



Introduction
Traumatic brain injury (TBI) is the leading cause of disability in people under the age of 40 years worldwide (World Health Organization, 2006). Long-term consequences of TBI include cognitive, emotional and behavioural dysregulation, such as disinhibition and aggression, which are associated with a higher risk of suicidal or criminal behaviour (Arciniegas & Wortzel, Reference Arciniegas and Wortzel2014; Bahraini, Simpson, Brenner, Hoffberg, & Schneider, Reference Bahraini, Simpson, Brenner, Hoffberg and Schneider2013; Bellesi, Barker, Brown, & Valmaggia, Reference Bellesi, Barker, Brown and Valmaggia2019; Kim, Reference Kim2002). Both suicide attempts and criminal offences are tied to great suffering among individuals involved as well as society in general (Hvidkjær et al., Reference Hvidkjær, Ranning, Madsen, Fleischer, Eckardt, Hjorthøj and Erlangsen2021; Parsonage, Reference Parsonage2016).
TBI has been linked to both psychiatric illness and suicide (Madsen et al., Reference Madsen, Erlangsen, Orlovska, Mofaddy, Nordentoft and Benros2018; Orlovska et al., Reference Orlovska, Pedersen, Benros, Mortensen, Agerbo and Nordentoft2014), but systematic reviews have only identified few studies examining the association to non-fatal suicide attempt (Bahraini et al., Reference Bahraini, Simpson, Brenner, Hoffberg and Schneider2013; Fralick et al., Reference Fralick, Sy, Hassan, Burke, Mostofsky and Karsies2019), which have methodological shortcomings including small sample sizes. Recently, a large study (n = 157 995) suggested an elevated risk of suicide attempt after TBI (Chang et al., Reference Chang, Hsu, Wu, Huang, Chang, Bai and Chen2019), but these findings were restricted to adolescents and young adults only and were thus not representative for a broad demographic range.
Regarding TBI and criminal behaviour, cross-sectional data has revealed that up to 60% of incarcerated offenders have been exposed to TBI (Hughes et al., Reference Hughes, Williams, Chitsabesan, Walesby, Mounce and Clasby2015; Shiroma, Ferguson, & Pickelsimer, Reference Shiroma, Ferguson and Pickelsimer2012). Although an association between TBI and violent crime has been shown in cohort studies (Fazel, Lichtenstein, Grann, & Långström, Reference Fazel, Lichtenstein, Grann and Långström2011; McIsaac et al., Reference McIsaac, Moser, Moineddin, Keown, Wilton, Stewart and Matheson2016; McKinlay, Corrigan, Horwood, & Fergusson, Reference McKinlay, Corrigan, Horwood and Fergusson2014; Schofield et al., Reference Schofield, Malacova, Preen, D'Este, Tate, Reekie and Butler2015; Timonen et al., Reference Timonen, Miettunen, Hakko, Zitting, Veijola, Von Wendt and Räsänen2002), a recent review highlighted the need for longitudinal cohorts that include defined measures of TBI, its severity, a non-offending comparison group, adjusted analyses, and use of criminal records instead of self-reported data (Huw Williams et al., Reference Huw Williams, Chitsabesan, Fazel, McMillan, Hughes, Parsonage and Tonks2018). Furthermore, it remains to be examined whether specific types of violent crimes are linked to higher rates.
The objective of this study was to analyse whether individuals with hospital-diagnosed TBI had higher rates of subsequent suicide attempt and violent crime compared to individuals with no hospital-diagnosed TBI. The Danish registers allowed us to assess variation between rates of suicide attempt and violent crime with respect to TBI severity, multiple TBI and time since TBI in a retrospective cohort design, while controlling for important confounders. Such findings will aid the development of preventive efforts against negative trajectories after TBI.
