endorsed BPD symptoms (as measured by the BPFSC): those with relatively higher self-reported BPD scores and greater relative left FAA scores reported worse feelings of social rejection (i.e., lower overall NTS scores). Conversely, individuals in the left FAA group who self-reported relatively fewer BPD symptoms reported relatively better feelings of social rejection following Cyberball (i.e., higher overall NTS scores). This differential effect was not observed for the right and middle FAA groups.
An exploratory plot analysis was also completed to include the BPD x FAA interaction effect and BPD diagnostic status (as determined via the CIBPD) (see Figure 2). This plot confirmed that those with relatively fewer self-reported BPD features were less likely to meet diagnostic criteria for BPD, and those with greater self-reported BPD features were more likely to have a definite BPD diagnosis. This analysis was a confirmation check to examine how our independent measure of self-reported BPD compared to a diagnostic measure of BPD.
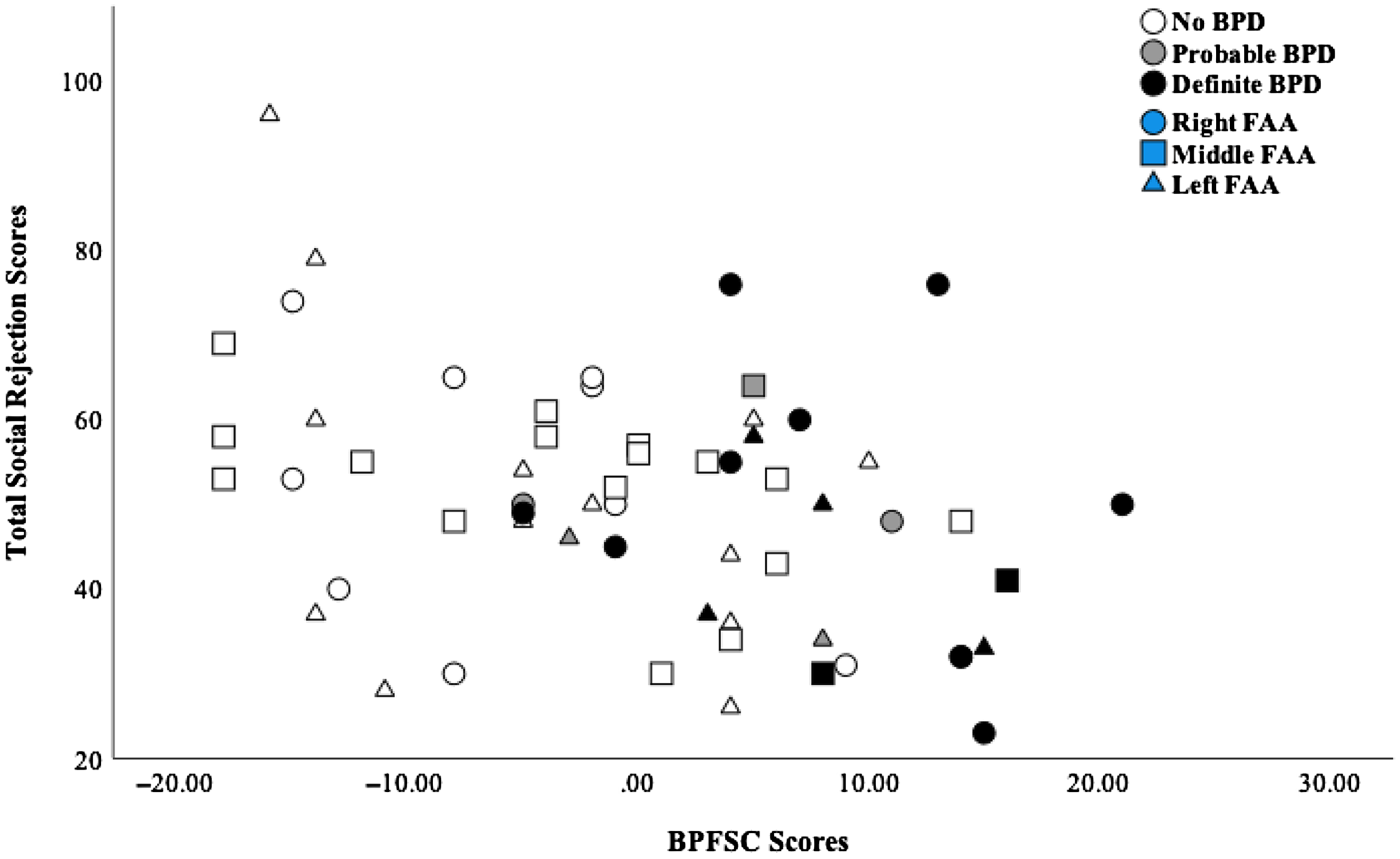
Figure 2. BPD x FAA Interaction Effect with BPD Diagnosis Categorized. Note: BPFSC = BPD symptoms; BPD Diagnoses (determined via the Childhood Interview for BPD) = No (zero to two BPD criteria met), Probable (three to four BPD criteria met), and Definite (at least five BPD criteria met); Total Social Rejection Scores = Total NTS score (higher scores less feelings of rejection).
