

On 6 December 1962, a Daily Mail headline announced: ‘12 People get notes from a Dead Man’. The newspaper article explained how a suicide victim had sent a letter outlining his decision to take his life ‘to his solicitors, his accountant, his bank manager, his next door neighbour, relatives and friends, a coroner and even the police’. Mr Herbert Jones, aged 77, resided in Southcliffe Road in Christchurch, Hampshire. He worked as a Borough engineer for his local council. Shortly after retirement, he was diagnosed with a terminal illness and his note explained that:
The necessity for hospital treatment is obviously becoming more and more imminent. I feel, however, unable to face the liability of causing so much inconvenience to a number of people, especially at this time of year, and so having the firm belief that my life is entirely my own responsibility, I have decided to end it by asphyxia. I am sorry to inflict this on you. … I wish to leave my body to Bristol University for research [sic].1
His neighbour Mr Reginald Wells explained to a Daily Mail reporter that the eloquence of the suicide note was typical of the deceased: ‘He was that sort of man, orderly, quiet and unselfish. He hated being a trouble to people.’ Further police enquiries established that Mr Jones had bought his family home, in which he committed suicide, for his only son. Sadly, the son had died a few months earlier, though the circumstances were not elaborated in the press. Jones had, according to neighbours, been bereft because he faced a double bereavement. His wife had died the year before in April 1961. Like Francis Partridge in Chapter 3, Herbert Jones was unable to cope with the pain of being both a widower and bereaved parent. Diagnosed as suffering from an incurable medical condition, he saw no reason to go on. Grief and memories did not outweigh his rationale that the quality of his life had been fundamentally diminished. An Inquest concluded that suicide was a measured decision. Jones wanted to cause the least disruption to medical staff at Christmas.2 Yet, ironically, the last request in his suicide note was to cause a lot of official consternation. As a Daily Mail reporter explained: ‘Mr. Jones’s last wish – to give his body to science – cannot be granted. The coroner has ordered a post-mortem.’ This simple statement published as a byline to the headline story exposed an explicit body dispute – on twelve prior occasions Jones had expressed in writing his explicit wishes to donate his body to medical research, which the coroner had the powers to countermand. As we shall see, this situation was in fact common because of the longevity of the powers, and ingrained procedural flaws, of the Coronial Office in the modern era: the central focus of this chapter.
Essentially, therefore, this fifth chapter is about these sorts of explicit disputes concerning the power and control over the dead body, body ethics and the boundaries and limits of professional practice, involving the official figure of the coroner. The chapter is thus split into two halves. In the first half we will encounter a brief history of the Coronial Office in England, before then engaging with a series of stories about explicit body disputes involving specific coroners. We will be focussing on the symbolic story of a dead girl called Carol Morris because the circumstances of her harvested human material proved to be very controversial. Her case exemplifies why tracking the material journeys of post-mortem bodies and their body parts matters in hidden histories of the dead. The details are lengthier than others presented so far in this book but that is because it was to be legally a very significant case. Thus, in the second half of the chapter, we explore why one human story is a historical prism for lots of others, and how micro-history can inform macro-trends of considerable longevity. In fact, as we shall see, the Carol Morris case made a significant contribution to establishing the legal precedent of anonymity for all donors in national and international law. Today, this remains in place, and we will be reflecting on the status quo of that standard of medical ethics, since the story behind its legal precedent is not known in the literature.
In other words, we will be asking: Does knowing the human circumstances of such cases change the way we view the ownership of the body once we know more about explicit body disputes, and what exactly were the long-term medico-legal ramifications of these stories that we have seldom thought about in the modern era of scientific achievement because they were neglected in the archives? In order not to dissect the storylines in the way that bodies were dissected and disassembled routinely inside the medical research community, with their human stories subsumed into a bio-commons, we will be looking in a little more detail this time at all the human factors and facets involved in the chosen representative cases. This means that the reader might wish to pause after the chapter’s first half, before discovering in the second half of this lengthier chapter the universal lessons that can be drawn from the newly discovered source material and the reasons for their historical longevity.
Our central analytical focus therefore is the palette and power exercised by coroners once a dead body was in their jurisdiction, despite explicit body disputes that were being generated between medico-legal officials and grieving relatives wanting to fulfil their loved ones’ dying wishes. It is also the case that in a transplant era the technical ability to harvest organs brought the Coronial Office into open conflict with the medical sciences. Historians of medicine have only very recently begun to examine these professional stand-offs through detailed case study, with most accounts still overly reliant on broad brush central government papers.3 Meanwhile, the lack of efficiency of the Coronial Office meant that important evidence about causes of death on coroners’ death certificates got lost inside the systems of forensic medicine and pathology, which should have been a ‘treasure trove of information’. Instead ‘real causes of death’ remained ‘hidden because of indifferent post-mortem examinations’ conducted hastily and which were often ‘obscured by deficient recording of data’.4 That common situation did not come to full public attention until the publication of the National Confidential Enquiry into Patient Outcome and Death in 2006 (hereafter NCEPOD). The National Patient Safety Agency commissioned the NCEPOD report into the professional conduct of the Coronial service because there were serious misgivings about its extensive powers of retention. It concluded that the system of certified autopsies had structural flaws throughout the twentieth century. Paradoxically, the history of explicit body disputes co-ordinated by the Coronial Office was one of many missed research opportunities for biomedicine too. We begin therefore with a short overview of the history of the Coronial Office in England.
Part I
The Coronial Office in Context
The history of the Coronial Office in England is one of slow expansion from the twelfth to early nineteenth centuries, during which the majority of coroners were legally, rather than medically, qualified.5 On average in England, they consistently dealt with about 5 per cent of all reported deaths from the early modern to modern period. Their main official responsibility was to investigate ‘unnatural deaths’ in the community. They did so by sifting gossip, and retrieving any relevant physical evidence at the scene of a death until foul play could be ruled out, or not. Coroners were under legal instruction, however, to wait until a suspicious death was reported to them. They had no official powers to investigate an unusual death. Legislation did not permit them to act just because they suspected that an unnatural or violent act of some description had occurred in their area of authority. Once, however, a suspicious death was reported officially to them and they had retrieved a dead body in their jurisdiction, they had a great deal of discretionary power. They could, for instance, decide how much to cut open the deceased or to leave the body intact. Each coroner could also waive the need for an Inquest if a cause of death in their opinion was obvious at a suicide or the scene of an accident at work or in the home. In this way, Coronial justice was often ‘remade from the margins’ because it involved a lot of discretionary powers of decision-making delegated to individual coroners.6
In suspicious circumstances, coroners have always been required to co-ordinate a ‘view of the body’.7 Normally from the thirteenth to the early twentieth century, this occurred within twelve hours of death. It involved calling a jury to service, composed of up to twelve local ratepayers respected for their social standing. The jury would congregate at a public house or another convenient place such as a gaol room or town hall. Here, a coroner’s assistant laid out the dead and jury members undertook a visual inspection of the deceased, looking for flesh wounds and suspicious bruising. This autopsy meant literally looking at the external appearances during the ‘view of the body’. At it, the coroner gave a verbal report that summarised for those assembled the physical evidence-gathering and general gossip garnered in the community. The jury under the coroner’s direction would then assess the circumstances surrounding the unexplained death and arrive at a verdict before releasing the body for burial. Disinterring bodies after Inquest was rare, even with new subsequent evidence. In the early Victorian era, formaldehyde replaced mummification and alcohol preservation of the body and tissues, respectively. Even so, it was hazardous to hold on to a corpse for long; contamination by contagious diseases, like cholera or diphtheria, was common. The smell of formaldehyde was also difficult to stomach and thus at the ‘view of the body’ chemicals tended to distort lingering synaesthesia impressions. The aim was thus to look quickly and get the body buried as soon as possible. By the 1880s, French morgues were introducing refrigeration techniques, and soon this was copied everywhere across Europe by the early twentieth century.8 Before then, it was vital for English coroners to conduct efficient enquiries in the thirty-six hours after death before the human material started to decompose. Putrefaction devalued human material from a forensic standpoint.
English coroners were under instructions to conduct themselves according to the legal principle of ‘the balance of probability’.9 In other words, provided the available evidence seemed to indicate that a death ‘probably’ looked ‘natural’, then the coroner had the discretion to pass a verdict without the need for an expensive Inquest. In the case of a drowning, this would be a suicide verdict, by way of example. Coroners were not required in law to prove that someone was guilty of causing that death. Nor did they need to abide by the legal stipulation that the accused was innocent until proven guilty in a court of law. Their role was to establish that neither manslaughter nor homicide was suspected, and, if it was, to refer on that serious matter to the local forces of law and order to investigate further and arrest the culprit. In which case, if it looked like a capital charge might go to the Quarter Sessions court, the coroner was duty-bound to ask a surgeon to perform a post-mortem on the dead body and report back to an Inquest jury.
From the 1830s, and following a concerted campaign in the Lancet, coroners slowly started to be medically qualified.10 They also tended to adopt standard post-mortem methods. Generally, this involved making a crucial incision from the neck to the naval, and across the chest cavity.11 An appointed surgeon would handle the heart and major organs, as well as closely examine the brain, for any suspected violent injuries. Coroners might also call additional medical witnesses who had the requisite expertise in, say, the forensics of poisoning to establish a death by misadventure.12 Likewise, an ‘unnatural’ cause of death could have been caused by a stabbing or a drunken brawl that got out of control. In which case, they could call on a medical man with a lot of experience in doing post-mortem examinations for high-profile cases tried at the Old Bailey in London. If subsequently at an Inquest a verdict of ‘murder’ was based on reliable medical evidence, the coroner would refer the matter to the appropriate legal authorities, and the dead person would be buried without further delay.13
The role of the coroner has always involved a very visual method of working. Looking at the surface of the body was important before medical science had X-ray technology, CT and MRI scans. There is therefore a long art history of the Coronial Office because such visual methods interested artists trained in life drawing who liked to sketch and paint dead bodies, and thus record coroners’ working-lives. For this reason, it is feasible to trace their broad development from the early nineteenth to early twentieth centuries through the medium of iconography. In Illustration 5.1, for instance, we see a typical satirical cartoon mocking the bumptious nature of the Coronial Office from the 1820s when arguments started to be made about the need to have medically, rather than just legally qualified coroners. The image thus lampoons an inept and legally qualified coroner who has little expertise in the metabolic mysteries of medical death. In this case, we can observe a blazing fire that may have warmed up a body, seemingly dead, but capable of resuscitation. To the disquiet of the surgeon on duty, it appears that the post-mortem he has been called in to perform in his clean pale apron might involve human vivisection. He wants to halt proceedings at the ‘view of the body’ because the so-called victim has in fact started to wake up. If the surgeon continues to cut the body in front of the assembled jury, he would be breaking the Hippocratic Oath ‘to do no harm’. Even so, the Coroner insists he carry on:
Surgeon [dressed in a yellow frock coat and apron] informs the Coroner: ‘The man’s alive. Sir, for he has opened one eye’.
Coroner [dressed in wig & dark coat and depicted as fat from his office fees] replies by deploying his discretionary justice: ‘Sir, the doctor declar’d him Dead two hours since & so he must remain Dead Sir’

Illustration 5.1 ©Wellcome Images, Reference Number V0010903, A Juror Protesting that the subject of the Coroner’s Inquest is alive; showing the dangers of blind faith in doctors when declaring medical death – Coloured aquatint by Thomas McLean, 26 The Haymarket, London, c. 1826, copyright cleared under creative commons Attribution Non-Commercial Share Alike 4.0 International, reproduced here under (CC BY-NC-SA, 4.0), authorised for open access, and non-profit making for academic purposes only.
By the late nineteenth century, the Coronial Inquest was held in private, away from prying eyes in a specially designed morgue. Seldom were the jury present by this time. Reporting the facts of forensic science at an Inquest court became accepted practice. Cutting the corpse involved hence a close working partnership behind closed doors between coroners, pathologists and anatomists working in tandem. We see this typical situation in Illustration 5.2. A coroner handed over a man to the St Bartholomew’s Hospital dissection room who died a ‘natural death’. The coroner had the discretion to rule that the death was obvious as the man died in the care of the Poor Law authorities and thus there was no need for an expensive Inquest. On 7 July 1894, when the corpse arrived, an artist skilled in pathology sketched the face and chest of the friendless man in order to study the nature of decomposition, represented here with the grey-scale area of shading, spreading down the right side of his torso, in reality a blue hue. The weather was hot at mid-summer and this accelerated putrefaction, despite the corpse being injected via the carotid artery with formaldehyde to replace bodily fluids over a forty-eight-hour period.
Further record linkage work from data previously collected by this author confirms that the corpse was that of William Smith, aged 64, who died in Islington Infirmary at Highgate Hill, North London.14 Supplied by a Poor Law dead house, he was dissected, then buried. Initially the coroner concluded from a visual examination of the body that William Smith the pauper had died from a common disease of poverty, namely ‘phthisis’ [tuberculosis]. This made his body ideal for study because it came into the dissection room without extensive post-mortem cuts. We can thus observe in Illustration 5.2 how the head supported by a brick has no lancet marks on the chest, where normally a crucial incision happened at autopsy. In other words, this is exactly the sort of supply mechanism that coroners were co-ordinating with medical schools on a regular basis and it placed the Coronial Office at the forefront of the expansion of medical education in the growing Victorian information state.15 In total, anatomists dissected William Smith for ‘250 days’ until 11 March 1895. His remaining body parts were interred into a shared pauper grave, next to six other bodies. This status quo was to remain largely intact for the poorest people in society at the behest of coroners even after WWII.