Methods
Study design and population
A cohort study design was applied. All residents in Denmark have a unique personal identification number, which allows for the linkage of data from continuously updated national registries. Data were extracted from the Civil Registration System (Pedersen, Reference Pedersen2011), the National Patient Register (NPR) (Lynge, Sandegaard, & Rebolj, Reference Lynge, Sandegaard and Rebolj2011), the Psychiatric Central Research Register (PCCR) (Mors, Perto, & Mortensen, Reference Mors, Perto and Mortensen2011), the Register of Causes of Death (Helweg-Larsen, Reference Helweg-Larsen2011), the Database for Integrated Labour Market Research (Timmermans, Reference Timmermans2010), and the National Criminal Register (‘Criminal Codes – Statistics Denmark (In Danish),’ n.d.; Jensen, Greve, Høyer, & Spencer, Reference Jensen, Greve, Høyer and Spencer2006). Diagnoses in NPR and PCCR were recorded according to the International Classification of Diseases (ICD, 8th revision until 1 January 1994 and 10th thereafter).
All individuals aged 10 years or older who lived in Denmark at some point from 1 January 1980, through 31 December 2016 were included.
Exposures
Information on exposure to TBI was retrieved from the NPR. The register contains data on hospital admissions since 1977 and outpatient and emergency room contacts since 1995. TBI was categorised as mild TBI (concussions); fractures to the skull or spine (without documented structural brain injury); and severe TBI (with evidence of structural brain injury) (see eTable 1) as suggested by the American Congress of Rehabilitation Medicine and applied previously (American Congress of Rehabilitation Medicine, 1993; Christensen et al., Reference Christensen, Pedersen, Pedersen, Sidenius, Olsen and Vestergaard2009; Madsen et al., Reference Madsen, Erlangsen, Orlovska, Mofaddy, Nordentoft and Benros2018). The severity of TBI was classified in mutually exclusive categories; ranging from mild TBI through skull or spine fractures to severe TBI. The onset of exposure was defined as the date of the first TBI diagnosis. Multiple diagnoses of TBI recorded within a 30-day period were considered as related to the same episode.
Outcomes
Suicide attempts were identified using ICD-8 codes (E950–E959) and ICD-10 codes (X60–X84) or where the reason for contact was indicated as a suicide attempt in NPR and PCCR.
Information on convicted violent crimes of individuals aged 15 years or older (age of criminal responsibility in Denmark) derived from the National Criminal Register. Following conducts were considered as violent (eTable 2): sexual offences, violent threats, assault, homicide, attempted homicide, robbery, arson, vandalism, driving accidents, drunk driving, possession of a weapon in a public space, and terrorism. The date of the offence was considered as the onset time for the outcome.
Covariates
Information on sex (female, male), calendar period, age group (10–19, 20–29, …, 80+), educational level (elementary school, vocational training, high school, university degree, ongoing, or missing), socioeconomic status (employed, unemployed, disability pension, early retirement, retirement, student or other) and cohabitation status (cohabitation, no cohabitation) were obtained from the Civil Registration System and the Database for Integrated Labour Market Research. For individuals below the age of 20, we used parent's highest socioeconomic status and educational level instead of individuals own. In addition, Charlson comorbidity index (1, 2, 3, 4+) (Charlson, Pompei, Ales, & MacKenzie, Reference Charlson, Pompei, Ales and MacKenzie1987), non-CNS fractures (i.e. number of fracture diagnoses not involving the skull or spine; no, 1, 2, 3+), epilepsy (no, yes), and psychiatric illness diagnosed prior to TBI exposure (no, yes) were included (see eTable 1).
Follow up
Individuals were followed from 1 January 1980 until the end of a study on 31 December 2016. If a person migrated out of the country or died, they were censored at the date of the respective event. Likewise, persons were censored after experiencing the outcome of the study. If an outcome was recorded during the first hospital contact for TBI, the exposure was ignored; hence, the individual was considered unexposed but having experienced the outcome of the study.
