



Multilumen peripherally inserted central catheters (PICCs) remain a common practice outside the critical care setting. Reference Climo, Diekema and Warren1,Reference Chopra, Flanders and Saint2 This practice may be due to lack of awareness of guidelines, resultant harms, or staff or patient convenience. Reference Chopra, Flanders and Saint2,Reference McMahon, Beyth and Burger3 Additionally, multiple lumens may be requested in anticipation of future needs. Reference Bozaan, Skicki and Brancaccio4 Although there are benefits relative to temporary central venous access catheters, a higher risk of complications remains relative to single-lumen PICCs, including central-line bloodstream infections (CLABSIs), thromboses, and occlusions. Reference Chopra, Ratz, Kuhn, Lopus, Chenoweth and Krein5,Reference Chopra, Kaatz and Grant6 These complications lead to prolonged length of stay and added healthcare costs. Reference Chopra, Flanders and Saint7
Previous interventions reduced unnecessary multilumen PICCs in academic centers. Reference Bozaan, Skicki and Brancaccio4,Reference O’Brien, Paquet, Lindsay and Valenti8,Reference Lam, Volling and Chan9 Although successful, they were implemented within smaller settings such as units and single centers. Additionally, these interventions were labor intensive and relied on significant resource utilization. The electronic health record (EHR) can be an effective tool in implementing wide-scale change with limited resources. A “nudge” is an intervention that changes how choices are presented to the provider to account for predictable ordering patterns and to improve decision making. Reference Last, Buttenheim, Timon, Mitra and Beidas10 The use of nudges, particularly within the EHR, allows for easier approval, implementation, and data collection across large, complex healthcare settings. Default nudges are often the most impactful and user friendly in that they do not add additional click burden. Reference Last, Buttenheim, Timon, Mitra and Beidas10 Here we describe a nudge-focused EHR intervention aimed to improve single-lumen PICC use across a large safety net health system.
Methods
Study design and setting
This quality improvement initiative was developed at New York City Health + Hospitals (NYC H + H), the largest public health system in the United States, comprising 11 teaching hospitals and >70 ambulatory centers (Supplementary Table 1 online). Our project was deemed a quality improvement project by the NYC H + H central research office; thus, an institutional review board submission was not required.
Table 1. Preintervention Versus Postintervention Percentage of Single-Lumen PICC Use

Note. PICC, peripherally inserted central catheter.
a Difference = postintervention minus preintervention.
* P < .05; **P < .01; ***P < .001.
Intervention
The intervention was led and designed by the System High Value Care Council at NYC H+H with interdisciplinary input from experts in infectious disease, internal medicine, critical care, infection control, quality and safety, interventional radiology, and nursing across the system.
Although the workflow regarding placement of a PICC line is different at each hospital, all hospitals use a consultation order as the first step. We therefore modified the EHR consultation order for interventional radiology (Fig. 1). In 2 hospitals with vascular access teams, the consultation orders for these vascular access teams were modified in the same way. If the PICC line is selected, the options for “single lumen” or “other” appear, with a default selection to single-lumen PICC. If the provider selected the “other” option, a cascading menu would appear with higher lumen counts (double or triple). Educational text was placed within the order stating the institutional guidelines for multiple lumens including vasopressors, total parenteral nutrition, chemotherapy with multiple-lumen needs, or multiple peripherally incompatible medications. The initiative was introduced in a one-time e-mail to clinical leadership across the system. No additional system-wide interventions targeted appropriate line placement.