Discussion
We examined the relations among BPD features, FAA, and feelings of social rejection following a social rejection context (validated social exclusion paradigm) in a sample of adolescents, covering the adolescent age period (11-17 years). We found that left frontal brain activity at rest moderated the relation between BPD features and rejection sensitivity. Individuals who exhibited greater relative left frontal brain activity displayed the highest and lowest scores of rejection sensitivity depending on whether they also had the highest and lowest BPD feature scores, respectively. Our findings also complement and extend some of the adult literature, illustrating left baseline FAA for both BPD and healthy control groups (Beeney et al., Reference Beeney, Levy, Gatzke-Kopp and Hallquist2014; Flasbeck et al., Reference Flasbeck, Popkirov and Brüne2017). Beeney and colleagues (Reference Beeney, Levy, Gatzke-Kopp and Hallquist2014) found that adults with BPD demonstrated greater relative left FAA. However, this association was found following the Cyberball task (i.e., post experiencing social rejection), and BPD individuals did not show a different pattern of resting FAA at baseline when compared to controls. Though we assessed FAA at different points (i.e., before versus after completing Cyberball), our results might be capturing the same underlying proneness to rejection sensitivity inherent in BPD (i.e., exclusion proneness) (Euler et al., Reference Euler, Wrege, Busmann, Lindenmeyer, Sollberger, Lang and Walter2018).
Beeney and colleagues (Reference Beeney, Levy, Gatzke-Kopp and Hallquist2014) might have been capturing feelings of rejection following a social rejection event, whereas the current study might be suggestive of a kind of “anticipatory” feelings of rejection. This premise of anticipatory feelings of rejection is taken from the work on anticipatory anxiety for social situations in individuals with social anxiety disorder (Rowa et al., Reference Rowa, Gavric, Stead, LeMoult and McCabe2016). Specifically, it might be that some individuals with BPD, who experience intensive fears of rejection/abandonment, might then develop anticipatory fears of rejection for social situations just like those with social anxiety disorder experience anticipatory fear of negative evaluation for social settings (Gunderson & Lyons-Ruth, Reference Gunderson and Lyons-Ruth2008; Matthies et al., Reference Matthies, Schiele, Koentges, Pini, Schmahl and Domschke2018; Rowa et al., Reference Rowa, Gavric, Stead, LeMoult and McCabe2016). Our participants were told after their first visit and right at the start of their second visit that they would be playing an online game with peers during this second visit. Given that BPD is associated with greater difficulties with rejection sensitivity, it is possible that anticipation of this “online game with peers” might produce more intense feelings for individuals with greater BPD symptom severity (Berenson et al., Reference Berenson, Downey, Rafaeli, Coifman and Paquin2011; Dixon-Gordon et al., Reference Dixon-Gordon, Chapman, Lovasz and Walters2011; Euler et al., Reference Euler, Wrege, Busmann, Lindenmeyer, Sollberger, Lang and Walter2018; Foxhall et al., Reference Foxhall, Hamilton-Giachritsis and Button2019; Gratz et al., Reference Gratz, Dixon-Gordon, Breetz and Tull2013; Sadikaj et al., Reference Rutter and Sroufe2013; Tragesser, et al., Reference Tragesser, Lippman, Trull and Barrett2008).
