



The coronavirus disease 2019 (COVID-19) (severe acute respiratory syndrome coronavirus 2 [SARS-CoV-2]) pandemic has disproportionately impacted racial and ethnic communities across the United States. According to the Centers for Disease Control and Prevention (CDC), racial and ethnic individuals have a higher risk of COVID-19 illness, hospitalization, and death compared with their White counterparts. 1 A study analyzing county-level data comparing counties with higher and lower proportions of Black people found that COVID-19 diagnoses and deaths were higher in counties that were disproportionately Black, with 52% of COVID-19 cases and 58% of COVID-19 deaths occurring in disproportionately Black counties within the United States. Reference Millett, Jones and Benkeser2 The same study also found that higher county-level unemployment was associated with fewer COVID-19 diagnoses, likely due to lower likelihood of exposure. Another study conducted by the Utah Department of Health found that the odds of infection with SARS-CoV-2 (the virus that causes COVID-19), and rates of hospitalization and testing were higher in areas of Utah with geographic social and economic inequities, including: (1) large proportions of Hispanic/Latinx and non-White residents; (2) persons working in manual, essential and public-facing employment sectors; (3) more crowded housing conditions; and (4) food and health care insecurity. Reference Lewis, Friedrichs and Wagstaff3
Crowded living conditions and unstable housing can also contribute significantly to the transmission of infectious diseases and can hinder the use of recommended prevention strategies (eg, social distancing and self-quarantine). A study using data from the 2017 American Housing Survey found that isolation or quarantine was impossible in 25.3 million (or 20.8%) of all US residential units because they did not have a sufficient number of bedrooms, bathrooms, or both. Indigenous and Latinx people were 2-3 times more likely, and Black and Asian people were 1.7 times more likely to occupy units where isolation or quarantine was not possible. Reference Sehgal, Himmelstein and Woolhandler4 Another study describing clinical outcomes of patients of color who were hospitalized for COVID-19 at an urban hospital found a COVID-19 associated death incidence of 38.6% among Black and Latinx patients. These individuals resided in areas of New Jersey with higher population densities, housing units, and lower income levels than the rest of the state. Reference Okoh, Sossou and Dangayach5 There have also been COVID-19 outbreaks in congregate settings such as prisons, homeless shelters, and long-term care facilities, where Black, Indigenous, and persons of color are overrepresented. Reference Wallace, Hagan and Curran6 Crowded, shared living environments such as these where there is difficulty social distancing and maintaining good hand hygiene, can hinder COVID-19 prevention strategies. Reference Sehgal, Himmelstein and Woolhandler4–Reference Wallace, Hagan and Curran6
In addition, racial and ethnic communities are disproportionately represented in essential work settings such as health care, food service industry, factories, farms, transportation, and warehouses. 7 Thus, these individuals may be at higher risk for exposure to COVID-19 because of the public-facing nature of their work and inability to work from home, as well as the lack of certain work benefits such as paid sick leave. 8 Inequities in access to high-quality education and income can lead to lower paying or less stable jobs which can also put individuals at higher risk of COVID-19 exposure. 1
In the Spring of 2020, the borough of Queens was home to the epicenter of the COVID-19 outbreak in New York City. The neighborhoods of Jackson Heights, Elmhurst, and Corona (which represent Districts 3 and 4 of Queens) were among the hardest hit communities. In Jackson Heights, over half (64%) of residents identify as Latinx, and 18% of residents identify as Asian. 9 In the neighborhoods of Elmhurst and Corona, 51% of residents identify as Latinx and 36% identify as Asian. 9 Approximately 60% percent of residents in all 3 neighborhoods were born outside of the United States, and approximately half have limited English proficiency. 9 Among the Districts 3 and 4 neighborhoods of Jackson Heights, Elmhurst, and Corona, over 80% of the population speaks a language other than English at home. Approximately half of households of adults 18 and older in these neighborhoods speak Spanish. 10 According to the New York City Department of Health and Mental Hygiene, 9 one-quarter (25 to 27%) of residents live in poverty and over half (59 to 62%) are rent burdened, higher than the citywide average. Over 20% of residents are uninsured, which is also higher than the rest of New York City. The obesity rates in Jackson Heights, Elmhurst, and Corona are approximately 20%, and over 10% of residents have been diagnosed with diabetes while nearly 30% of residents have been diagnosed with hypertension. For every supermarket in Jackson Heights, Corona, and Elmhurst, there are 16 to 17 small grocery stores known as bodegas, which are less likely to have healthy food options compared with supermarkets. 9 The high percentage of Latinx and foreign-born residents, poverty, rent burden, uninsured population, and high prevalence of chronic disease such as obesity, diabetes, and hypertension underscore the reasons for communities in Queens being disproportionately affected by the COVID-19 pandemic.