Statistical analysis
Incidence rate ratios (IRR) with 95% confidence intervals were estimated by Poisson regression models comparing outcome rates of people exposed to TBI with those not exposed. Analyses were conducted separate for females and males due to the interaction of sex with exposure and outcome. The basic model was adjusted for age and calendar period, while the full model was additionally adjusted for educational level, socioeconomic status, cohabitation status, non-CNS fractures, epilepsy, Charlson comorbidity index and psychiatric illness. Associations were assessed with respect to severity (mild TBI, skull fracture, severe TBI), number of distinct hospital contacts (0, 1, 2, 3, 4, ≥5); time since last hospital contact (0–6 months, >6–12 months, >1–2 years, >2–3 years, >3–4 years, >4–5 years, >5–6 years, >6 years); and patient type (ER/outpatient v. inpatient treatment). Associations to different types of violent crimes were examined in separate models. As previous studies have demonstrated a higher occurrence of psychiatric illness among people with TBI in Denmark, (Orlovska et al., Reference Orlovska, Pedersen, Benros, Mortensen, Agerbo and Nordentoft2014) we examined in analyses confined to patients with TBI (1) whether rates of outcomes were higher in individuals with pre-TBI psychiatric illness compared to those without and (2) whether post-TBI psychiatric illness might act as a mediator by comparing rates of outcomes in individuals diagnosed with and without psychiatric illness after TBI. We used adjusted IRRs to estimate the population attributable risks (PAR). To validate our primary analyses, we conducted a sensitivity analysis where the sample was restricted to individuals born in 1976 or later, allowing for lifetime coverage of hospital admissions. Another sensitivity analysis further adjusted for parental background (educational level, socioeconomic status, suicidal or criminal behaviour and psychiatric illness).
All data processing and analyses were performed using SAS version 9.4. An anonymised data set was used for the analyses, and the project was approved by the Danish Data Protection Agency (RHP-2012-021).
Results
The study population consisted of 7 783 951 individuals (3 833 579 females and 3 950 372 males) who lived in Denmark at some point during 1980–2016 and were observed for a total of 172 398 267 person-years. In all, 587 522 individuals received a diagnosis of TBI where 443 971 (5.7%) were diagnosed with mild TBI, 24 800 (0.3%) with a skull fracture, and 118 751 (1.5%) with severe TBI. The median age at first diagnosis was 29 [interquartile range (IQR): 14–57] for females and 25 (IQR: 14–47) for males.
Suicide attempt
During the 37-year follow-up, 124 302 individuals (57% females) had at least one suicide attempt, of which 17 618 (14%) had experienced a TBI beforehand (eTables 3 and 4). The incidence rate of suicide attempt was 214.9 (95% CI 210.1–219.7) per 100 000 person-years for females with TBI v. 75.6 (95% CI 75.0–76.2) for those without (Table 1). The corresponding rates for males were 183.1 (95% CI 179.5–186.7) and 54.4 (95% CI 53.9–54.9), respectively. A higher IRR of suicide attempt was found for individuals with TBI (females IRR, 2.78; 95% CI 2.71–2.85; males IRR, 3.00; 95% CI 2.93–3.08) when compared to those without TBI. Higher IRRs were found for females exposed to mild TBI (2.84; 95% CI 2.76–2.91) than severe TBI (2.45; 95% CI 2.29–2.64) relative to females not exposed to TBI (p < 0.001). Males exposed to mild TBI also had higher IRRs (3.07, 95% CI 2.99–3.15) than those with severe TBI (2.73, 95% CI 2.58–2.89; p < 0.001) relative to males not exposed (p < 0.001).
Table 1. Suicide attempt incidence rates and incidence rate ratios by medical contact for traumatic brain injury

CI, confidence interval; IR, incidence rate; IRR, incidence rate ratio; PY, person-years; TBI, traumatic brain injury.
a Basic adjusted: Adjusted for calendar period, and age group.
b Fully adjusted: Adjusted for calendar period, age group, educational level, socioeconomic status, cohabitation status, non-CNS fractures, epilepsy, Charlson comorbidity index, and psychiatric illness.