The findings from this study and the study by Beeney et al. (Reference Beeney, Levy, Gatzke-Kopp and Hallquist2014), highlight the work of Coan and colleagues’ (Reference Coan and Allen2006) capability model of FAA. The capability model emphasizes the need to assess people’s responses (i.e., EEG reactivity versus resting baseline) to specific stressors or emotionally evocative stimuli for a more ecologically valid measure of underlying motivational tendencies that is likely not captured in resting baseline assessments (Beeney et al., Reference Beeney, Levy, Gatzke-Kopp and Hallquist2014; Coan et al., Reference Coan, Allen and McKnight2006). Accordingly, even though we are uncertain if our findings are a result of an anticipatory response to possible rejection, our findings support the idea that individual differences in resting frontal brain activity might be a vulnerability factor in some cases, and a protective factor in other cases, and also suggest the need for conducting more ecologically valid clinical research using the FAA measure to index these biases. This idea will be important to further assess in future research, as it may have important implications regarding therapy outcomes for individuals with BPD (i.e., a hindered capacity for alliance with therapists and in group therapy due to an underlying proneness for anticipatory rejection) (Euler et al., Reference Euler, Wrege, Busmann, Lindenmeyer, Sollberger, Lang and Walter2018).
Our results in adolescents also replicated similar findings in adult samples, suggesting that BPD symptoms are related to worse feelings of social rejection following a social rejection task, Cyberball (Beeney, et al.; Reference Beeney, Levy, Gatzke-Kopp and Hallquist2014; Gratz et al., Reference Gratz, Dixon-Gordon, Breetz and Tull2013; Lawrence et al., Reference Lawrence, Chanen and Allen2011; Seidl et al., Reference Seidl, Padberg, Bauriedl-Schmidt, Albert, Daltrozzo, Hall, Renneberg, Seidl and Jobst2020; Staebler et al., Reference Staebler, Helbing, Rosenbach and Renneberg2011; Weinbrecht et al., Reference Weinbrecht, Niedeggen, Roepke and Renneberg2018). Previous research has also illustrated that rejection sensitivity is an underlying feature of BPD pathology (Foxhall et al., Reference Foxhall, Hamilton-Giachritsis and Button2019). Taken together, these findings may illustrate that rejection sensitivity, inherent in BPD, might be similar in both adolescents and adults with BPD. However, a study comparing these two developmental groups would need to be conducted to test such an assertion.
Theoretical Implications
What role does left frontal brain activity play in helping us understand the relation between BPD and social rejection? Our findings have possible implications supporting a differential susceptibility model. For example, our results might suggest that left FAA serves as a biological sensitivity factor within our sample, that is capable of supporting both positive and negative behavioral outcomes (i.e., self-reported social rejection) depending on the degree of self-reported BPD pathology (low to high). This notion is not new, as relative left FAA at rest has been previously linked with both positive and negative emotions and corresponding behavioral outcomes (see, for example, Fortier et al., Reference Fortier, Van Lieshout, Waxman, Boyle, Saigal and Schmidt2014; Harmon-Jones, et al., Reference Harmon-Jones, Harmon-Jones and Price2013, and Lahat et al., Reference Lahat, Tang, Tanaka, Van Lieshout, MacMillan and Schmidt2018); therefore, when left FAA is conceptualized in terms of a differential susceptibility variable it supports both the most positive and negative outcomes (Belsky et al., Reference Belsky and Bakermans-Kranenburg2007; Belsky & Pluess, Reference Belsky and Pluess2009; Belsky & Pluess, Reference Belsky and Pluess2013; Ellis et al., Reference Ellis, Boyce, Belsky, Bakermans-Kranenburg and Van IJzendoorn2011). In our sample, it appears that left FAA was a protective factor in the presence of fewer BPD features but a risk factor in the presence of more BPD features, in relation to feelings of social rejection.