One factor that has not been explored to date is the level of pandemic readiness in the diverse communities such as Queens, New York. This is especially important to assess the needs for community outreach and education of residents. In addition, this information would help public health professionals to develop linguistically and culturally suitable approaches to prepare residents for future pandemics.
Methods
We conducted a cross-sectional study to assess pandemic readiness adult English- and Spanish-speaking residents of Districts 3 and 4 in Queens, New York based on the gap in research and literature. A survey questionnaire was developed in English using a basic pandemic assessment tool from the Red Cross and materials from the Centers for Disease Control and Prevention (CDC) on preventing COVID-19 infection in crowded living conditions. 11,12 The questionnaire was also translated into Spanish by a scholar with training and expertise in survey instrument development. Participants were recruited from community agencies serving residents in Queens Districts 3 and 4. We leveraged our existing relationships with community leaders (including healthcare agencies, community-based organizations, religious institutions, businesses, and elected officials) to promote the study. An electronic version of the survey questionnaire was developed and the weblink was disseminated via emails, newsletters, websites, and/or text messages to the residents within the communities in Queens Districts 3 and 4. The survey questionnaire included basic demographic information (e.g. age, race, education, and employment status), assessment of participants’ readiness for a pandemic (e.g. ability to socially distance under crowded conditions, capacity to avoid others who are ill), and assessment of participant knowledge gain on COVID-19 preparedness after study participation.
Survey results was transferred from a secure online database to Statistical Analysis System (SAS) Software Version 9.4 (SAS Institute) for data analysis. A descriptive frequency analysis was subsequently conducted to examine the demographic variables. A bivariate analysis was performed using Pearson’s Chi-square test to determine the association between various social determinant factors (such as education, employment, social support, and access to healthcare) and preparedness for a pandemic. Multivariate regression analysis was employed to detect whether race, education, and/or overcrowding were causal factors to poor preparedness planning.
To rate the levels of readiness, we categorized survey response using three different levels: beginner, intermediate, and advanced. Beginner level was defined as pandemic readiness with two-weeks supplies of food, water, antibacterial soap, hand sanitizer, disinfectant, and prescription medications (if applicable). Intermediate level was defined as pandemic readiness which included beginner level readiness plus social support to run errands, access to over-the-counter medications, receipt of COVID-19 information from a credible source, access to primary provider and hospital/urgent care, ability to separate 6 feet from others, avoid gathering places, ability to quarantine for 14 days, and ability to avoid preparing foods or laundry if ill from the pandemic. Advanced level readiness was defined as beginner and intermediate level readiness, in addition to having spatial capacity, protective physical barriers, ability to clean and disinfect bathrooms, air circulation using a fan, and being educated about pandemic readiness.
Results
Six hundred fifty-one participants responded to the study. Of those, 516 were qualified to participate in the study, and 306 completed the survey (a response rate of 59%). Among participants who completed the survey, 75% were females, 24% were males, and 1% identified as “Other” (Table 1). Participants resided in the following communities within Districts 3 and 4 of Queens, New York: 70% in Jackson Heights, 21% in Elmhurst, and 9% in Corona. Two percent of participants were between 18 and 24 y of age, 43% of participants were between 25 and 44 y of age, 41% were between 45 and 64 y of age, and 13% were 65 y of age or older. Forty-five percent of participants identified as White, 37% as Latinx, 10% as Asian, 5% as Black, and 2% as Other. Sixty-eight percent were employed for wages, 18% were not employed, and 11% were retired. With regard to educational status, 73% of participants were college-educated, 25% had a high-school diploma or less, and 2% had vocational training. Sixty-five percent also reported having children.