Having multiple hospital contacts for TBI was associated with higher rates of suicide attempt in a dose-response association up to four TBI's (p ≤ 0.05; Fig. 1a and e Table 7). Relative to no TBI the IRR for females with one TBI was 2.57 (2.50–2.64), two TBIs 4.18 (3.93–4.45), three TBIs 4.95 (4.38–5.60), four TBIs 6.97 (5.66–8.58) and five or more TBIs 6.48 (5.02–8.34). The corresponding IRRs for males were; for one TBI 2.61 (2.54–2.68), two TBIs 4.57 (4.35–4.80), three TBIs 6.18 (5.69–6.72), four TBIs 7.27 (6.40–8.26) and five or more TBIs 7.21 (6.27–8.20). IRR was highest in the first 6 months after hospital contact for TBI (females IRR, 4.71; 95% CI 4.36–5.09; males IRR, 5.61; 95% CI 5.25–5.99) compared to those without TBI (Fig. 1b). Compared to people with no TBI or fractures, those with TBI had higher IRRs (females IRR, 2.73; 95% CI 2.66–2.80; males IRR, 3.03; 95% CI 2.96–3.10) than those with non-CNS fractures (females IRR, 1.44; 95% CI 1.40–1.47; males IRR, 1.54; 95% CI 1.50–1.58) (p < 0.001; Fig. 1c).
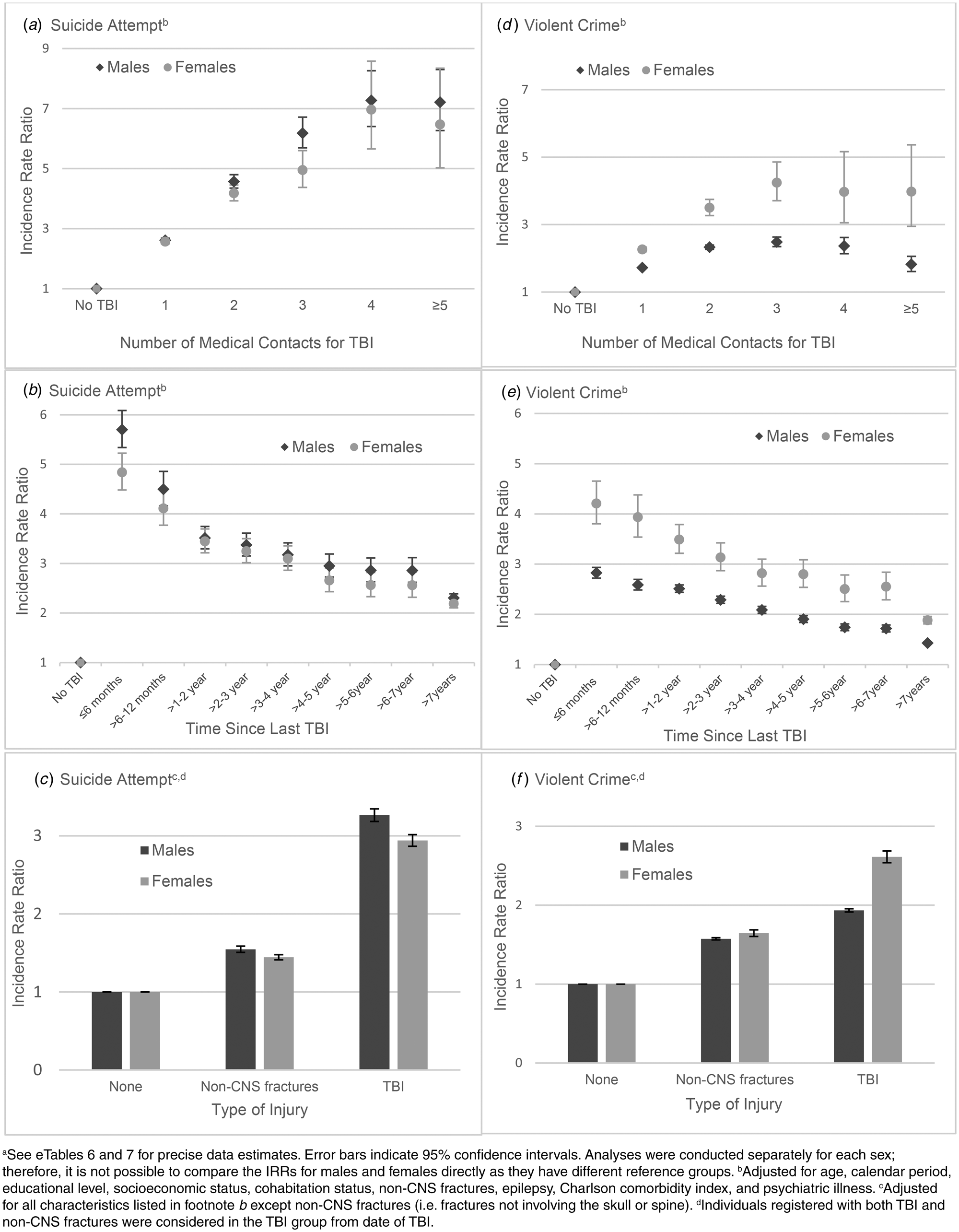
Fig. 1. Incidence rate ratios of suicide attempt and violent crime in individuals with TBI, 1980–2016a.