The above proposed differential susceptibility model for FAA also fits within the biosocial developmental model of BPD, which asserts that BPD pathology develops through a complex interaction between a person’s biology and an invalidating environment (Crowell et al., Reference Crowell, Beauchaine and Linehan2009; Linehan, Reference Linehan1993). A previous prospective study found that children who had higher levels of dysregulation (i.e., an emotional vulnerability) were prone to the development of BPD symptoms in adolescents when exposed to peer bullying (environmental risk factor). These children with greater dysregulation were also more likely to be exposed to this environmental risk factor (i.e., bullying) (Winsper et al., Reference Winsper, Hall, Strauss and Wolke2017; Wolke et al., Reference Wolke, Schreier, Zanarini and Winsper2012). These findings are in line with the notion, purported by the biosocial developmental model, that BPD develops from the interaction and transaction of biology and environment over time (Crowell et al., Reference Crowell, Beauchaine and Linehan2009).
Our findings illustrating worse feelings of rejection for those with relative left FAA (approach motivation) and greater BPD, then, might be capturing individuals with a greater underlying emotional vulnerability (i.e., relative left FAA) who also might be more susceptible to experiences of rejection (Winsper et al., Reference Winsper, Hall, Strauss and Wolke2017; Wolke et al., Reference Wolke, Schreier, Zanarini and Winsper2012). In our study, this might be captured by greater rejection scores following Cyberball. It is possible that those with greater BPD symptoms and a relative left FAA (i.e., biological approach-related motivational underpinning) might 1) experience more instances of rejection given their approach motivational tendency, and 2) be more negatively affected by the rejection than those with a withdrawal-motivational tendency, given the mismatch in underlying motivational needs (i.e., behavioral approach met with rejection being obvious rejection compared to someone who withdrawals before experiencing rejection). (Gunderson & Lyons-Ruth, Reference Gunderson and Lyons-Ruth2008; Harmon-Jones, et al., Reference Harmon-Jones, Harmon-Jones and Price2013; Matties et al., Reference Marston, Hare and Allen2018). Moreover, ADHD, a disorder that shares features of BPD, has been shown to be associated with an excessive approach tendency (or motivational dysfunction) (Hale et al. Reference Hale, Smalley, Hanada, Macion, McCracken, McGough and Loo2009; Keune et al., Reference Keune, Wiedemann, Schneidt and Schönenberg2015; Stepp et al., Reference Stepp, Burke, Hipwell and Loeber2012). It is possible that our results might be capturing BPD individuals with greater relative left FAA that have an excessive approach tendency similar to those with ADHD. However, the underlying mechanism of these approach tendencies might differ by disorder, with BPD largely due to an underlying rejection sensitivity, and what makes these disorders distinct from one another.
Conversely, it may be possible that an approach-motivational tendency, which is sometimes correlated with positive affect (e.g., joy), is a protective factor when in combination with lower levels of BPD pathology and in the context of social rejection (Harmon-Jones, et al., Reference Harmon-Jones, Harmon-Jones and Price2013). These left FAA with low BPD symptom individuals likely do not experience the underlying fear of abandonment that is characteristic of BPD, and thus are not as prone to the negative effects of rejection (Winsper et al., Reference Winsper, Hall, Strauss and Wolke2017). Additionally, the adolescents within our sample with relative right FAA and high levels of BPD symptoms showed moderate levels of feelings of rejection following Cyberball. These feelings of rejection were not significantly different than those endorsed by adolescents with lower levels of BPD symptoms (and relative right FAA). Thus, it may be possible that having a relative right FAA for individuals with greater BPD symptoms acts as a buffer for these individuals with BPD. Overall, our findings might be indexing individual differences in BPD pathology. However, these ideas are only speculative and future work that also includes important considerations from Coan’s capability model of FAA is needed to truly test these assertions (see Coan et al., Reference Coan, Allen and McKnight2006). Furthermore, future prospective work that examines the relation between FAA and temperament/personality factors, especially, those considered possible BPD precursors, is likely also needed for us to better understand the complex relation between BPD, social rejection, and frontal brain activity (Cicchetti, Reference Cicchetti2014; Winsper, Reference Winsper2018).