Illustration 5.2 ©Wellcome Images, Reference Number L0062513, Watercolour drawing done by Leonard Portal Mark on 7 July 1894, depicting the face and chest of a man (unnamed) to show the appearance caused by rapid post-mortem decomposition. It was made about twelve hours after death, during the hot weather of July 1894 at St Bartholomew’s Hospital dissection room, copyright cleared under creative commons Attribution Non-Commercial Share Alike 4.0 International, reproduced here under (CC BY-NC-SA, 4.0), authorised for open access, and non-profit making for academic purposes only.
In a third image, Illustration 5.3, we glimpse the modern situation during the late twentieth century. Instead of the coroner conducting a post-mortem in-tandem, the forensic examination has now been delegated entirely to a hospital pathologist. We can observe the cross-like pencil lines of the crucial incision down and across the torso. The equipment is sterile and resembles the design of an operating theatre, rather than an old late-Victorian morgue. There is a basin at the foot of the steel table to collect the major organs and any tissue samples retained for further pathological study or transplant surgery. Notice, too, the ridges on the steel table to scrub down the equipment after each post-mortem. The pathologist likewise wears surgical gloves and a disposable apron. To the rear are the large refrigeration units that keep the body fresh. Here there is little physical indication of putrefaction of the sort seen in Illustration 5.2. The coroner’s role is cleaned up, with the aid of biotechnology. The facial identities of both the pathologist and the body on the dissection table are indistinct: anonymity is an ethical choice here, but it also distances medical science from human stories and their hidden histories.

Illustration 5.3 ©Wellcome Images, Reference Number L0029414, ‘Royal Liverpool University Hospital: a pathologist cutting open a body in the mortuary’, original drawing on site by Julia Midgley, Liverpool, 1998, artwork dimensions 42 x 29.7cm, copyright cleared under creative commons Attribution Non-Commercial Share Alike 4.0 International, reproduced here under (CC BY-NC-SA, 4.0), authorised for open access, and non-profit making for academic purposes only.
Further record linkage work confirms that at the Royal Liverpool University Hospital in the 1990s this unnamed body in Illustration 5.3 was one of nineteen bequests (see Chapter 4, Table 4.3) that passed into the official ownership of the medical sciences. Its donation point was co-ordinated and delegated to a pathologist on duty via the Liverpool Coronial Office. This third image is hence the logical expression of a century of scientific co-operation – by coroners, the forensic sciences, pathologists and dissection rooms – in order to cement professional status. It represents what happened to Mr Herbert Jones in our opening story too. The coroner for south Hampshire examined his body; a hospital duty pathologist confirmed the cause of death; but there was no further dissection at Bristol medical school. The coroner had the discretionary justice to decide otherwise in an explicit dispute about the deadline and its dead-end of life: one of many cases we will be encountering in this chapter.
One of the main reasons the coroner did not send Mr Herbert Jones automatically for dissection was that at the time of his death old legislation outlawing suicide had recently been changed. To allow for suicide (no longer illegal) but prevent euthanasia (still illegal), the coroner was now legally obliged to make sure that nobody else was involved in the decision of the victim to take his life, even those patients facing an imminent fatal medical prognosis: a context from 1962 that still occupies policy-makers today. The Suicide Act (9 & 10 Eliz. 2 c. 60: 1961) had only recently legalised ‘self-murder’. There was thus extensive debate in the press and medical journals at the time whether ‘doctors should prolong dying or not’.16 Debates about what constituted medical euthanasia appeared often in the media. Against that liberalisation of suicide backdrop, it remained, however, still illegal to assist an individual dying from a fatal prognosis in making the decision to end their life, termed ‘complicity in suicide’. According to Section 2 of the Act, which still remains in force in Britain: ‘A person who aids, abets, counsels or procures the suicide of another, or attempt by another to commit suicide shall be liable on conviction on indictment to imprisonment for a term not exceeding fourteen years.’ Legally this can result in a charge of ‘conspiracy’ in ‘assisted dying’. The twelve letters that Mr Herbert Jones penned to his bank, legal representative, coroner, police and neighbours seem, therefore, to have been some sort of legal safeguard to make sure that this eventuality was ruled out at Inquest. The paper trail implied that he alone made the decision to commit suicide and donate his body to medical research. He was a careful and meticulous man, and thus his actions were in character. Even so, the coroner was sensitive to what amounted to his first case of this sort of suicide situation under the new legal guidelines. He acted conservatively, investigating the full circumstances of death and the ‘gift relationship’ attached to it. Using his discretionary powers, he ordered a post-mortem to clarify Coronial Office guidance, as to:
Whether the action which caused the death was done deliberately
Whether the intended consequence of the action was their death
If the individual did not intend to take the action, their death may have resulted from an ‘accident’ to be recorded by the coroner’s verdict
If the individual action was deliberate but the consequence was not intended to be fatal, then the coroner should record ‘a verdict of misadventure’
If the individual’s intention was unclear, the short-form conclusion by the coroner would be an ‘open’ verdict17
In other words, legally coroners could recommend verdicts according to the ‘balance of probability’; in practice, suicide and its assistance (or not) made it imperative for the coroner to dispute Herbert Jones’s explicit wishes.
Complicating this situation was the fact that the coroner was also working with another important context, and one of material significance to the eventual destination of the cadaver in this sad case. Herbert Jones self-evidently wanted to bequest his body to medical research. But whether it was suitable for donation or not could be disputed by those the coroner might decide to hand the corpse over to. If the cancer about to kill Herbert Jones riddled his dying body, then in death this made it of less material use for anatomical teaching. In which case, the body would be sent for cremation without delay once the coroner passed his verdict. If, however, the specific cancer was of research interest to medical science, then parts of the body and human tissue could still be used in part for further pathological study. Another alternative is that if the body did not have significant secondary tumours, but a key organ had deteriorated to such an extent that it threatened a patient’s life, then ‘parts of’ that dead body were still a very useful teaching and medical research resource. In other words, in hidden histories of the dead, the coroner had a very important role indeed to play in starting off the post-mortem after-life of human material that came into the Coronial Office jurisdiction: a factor seldom traced in the archives, and one which we will be elaborating on later when we encounter the detailed case of Carol Morris. In the meantime, the critical point to appreciate at this point in this chapter’s developing argument is that the type of Inquest ordered, given the diseased condition of the dead body, mattered a lot to its eventual destination for harvesting. Coroners typically faced two competing tensions in this situation – how much the pathologist should cut to complete death certification procedures and how a coroner could prioritise anatomists’ need for a clean corpse to dissect.
There is one final operational issue that many coroners had to work with. Most experienced moral pressure from grieving families to alter upsetting suicide rulings. Coroners thus typically recorded ‘accident’, ‘misadventure’ and ‘open’ verdicts on death certificates. In other words, disputed bodies were contested sites of multiple research agendas and reflected family sensitivities. That said, in Mr Jones’s case his wife and son had pre-deceased him. He died without family involvement. This case’s explicit body dispute was thus exclusively between the coroner and a dead person: the former over-ruled the latter because the dead, as we saw in Chapter 2, are Res Nullius – Nobody’s Thing. Herbert Jones’s post-mortem was thus akin to those of Keith Simpson, a leading pathologist who told the Listener magazine in 1977 that for all pathologists: ‘My patients never complain to me. If their illness is perplexing, I can put them in the refrigerator and come back later on.’18 Silent conversations in cold storage facilitated the medical sciences co-creating with the Coronial Office; yet these actor networks and their working arrangements remain opaque in the historical literature. Explicit body disputes involving those such as Herbert Jones sent for cremation rather than further study remain too often undisclosed in the paper trail of a bureaucracy that made these ‘mechanisms of body donation’ both function and malfunction. It is to this paper trail that we now turn. We begin by examining first some of the common systemic flaws in the system that processed and recycled the dead.
Auditing a System with Systemic Flaws
At the various public enquiries into the NHS organ retention scandals that led to HTA2004, a considerable weight of evidence was presented that the paper trail relating to dead bodies and co-ordinated by coroners, pathologists, anatomists or medical researchers was inadequate. At the time, the Chief Medical Officer Sir Liam Donaldson concluded that it was essential to carry out a full audit of all human material held in medical schools and Coronial facilities, as well as museums, to ascertain the extent of both historical and recent retentions. In a previous chapter we briefly discussed how the final report revealed that there were ‘105,000 organs, body parts and fetuses that had been retained in 210 English NHS trusts and medical schools’.19 Of these 210, ‘around 25 leading institutions accounted for nearly 90% of the body parts retained’. Michael Redfern QC, who conducted a separate public enquiry into organ retention involving the nuclear industry, likewise concluded there was: ‘a weak and poorly understood legal framework that had allowed bad practice to flourish’.20 It was difficult not to reach the conclusion that medical scientists of all descriptions had intentionally kept patients and their families in the dark. In response, the Royal College of Pathologists issued a statement defending their position and proposing to conduct an extensive internal investigation into working practices. Even so, a concerted press campaign reported on how some pathologists with the co-operation of coroners had conducted ‘their business by stealth’. This use of emotive language to describe medical research as a ‘business’ drew widespread criticism from inside the medical profession. Many were stung by the quoting of an old English proverb: ‘A thief is a thief, whether he steals a diamond, a purse, or a small part of you.’ There was soon a cultural stand-off. Yet it was established by a series of timely new historical studies that the term ‘business’ was an accurate depiction of dissection and its hidden histories, which were closely associated with the Coronial Office and its pathology partners.
The ‘business of anatomy’ flourished because AA1832 permitted it to do so until HTA2004 became law (see Chapters 1 and 2).21 However, because the medical sciences had very little historical sense of their own inner workings, the paper trail that was created to make this system of supply function was never retained by those in charge. As a result, when scandals about the retention of human material reached the press, there was a tendency to apportion blame to HTA1961 or HTA1984 without appreciating that AA1832 had stated transparently the need to keep records. The original legislation did have a tracking system for its mechanisms of body supply. Until at least the 1930s this monitored human material much better than any modern legislation, with up to twelve certificates issued each time a body or part moved from source to dissection table. The flaw in the system was that, once audited, usually every three months, destroying paperwork became the norm to avoid unwelcome publicity. Civil servants misunderstood therefore what happened inside the system by the 1950s. They assumed there had never been a system of accountability in the past because they could not find evidence of it when drafting new parliamentary bills. Their modus operandi was thus to tinker with statutes, instead of overhauling them. As a result, histories of anatomy often assume, incorrectly, that AA1832 had no paper trail and audit procedures. The opposite was the case. There was a complex system with detailed paperwork: a classic case of the medical sciences needing to look forward to the past.
The anatomy ‘business’ was also enterprising and inventive. Staff sought practical solutions to overcome any operational issues in the most pragmatic way; and, it was logical to do so. That status quo reflected the fact that, as Joanna Innes points out, parliamentary statutes for centuries were written with ‘a sufficient level of generality to cope with diverse local circumstances’.22 From the Georgian era onwards, successive governments drafted legislation in a cursory manner because what was proposed ‘often did not commend’ itself ‘to eighteenth-century Britons’. This meant that when it came to medical reforms, discretionary powers shaped procedures. There was a high degree of discretionary justice deliberately written into ‘orders’ and ‘guidelines’ accompanying any new legislation. Coroners soon used those powers to develop close working relationships with anatomists and pathologists. So much so, Coronial officials often made up procedures as they got on with the task in hand. Over time, this created a sense that medical paternalism mattered more than death’s customary rituals in Britain. A lack of public accountability had a ripple effect in other parts of the global community too, notably in Canada, Australia, New Zealand and other Commonwealth countries, where the British legislative framework continued to shape medico-legal standards until the 1990s.23 The odd thing about this backdrop is that AA1832 never intended this outcome.
When the NHS was created in 1948, new legislation gave the impression that teaching hospitals were now meticulous about the retention and disposal of human remains, but this was not always so. One example is illustrative of what could go wrong when procedures in morgues became disorganised. On Friday 14 December 2001, the Evening Standard reported on a case where procedures in a teaching hospital went awry. Paperwork was not properly attached to a dead fetus:
A baby has been found dead among hospital laundry in London. Scotland Yard were called just after 5am yesterday after reports of a ‘human foetus’ at the Laundry in Acre Lane, Brixton. Police are checking which hospitals provide the unit with laundry. One report said the body was that of a foetus of about seven month gestation. They are trying to establish whether the baby was born naturally or as a result of a miscarriage or abortion. A post-mortem will be carried out today.24
The Times some weeks later, on 13 January 2002, explained the events in more detail:
The body was that of a baby boy, J. K., who had died one hour after being born at Queen Mary’s Hospital, Sidcup. He had been born at 23 weeks gestation, some 17 weeks prematurely, his weight at birth having been 1lb 1oz. After death the child had been wrapped in a sheet and taken to the mortuary and placed in a refrigerated drawer. Next to the drawer was a bag for laundry from the mortuary and the wrapped body had accidentally been transferred to the laundry-bag. From there it had been taken to the Sunlight laundry, Brixton and had been put through a boil wash. The father, aged 36, and mother, aged 25, were both named, the latter being a Spanish national who had since returned to Spain to recover.25
In reviewing this case, and the circumstances that led to it, Robert Bruce-Chwatt MBBS, MFTM RCPS (Glasg.), Senior FME, Metropolitan Police, concluded that there had been ‘an error of omission’ in the paperwork process when the fetus was placed in the fridge next to the laundry basket. He did not find ‘an error of commission’ involving organ and tissue harvesting of the sort practiced at Liverpool Children’s Hospital at Alder Hey by Professor Dick van Velzen.26 The fetus had self-evidently come under the jurisdiction of HTA1984. When it was moved after being stillborn it should have thus been sent to the hospital morgue with the standard paperwork attached to it. But this had been ‘mislaid’ in ‘either theatre, the labour ward, or mortuary, with the soiled laundry’. It is thus a historical prism of the sorts of material anomalies that happened inside the system as soon as the dead were moved from one jurisdiction (hospital ward) to another (morgue, Coronial facility, pathologists’ lab). Along the way, parts of the person might be consigned as ‘clinical waste’ due to carelessness. For in the case under discussion, nobody could explain how exactly the stillbirth was taken out of the refrigerated drawer in the morgue and dropped into the laundry basket by mistake. Something had gone wrong, but who was involved remained undisclosed.