Table 1. Descriptive statistics of study participants in District 3 and 4, Queens, NY
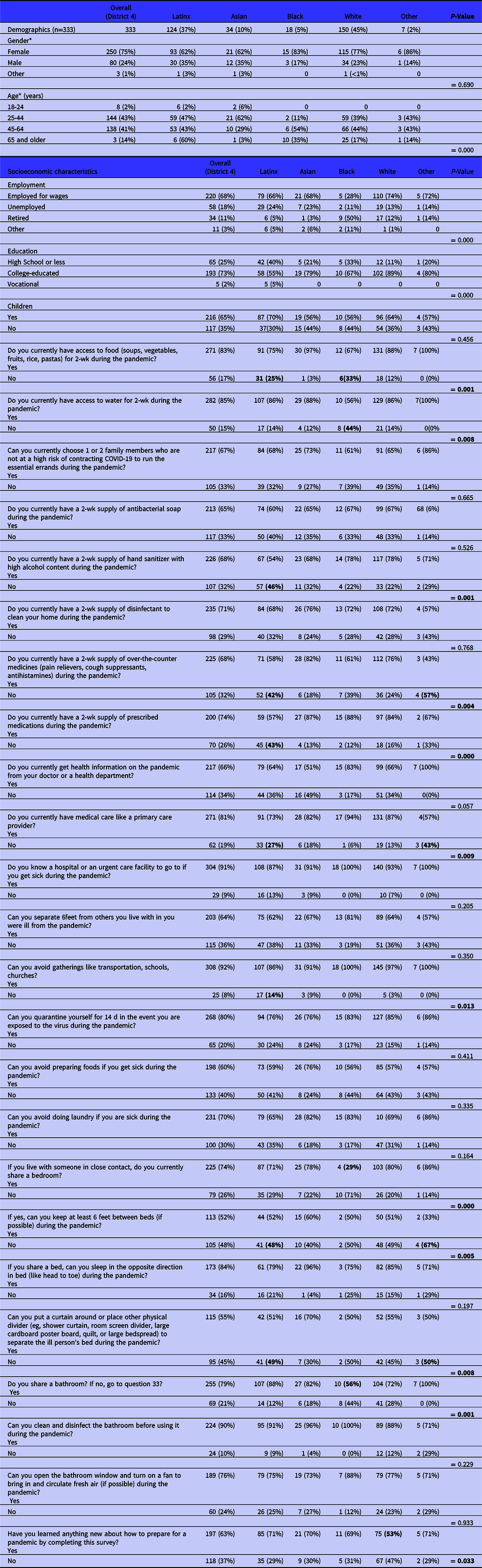
* Percentages may not add up to 100% due to rounding.
The data highlighted in bold shows significance.
Table 1 highlights the significant pandemic readiness findings using Pearson’s chi-squared tests. For basic pandemic readiness, 17% of participants reported not having a 2-wk supply of food. Among these participants, Latinx and White participants were less likely to have a 2-wk supply of food than the other racial/ethnic groups (33 and 25%, respectively; P = 0.001). Fifteen percent (15%) of participants reported not having a 2-wk supply of water during the pandemic, with Black participants overrepresented compared with other racial/ethnic groups, and Asian participants being the least represented (44% and 12%, respectively; P = 0.008). With regard to the survey question addressing a 2-wk stockpile of hand sanitizers, 32% of participants reported not having adequate supply. Among these participants, the Latinx participants were most likely to not have this 2-wk stockpile compared with other racial/ethnic groups (46%; P = 0.001). In terms of not having a 2-wk stockpile of prescription medications, Latinx were overrepresented at 43% compared with the other racial/ethnic groups (P = 0.00014). For over-the-counter medication, 32% of participants did not have access to a necessary 2-wk supply. Among these participants, those who identified as “Other,” Latinx or Black were overrepresented at 57%, 42%, and 39%, respectively (P = 0.004).
When examining access to health care such as a primary care provider, 19% of participants did not have a current one identified. Of these participants, those who identified as “Other” or Latinx accounted for the large majority of responses (43% and 27%, respectively; P = 0.009). With respect to residents’ status with social distancing, 8% of participants were unable to avoid gatherings (eg, schools, and churches) or the use of transportation. Of these participants, those who identified as Latinx were overrepresented at 68% compared with the other racial/ethnic groups (P = 0.013).
The majority of participants who lived with someone shared a bedroom. Of these participants, those who identified as “Other,” or Latinx represented the large majority at 67% and 48%, respectively (P = 0.005). With regard to separating 6 feet apart between beds, 48% of participants were unable to do so. When asked about having to the ability to separate ill persons between beds (eg, protective physical divider), 45% of participants were unable to do so.
At the conclusion of the survey questionnaire, 63% of participants revealed that they had learned “something new” about pandemic readiness through their participation. Of these participants, those who identified as White (53%) were least likely to report having learned something new by completing the survey compared with the other racial/ethnic groups (P = 0.033).
Table 2 presents the results of pandemic readiness according to each level, beginner, intermediate, and advanced. For the beginner level, 11.4% were found to be pandemic ready with 2 wk supplies of food, water, antibacterial soap, hand sanitizer, disinfectant, and prescription medication. For the intermediate level, 5.6% of participants were pandemic ready which includes beginner readiness plus social support to run errands, over-the-counter medications, receiving COVID-19 information from a credible source, access to primary provider and hospital/urgent care, ability to separate 6 feet from others, avoid gathering places, ability to quarantine for 14 d, and ability to avoid preparing foods or laundry if ill from the pandemic. Approximately 7% of participants were advanced ready, which means that they met beginner and intermediate levels in addition to spatial capacity, protective physical barrier, cleaning and disinfecting bathroom, air circulation using a fan, and being educated about pandemic readiness.