Possible Confounding Influences for Consideration
We included biological sex and gender identity in our regression models, due to differential associations with BPD and rejection sensitivity. Firstly, previous epidemiological and clinical research in the field of BPD has documented that there are no sex differences in individuals with BPD, but BPD is more prevalent in females in clinical settings (Kaess et al., Reference Kaess, Brunner and Chanen2014; Sharp & Wall, Reference Sharp and Wall2018). Secondly, some work indicates that male adolescents experience higher levels of distress from social rejection, likely due to gender socialization (London et al., Reference London, Downey, Bonica and Paltin2007; Marston, et al., Reference Marston, Hare and Allen2010). We found no sex or gender differences in our regression analyses examining social rejection in this mixed clinical-community sample. This could illustrate that, within our sample, males, females and transgender individuals were comparably vulnerable to BPD and feelings of social rejection. These findings also could be due to our small sample size, limiting the detection of sex and gender effects. Further research with larger samples of equally represented individuals is needed in order to make more accurate conclusions about gender identity in relation to BPD and social rejection.
Another important finding from this study was that the BPD x FAA interaction was predictive of feelings of overall social rejection above and beyond depression. The very strong association between BPD and depressive symptoms presents problems for diagnosticians working with adolescents, where BPD symptoms are typically overlooked as normative or part of depression in adolescents (Boylan, Reference Boylan2018). Additionally, heightened sensitivity to rejection is overrepresented in both BPD and depression samples (Ayduk et al., Reference Ayduk, Downey and Kim2001; Beeney et al., Reference Beeney, Levy, Gatzke-Kopp and Hallquist2014; Gunderson, Reference Gunderson2007; Kaess et al., Reference Kaess, Brunner and Chanen2014; Slavich et al., Reference Slavich, Thornton, Torres, Monroe and Gotlib2009). Future studies are needed that precisely target the association between BPD, depression and social rejection, given these important clinical considerations for identifying adolescents with BPD.
Our sample comprised adolescents who did not have any known mental health diagnosis, had a probable or definite BPD diagnosis, or who met diagnostic criteria for a disorder other than BPD. These clinical characteristics and the developmental stage of our sample participants were associated with heightened levels of emotion dysregulation, which is also a core feature of BPD. We controlled for BPD diagnosis status to account for any variance that those individuals with a probable or definite BPD diagnosis might be contributing to our overall results. Overall, our interaction effect predicted total social rejection scores above and beyond BPD diagnosis status. These are particularly important findings and should also be considered in future research since diagnostic classifications and groupings are often solely used in research and clinical practice (Stead et al., Reference Stead, Boylan and Schmidt2019).
Study Limitations
Our study should be considered in light of its limitations. First, we relied on a relatively small clinical sample, and a relatively smaller group of typically developing youth. More importantly, our participants comprised of a sample of convenience, meaning that we cannot generalize our results outside of our sample (Acharya et al., Reference Acharya, Prakash, Saxena and Nigam2013). Second, we only examined EEG power in two frontal (i.e., F3 and F4) and parietal (i.e., P3 and P4) electrode sites that were selected a priori given the role of these frontal sites in emotion dys/regulatory processes (see, e.g., Reznick & Allen, Reference Renneberg, Herm, Hahn, Staebler, Lammers and Roepke2018, for a recent review). However, the relatively small number of sites used limits our ability to fully interpret our results without knowing what other activity is occurring in other parts of the brain. Third, the measure of social rejection and EEG were assessed concurrently, so causal relations cannot be inferred. Fourth, the high degree of comorbid issues in the type of clinical sample used herein, could contribute to the pattern of BPD symptom effects. Although we considered and controlled for depression, anxiety, particularly social anxiety, might be contributing to the observed effects. Fifth, although we controlled for chronological age, we did not evaluate pubertal status, which could have identified developmental effects where age did not. Sixth, our sample consisted of predominantly White, cisgender and heterosexual adolescents. Therefore, caution should be taken when generalizing the findings to other non-White adolescents, and adolescents of different sexual orientations and gender identities. It is imperative that future research includes a wider range of participants from different ethnic/cultural and sexual minority backgrounds. Seventh, we used a Cz reference for our EEG data collection, and some investigators have been critical of this particular reference location for asymmetry work as it may confound findings (see Hagemann et al., Reference Hagemann, Naumann and Thayer2001). Finally, though all participants reported that their medications remained stable over the two-week testing period, we did not control for medication in our analyses. This was due to incomplete reporting (e.g., individuals being unaware of their medication dosage), numerous classes of psychotropic and non-psychotropic medications, and individual differences with medication adherence. Future studies should assess and control for the potential effects of medication on patterns of frontal brain activity over time.