The fetus was found to be ‘5–6 months old’ when examined for forensic purposes, and it now had to be disposed of according to current regulations. But these were not necessarily what the general public would have expected either. There were three legal options. If the stillborn fetus was still intact (it was in fact in a poor state having been through a boil wash in the washing machine), then it came under the Burial Laws Amendment Act (43 & 44 Vict. c. 42: 1880). Where it was instead to be cremated (after its post-mortem), then this would be carried out in accordance with the Cremations Act (15 & 16 Geo. 6 & 1 Eliz. 2 c. 31: 1952).27 Even so, if the pathologists found the fetus to be incomplete in terms of its identity, and thus its body was, strictly speaking, in parts (again, having been through a double-spin cycle), it was then in law defined as ‘clinical waste’. In which case, it could only be disposed of according to the Control of Pollution Act (Eliz. 2 c. 40: 1974), or the Environment Protection Act (Eliz. 2 c. 43: 1990). In other words, there should have been a careful paperwork trail, but it was omitted. All those involved expected the Coronial Office to use its extensive discretionary powers to put things right after a dereliction of duty.
These overlapping agencies and statutes are illustrative of the sorts of misunderstandings that could occur about the bureaucracy attached to the movement of the dead and their disposal in England. It exemplifies how the paperwork attached to the deceased was often delegated by default to the coroner, especially when things went wrong in NHS hospitals. Indeed, as Chapters 1 and 2 pointed out, the central flaw in HTA1961 was that everyone assumed that each hospital owned human material that died on its premises. They thus had the authority to dispose of their mistakes with the help of any coroners and pathologists on duty. Even after HTA1984 tried to correct this, the situation was further complicated by clause 42 of the Coroners Rules (SI 1984 No. 552), which ‘expressly provided that no verdict’ should be framed in such a way as ‘to appear to determine any question of criminal liability on the part of the named person or civil liability’.28 In other words, even when things went wrong and hospital negligence was self-evident, Coronial rules meant that at a public Inquest there was no legal leeway to name either a negligent medical professional or an NHS facility as substandard. The facility staff might look morally culpable of contributing to a death, but it was not up to the Coronial Office to determine whether this constituted a criminal offence. The Times newspaper thus explained that if, for example, a man having a very bad asthma attack died as a result of a severe delay in the arrival of an ambulance, even when there was evidence of medical negligence and an ‘unnatural’ death, the coroner could not apportion blame.29 The pathologist doing the post-mortem was correct to state that the deceased had died from ‘status asthmaticus’ [a prolonged asthma attack], but whether the circumstances surrounding the death decreased the patient’s survival chances or not, and to what extent these constituted ‘a lack of care’, was open to legal interpretation. Technically in dispute was not ‘the cause of death’ in such a case, even if the circumstances surrounding the outcome were in doubt. This common situation recurred often during the 1990s in landmark cases like that of Regina v. the Coroner for North Humberside and Scunthorpe involving a prisoner put on a suicide-watch because he threatened to take his life.30 Due to a staff shortage, the man went unobserved for periods in his prison cell, and so died of asphyxia. Whether this was, strictly speaking, ‘self-neglect’ or due to ‘a lack of care’ was ‘blurred’. The question of how long the body should be retained and which parts of it should be taken for a criminal case (or not) remained contentious.
Coroners thus continued to act conservatively and often asked their designated pathologist to remove what ‘might possibly’ be required to determine ‘the balance of probability’: a judgement call based on their individual career experiences, as we saw in this chapter’s opening story of Mr Herbert Jones. To understand how this complicated medico-legal situation worked in practice, however, it is necessary to examine a broader selection of representative cases than the ones we have encountered so far in this chapter. In each, we can observe a coroner in conflict with those that claimed agency over the dead. The Coronial Office would nonetheless prove to have extensive powers of discretionary justice in the transplant era of the 1970s. The explicit disputes that occurred often exemplified the frustration that bereaved families felt to determine the material fate and resting place of their loved ones. Since this backdrop shaped a political consensus to pass HTA2004 and those new standards were adopted in many parts of the world, a detailed analysis of the role that coroners played in the circumstances that led to a system of informed consent to correct explicit disputes are of some relevance to this book’s central focus.
Coroner’s Explicit Disputes and Organ Donation Cards – The Alcock Case
In 1983, the Department of Health and Social Security (hereafter DHSS) had taken a strategic decision to re-launch a national organ donation campaign: outlined briefly in Chapter 2 and now elaborated with human stories here. The Conservative government of Margaret Thatcher was concerned that just 15 per cent of the population were carrying organ donation cards in Britain. As a result, the British Medical Association reported that transplant waiting lists were getting longer. The DHSS commissioned a number of social surveys to measure public opinion. These indicated that NHS patients were broadly in favour of donation, but this cultural trend did not translate into positive action. The DHSS therefore allocated a budget to raise the media profile of carrying organ donation cards, taking out expensive one-page advertisements in the national press. On the eve of the campaign, the actions of a coroner from North Staffordshire brought instead unwelcome publicity about explicit body disputes. The case was to highlight the extensive powers of coroners to requisition and hold on to human material without government or familial interference.
Thus, in December 1983, The Times reported on ‘a dispute over a Staffordshire coroner’s decision to stop the heart of a maintenance fitter being used in a heart transplant operation’. He had been ‘killed accidentally’ at work.31 The facts of the story were that:
Mr Graham Alcock, aged 28, a fitter at an excavator factory in Rocester [sic], had carried a donor card with him. Before he died last Tuesday, he told his relatives that he wanted his heart and kidneys to be used for transplants.
As a result of the request doctors at the Royal Infirmary in North Staffordshire kept him alive until suitable recipients could be found for the heart and kidneys. Tests were carried out on his organs to match those of patients waiting for a transplant.32
Several hours later a ‘suitable patient was found at Harefield Hospital in Uxbridge, West London’ and an air ambulance was ordered. A helicopter flight was the quickest way to get the donated heart from Staffordshire to London. At the last minute, however, the deputy coroner for Stoke-on-Trent, Mr John Wain, informed the head of the transplant team that he had ‘unexpectedly called a halt to the removal of Mr Alcock’s heart’. The Coronial Office issued an official statement that ‘the pre-existing condition of the deceased’s heart might be relevant to the Jury Inquest in due course’ and this necessitated halting the transplantation. If the man had an underlying heart complaint, then his employers might be guilty of a breach in health and safety standards at work where he had died from an accident. There could therefore be legal implications from the case and his human material needed to determine liability or not.
The widow of Graham Alcock was upset by this turn of events. She disputed the moral right of the coroner to prevent what her husband had explicitly requested in writing on his organ donation card. Interviewed by David Cross of The Times newspaper, she complained ‘that the dying wish of her husband had not been honoured’.33 As she stressed: ‘It seems he died in vain.’ The rest of her family were also critical of the decision. They thought it was counter-productive for the medical sciences. Mrs Dorothy Alcock (mother of the deceased) told the press: ‘Many people with organ donor cards could be dismayed that their wishes were not carried out. This has lost them hundreds of donor cards.’ Likewise, Mr Ray Alcock, father of the dead man, disputed the coroner’s actions, and in calling for a public enquiry declared: ‘It seems pointless to carry a donor card if the parents cannot carry out the wishes of their dead son.’ The transplant team supported their moral position. However, as a hospital spokesman explained, they had no choice. They had to ‘pay attention to what a coroner decided – We cannot argue about it.’34 The Coronial Office was all-powerful at the dead-end of life: a procedural fact that would be debated extensively in the 1980s, as we shall see later in this chapter when we examine similar representative cases.
The coroner in this case, Mr John Wain, did in fact have a very good reputation for representing people in his local community over his thirty-year career. On his death aged 77 in 2014, after ‘a long battle with cancer’, the Stoke Sentinel described him as ‘a much loved character’ whose ‘life touched many in Staffordshire’.35 He was regarded as fair-minded, and an advocate for the underdog, according to his colleagues. It was reported that he: ‘sprang from humble roots in the city’s neck-end [sic] and took his first fumbling steps into the legal profession as an articled clerk without even a law degree (back then)’. He obtained two A-levels, worked as journalist for a short time and eventually rose in the legal profession to run one of the busiest Coronial Offices in the country. In Stoke-on-Trent he was renowned for his human empathy, as a local obituary writer elaborated:
Because he came from the same humble origins, he had a deep affinity with ordinary families as he helped them to seek answers to how their loved ones died. As their champion he would fearlessly take on at times protected interests of the establishment to get to the truth. That could be anything from top surgeons messing up operations, and social workers ignoring alarm signs from the vulnerable, to deaths in police custody. At times he stretched coroner’s legal flexibility to its limit to announce verdicts which brought maximum benefit to those left behind.36
John Wain was also a keen advocate of opening up Coronial records if they could help further medical research into, for instance, the underlying causes of suicide in his district. In January 1999 he thus co-operated with a large-scale study covering North Staffordshire in which Wain had been the presiding coroner. Data was collected on ‘all cases of suicide’ and ‘undetermined injury’ between ‘1991 and 1995’ in which ‘212 cases and controls’ were identified.37 The study team concluded that ‘the risk of death due to suicide and undetermined death was associated with: recent separation, relationship difficulties, experience of financial difficulties, history of past criminal charges or contact with the police, a past history of deliberate self-harm, being on psychotropic medication at the time of death and a diagnosis of bipolar affective disorder’. In a similar refrain, Wain had assisted with an NHS study into whether ‘pre-hospital deaths from accidental injury were preventable’.38 Again he released Coronial records covering the period ‘1 January 1987 to 31 December 1990’ in which there were ‘152 pre-hospital deaths from accidental injury (110 males and 42 females)’. The important conclusion of this study was that: ‘Death was potentially preventable in at least 39% of those who died from accidental injury before they reached hospital. Training in first aid should be available more widely, and particularly to motorists as many pre-hospital deaths that could be prevented are due to road accidents.’ Wain was thus not the sort of coroner who would routinely hold up a heart transplant unless he believed it was necessary.
Nevertheless, the Alcock family thought he was guilty of having ‘stretched coroner’s legal flexibility’ (to use his obituary writer’s precise phrasing). Even so, whether the bereaved family had legal grounds to challenge what happened or not, what really mattered in the end to them was that Wain had the discretionary justice to act as he did and he brought about a dispute at a key discrete research threshold point in a donation process. Generating explicit disputes in a transplant era was, seemingly, often part and parcel of a coroner’s normal working-life. Since cases like this raise the issue of representativeness, it is important to explore general trends regarding the retention of human remains involving the Coronial Office covering elsewhere in England. As we shall see, other coroners also took a similar view of their extensive powers to be advocates for the bereaved but also to query organ donations and hold them up if necessary. An important case of Carol Morris outlined next is illustrative of general trends in the Midlands. It is, moreover, a significant story because it was to make medico-legal history by changing the law on the anonymity of organ donation in Britain and around the world (as we shall see in Part II of this chapter, where we discuss the case’s ingrained lessons and their historical longevity involving coroners).
The Carol Morris Case
On 6 August 1977, the BMJ carried a detailed report on the modus operandi of the coroner for Leicester City and South Leicestershire.39 Since what he wrote was to have far-reaching consequences just three years later in another explicit body dispute, it is important to pause and consider the coroner’s detailed letter to the BMJ to set the scene in what became known as the Carol Morris Case. Mr Michael Charman explained in 1977 that he was legally qualified. On average, he oversaw about ‘1400 unexplained deaths’ every year in a busy area of the Midlands. He paid careful attention to the bereaved and tried where possible to relieve their stressful situation, as he explained:
Of necessity the reports issued to me by my pathologists are all couched in medical terms and when I first became a coroner I had to unravel this terminology to discover the cause of death. I also determined that to be efficient I would need to obtain explanations from my pathologists. I therefore not only view the body but also, in cases in which there is some difficulty or peculiarity, will view the body while the necropsy is taking place and my pathologists are kind enough to demonstrate to me the actual cause of death. In cases of death from a cause other than a natural one, I find this very helpful indeed when taking the inquest. Since usually the only medically qualified person at an inquest is my pathologist he is also careful to give an explanation in non-medical terms of the cause of death so that those present, including the jury, understand precisely what has happened.40
Charman told the BMJ that he worked with one of four pathologists, and he carried on the tradition at Leicester of allowing the duty-pathologist to pass on a copy of his report to the bereaved family’s general practitioner once an Inquest had been finished. He was not legally obliged to do this, but he felt that it did alleviate grief. Often the GP was in a better position to reassure a family that the deceased had not suffered or been in a painful condition. In terms of the grey areas of these legalities, he elaborated that:
It must be remembered that in England the post-mortem report on any sudden death is prepared by a pathologist appointed by the coroner and that the report is the coroner’s and belongs to no one else; furthermore it is not a public document until after the inquest or the issue of the coroner’s certificate that the death was by natural causes. It therefore follows that it would be very difficult indeed for the pathologist conducting the examination to give any explanation to a relative except in the vaguest of terms until the legal formalities have been completed. Once this has happened I personally, as coroner, would be very happy indeed to permit any of my pathologists to alleviate distress by giving simple explanations, but at the same time I know they are very busy people. …41
It would be precisely this medico-legal situation – a coroner having extensive powers to withhold information if he judged it to be in the public interest – and with the co-operation of his pathologist often pushed for time – which was to cause an explicit dispute that made national headlines. Events at Leicester by 1980 would prove contentious and ultimately change the terms of reference of working coroners everywhere in England. We begin with a tragic accident in the Carol Morris case files.