Fig. 1. Default nudge for single-lumen PICC insertion.
Measures and Statistical Analysis
Our outcome measure was the proportion of single-lumen PICCs inserted out of the total number of PICCs. The preintervention period (January 2, 2020, to May 2, 2021, 16 months) was compared with the postintervention period (May 3, 2021, to July 31, 2022, 15 months). We measured the intervention’s system-wide impact using 2 approaches. First, we performed a quasi-experimental interrupted time-series binomial regression. Individual data points consisted of weekly proportions of single-lumen PICC usage. Two separate regression lines were generated using the weekly proportions, one for the preintervention period and another for the postintervention period. The difference in the line intercepts at the intervention date allowed us to measure the immediate change in single-lumen PICC utilization (ie, level difference). The differences in the temporal slopes of the lines allowed us to compare longer-term trend changes (ie, slope difference). These differences were compared via multivariate t tests. Additionally, a counterfactual preintervention regression line was extended into the postintervention period to show predicted single-lumen PICC utilization in the absence of an intervention. The second approach compared average preintervention versus postintervention average single-lumen PICC utilization, without adjusting for temporal trends, using a binomial regression with a binary variable for the postintervention period. To ensure that the patient population was similar before and after the intervention, median age and length of stay were compared for patients with documented PICC placements. These were all statistically compared using an unpaired t test assuming unequal variance (ie, the Welch test).
Next, we compared the preintervention versus the postintervention monthly CLABSI counts, correlating PICC lines to CLABSIs. Statistical significance was measured using a Poisson regression. National Healthcare Safety Network definitions (2020–2022) for CLABSIs were used. We stratified preintervention versus postintervention PICC lumen counts by hospital. We also stratified postintervention PICC placement orders by lumen count and provider type and specialty to better understand differences in utilization.
Data were abstracted through SQL queries on the Epic Clarity database and were analyzed statistically using R version 4.0.3 software (R Foundation for Statistical Computing, Vienna, Austria, 2020). Data for PICC lines were analyzed from lines, drains, and airway documentation updated by nursing staff. Data from clinician orders were also analyzed.
Results
Patient and hospital characteristics are presented in the Supplementary Material (online). Single-lumen PICC utilization significantly increased compared to the preintervention period (Table 1). When not adjusting for temporal trends, average single-lumen PICC utilization increased by 25.5%, from 44.4% to 69.9% (P < .001). When adjusting for temporal trends, there was no significant slope difference (Fig. 2). We detected a significant level difference, with utilization increasing by 22.2%, from 46.7% to 68.9% at the intervention date (P < .001). When examining CLABSI rates from PICC lines, the CLABSI rates had a nonsignificant reduction by 26.7% from 2.44 to 1.79 infections per month (P = .255). Median age was unchanged before the intervention versus after the intervention (61.0 vs 61.0 years; P = .76), as was length of stay (12.9 days vs 13.6 days; P = .65), along with other patient demographics including sex, race, and insurance status (Supplementary Table 2 online). Notably, total PICCs decreased from the preintervention to the postintervention period (Table 1); the average weekly PICC placement rate decreased from 46.7 to 42.2 (P = .00169).

Fig. 2. Binomial regression of single-lumen PICC usage as a percentage of total PICCs.
Table 2. Postintervention PICC Utilization by Provider Type and Provider Specialty