Conclusions
BPD is a debilitating mental health disorder. Though there are numerous evidence-based treatments, the interpersonal dysfunction associated with BPD tends to persist after treatment and even remission of the disorder (Wright et al., Reference Wright, Zalewski, Hallquist, Hipwell and Stepp2016). Early identification and treatment of BPD produces greater symptom reduction and remission (Chanen & McCutcheon, Reference Chanen and McCutcheon2013; Kaess et al., Reference Kaess, Brunner and Chanen2014; Sharp & Wall, Reference Sharp and Wall2018). Due to adolescence being a peak period of BPD symptom emergence, it is imperative for us to study interpersonal dysfunction in adolescents with, or at risk of, developing BPD to identify opportunities for intervention (Conway et al., Reference Conway, Hipwell and Stepp2017; Courtney-Seidler, et al., Reference Crowley, Wu, Molfese and Mayes2013; Sharp & Wall, Reference Sharp and Wall2018).
Additionally, there is a large body of research that supports the use of neural correlates via FAA as a marker of emotional and motivational profiles (Coan & Allen, Reference Coan and Allen2004). The previous research on FAA in BPD is sparse, with inconsistent results due to differing methodologies (Beeney et al. Reference Beeney, Levy, Gatzke-Kopp and Hallquist2014; Flasbeck et al., Reference Flasbeck, Popkirov and Brüne2017; Popkirov et al., Reference Popkirov, Flasbeck, Schlegel, Juckel and Brüne2019). Our results may be interpreted within and inform the biosocial development and differential susceptibility models in understanding the relations among BPD, FAA, and rejection sensitivity. By better understanding FAA patterns in BPD, we can arguably better understand emotional functioning and motivational patterns and implement this knowledge in our treatments of BPD, especially in the area of interpersonal dysfunction, a stimulus of motivational tendencies.
Adolescence is a developmental period when rejection sensitivity is heightened (Levine et al., Reference Levine, Marziali and Hood1997; Tang, et al., Reference Tang, Lahat, Crowley, Wu and Schmidt2019), and late adolescence may denote a period when individuals experience greater negative feelings in relation to perceived social rejection (Marston et al., Reference Marston, Hare and Allen2010). Our results indicated no age differences in relation to BPD features in predicting feelings of social rejection. Thus, having symptoms of BPD might inherently place adolescents at an increased risk for experiencing heightened sensitivity to perceived rejection. However, this is a complex issue, and age alone does not provide enough information about developmental contexts.
In the era of social media, adolescents are now more exposed to negative perceptions, interactions, and feelings related to social rejection via social media (Lenhart et al., Reference Lenhart, Ling, Campbell and Purcell2010; O’Keeffe & Clarke-Pearson, Reference O’Keeffe and Clarke-Pearson2011). Having more exposure to social media, and thus an increased number of instances of social rejection (the invalidating environmental context), might have the potential to further reinforce BPD pathology. Therefore, given today’s social media climate, more research is needed to elucidate the development of BPD pathology and social rejection in adolescents in the context of social media.
Acknowledgments
A special thanks to the many participants and their family members who made the D-Psypher Project possible. We are also very grateful to Debra Hughes, who was instrumental in recruitment and data collection.
Funding statement
This study was supported by a Social Sciences and Humanities Research Council of Canada (SSHRC) Doctoral Fellowship awarded to VES, and operating grants from the Ontario Mental Health Foundation to KB and the SSHRC to LAS.
Conflicts of Interest
None.