On 25 January 1980, Carol Morris, a young woman aged 16, was driving a moped in the early rush hour at Houghton-on-the-Hill village about 6 miles from Leicester city-centre.42 It was a cold and icy winter’s day. Near a crossroads in the centre of the village close to a garage, Carol Morris tried to join the oncoming traffic down the lane from her home. The location was notorious for car accidents where the B3129 crossed the A47. Tragically, in the inclement conditions a 40-foot lorry collided with the moped as it exited from a side road into the main arterial route into the city. Carol lay on the ground seriously injured. She was soon taken unconscious by ambulance to Leicester Royal Infirmary, where three days after the accident she died from her injuries. Carol Morris was carrying a donor card. Dr David Riley, a surgical registrar on duty, thus began the formal medico-legal process of checking on whether the accident victim was a suitable transplant donor. He needed to liaise with a transplant team at Papworth Hospital in Cambridgeshire to carry out a tissue match with patients on the organ donation waiting list covering East Anglia and the Midlands NHS regions. Because Carol Morris was aged 16, there were two lifestyle factors to assess. An evaluation of her general health condition prior to the accident was undertaken. The doctor found in her case-notes that it had been generally very good before the fatality. She was a fit and healthy young woman. There was every chance therefore that her kidneys (specifically ticked by Carol Morris on her organ donation card) would be healthy and ideal for transplant. The medical team also needed to assess the wishes of her bereaved parents and their familial relationship with Carol. She was aged 16 and so over the legal age of adult consent, but she was not yet 18 years old; therefore, her parents had guardianship of their daughter as next of kin. They wanted to respect Carol’s wishes to donate, and so the transplant team prepared the body without further delay. What happened next nevertheless was to cause considerable controversy – so much so that it generated a national debate in Parliament about the need for a change in the law to enshrine the principle of anonymity into organ donation programmes across Britain. The catalyst was the actions of the coroner for Leicester City, Mr Michael Charman, and the involvement of some journalists working for a number of popular daily newspapers who acted unscrupulously to get a news scoop.
Carol Morris remained on a ventilator until ‘her heart, kidneys and eyes were all removed for transplant’.43 The heart was despatched by plane and car to Papworth Hospital in Cambridgeshire on the night of 28 January. The transplant team were waiting on it. The pathologist on duty did a careful tissue crossmatch. Then the leading surgical consultant, Mr David English, and his colleagues completed a successful operation on ‘Mr Nigel Olney a 35 year old man’ from Bedfordshire, a patient desperately in need of a new heart. He was in due course to be the fourth heart transplant patient at Papworth after the relaunch of its surgical programme in 1979. Olney lived for almost nine years before he needed a second (unsuccessful) heart transplant in December 1988.44 He was thus one of the longest survivors at that time.45 Meanwhile, the Papworth team had recalibrated their working practices with some success from 1973, as recent histories of the hospital explain:
During 1973, 162 open heart operations were undertaken with a mortality rate of 5%. However, surgical activity increased rapidly and, after visiting Stanford [University], Terence [English] decided Britain needed a heart transplant programme. A major problem was lack of support from the cardiologists. However, after research at Huntingdon Research Centre where techniques for preserving the donor heart prior to its implantation in the recipient were developed, the first heart transplant was performed in January 1979. This was not successful, but four of the next five cases lived between three and eight years. Funding was also a problem in the early years, but help from the National Heart Research Fund and the Robinson Charitable Trust helped until Papworth Hospital was designated a national centre for transplantation.46
In addition, in 1980, around the time of Carol Morris’s death, a British Heart Foundation Research Group established itself at Papworth. This initiative funded the additional staff needed to expand innovative heart transplant work. Indeed, from 1981, they were able to undertake heart-lung transplants on site for the first time. In no small measure then the heart of Carol Morris was to contribute to Papworth’s becoming the preeminent heart and lung transplant unit in the UK. Even so, although the staff that led the unit feature as ‘Papworth’s heroes’ today on the hospital’s public engagement website, and the fund-raising efforts of Mr Nigel Olney after his first heart transplant are detailed (with Christopher Hubbard), no mention is made of Carol Morris. She never became an official Papworth heroine. Evidently, once removed, a body part became a discrete research step – ‘Nobody’s Thing’. That remapped the whole person into a series of hidden histories of the body, the equivalent of a consignment in the cul-de-sac of history, omitted from the success story of biomedicine.
Once Carol Morris’s heart was transplanted, the rest of her body was still technically under the official jurisdiction of the Leicester City coroner. He was required to commission a post-mortem from his duty-pathologist since the road accident might later result in the police charging the lorry driver with death by dangerous driving. There would need to be material evidence of sudden death, made available at any subsequent prosecution. An Inquest was thus scheduled. Before it convened, however, the coroner noticed that there was a discrepancy in his pathologist’s paperwork. Dr David Riley, the surgical registrar on duty at Leicester Royal Infirmary the night that Carol Morris died, asked the coroner to authorise the removal of her kidneys. Carol stated this option explicitly on her organ donation card and so her parents decided to comply with their dead daughter’s wishes, as we have seen. However, the deceased did not tick any other organs for donation. There were separate cards for each organ at the time. The bereaved parents searched their dead daughter’s belongings in her bedroom but found nothing. Carol’s intention seems to have been to donate her kidneys, probably because (her parents thought) there had been a number of media campaigns to improve their donation in the national press over the previous three years or so under the auspices of the DHSS (as described above). The coroner, Mr Michael Charman, was very mindful of being sensitive to the parents’ shocking bereavement. Indeed, he had a long history of sharing pathologists’ reports with grieving families shocked by the sudden death of their relatives in tragic circumstances, as he had previously explained to the BMJ. He felt he was now in a very difficult medico-legal and ethical situation. He had been officially asked for the kidneys of Carol Morris but not her heart and eyes which, it seemed to him, had been harvested as ‘extras’ for organ transplant and grafting purposes, respectively. The parents told the hospital staff in Leicester that they were ‘keen’ for ‘all the organs to be donated’; they interpreted the fact of their dead daughter’s having a donor card as confirmation that she was a supporter of transplant surgery per se. The coroner nevertheless believed that in case of the need for a subsequent prosecution involving the lorry driver and the question of his legal culpability on the morning of the fatal collision, the dead body had to remain solely in a Coronial officer’s medico-legal jurisdiction. He felt the transplant team at Papworth Hospital was deliberately ignoring this legal consideration, with the support of their surgical liaison at Leicester Royal Infirmary. Together they had harvested more than he had authorised. There would soon prove to be a very difficult professional stand-off between all the interested parties at the Inquest.
The Inquest opened on the Thursday after the death of Carol Morris. Charman was mindful of the stressful situation for the bereaved family, but there were a number of pathology discrepancies that in his opinion required action. He stated that he felt very uneasy about what had happened and how much was harvested from the body of Carol Morris, having ordered that: ‘no organs could be removed in his area without his written consent, countersigned by the surgeon carrying out the removal’. This claim by Charman that the ‘body of anyone who had died suddenly was his to decide upon’ was, however, ‘contested at the Inquest’. Carol Morris’s father stated categorically that as far as his family was concerned his daughter wanted to be an organ donor, stated so explicitly on a donor card, and they needed to comply with her wishes under the tragic circumstances. To do otherwise would mean she had died in vain (echoing the sentiments of the Alcock case outlined earlier in this chapter). Even so, Michael Charman replied:
His contention is that coroners should have the ultimate power of decision over how the bodies of potential organ donors are to be handled. The law, which is based on the Human Tissue Act of 1961, is at best open to interpretations, and at worst confused, say medico-legal experts.47
As the atmosphere at the Inquest was adversarial, Charman took the unusual step of calling a press conference afterwards. This upset the bereaved family, and with good reason, for since the death of Carol Morris they had been the focus of considerable unwelcome media attention. Before examining in more detail what the coroner said to the media, we first need to factor in what had been happening to the Morris family since the night of the fatality.
The Morris family had been under a media siege at Houghton-on-the-Hill since the death of their daughter on the night of 28 January 1980. So intense was the media intrusion that George Morris made an official complaint to the Press Council (hereafter PC) in London.48 He told them that: ‘on the 1 o’clock news on 29 January it was reported that a heart transplant operation had taken place at Papworth hospital and that the family of the donor particularly wished to remain anonymous’.49 He elaborated that ‘a [news] leak occurred and within three or four hours’ from someone working at Leicester Infirmary, Papworth Hospital or a PC news agency. The Evening News was the first media outlet to telephone the family for further information about the heart transplant that had taken place. Then the phone started to ring and ring. George Morris described how the phone ‘rang continuously’ from 1 p.m. to 5 p.m. when the family finally decided to ‘take it off the hook’. Events were, however, to get worse, as he explained:
However, that did not alleviate the position. The newspapers that had been told by telephone that the family were not prepared to comment sent reporters to the door. To add insult to injury, most reporters attempted to obtain additional information and a photograph of the dead girl from the villagers, despite the family’s request for anonymity.50
The family felt that ‘particular newspapers, such as the Daily Mail … behaved especially badly’. They even contacted their ‘next-door neighbour, Mr. Stephen Turnbull, giving the impression that they were friends of the family requesting information’. George Morris explained that the way that the reporters worked was to inquire ‘about the donor card’ and only later admit that they were journalists seeking a news scoop. In the family’s opinion at such a sensitive time, they all felt understandably: ‘That is a despicable way of obtaining information.’ Yet, worse was to come.
George Morris alleged that one determined reporter for the Daily Mail (Sally Brompton) waited outside the Morris family home ‘from 10 am on 30 January until 6 pm’.51 She then ‘canvassed the village from door to door in an attempt to buy a photograph of Mr. Morris’ daughter Carol’. George Morris subsequently relayed to his member of Parliament how ‘Miss Brompton even attempted to persuade a 14-year-old girl to go into her elder sister’s bedroom to remove a photograph of Carol’. She finally toned down her actions when ‘at about 6 pm Miss Brompton left a card with Mr Morris requesting an interview at a later date’. The family had taken enough. They requested and were granted police protection by the Leicestershire constabulary. A police officer, posted outside the family home at Weir Lane in Houghton-on-the-Hill, also arranged for British Telecom to make the home telephone number ex-directory until further notice. Mr Morris did acknowledge to the PC that although the Guardian newspaper and the Leicester Mercury had obtained photographs of his dead daughter, they decided not to print them once it came to light that they had been obtained by unscrupulous means. Their editors had acted, in his opinion, with common decency, unlike all the other newspaper tabloids which had ‘not acted in a professional manner’ at such a tragic time. The family now found themselves in the middle of a media storm not of their making and one which the coroner for Leicester city centre was about to exacerbate by calling a press conference after the Inquest about an explicit body dispute.
Michael Charman explained to the media that he felt obliged to call a press conference about the circumstances surrounding the death and harvesting of the organs (heart, kidneys and eyes) from Carol Morris because he believed procedures were unethical and technically illegal. He clashed with Mr Bernard Hargrove, head of a legal team who appeared for the three transplant surgeons involved: one at Leicester and two at Papworth Hospital. The Medical Defence Union funded Hargrove. He insisted that since 1977 the Home Secretary had taken the view that ‘no coroner could refuse for the removal of an organ unless it was needed for criminal proceedings or had been faulty’.52 In the case of a fatal road accident arising from careless driving causing brain-stem death, the retention of the brain in question would suffice as material evidence of medical death at a criminal prosecution. Hargrove also insisted that in the opinion of most doctors it was their medico-scientific duty to facilitate ‘all organ donation’. Yet, as a newspaper reporter for the Guardian who was present at the Inquest press conference explained, it really came down to one key question in this controversial case: ‘Who has the ultimate right to decide’ on organ donation in a Coronial case – ‘the coroner or the family?’ Moreover, this raised an important procedural point too – ‘Could a coroner refuse permission for the removal of organs, even if the deceased carried a donor card?’ Charman defended that he was very concerned that the surgeons who removed the heart had effectively ‘disregarded the law of the land which says that my consent must be obtained’. He clarified that he was not accusing the transplant team of deliberately flouting the law – ‘What they did was make assumptions which didn’t exist and thought that they had got consent when it wasn’t there at all.’ Soon, the storm created encouraged other medical bodies to get involved in the widening debate about this and other explicit body disputes involving the Coronial Office in England.