Individuals diagnosed with psychiatric illness before their TBI had higher rates of suicide attempt (females IRR, 5.24; 95% CI 4.92–5.57; males IRR, 3.18; 95% CI 2.96–3.27) (Table 2) than those with TBI only. Likewise, individuals first diagnosed with the psychiatric illness after TBI had higher IRR's (females IRR, 14.81; 95% CI 14.02–15.65; males IRR, 12.44; 95% CI 11.88–13.03) than those with TBI only.
Table 2. Suicide attempt and violent crime incidence rates and incidence rate ratios among individuals with TBI, according to the timing of first psychiatric diagnosis

CI, confidence interval; IR, incidence rate; IRR, incidence rate ratio; PY, person-years; TBI, traumatic brain injury.
a Basic adjusted: Adjusted for calendar period, and age group.
b Fully adjusted: Adjusted for calendar period, age group, educational level, socioeconomic status, cohabitation status, non-CNS fractures, epilepsy, and Charlson comorbidity index.
PAR for females and males with TBI were 6.8% (95% CI 6.6–7.1) and 11.3% (95% CI 10.9–11.7) for suicide attempts, respectively. This indicates the proportion of total suicide attempts, which could be avoided if it was possible to reduce TBI, under the assumption that the association is causal and not due to confounding.
In a sensitivity analysis, where the sample was restricted to individuals born after 1976 to have a complete follow-up from birth, associations between TBI and suicide attempt (females IRR, 3.20; 95% CI 3.04–3.38; males IRR, 3.13; 95% CI 2.99–3.27) remained (eTable 9). When further adjusting for parental background information, such as socioeconomic status and suicidal behaviour, associations also remained (females IRR, 2.55; 95% CI 2.46–2.65; males IRR, 3.27; 95% CI 3.10–3.45).
Violent crime
In all, 494 348 individuals (11% females) were convicted of one or more violent crimes, of which 52 451 (11%) had experienced a TBI beforehand (eTables 5 and 6). Female incidence rates were 180.0 (95% CI 175.6–184.4) per 100 000 person-years for those with TBI compared to 59.8 (95% CI 59.2–60.3) among those without (Table 3). For males, the corresponding rates were 1096.9 (95% CI 1086.9–1107.0) and 531.1 (95% CI 529.4–532.7), respectively. Higher IRRs of violent crime were found for females (IRR, 2.43; 95% CI 2.36–2.49) and males (IRR, 1.80, 95% CI 1.78–1.82) with TBI compared with individuals without TBI. When assessing rates for different types of crimes, higher rates were obtained for people with TBI across all groups (Table 4).