Note. PICC, peripherally inserted central catheter; APP, advance practice practitioner; NP, nurse practitioner; PA, physician assistant.
We detected heterogeneity when stratifying postintervention PICC placement orders by provider type and by specialty type. When comparing provider types, fellows had the highest single-lumen PICC utilization at 94.6%, whereas physician associates (PAs) and nurse practitioners (NPs) had the lowest utilization at 67.7% (Table 2). When comparing specialty types, orthopedics had the highest single-lumen PICC utilization at 97.7%, whereas neurology had the lowest utilization at 31.8% (Table 2).
Increases in single-lumen PICC utilization stratified by hospital ranged from 3.7% at Woodhull Hospital to 63.0% at Lincoln Hospital (Table 3). Lower increases were observed at hospitals with high single-lumen PICC utilization before the intervention such as Woodhull Hospital (77.9%), Coney Island Hospital (78.9%), and Kings County Hospital (60.8%). Similarly, larger increases were observed in hospitals with the lowest preintervention single-lumen PICC utilization: Lincoln Hospital (18.0%), Jacobi/North Central Bronx (NCB) Hospital (23.1%), and Harlem Hospital (35.4%). Notably, hospital data for Jacobi and NCB were combined into a single entity based on their similar data-reporting structures.
Table 3. Preintervention Versus Postintervention Single-Lumen PICC Use by Hospital a
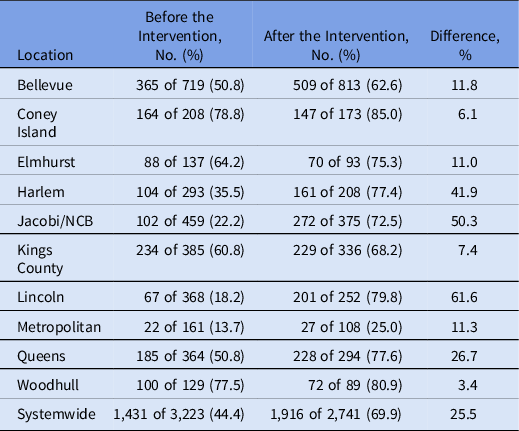
Note. PICC, peripherally inserted central catheter; NCB, North Central Bronx Hospital.
a Percentage based on total PICCs (single, double, and triple lumen).
Discussion
We successfully increased single-lumen PICC use and reduced potentially unnecessary multilumen use across 11 hospitals. This research expands on previous work that employed default nudges, with implementation across a larger, resource-limited setting. Reference Bozaan, Skicki and Brancaccio4,Reference Lam, Volling and Chan9 Although it was not statistically significant, we noted a relative reduction in PICC-related CLABSI rates by 27%; thus, a longer postintervention study period may be needed.
Our 26% increase in single-lumen PICC use was less than the 48% increase reported by Lam et al. Reference Lam, Volling and Chan9 This difference may be attributed to their concurrent local publicity campaign, as they announced within their meetings and rounds within units and teams. Education and awareness campaigns are more effective in smaller settings, possibly creating this significant additive effect. Reference Soong and Shojania11 Although we sent a mass e-mail to executive and clinical leadership, practically, we were unable to speak in person in each of the local units or services across 11 hospitals. Interestingly, when comparing our increase with Bozaan et al Reference Bozaan, Skicki and Brancaccio4 (29%), our results were similar. Their intervention was more robust, including having their vascular-access service team review the appropriateness of indications and escalating to clinical pharmacists when inappropriate. However, their single-lumen PICC use likely reached a ceiling at 94%, and a larger increase may have manifested if their baseline use had been lower.
Significant variation was observed among provider types and provider specialties. Among provider types, we observed lower use of single-lumen PICCs after the intervention among advanced practice providers (APPs; 67.7%) compared to physicians (82.4%–94.6%). This novel finding warrants further study; there may be opportunities to investigate APP attitudes regarding vascular access that explain this difference from physicians. In broader context, previous research regarding overuse among APPs versus physicians is mixed. Reference Roman, Yang, Masciale and Korenstein12–Reference Hughes, Jiang and Duszak14 Among provider specialties, there was a wide range of single-lumen PICC utilization (31.8%–97.7%), with neurology and neurosurgery having the lowest rates. Although there may be a higher need for multiple lumens among certain specialties, this variation may also reflect areas in which education and additional reinforcement could be beneficial. We were unable to obtain preintervention provider type and provider specialty data due to the lack of PICC lumen options on the previous consultation orders. Future investigation on the effect of nudge interventions for reducing overuse on these variables could be beneficial.
Significant variation was noted across individual hospitals. This finding may represent differences in clinician engagement and willingness to change their practice to placing single-lumen PICCs. Larger increases were observed in hospitals with the lowest preintervention single-lumen utilization: Lincoln (18.0%), Jacobi/NCB (16.8%), and Harlem (35.4%). This finding suggests that with appropriate nudging, providers are open to changing their clinical practice.
Implementation within safety net systems remains challenging. Understaffing and high staff turnover are mentioned nearly universally in literature, along with “self-siloing” and delayed uptake of newer practices. Reference Lyles, Handley and Ackerman15 Thus, low-effort, high-impact interventions are critical to improving value within resource-limited settings. Models for prioritization of projects, such as those used by Stinnett-Donnelly et al, Reference Stinnett-Donnelly, Stevens and Hood16 may prove more useful in safety net systems. Our intervention may provide an additional framework for improving value with limited resources.
This study had several limitations. First, this intervention lacked randomization or concurrent control. Second, our analysis did not include other complications of PICCs (eg, thrombosis or occlusion) or alternative intravenous access usage. We also suspect that in rare instances, PICC lines were placed outside of the EHR workflow, with a potentially marginal effect on this intervention. Additionally, our initiative does not address or assess the appropriateness of PICC placement over alternative IV access. Notably, our data relied on accurate documentation in the Lines, Drains, Airways (LDA) section of the chart, and though documentation patterns likely did not change before versus after the intervention, there may be some inaccuracies in the data. Lastly, this intervention occurred during the coronavirus disease 2019 (COVID-19) pandemic, including during surges. Hospital-acquired conditions, such as CLABSIs, increased significantly during this period, which may limit generalizability of our findings to nonpandemic periods. Reference Fakih, Bufalino and Sturm17 However, the positive effect of this intervention across the hospitals remains intact.
This initiative successfully improved single-lumen PICC line usage across a 11-hospital safety net health system. Further study is needed to understand effectiveness of default nudge interventions among different provider types and specialties.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/ice.2022.306
Acknowledgments
Financial support
No financial support was provided relevant to this article.
Conflicts of interest
All authors report no conflicts of interest relevant to this article.