The British Medical Association (hereafter BMA) was quick to respond, issuing a press statement that they were worried that the adverse publicity could dissuade other organ donors from coming forward in the future. If all coroners requested a written rather than a verbal consent (the latter was standard practice in some transplant units), then that might also delay the removal of a heart and render it unsuitable to transplant in time. But Charman pointed out that this was nonsense, since written permission from the coroner delayed matters for no more than ‘an hour at the most’.53 Besides, he pointed out, in practical terms most donor patients were kept ‘on a heart-lung machine and time is not so vital, except at the moment of removal’. The Coroners’ Society for England and Wales (hereafter CSE&W) nevertheless joined in with the BMA’s concerns since both professional bodies were pro-transplantation. Dr Burton, a spokesman for the CSE&W, told the press that he had been a member of the Transplant Panel which had been convened to monitor the progress of transplantation, and in his experience: ‘For years we have been slowly moving towards the general public’s general acceptance of transplants as a routine matter of course. Every time this sort of thing happens’, where there is a stand-off between a coroner and the bereaved involving an explicit body dispute, ‘it sets the progress back years’. The assembled reporters thus asked Charman how he felt about contravening the family’s wishes. Did he consider whether he was going against the wishes of the bereaved and making things much more difficult for them? In reply, Charman defended: ‘No, I don’t. They must of course consent before my consent is asked for. I don’t think that in any way asking them for written permission affects it’ (that is, the decision to donate or not by the bereaved). He told the packed Inquest that the police had found that ‘there was not sufficient evidence to prosecute anyone for contravening the Human Tissue Act 1961’. Moreover, after hearing all the evidence collected from the roadside scene, there was no evidence that the lorry driver was guilty of dangerous driving. It was a tragic case; in the end, the coroner recorded a verdict of ‘accidental death’.
At the close of the public controversy, the BMA issued a further statement. They did so to clarify that each Coronial official should have sole jurisdiction of bodies in unexplained circumstances. And yet, they went on to state that HTA1961 gave ‘the next of kin ownership of their loved one’ when they were a whole person, whereas ‘the removal of parts of it must be up to a coroner’.54 This meant that as far as all the medico-legal officials involved were concerned Carol Morris had been a person with a family history that gave her a sense of community and belonging – until, that is, in death, she had become a cause célèbre because she wanted to ‘gift’ part of her body as a bequest. Consequently, her lack of agency in death and dwindling material integrity because of becoming a transplant target meant that she became recycled for public consumption: an outcome that her family found painful to come to terms with. They now had a very difficult decision to make about whether they should retreat into private grief or seek public redress from the press for being hounded. Given how much their privacy was breached, few onlookers would have blamed them for closing ranks and never speaking again about the dreadful circumstances of Carol Morris’s donation. Yet, with emotional fortitude, they decided to contact their local member of Parliament and asked him on their behalf to highlight the dreadful experience they had been through as an organ donation family. For, they did not want others to be in the same position of exposure to such intense public censure. And thus, we see how an explicit dispute came to national attention.
Donor Anonymity – A National Issue
On 5 March 1980, the Right Hon. Mr John Farr, MP for Market Harborough in Leicestershire, tabled an early day motion in the House of Commons. He did so on behalf of his constituents the Morris family:
I beg to move, that leave be given to bring in a Bill to provide for protection of the identity of donors of human organs. My reason for rising to present this Bill to the House is to respond to a request from one of my constituents whose daughter was recently tragically killed. After her death my constituent and his family underwent what can only be described as persecution by the media in a most improper way during their time of sorrow.55
Farr explained that he had ‘cross-party support’ for an amendment to the new Health Services Bill about to come before Parliament. The proposal was to attach to it a revised Code of Practice introduced in 1979, with the support of the BMA, to better regulate the transplant surgery of hearts by making all donations anonymous. There were thus two ways forward, as Farr explained: ‘First, again in order to assist anonymity, could not all the cards of those who wish to remain anonymous have the word “anonymous” printed diagonally in large type across the top? Secondly, in these days when organs of all types are so pressingly needed, could not we have a single donor card for all organs, which would greatly simplify the system?’ Farr had consulted the Secretary of State for Health, who was supportive. There was general agreement that the new procedures would protect families like the Morris’s from such public exposure for an altruistic act at a time of tragedy.
During the early day motion debate, Farr explained to his fellow MPs that the pace of transplant surgery in terms of its new techniques was moving faster than the law in Britain.56 So, whilst a Code of Practice for the Organ Donation(s) of kidneys was well known and had been operating efficiently for some time, the surgical ability to do spare-part surgery with hearts had exposed explicit body disputes that would become more contentious. The heart seemed to rouse public sensibilities because of its important cultural symbolism in Western society. It meant that any lack of clarity in the Code of Practice left heart transplant surgeons exposed to media harassment. Families that donated faced a maelstrom of press intrusion too. Yet, the Code’s language was loose when transplant techniques were influx. The press were thus quick to quote any lack of clarity in the wording. It was now important, in Farr’s opinion, to alter the discourse to reflect the changing realities of biotechnology by 1980. This would then ensure that compliance was transparent. He gave an example of how ‘paragraph 37 of the Code’ states that: ‘The staff of hospitals and organ exchange organisations should always try to maintain the anonymity of the donor and of the recipient.’ He reiterated: ‘I do not believe that that goes far enough today. I should like to see a fresh code drawn up.’ If the Code was redrafted in ‘plainer language’ – replacing should with must – this would guarantee anonymity for all involved on both sides of the donation exchange. The time had come to no longer fudge the pressing ‘question of anonymity’. It ought not to be dealt with ‘in a cavalier manner’ of the sort that the Morris family had experienced. In a final gesture that acknowledged the stressful situation his constituents found themselves in, Farr closed his speech by clarifying the current law according to HTA1961: ‘That Act clearly lays down that coroners have the right to require consultation before organs are secured. However, I understand that most organs are obtained after telephone consultation with the coroner, which I believe is a proper and correct procedure, which does not take up very much time.’ This reiterated that although the Leicester coroner was correct in medico-legal terms, others were working their way around the law in practical ways to facilitate transplant surgery. Reforms to working practices would thus ensure the Coronial Office avoided generating explicit body and body parts disputes.
In due course, as Hansard confirms, ‘Mr. John Farr accordingly presented a Bill to provide for protection of the identity of donors of human organs: And the same was read the First time; and ordered to be read a Second time upon Friday 14 March and to be printed. [Bill 160].’57 He did so successfully because he had widespread support in the Commons, including amongst the ranks of an influential lobby of leading exponents of transplant surgery:
Mr. Greville Janner Labour MP for Leicester West (1974–1997), Mr. Tony Marlow Conservative MP for Northampton North (1979–1997), Mr. Jack Ashley Labour MP for Stoke-on-Trent (1966–1992), Mr. R. A. McCrindle Conservative MP for Brentwood and Ongar (1974–1992), Mr. Tam Dalyell Scottish Labour Party MP for West Lothian (1962–82) and then Linlithgow (1983–2005), and Mr. Michael Hamilton Conservative MP for Wellingborough (1959–64) and then Salisbury (1965–1993).58
Of these, Tam Dayell had been one of the most high-profile spokespersons in Britain. He wrote a regular column for the New Scientist in which he often featured the need for more transplants and the lobbying on this issue that he was undertaking in Parliament.59 Likewise, Jack Ashley was a lifelong exponent of disability health issues and he promoted the re-enablement of those who could benefit from new medical treatments. All the others had strong local political connections to the East Anglian and Midlands regional areas of the NHS where many of the explicit Coronial disputes were being generated during the 1970s and early 1980s.60 Together they thus constituted a powerful faction that could substantiate the unpalatable position of donor families from across the social and political spectrum. As John Farr emphasised, the issue of anonymity was an emotive one because it had real consequences:
Mr. Morris alleges that the behaviour of the media caused more pain and anguish to my wife and daughter. The newspaper reporters even had the nerve to challenge Mr. Morris when he wished to leave his house, as if he were a criminal on the run. Mr. Morris said if transplants are to continue donor organs are essential. Families will not consent to the use of deceased relatives’ organs if the media continue to act in such a disgraceful and unsympathetic way. If families are to be badgered in this disgraceful and unsympathetic way by the media even when requests for anonymity have been made, the source of organs for transplant will dry up. I agree with Mr. Morris, and though I am in the van of those who believe in the need for a free press, I believe that the conduct that I have described is evil. We must therefore make it as difficult as possible for such ghouls to gain any clue as to the identity of sorrowing families.61
‘Evil’ was a strong term to use – too strong for some newspapers editors – and so soon events would prove that anonymity was not necessarily as straightforward as was implied in Parliament; for, there was another side to the Carol Morris controversy that came to light too.
The Controversial Nigel Olney Case
The PC and its media outlets were somewhat stung by the criticism being levelled at them in the Carol Morris case. Indeed, it was clear that the disputed actions of some journalists could lead to a change in the law. This would give donors, and their recipients, anonymity in transplant surgery on a permanent legal basis. If the press were to make a case for more public accountability, then they needed to take a new tack. They soon found a news angle. Reporters were despatched to investigate the personal circumstances of Mr Nigel Olney who had received the ‘gift’ of Carol Morris’s heart. The Guardian newspaper was one of a number of the broad sheets and popular dailies that opened with a report that was positive in its tone. It informed readers that Nigel Olney had been sitting up in his hospital bed at Papworth, and he was recovering well from the heart transplant operation, which took ‘five hours and seven minutes and was led by the South African-born surgeon Mr Terence English’. Then lead articles turned into an exposé:
Mr Olney, a Leighton Buzzard, Bedfordshire, chiropodist, had separated from his wife and two young children and lives with his parents. His severe heart complaint was amongst the factors that had saved him from being sent to prison last year after he was found guilty of obtaining £5, 553 from two local health authorities by deception. At Bedford Crown Court he admitted claiming money for patients who had died or moved. Suspending an 18-month sentence for two years Judge David Lowe said: You are a man of no previous convictions and we take into account your medical condition [sic].62
The unwitting testimony implied in this editorial line was that this was a man with questionable morals by virtue of his pending divorce (allegations of adultery and child custody rights for men were still a sensitive social issue in the 1980s). He was also a convicted fraudster that had benefitted from being in an NHS facility paid for by the same taxpayers he had defrauded in his chiropody work in the community. The Guardian newspaper was nevertheless careful to balance its editorial slant. Interviews were obtained from Mr Olney’s soon-to-be ex-wife, his near-relations, and a Papworth Hospital spokesman about the costs of his operation and aftercare. All stressed that he was a suitable donor recipient. A neighbour of the Olney family in Leighton Buzzard, Mary Campbell, described Nigel: ‘He is a hell of a nice guy. Nobody deserves to live more than he does. He’s been so weak recently he’s had to be carried when he goes out.’ In mitigation, she alleged: ‘I think his illness and his marriage problems would account for some of his other troubles.’ Likewise, Nigel Olney’s separated spouse who had moved to a Hertfordshire village with ‘her two children Jason and Nicole’ told a reporter on her doorstep: ‘I am extremely concerned and hope Nigel makes a steady recovery.’ It was a dignified response from his separated wife in the face of full public exposure. Nigel Olney’s parents similarly ignored the accusations of his unworthiness and stressed instead in a statement to the press: ‘We are most grateful to the hospital for accepting our son and taking such good care of him.’ A Papworth Hospital spokesperson meanwhile explained that recently the transplant team received a charitable grant of £50,000 from the National Heart Research Fund and this money, not NHS resources, was funding the transplant and aftercare required. When pressed, the transplant team estimated that ‘the operation and a year’s aftercare would cost about £15,000’ in each case. In other words, the Carol Morris explicit dispute with a coroner was now being recycled into a much wider set of other body part disputes about the future medical ethics of transplant surgery in a modern world.
It was well known at that time that the NHS had refused to fund such risky surgical procedures as heart transplant. On the one hand, then, the newspaper coverage was being duplicitous in connecting Mr Olney’s fraudulent behaviour to his alleged exploitation of public healthcare funds. On the other hand, the NHS had built Papworth Hospital in the first place from central taxation and so Nigel Olney was technically receiving a benefit in kind by being cared for in that facility. Evidently, the assessment of the case on financial, medical and moral grounds rested entirely with the transplant team and the charity in question. Indeed, the medical team stressed that they examined the best surgical chance for a tissue match and, provided the pathologist on the transplant team found that the immunology looked favourable, it was judged prudent to go ahead. There would have been a sound medical case for the transplant to proceed. It was not, moreover, for transplant surgeons to investigate the moral grounds for proceeding in individual cases. However, this question of the morality of transplant work did not abate, either at the time of the Olney case or subsequently once liver transplants became feasible. Often the media would ask: Should an alcoholic (for instance) receive a liver transplant? It was an ethical question that featured in many high-profile cases such as the ex-footballer George Best, famous for his hedonistic lifestyle and family history of alcoholism.63 Yet, Nigel Olney’s brother in response to the considerable media storm, and the very personal criticisms being levied, reiterated to the Guardian: ‘the family are very distressed that Nigel’s past has been “raked up” when he was still in intensive care’.64 In many respects then Nigel Olney was a test case for what would prove to be ongoing ‘moral’ debates surrounding transplants and the anonymity for recipients in Britain and Europe. What Carol Morris’s bereaved family felt when they discovered the personal circumstances and criminal record of Mr Nigel Olney was not recorded publicly at the time in the newspapers; yet, it cannot have been palatable to be part of an ongoing press exposé, even by association, during the first stages of grief.
The balance of the evidence in this symbolic case makes it clear that heart transplant surgery was an emotive issue in the British media – journalists tapped into a long history of the heart being a central and enduring symbol of humanity in histories of the body for many cultures.65 Yet, it was also a litmus test for many of the procedures put in place when the Victorian Information State established working arrangements, aspects often neglected in standard historical studies.66 Coroners had extensive powers of discretionary justice, and they had worked hard to promote their image as protectors of law and order in the community. As they moved from being legally to medically qualified, and worked alongside pathologists more regularly, it enhanced their professional status. Their individual sense of personal agency increased too. So much so, that by the modern era they had become the fulcrum of advances in forensic medicine and pathology. In an era when medico-legal jurisdiction over the body was to become contentious as researchers inside the medical sciences competed for better access to cadavers and ‘live’ donors (in kidney transplants, for instance), coroners began to clash with those they had co-operated with in the first place to raise their professional status. The Carol Morris case exemplified that trend and soon led to international scrutiny too. In this way, explicit disputes had a global impact.