Table 3. Violent crime incidence rates and incidence rate ratios by medical contact for traumatic brain injury

CI, confidence interval; IR, incidence rate; IRR, incidence rate ratio; PY, person-years; TBI, traumatic brain injury.
a Basic adjusted: Adjusted for calendar period, and age group.
b Fully adjusted: Adjusted for calendar period, age group, educational level, socioeconomic status, cohabitation status, non-CNS fractures, epilepsy, Charlson comorbidity index, and psychiatric illness.
Table 4. Specific violent crimes incidence rates and incidence rate ratios in individuals with and without a traumatic brain injury diagnosis

IR, incidence rate; IRR, incidence rate ratio; TBI, traumatic brain injury.
a Rate per 100 000 person-years.
b Adjusted for calendar period, age group, educational level, socioeconomic status, cohabitation status, non-CNS fractures, epilepsy, Charlson comorbidity index, and psychiatric illness.
c Including assault, aggravated assault, threats, homicide and attempted homicide.
Multiple hospital contacts for TBI was associated with higher crime rates in a dose-response association up to three TBI's (p < 0.05; Fig. 1d and e Table 8). Relative to no TBI the IRR for females with one TBI was 2.26 (2.20–2.33), two TBIs 3.50 (3.27–3.75), three TBIs 4.24 (3.71–4.86), four TBIs 3.97 (3.05–5.16) and five or more TBIs 3.98 (2.95–5.37). The corresponding IRRs for males were; for one TBI 1.72 (1.70–1.74), two TBIs 2.33 (2.27–2.39), three TBIs 2.49 (2.35–2.63), four TBIs 2.37 (2.14–2.62) and five or more TBIs 1.82 (1.61–2.06). However, males with 4 TBI's had higher IRR (2.37; 95% CI 2.14–2.62) than males with ≥5 TBI's relative to no TBI (p < 0.001). The IRR was highest in the first 6 months after a hospital contact for TBI (females IRR, 4.21; 95% CI 3.80–4.65; males IRR, 2.83; 95% CI 2.72–2.94) compared to those without TBI (Fig. 1e). In comparison to people with no TBI or fracture, elevated rates were noted for those with TBI (females IRR, 2.00; 95% CI 1.89–2.12; males IRR, 1.93; 95% CI 1.91–1.96) and those with non-CNS fractures (females IRR, 1.65; 95% CI 1.60–1.69; males IRR, 1.57; 95% CI 1.56–1.59; Fig. 1f). For males, a lower crime rate was noted for those whose TBI required inpatient treatment (IRR, 0.92; 95% CI 0.90–0.94) than for those exclusively treated in ER or outpatient settings.
Individuals with psychiatric illness before TBI had higher rates of violent crime (IRR for females, 3.18; 95% CI 2.96–3.41; IRR for males, 2.25; 95% CI 2.26–2.35) than those with TBI only. Likewise, individuals first diagnosed with the psychiatric illness after TBI had higher rates (females IRR, 4.02; 95% CI 3.77–4.27; males IRR, 2.38; 95% CI 2.31–2.45; Table 2) than those with TBI only.
PAR for violent crime of 5.6% (95% CI 5.3–5.8) and 4.1% (95% CI 4.0–4.2) were found for TBI-exposed females and males, denoting the proportion of crimes that might be avoided if it was possible to reduce TBI incidents to zero, under the assumption that the association is causal and not due to confounding
The association between TBI and violent crime (females IRR, 2.43; 95% CI 2.31–2.55; males IRR, 2.20; 95% CI 2.17–2.23) remained when restricting the sample to those with complete data on background factors (eTable 9). Also, when further adjusting for parental background, such as socioeconomic status and criminal behaviour (females IRR, 2.55; 95% CI 2.46–2.65; males IRR, 3.37; 95% CI 3.10–3.45).
Discussion
We found that TBI was associated with elevated rates of suicide attempt and violent crime. Rates were highest within the first 6 months after a hospital contact for TBI, suggesting a temporal proximity association, and also higher after multiple TBI contacts. Associations could be mediated by psychiatric illness, as rates of suicide attempt and violent crime were higher among individuals who were diagnosed with a psychiatric illness following TBI than those with TBI but no psychiatric illness.
TBI is a major public health concern; although 76% of the exposed in this study were classified as mild TBI, these can still result in long-term consequences (Ryan & Warden, Reference Ryan and Warden2003; Sariaslan, Sharp, D'Onofrio, Larsson, & Fazel, Reference Sariaslan, Sharp, D'Onofrio, Larsson and Fazel2016). The high prevalence of TBI globally emphasises the importance for preventing TBI to mitigate sequalae, especially for high-risk groups such as veterans or victims of traffic accidents (Feigin et al., Reference Feigin, Theadom, Barker-Collo, Starkey, McPherson, Kahan and Ameratunga2013; Peeters et al., Reference Peeters, van den Brande, Polinder, Brazinova, Steyerberg, Lingsma and Maas2015). The importance of informing physicians and patients about the risk of adverse outcomes after TBI are emphasised by the fact that 14% of all people with a suicide attempt and 11% of those with a violent crime had experienced a TBI beforehand. Further, PAR estimates indicate that as many as 11% of suicide attempts and 6% of violent crimes in Denmark may be avoided by preventing TBI, if the association is causal. These high-risk estimates are from a high welfare Scandinavian country with access to free health care and good possibilities of rehabilitation after brain injury. Thus, the risk of suicide attempt and violence ascribed to TBI could potentially be higher in areas with less possibility and lower quality of treatment after TBI.
To our knowledge, this is the first nationwide study to assess rates of suicide attempt after TBI for all age groups. The rate ratios for suicide attempt obtained in this study were lower than those reported for young persons (Chang et al., Reference Chang, Hsu, Wu, Huang, Chang, Bai and Chen2019). In addition to sample differences, we accounted for an extensive list of potential confounders, such as other injuries and epilepsy, which might explain the difference. In contrast to earlier reports on suicidal behaviour, we found an inverse association with the severity of TBI (Chang et al., Reference Chang, Hsu, Wu, Huang, Chang, Bai and Chen2019; Madsen et al., Reference Madsen, Erlangsen, Orlovska, Mofaddy, Nordentoft and Benros2018). It is possible that the severity of the TBI might have affected the person's likelihood of having a suicide attempt because of, for instance, serious disabilities as a result of the TBI, increased medical attention averted adverse mental health outcomes, or suicidal acts tended to be fatal rather than non-fatal after severe TBI.
Our findings regarding the risk of violent crime after TBI support previous findings although levels of risk differed (Fazel et al., Reference Fazel, Lichtenstein, Grann and Långström2011; McIsaac et al., Reference McIsaac, Moser, Moineddin, Keown, Wilton, Stewart and Matheson2016; McKinlay et al., Reference McKinlay, Corrigan, Horwood and Fergusson2014; Schofield et al., Reference Schofield, Malacova, Preen, D'Este, Tate, Reekie and Butler2015; Timonen et al., Reference Timonen, Miettunen, Hakko, Zitting, Veijola, Von Wendt and Räsänen2002). The difference could be due to diverging measures (e.g. self-reported crimes (McKinlay et al., Reference McKinlay, Corrigan, Horwood and Fergusson2014) or including all types of crimes (McIsaac et al., Reference McIsaac, Moser, Moineddin, Keown, Wilton, Stewart and Matheson2016)), small sample size (Timonen et al., Reference Timonen, Miettunen, Hakko, Zitting, Veijola, Von Wendt and Räsänen2002), or a less comprehensive assessment for potential confounders (Fazel et al., Reference Fazel, Lichtenstein, Grann and Långström2011; McKinlay et al., Reference McKinlay, Corrigan, Horwood and Fergusson2014; Timonen et al., Reference Timonen, Miettunen, Hakko, Zitting, Veijola, Von Wendt and Räsänen2002). Associations for different types of violent crimes have, to our knowledge, not been examined before, and we found elevated rates for all types of crime after TBI. Previous findings stratified by sex (McIsaac et al., Reference McIsaac, Moser, Moineddin, Keown, Wilton, Stewart and Matheson2016; Schofield et al., Reference Schofield, Malacova, Preen, D'Este, Tate, Reekie and Butler2015) did not report differences between males and females with respect to risk of violent crime after TBI when comparing those with and without TBI. Even though females had lower, absolute rates of violent crime than males, we observed the highest increase in the IRR among females with TBI compared to females without TBI. This could suggest that females' risk of violent crime might be stronger affected by TBI, possibly due to the low base rate of violent crimes among females without TBI, whereas the base crime rate among males without TBI is rather high (i.e. there is a ceiling effect for males).