International Impact
There had been an initial ‘transplant fever’ across the world from 1968. As the Observer reflected there were ‘more than 100 heart transplants by 64 teams in 22 countries. But most of the patients died, succumbed to infection or rejection, the biochemistry of which was not clearly understood, and the fever never faded’.67 In the mid-1970s, many thought that the transplant era ‘was over’ because the new technology had ‘left in its wake considerable distaste for the eagerness with which some surgeons had joined the transplant rush’.68 An added logistical issue was that governments saw such risky operations as an electoral liability. Few wanted to divert their healthcare budgets to fund the research and development of transplant units, even though survival rates and immunosuppressive drugs had improved by the end of the 1970s. Papworth had raised the profile of heart transplants in Britain, but whether they could sustain their success depended on more funding by medical charities and better management of the attendant media publicity. This is what made the Carol Morris case noteworthy. For, it exemplified that public relations were an intrinsic aspect of the transplantation era whether the medical community liked it or not.
It was in many respects ironic then that those involved in the Carol Morris/Nigel Olney heart swap expressed surprise about the negative coverage after the coroner’s explicit dispute exposed the details of the case to media scrutiny. For, in an interview with Christian Bernard (who carried out the first heart transplant in the world) for Tomorrow’s World televised on the BBC in 1968, the audience of medical experts and church leaders assembled from across Britain kept making repeated criticisms of his team’s ‘mishandling of the media publicity’.69 He was asked ‘why he had made available pictures of the donor and his relatives’, and ‘why had he made the personal details of the donor made known to the recipient’ when this was unnecessary? It could be interpreted as a breach of the Hippocratic Oath’s commitment, to maintain patient confidentiality at all times. Bernard defended:
‘If you could do that you’re a better man than I am. … It was just impossible’. He elaborated on how: ‘We tried to stop all publicity to start with but you will well remember that when you heard the first reports of this no names were mentioned. But after this it was completely impossible, it just snow-balled, we had no control over the matter. It’s just something that you can’t control’.70
Bernard then threw down a challenge to whoever did become the first heart transplant surgeon in Britain. If they and their team succeeded in controlling, limiting or stopping the publicity of the inevitable media frenzy, then he would, he said, ‘Take my hat off to them!’ The transplant team at Papworth Hospital soon found themselves in an equivalent situation in the early 1980s. Yet, they could have designed a better and more confidential transfer handover process. Precedents in kidney transplants were established, and the controversial South African heart transplant situation meant professional lessons had been publicised. Equally, the Coronial Office could, and sometimes did, countermand new procedures that were put in place because they had the individual discretionary justice to do so in England. Explicit disputes were thus literally ‘the heart of the matter’ in many localities outside of London.
The change in the law that the Carol Morris case created to protect the anonymity of donor families, and by extension their recipients, was to have far-reaching sociocultural consequences, but not necessarily ones that were anticipated at the time. There did appear to be strong ethical grounds for checking media intrusion, especially in Britain where the tabloid press were persistent in pursuit of a newsworthy medical breakthrough. There was also a reasoned medical case put forward that some recipients who knew their donor’s identity did experience psychological pressures, which included feeling guilty about being the beneficiary of someone’s death. Recipients likewise expressed concern about not having the physical energy for any emotional involvement in another family’s trauma. Yet, it is equally apparent that around the world as countries adopted British standards, the sociocultural distance between donor ‘gift’ and recipient got wider and wider as transplant techniques improved. So much so that eventually ‘Red Markets’ have been created in countries like India, as Scott Cairney points out (see Chapter 1), which have facilitated organ ‘vendors’.71 It is a disturbing irony that anonymity, which was introduced to protect the Morris family and many others like them, also shields unscrupulous body brokers operating as spare-parts traders via the Internet in many of the poorest parts of the world today. This socio-medico reality has recently been the subject of renewed debates in transplant surgery circles about whether to rescind or keep anonymity. Briefly, we consider this outcome of the human stories we have been examining in this first half of the chapter, and which reflects the importance of their wider historical lessons.
In Belgium, politicians debated in 2009 whether better communication should be facilitated between ‘live’ donors (and/or grieving families in cases of sudden death) and their living recipients.72 They commissioned studies to test public sentiments. In one leading example, a representative sample was identified of 249 transplant patients, and, of these, 176 people took part in an opinion survey. Some 70 per cent of those participants (n=123) wanted to maintain the status quo for the psychological reasons stated above, namely, the recipient would find it very difficult to cope with any emotional engagement with the donor family. Around 19 per cent (n=11) were keen, however, ‘to obtain some information about their donor’ and would at some point wish to ‘express their gratitude’. Meanwhile about 42 per cent (n=72) of the sample ‘would worry about the donor having a different background to them’, and what differences would mean (there was no suggestion of racism but rather concerns about socio-economic status, class and educational differences) in terms of relating to each other. Nonetheless, 36 per cent (n=55), having considered the survey carefully, thought there probably should be a change in the law to connect people in the ‘gift’ relationship and make it more ethically transparent. Eventually, it was concluded that: ‘Prudence to change the law is warranted, as only a minority of patients are in favour of rescinding the anonymity.’ The matter was tested again in the Netherlands in 2015, and a survey of about the same size and scope (again involving liver donations) came to the conclusion that: ‘There is no need to change the current legislation on anonymity of organ donation.’ However, it also found ‘that most liver transplant recipients would like to receive some general [author’s emphasis] information about their donor’. Therefore, ‘clear guidelines on the sharing of donor data with recipients needs to be established’.73 Moreover, in countries like Israel and the USA, studies have recently been delivering similar messages. Provided transplant co-ordinators take the initiative and facilitate appropriate contact between donor families and recipients in all types of surgical interventions (heart, lungs, kidneys, eyes and liver), then there is a public appetite for promoting more personal interactions, paced properly and sensitively handled.74 The Carol Morris case continues hence to be the focus of global ethical debates, even by those who are unaware of how the powers of an explicit body parts dispute by her Leicester City coroner were to change the terms of reference in transplant history for everybody in Europe and beyond. Having therefore engaged with these human stories we now need in Part II of this chapter to evaluate their ingrained historical lessons to reconsider how and with what outcomes the power and palette of the Coronial Office endured for so long. To do this, we need to look in more detail at the systemic flaws in the Coronial system of handling the dead – picking up on themes we have encountered in Chapters 2 and 4 and now expanding on them – namely, the extra time coroners spent with human material, how it was harvested, and in what ways the flawed system of death certification potentially undermined the precious information that could be generated from ‘causes of death’ pathologies to further medical research in the modern era. In other words, the next section is concerned with how micro-stories, reassembled from their dissected remains, have macro-lessons of significant longevity in hidden histories of the dead.
Part II
More Extra Time of the Dead
Adverse publicity generated by the Coronial Office was placing anatomists too in a very uncomfortable professional position by the 1980s. In the media, they had been busy promoting body bequests as the ethical way forward since 1954. Few relished being tarnished by the sorts of explicit body disputes happening routinely in organ donation. Practically speaking, however, anatomists had to find a way to continue to work with coroners involved in sensitive explicit disputes to keep up their supply-lines. As a result, most anatomists became evasive and publicity shy when asked about the specifics of their workload, fearful that being honest could undermine their campaign for more body bequests. This atmosphere of public engagement on the one hand and public retreat on the other hand, sometimes created the misimpression that all cadaver work was suspect, when, in fact, anatomists were just being cautious to protect essential supply-lines for better medical education. An added operational difficulty was that in the Thatcher era, all NHS facilities were under intense financial pressures to cut budgets. Staff were being made redundant or leaving voluntarily to train in another career. Hence, the medical research sector started to contract. Often administrators were hit by the first rounds of budget squeezes. As a result, the bureaucratic time it took to process dead body bequests inside the medical school system was elongated. By 1993, it could take up to an extra thirty-one months in some training facilities to get human material signed off officially by the Anatomy Inspectorate at the DHSS. These bureaucratic inefficiencies not only created the potential for discrepancies to occur from time to time but also started to alert the public to paperwork slippages. Those covered in the media created a climate of mistrust by the end of the 1990s when the tide of public opinion turned against the medical research community. To appreciate that context, and how it was to shape debates surrounding HTA2004, it is important to engage with how much extra time with the dead was first created inside the system (as we did in Chapter 4) and then extended (as we will do here).
The way that the system of supply worked was that when a death occurred on the wards of a teaching hospital, it was reported to a coroner. S/he then asked a pathologist to do a post-mortem to rule out medical negligence, as we saw above. If the cause of death was obvious, then the body could be passed on as a bequest, or a body part such as the heart could be retained for future research. This was entirely in the ‘gift’ of the coroner, provided the donor family had been consulted beforehand. That then opened up the possibility for dissection. Provided there was no reason not to go ahead, a medical school would receive a bequest body in the usual way. For up to two years, medical students would train on the corpse. Once this had finished, the human remains went for ‘disposal’, generally by cremation authorised by the anatomist on duty (see Chapter 2). All of the paperwork so far inside this system of supply looked straightforward, until, that is, one examines the official returns to the Anatomy Inspectorate for the 1990s. These reveal minor but important paperwork discrepancies.
In a significant number of cases, the signing-off certificate that should have been issued at the time of cremation was delayed – sometimes for up to another three years post-cremation. Grieving families generally assumed that at cremation, ‘disposal’ was certified and then the case closed as signed off by the dissection team, but this was not always the case. The coroner, for example, could delay issuing a final sign-off certificate if body parts, human tissue or cell-lines had been retained for ‘further consideration’. Hence, these were not cremated with the residual corpse after dissection, a situation exposed during the NHS organ retention scandals in 1999. The absence of a final signing-off notification was in fact ample proof that parts and pieces of the corpse might be used to push past a deadline. The anatomy auditors either did not notice this discrepancy on the part of pathologists (who kept the retentions), or by convention chose to ignore what was not their business. Either way, the system of supply did not operate in such a way that officials could easily take an overview of all the discrete research steps involved, reiterating the autonomy and discretionary power that has often featured in this book. The power and palette of the coroner was pivotal to this system of retention and recycling.
A further complication is that even though most anatomists worked within the law according to HTA1984 (keeping detailed records and ensuring that bodies were signed off locally before cremation to complete paper trails), the DHSS centrally was not necessarily following suit. Serious underfunding of the Anatomy Inspectorate during the Thatcher era meant that if for any reason paperwork related to a dead body that then went for cremation got held up inside the reporting system (the local sending in returns to central control that got delayed), it could remain in an overworked official’s in-tray (now that staffing had shrunk) and not signed off centrally, sometimes for as long as three years. Under normal circumstances, this would not have mattered. After all, it was an internal procedure. The body in question had finished being dissected and was cremated properly with an appropriate ceremony. Yet, it also left open the opportunity for future criticism of anatomists that they were not in full control of their internal audit mechanisms: facets of their working-life that would be closely scrutinised in the run-up to the HTA2004. Anatomists also kept little track of Coronial material designated for ‘further consideration’ that might involve more research study for an extended time period. Several cases are illustrative of this sort of routine gap in the record-keeping.
An elderly man aged 85 died of a stroke on 22 March 1993. His body went to King’s College medical school. This was done with the co-operation of the Coronial Office on 25 March 1993.75 The original cadaver was then sent for ‘disposal by cremation on 23 May 1994 to the South London Crematorium’. Thus, it underwent dissection study for 14 months in total. The final signing-off certificate was not, however, issued by the Anatomy Inspectorate, centrally (having been originally countersigned locally by King’s College anatomy department) until 12 December 1996, another 2 years and 5 months post-cremation. Whether this involved the ‘further consideration’ of any human material taken from the Coronial supply-chain was not disclosed or recorded. Similarly, when a female aged 75 died of ‘MI [myocardial infraction, a heart attack due to lack of blood flow] on 3 January 1993’, with the co-operation of a hospital coroner, she was passed over to St George’s Hospital medical school for dissection on 7 January 1993. That is, once the pathology had been done on her defective heart over 5 days, the original body shell was then dissected until 6 October 1993 before being ‘disposed of by cremation’, again at South London Crematorium. Once more, however, the signing-off certificate was delayed, not issued in this case until 12 November 1996, another 3 years and 1 month post-cremation. In terms of the complete paperwork trail, this body looked like it had been retained for a total of 3 years and 11 months, whole and in part(s). Again, whether this covered human bio-commons taken for ‘extra consideration’ is not clear.
The anatomical sciences, without anticipating how public perceptions might view this bureaucratic slippage, were leaving themselves wide open to future criticism that they had lost sight of a series of all their discrete research steps, when in fact it was the central authority that was letting them down. It was unfortunate that systemic flaws in the bureaucratic system for signing off the dead (the result of understaffing problems) made it look like what was happening was that hidden histories of the body were designed to deliberately flout HTA1984. Generally, they were not, but the gap between the public rhetoric denying systemic problems (everything is fine and functioning well – the official DHSS line) and the reality of financial constraints (constant financial cuts, and corners cut in paperwork by exhausted personnel) was never properly explained to the general public to protect the supply-lines of anatomists from coroners. As a result, when we look at the official figures from this time period, they look odd. It appears that anatomists were spending more extra time with the dead than may always in fact have been the case. Figure 5.1 illustrates this common situation by using the example of UMDS medical school (one of the biggest in London, combining anatomical, medical teaching and dentistry training) which first featured in Chapter 4. A sample year of 1993 has been chosen to illustrate trends in the time lag of signing-off procedures. However, although these figures show that the creation of this extra time of the dead was not the fault of those working in individual medical schools, it does raise the question: Did these time lapses created by the central authority become something that later those that wanted to keep hold of more human material for ‘extra consideration’ took advantage of? In other words, did the systemic flaws in the system of processing the dead, after Coronial, pathological and anatomical work, create the canvas on which explicit body disputes were to be played out? To answer this question, we need to delve deeper into the archive material.