While our findings cannot establish causality, they support the perception that sequalae of TBI, such as behavioural dysregulation, psychiatric symptoms, aggression or disinhibition, could lead to suicidal or criminal behaviour (Arciniegas & Wortzel, Reference Arciniegas and Wortzel2014; Bahraini et al., Reference Bahraini, Simpson, Brenner, Hoffberg and Schneider2013; Bellesi et al., Reference Bellesi, Barker, Brown and Valmaggia2019; Kim, Reference Kim2002; Orlovska et al., Reference Orlovska, Pedersen, Benros, Mortensen, Agerbo and Nordentoft2014). It is also possible that individuals with risk-taking behaviours or substance abuse, which both are associated with suicidal and criminal behaviours, are more prone to accidents and TBI (Huw Williams et al., Reference Huw Williams, Chitsabesan, Fazel, McMillan, Hughes, Parsonage and Tonks2018; Weil, Corrigan, & Karelina, Reference Weil, Corrigan and Karelina2018). The fact that having multiple TBI episodes was linked to elevated rates of suicide attempt and violent crime, could support a hypothesis of a behavioural phenotype. This was further explored by accounting for proneness to accidents; firstly, by controlling for non-CNS fractures and, secondly, by comparing those with TBI with non-CNS fractures. However, the higher rates of both outcomes for individuals with TBI than for those with non-CNS fractures suggest that a behavioural phenotype is not the only explanation for increased rates after TBI. To explore whether heredity might be a driving force for the association, we adjusted for parental psychiatric illness and suicidal or criminal behaviour in a sensitivity analysis; however, this did not alter the results.
Strengths and limitations
This study had several strengths. First, a large nationwide cohort was studied over a long period with no or little loss to follow-up (Pedersen, Reference Pedersen2011). Second, the precision of estimates was improved by using records, such as diagnoses and verdicts, rather than self-reported data, adjusting for potential confounders, and using time-varying covariates, while presenting separate estimates for males and females. Third, longitudinal data ensured that TBI exposure occurred prior to the outcomes of the study, hence, avoiding potential reverse causation.
Limitations should also be noted. First, mild TBI could be under-recorded as some individuals might not seek hospital treatment and ER and outpatient contacts were not recorded prior to 1995. Second, suicide attempts (Morthorst, Soegaard, Nordentoft, & Erlangsen, Reference Morthorst, Soegaard, Nordentoft and Erlangsen2016) and violent crimes were likely under-recorded; implying that our estimates might be conservative. Third, information on provided treatment for TBI was not available, which may impact the risk of outcomes. Fourth, as NPR was initiated in 1977, individuals with TBI or suicide attempt prior to this time could bias results in a conservative direction; yet, sensitivity analysis with lifetime follow-up supported the overall results. Fifth, the first time of diagnosis of psychiatric illness might not reflect the true time of onset of illness and some psychiatric disorders might not be treated in hospital settings. Therefore, information about psychopathology as well as additional covariates, such as suicidal thoughts, home violence or early behavioural problems might have added further value to our analyses.
Conclusion
In this nationwide, registry-based cohort study, we found that individuals with hospital contact for TBI had increased rates of suicide attempt and violent crime, when compared to the general population without TBI. Rates were highest in the time shortly after diagnosis, suggesting that preventive efforts at the time of or soon after TBI diagnosis may help mitigate the trajectories toward suicidal or violent behaviour.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0033291722000769
Conflict of interest
None.