Returning to the large anatomy data-set of national trends that underpinned Chapter 4 (data displayed in Figures 4.6 and 4.7, and Table 4.3), it would appear that from 1993 onwards it became normal to delay the sign-off of human material post-dissection.76 This happened as a matter of course not just at leading London medical schools, like King’s College, St. George’s and UMDS, but also at Bristol, Manchester and Liverpool medical schools too. Consequently, in the record-keeping one can observe the broad contours of what would become the prime locations of NHS organ, heart and human tissue scandals, some seven years before they came to public attention. Thus (by way of example), there were 55 bodies in the 1993 teaching cycle in which ‘extra time’ was created after initial cremation. Again Figure 5.1 focusses on 30 of those 55 bodies donated to UMDS, since it illustrates the typical time frames of retentions that may have involved more recycling of material. Altogether the human material was not officially signed off for 3 years and 10 months, even though the corpses supplied from Coronial officers were cremated after 1.5 years. In other words, in cases that were potentially already explicit disputes inside the system of processing for teaching and research purposes, there is an extra time of the dead of 2 years and 4 months which is unaccounted for. It might be a bureaucratic slippage as a result of financial factors constraining less staff to sign off the paperwork centrally, or we could be viewing a process of ‘extra consideration’. We will probably never know which because the archival record is so patchy, but nonetheless we are glimpsing a hidden history of the dead arising out of explicit disputes, and one of some longevity. Today this is no longer legal, as Figure 5.2 explains.
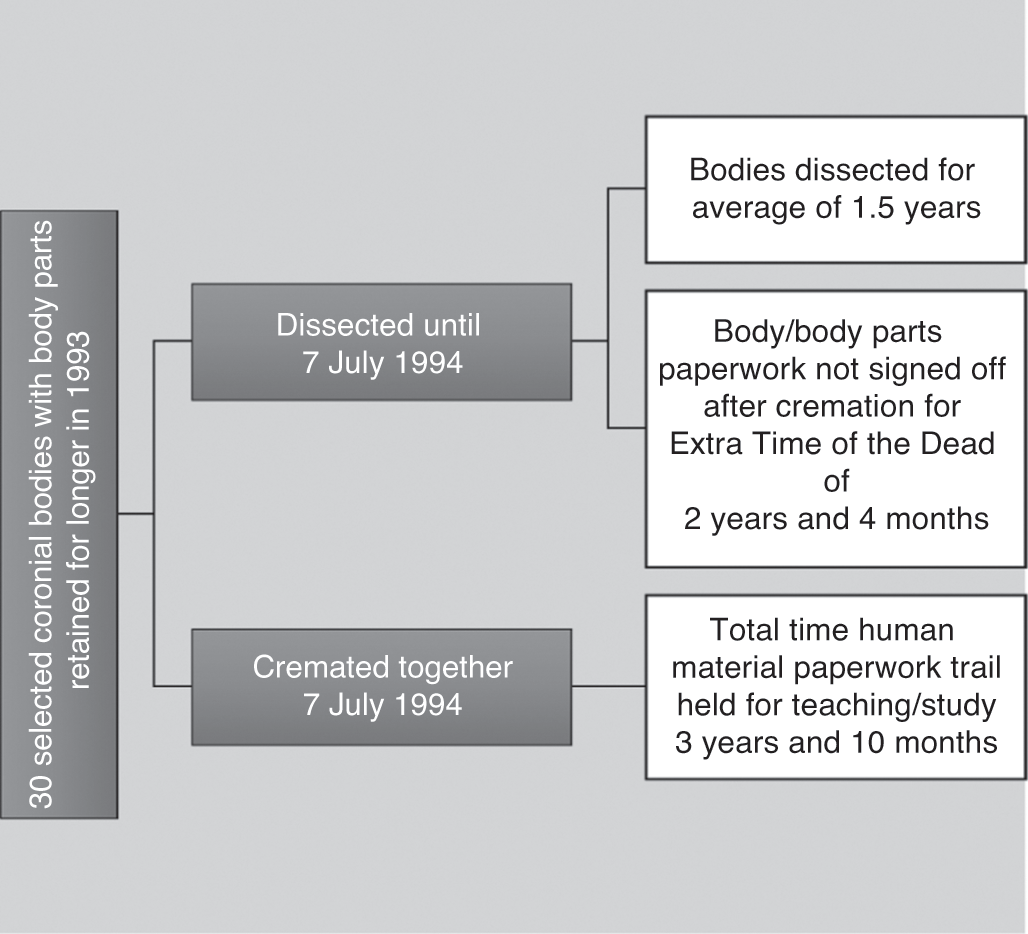
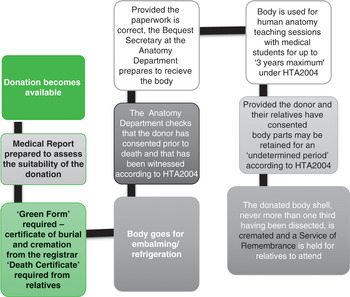
Any attempt (intended or by default) to elongate the authorised paperwork trail that processes the donated dead is no longer permissible under HTA2004. As Figure 5.2 shows, the maximum retention period is three years for the body, though generally most are cremated after two. Significantly, no more than one third of the donation bequest is used for ‘teaching and/or further examination’. This code of practice is to guarantee human dignity in the dissection room. Provided, however, that the donor and their relatives have agreed to it, body parts can be subject to a bequest for ‘an undetermined’ period. This must nonetheless have been the result of fully informed consent. In other words, there is still an ‘extra time of the dead’ inside the system, but it is now a transparent process rather than a covert one. Altogether the old system of ‘extra consideration’ that we saw in Figure 5.1 has now been outlawed by the new system of ‘an undetermined period’ with fully informed consent in Figure 5.2. This means that the explicit disputes of the past have now been redressed, but before we leave behind that context we need to pause and appreciate what all this extra time with the dead (intended and unintended) meant. Thomas Laqueur writes: ‘Death in culture takes time because it takes time for the rent in the social fabric to be rewoven and for the dead to do their work in creating, recreating, representing, or disrupting the social order of which they had been a part.’77 We can only know this, however, in terms of how medical research recycles the dead by first finding and mapping material fates found in the death certification processes of dissection, its pathologies and the performance of actor networks. If we are to follow explicit disputes from human story to advancement in medical science, then we need to also ask two related research questions in the final stages of this fifth chapter. If Coronial remains were pivotal for anatomical teaching and practice, the expansion of pathology and forensic medicine, as well as more wider research cultures, what role did their death certification process play in improving public health in Britain after WWII? In this way, were body disputes the bedrock of better medicine for everybody, and did this justify their bio-commons?
Coronial Necropsies – Missed Opportunities and Their Public Health Costs
In the early 1980s, the National Patient Safety Agency (hereafter NPSA) commissioned a series of annual reports paid for by medical charity funding under the auspices of the National Confidential Enquiry into Patient Outcome and Death (referred to from now on as the NCEPOD), which we touched on in the introduction to this chapter.78 The aim of the initiative was threefold: first, to better understand why patients died in large medical facilities, such as NHS teaching hospitals. Second, to ascertain what Coronial reports indicated about ‘real’ causes of death on a national, regional and local basis in order to improve healthcare standards. Third, to identify whether pathologists could help improve autopsy reports and assist with auditing perioperative deaths. Professional bodies like the Association of Anaesthetists and Surgeons and the Royal College of Pathologists and the Coroners’ Society agreed to co-operate with the NCEPOD to try to improve best practice. It was, however, the NCEPOD report for 1990 that would cause the most controversy by identifying that with respect to autopsy reports, ‘communications between pathologists’ (whether working in hospitals or with coroners) ‘and clinicians is so poor that useful lessons cannot often be learnt’. As a result, a Joint Working Party of the Royal Colleges convened in 1991. It recommended that there should be a more ‘systematic monitoring of the discrepancy rates between ante-mortem [patients’ health profiles] and post-mortem diagnoses’, with this vital clinical information being made ‘more widely available to consultants’.79 In other words, there was a recognition that explicit body disputes existed, they were generated by Coronial cases, and yet, not enough was being done to learn from them. Cases that attracted a lot of adverse publicity had therefore no balancing mechanism of a public gain for the medical scientific community. Bio-commons was not necessarily beneficial for everybody.
Further complicating this common situation was that central government defended its position about a lack of public health gains by pointing to better clinical audit procedures that were enshrined into the National Health Service and Community Care Act (Eliz. 2 c. 19: 1990). That new legislation had created self-governing NHS trusts, as well as GP fund-holding practices. They were now responsible for managing healthcare and welfare services in the community, including their financing.80 This was creating serious resource issues for the Coronial Office, with central government finance re-diverted to NHS frontline need. With less in local budgets for coroners and pathologists to spend, fewer healthcare lessons were passed on. The situation was a missed opportunity cost. It was becoming unaffordable for the dead to improve medical outcomes for the living. There thus remained uncertainty inside the reorganised NHS system as to whether autopsy results were in reality informing clinical practice or not, with many practitioners sceptical that they did so.81 Against this backdrop, the fact that autopsy rates declined significantly between the 1990s and the passing of HTA2004 appeared to be a worrying trend. Consequently, the NCEPOD in 2006 undertook a new investigation styled: ‘The Coroner’s Autopsy: Do we deserve better?’ Its ramifications were to be far-reaching.
The NCEPOD 2006 audit highlighted that the Broderick Report (1971)82 and the Lucre Report (2003)83 had both indicated that there were persistent problems with autopsy reporting procedures across the United Kingdom. It remained the case that as late as 2006 there was ‘no single body or department that oversees death certification and coroners’. Exacerbating this situation was the fact that ‘the service is part local and part national’. Although most pathologists worked for the NHS, ‘coroners are appointed by the Lord Chief Justice and come under the Department of Constitutional Affairs’. So even when a coroner and pathologist worked side by side, each had a different reporting mechanism, as well as different systems of audit and accountability. In addition, the Registrars of Death responsible for monitoring the accuracy of death certificates remained the responsibility of ‘the Office for National Statistics … under the aegis of Her Majesty’s Treasury’. The NCEPOD thus concluded: ‘There is no centralisation or unification of responsibility and accountability’ involving the Coronial Office. As a result, potentially many sorts of body disputes were being generated by a lack of communication, sporadic co-ordination, and ad hoc customary practices in Coronial autopsies, even post-HTA2004. They hence asked a pressing question: ‘What level of quality in the Coronial autopsy service does the public want?’ Answering this conundrum proved to be provocative because there was a mismatch between public perceptions and actual Coronial working practices of some longevity.
NCEPOD 2006 set out that there was a historical problem with the basic cost of autopsies to the taxpayer – a controversy stretching back to the 1830s – which had never been resolved.84 It had continually undermined the official reach of the Coronial Office in England and Wales. The public expected a high standard of service and coroners to be accountable, but such aspirations did not match adequate funding allocations. As NCEPOD pointed out, ‘when considering the variable quality of the current autopsy process, several pathologists and coroners commented: What do you expect for £87.70 [the current fee for a standard autopsy without further investigations]?’ Low fees meant spending no more than thirty minutes on an autopsy. Coroners paid pathologists to do their pathology work but had to factor in the opportunity costs associated with budget shortfalls. This had given rise to what this book calls a system of presumptions. That is, over time the public made assumptions about coroner/pathologist working relationships that did not match realities. For instance, most coroners on cost grounds continued to tolerate a certain level of amateurish procedures due to underfunding. Many autopsies had the official appearance of a forensic examination, but they are nothing of the sort, as the standard modus operandi of a detailed ‘post-mortem’ remained undefined in law. Consequently, the NCEPOD found that there were significant levels of misinformation inside the autopsy system, exacerbating a lack of clinical clarity. Very basic and routine mistakes happened a lot because of poor or illegible handwriting on rushed reports written hastily by coroners and pathologists. It was impossible to engage with autopsy outcomes because they were often indecipherable. In a digital age, this was unquestionably outdated and represented an opportunity cost for researchers to better engage with both the demographic and geographical subtleties of mortality rates in community medicine. Against this backdrop, the NCEPOD report in 2006 became the focus of a national debate about the future of the Coronial Office.
In 2005–6, the NCEPOD audited 114,600 autopsies (some 22 per cent of a total of 513,000 deaths that year) in which the Coronial Office was involved in England and Wales. In terms of those demographics, one headline announcement that was to shape media reaction was that ‘the advisors had concerns over the quality of autopsy examinations in the very elderly’. They concluded that ‘these were done less carefully than those on younger patients’. In an ageing population, this was a noteworthy trend, especially since anatomy teaching and research were reliant on the gerontology of necropsy bequests. There was little joined-up thinking between coroners/pathologists/anatomists of the sort that had characterised the Victorian era. A summary of the audit study also observed how:
One in four autopsy reports was judged as poor or unacceptable
In one third of mortuaries, the pathologist failed to inspect the body before the anatomical pathology technologist commenced opening it and removed the organs
In one in sixteen cases, it was deemed that histology should have been taken in order to determine the cause of death
In nearly one in five cases, the cause of death as stated was questionable
The extent of the examination of the heart, in those with abnormalities that might be due to cardiomyopathy (some of which are inherited), was poor
The extent of the examination of patients with known epilepsy who died unexpectedly was poor
There was poor recording of the presence of external injuries
The examination of decomposed bodies was of poor quality
There was poor communication between coroners and pathologists
There were significant gaps in the information provided to the pathologists by the coroner85
Since WWII, it ought to have been the case that Coronial necropsies were a potential ‘treasure trove of information’ (as this chapter argued earlier). Instead, ‘real causes of death’ remained ‘hidden because of indifferent post-mortem examinations’. Done hastily, they were often ‘obscured by deficient recording of data’. Such basic flaws had not been resolved for over fifty years.86 It was thus self-evident to many inside the profession why disputed bodies came about from the 1960s to the 1990s. As one coroner described it: ‘The system is confused chaos [run] more by default than by design.’ Hidden histories of the dead thus mattered and still matter for the living. For every explicit dispute, there needed to be a much better public health gain. Central government’s solution was to launch an inquiry into the power and palette of the Coronial Office, but this soon proved to be controversial too.
Around 2006, after the NCEPOD report was published, the media turned their attention to a central government proposal to create a new Chief Coroner for England and Wales. Extensive newspaper coverage debated whether this was justified on costs grounds or not. Central government proposed that the person appointed to the new role must get rid of a lot of wasteful bureaucracy and instigate a reformed system. Only this approach, it was argued, would begin to counteract explicit body disputes and the lack of public health gains: the latter was occurring on a regular basis. Everyone agreed with the NCEPOD main findings. Public health schemes should be better informed by Coronial statistics in a biomedical era. Yet, how this was to be counterbalanced with the desire to strengthen the impact of the Inquest process was unclear. What complicated the contemporary debates was that a global recession occurred in 2007. It would require a large budget to set up a new Chief Coroner’s Office at a time of severe government cutbacks. Exacerbating this budget issue was that after the Coroners and Justice Act (Eliz. 2 c. 25: 2009), there was an expectation that the new legislation would overhaul a Coronial system with three inherent structural problems. First, there needed to be unambiguous leadership at the top of the Coronial service to direct future policy making. This strategic focus should be in line with central government thinking and reflect the range of stakeholders that coroners had to work with on a regular basis, including the public, pathologists and the police. Second, there had to be a better system of public accountability that would involve streamlining diverse local working practices so that these were co-ordinated around strategic priorities to improve the Coronial service overall. Third, the devolution of funding and its historical discrepancies had to be rectified. What then complicated this tripartite juggling act was a political commitment in the new Bill. It promised to uphold a new Charter for the Bereaved, which ‘set out a range of service standards and consumer rights’.87 The general public wanted more medical information, better consultation and improved communication channels, with the option to appeal against a coroner’s verdict when, for example, ‘viewing a body’ or attending an Inquest.
In considering this insider/outsider set of stakeholders and their different perspectives, Alexander Pitman was one of a number of expert commentators who highlighted the inherent flaw with central government’s public engagement aspirations. He told the press, ‘The possibility remained that the Charter might raise expectations beyond the capabilities of the service, offering bereaved people a list of laudable but unenforceable empty promises [sic].’ The latter was discussed at length during the second reading of the Bill.88 In other words, the question of how to bridge rhetoric (legislation) versus reality (working styles) was a significant Coronial hurdle. As a result, a three-year consultation process began against the backdrop of the global financial crisis.89 The Coalition government (2010–15) threatened to cancel the new office of Chief Coroner to help meet the budget deficit, but then did another volte-face when confronted with concerted opposition by Parliaments’ Public Administration Select Committee, influential pressure groups such as INQUEST and the House of Lords. After much political wrangling, the new Chief Coroner, appointed from the judicial circuit, was told to prioritise cost analysis right from the start of taking up office in July 2013. Reviewing the subsequent annual returns of the reformed Coronial Office is instructive about how exactly the new changes would redress explicit body disputes, improve public health gains from Inquest information and streamline procedures that were still ad hoc in the regions. The simple answer is that this was an impossible task. Findings explain the longevity of ingrained problems with the power and palette of Coronial Office responsibilities, as we approach the conclusion to this chapter.
The Coroners’ Statistics Annual Report for England and Wales is issued in May each year as a Ministry of Justice bulletin. It is the main legal instrument by which leadership, accountability and devolved budgets of the Chief Coroner are measured. These three facets of the working portfolios of all Coronial offices also feed into the Office for National Statistics mortality figures. In 2015 some
234,406 deaths were reported to coroners … an increase of 12,565 (6%) from 2014 … [with] just under half (45%) of all registered deaths [being] reported to coroners … [in] the last ten years, this proportion has been generally consistent within the range of 45% to 47%.90
In terms of post-mortems, some ‘89,206’ were ordered by coroners, or ‘38% of all cases reported to them’. That said, not all post-mortems required that an Inquest come to court. Some are now ‘a paper inquest’ – a process that used to be known as a ‘non-Jury’ inquest in the past. In fact, since ‘1995, the proportion of post-mortem inquests has decreased by 23 percentage points, from 61% to 38%’. Examining those statistics in Figure 5.3, it is evident that there had been a decline in post-mortem work (broadly defined) after the mid-1990s, from 126,398 cases in 1995 to 119,610 by 2003. Yet after the passing of HTA2004, there was a further falling off of post-mortem work, with a downward trend of about 5,000 Coronial cases in every biennial accounting cycle. Chapter 6 will be exploring the impact of these trends on the work of pathologists, too. Meantime, the overall picture of post-mortems from 2011 to 2015 now has stabilised, with 95 per cent of all coroners’ cases requiring a standard post-mortem.91 Generally, 20 per cent required histology and 14 per cent toxicology (to ascertain class A drug or alcohol abuse, as well as poison from a drug overdose in cases of suicide). These are therefore the remaining potential explicit body disputes still in the system, though many have now been modified by the HTA2004’s fully informed consent provisions. It remains, however, to be seen whether public health measures will improve because the system is still not uniform, remains underfunded and still operates by a considerable amount of discretionary justice: we conclude by reflecting on these historical observations of some longevity from Part I (human stories of explicit disputes) and Part II (their creation by the Coronial Office) of this chapter.

Conclusion
Delays have been a very big problem, and they continue to be a big problem. If there is one thing that comes across my desk on a regular basis, which is more distressing than anything else, it is families writing, saying: Why has there been three years’ delay? Why has there been five years’ delay? Why has there been seven years’ delay? Why has there been no date? Why don’t I have a date for anything? When is my inquest going to be? What about my family? We are all distressed. One case came in my direction recently where the High Court had ordered a coroner to resume an inquest. He had decided that there was no need to resume the inquest, and was going to leave it at that. But the High Court decided otherwise. So they ordered the coroner to resume the inquest. Unfortunately that case got forgotten about. The papers got put on a shelf in the back of the office for six and a half years. When it was brought back, the family not surprisingly wanted a new coroner to conduct their inquest. I helped them, and they got one. So delays are really poor, and they need to be reduced.92
In a history of explicit disputes, it was the sense of more ‘extra time of the dead’ inside the Coronial system that created the context for families to become frustrated by the amount of bureaucracy involved. Many expressed cultural reservations about losing control of a loved one’s body, especially once the transplantation era opened. And, as the above quotation by the Chief Coroner for England and Wales confirms from 2013, this historical problem of procedural delays has not necessarily been resolved in the intervening years. Hence, in 2015 the Criminal Law and Justice Weekly reported that: ‘The most recent report of the Judicial Conduct Investigations Office showed 556 complaints were made about coroners in 2015–2016, up from 262 in 2014–2015 and 51 in 2013–2014.’ By way of example, they cited the following case:
Mary Hassell, senior coroner for Camden, Islington, Hackney and Tower Hamlets, in a letter to Camden Council, extracts from which were quoted by the Mail on Sunday last year, alleged bullying and intimidation by the Orthodox Jewish Community in the wake of her decisions to order autopsies against the wishes of some members of devout religions. Following investigation of a complaint against her, to the Judicial Conduct Investigations Office, the Lord Chancellor and the Lord Chief Justice concluded that Ms Hassell had not misrepresented or distorted the position in her letter, as had been alleged, and dismissed this aspect of the complaint. However, they found that her decision to disclose the ‘private letter’ to the media demonstrated a serious lack of judgment, amounting to misconduct, and issued a reprimand.93
This question of tense relationships with the media and what public statements an individual coroner could make has remained one of the most challenging for the Coronial service in its long history. Indeed, at the heart of the all the representative cases cited in this chapter involving organ donation cards was the problem of how to manage the bereaved wanting agency over their dead loved one, transplant stakeholders in NHS facilities and media interest in new biotechnologies, which was often intrusive at the most tragic moment in family life. It was no easy task for coroners to be public advocates and protect the privacy of the grieving. An added difficulty has been the way that coroners were appointed, and then authorised to work on an ad hoc basis. Again, as the Chief Coroner explained in 2013:
There are also signs of a lack of a modern approach amongst some coroners’ offices. I went to one coroner’s office in the north, I won’t say where, where there had been problems with delays, and they were using typewriters. That was a symbol, it seemed to me, of a problem of lack of organisation, and of efficiency. If you don’t have efficiency, you will have delays. You will put that case at the back of the shelf and forget about it because it is a bit troublesome. So there are procedural reforms which have a rather more modern look to them. They involve opening inquests in public, recording all the hearings, setting a date for the next hearing, hopefully the final hearing, at an early stage, and giving directions to experts to provide reports and statements within a short period of time. One coroner said to me: ‘I have a pathologist who’s a bit slow. Usually it takes her a year to produce a report.’ I said ‘That’s not a report. That’s a guess about what her notes mean’ [sic].94
The only way to resolve this situation is to acknowledge that coroners have, for far too long, relied on underfunded post-mortems, often scribbled down, frequently illegible, and these have represented missed opportunities for biomedicine to learn from the dead for the living with fully informed consent. Inside the system, any legal loopholes created by inefficient bureaucracy also shaped public misperceptions in the run-up to HTA2004 that medico-legal staff acted duplicitously with taxpayers that paid their salaries in the NHS. Most did not do so deliberately, but it was nonetheless the impression fashioned in the public imagination. Anatomists suffered from this situation too when their final certificates after cremation were not signed off efficiently or officially by the Anatomy Inspectorate during the 1990s, in some cases by as much as three years at the DHSS. It looked like they were as guilty as pathologists of working their way around the law, when in fact most had been meticulous. Anywhere inside the system in fact, where too many overlapping agencies had been created, gave rise to a potential pathway for a future body dispute – a trend that medico-legal officials lost public sight of. Some medico-legal staff took advantage of this situation to conduct ‘extra considerations’ – a slippery medical research term – that we can only glimpse happening in an imperfect historical record filled with gaps and paperwork consigned for shredding.
The case of Carol Morris (and many others like it) is hence symbolic of heightened disputes about when to ‘call death’ and who could officially vie for disputed body parts from the 1960s through to the end of the 1990s. Herbert Jones (who opened this chapter), for instance, expressed in writing to numerous officials, close friends and remaining relatives in his life his wish to donate post-mortem and give the ‘gift’ of new ways of seeing his body. Yet, once peri-mortem (at or near the point of death), he was frustrated by the Coronial Office involved. This was because he was (strictly speaking) one of the first legal suicide cases in Britain once any foul play and assisted suicide was ruled out: and the ramifications of that Coronial dilemma are still unresolved in Britain today. As we shall see in Chapter 7, the ethical boundaries between suicide and assisted dying remain very controversial – even more so than in Herbert Jones’s day. A painful prognosis like fatal cancer continues on many occasions to confound caring and understandably cautious medico-legal staff. Nonetheless, his explicit dispute is informative about the number of officials that had an official opinion in processes of decision-making. These actor networks could be very extensive indeed. Yet, it has always been vital for coroners to work collaboratively whatever the circumstances of their working-lives. Indeed, this is a commonplace situation that the Chief Coroner acknowledged in 2013, when he commented: ‘It is no good for the coroner to sit back in his office, with the typewriters clicking away in the next room. He has got to work with that rather peculiar triangle within which he has to operate.’95 Unquestionably, he elaborated, one of the main procedural difficulties is that:
A senior coroner is appointed by the local authority but not employed by them, so their line manager is the Chief Coroner, or possibly the Lord Chief Justice. Then you have coroners’ officers, employed by the police. Their line manager is a detective sergeant, or some other officer. Then you have administrative staff, who are employed by the local authority, and line managed by someone there.
In other words, there was, and has continued to be, a: ‘peculiar triangle and it only works if everybody is working together.’ The solution, the Chief Coroner believes, especially when dealing with disputed bodies and complaints about coroners on the rise, is: ‘talking about problems, making sure where there is a disciplinary problem in the office and getting that sorted out, keeping a review of cases on a monthly basis, discussing, collaborating’. The ‘balance of probability’ has always been decided by public engagement, and it thus remains one of the most important communication tools in explicit body disputes involving the Coronial Office.
In the next chapter, we thus explore in more detail why it was that pathologists got that balance wrong in their working-lives and protocols of medical research. We turn next to consider brain retention work because it is even more emblematic to families in body disputes than organs and tissues taken from those involved in tragic accidents like that of Carol Morris that were to make national and international headlines in transplantation with far-reaching consequences for medical law and bioethics. Our final substantive chapter is going to focus on missed disputes that involved research on the brain and its controversial nature in the modern era. For as professionals, pathologists looked very guilty of working their way around the law because the time constraints they operated with proved to be very different from those of everyone else in hidden histories of the body.







 Open access
Open access