Table 2. Level of pandemic readiness in District 3 and 4, Queens, NY

Table 3 compared the level of pandemic readiness with education and employment status. Overall, 82% of participants were not pandemic ready. Participants with no college experience (74%) were more ready than those with college experience (69%). When considering participants at beginner-level readiness, those with college experience were more ready (20%) than those without college-level education (14%). For those classified at an intermediate level of readiness, participants without college-level experience were more ready (10%) than participants with college experience (8.3%). Finally, when evaluating those in the advanced-level of readiness, those with a college level education were more ready (2.1%) than those without a college-level education (1.4%). With regard to employment, a larger percentage of participants who were currently working were not ready (85%) than those who were not working at the time of the study (68%). Conversely, a larger percentage of participants who were ranked in the beginner, intermediate, and advanced level of readiness were not currently working. In considering beginner-level readiness, more participants who were currently not working were beginner-level ready (19%) compared with those who were currently working (10%). This trend held true for the intermediate and advanced readiness level, with a higher percentage of participants who were currently not working considered to be at this level in comparison to those who were currently working.
Table 3. Level of pandemic readiness in District 3 and 4, Queens, NY, by education and employment status

To further elucidate the level of readiness by employment status, the odds ratio (OR) was estimated using logistic regression. Participants who were working had a statically significant lower odds of beginner readiness when compared with those who were not working (OR 0.378). However, when adjusted for gender and race, this was no longer statistically significant.
Discussion
This study aimed to explore the level of pandemic readiness in crowded vulnerable urban communities in Queens, New York. The study shows that urban communities were not adequately prepared for the second and third wave of the pandemic, almost a year into the pandemic. Consistent with other studies, racial/ethnic minorities were less prepared for the pandemic a year following the onset of the pandemic, and after significant resources were likely provided to impacted communities. Latinx persons lack preparedness in almost all areas. They were less likely to have a 2-wk supply of food, hand sanitizer, prescription medication, and over-the-counter medication. One of the reasons for poor preparedness may be related to lack of affordability of these essential supplies due to low income. According to the New York City Department of Health & Mental Hygiene (NYCDOHMH), poverty in these communities is higher than Queens and NYC in general. 9 Surprisingly, Blacks reported not having a 2-wk supply of water. It is possible that Black respondents may have interpreted the question as having a 2-wk supply of bottled water as NYC is known to have reliable and clean tap water for consumption.
The study also showed that both Latinx and Blacks were less likely to have food for 2 wk, which may point to a broader issue of food insecurity in these communities. During the pandemic, it was apparent that racial/ethnic minorities were more likely to be essential workers at supermarkets, food delivery service, and public service industries. Reference Goldman, Pebley and Lee13 Unfortunately, many of these jobs have low-paying wages, which makes it difficult to afford a surplus of food, water, and other supplies for 2 wk or more.
The study revealed a cascading effect of behaviors and factors that make certain racial and ethnic groups more susceptible to COVID-19 infection. Many of these factors impact the communities’ ability to adhere to public health guidance such as socially distancing, wearing masks, avoiding cooking or laundry, and/or having 1 person run errands if ill from COVID-19. For instance, as previously stated Latinx persons were shown to have overwhelming poor pandemic readiness such as the lack of 2-wk supply of food, inability to socially distance, and avoid large social gatherings. The lack of food supply suggests that Latinx persons may not be able to afford food to last for a 2-wk duration or more. The inability to stockpile on necessary food items will force the community to shop at grocery stores, making it difficult to socially distance. Furthermore, the majority of Latinx persons reported sharing a bedroom and unable separate 6 feet apart at home, demonstrating that many may live in severely crowded conditions as indicated in NYC’s data. 14 These compounding factors if left unattended will increase Latinx persons’ risk for COVID-19 infection, and may explain the elevated rate of COVID-19 incidence in Districts 3 and 4.
In terms of the actual level of readiness (preparedness), most people were not prepared for the second and third wave of the pandemic. Many of these communities were still not able to achieve basic pandemic readiness. In fact, the pandemic unearthed many other health disparities experienced by vulnerable communities. For instance, several studies indicated that communities of color (like those represented in Districts 3 and 4) faced an overwhelming inequality with food insecurity during the pandemic. Reference Becerra, Mshigeni and Becerra15,Reference Silver, Faye and Rogers16
The intermediate level of readiness represented the least proportion of the sample. Only 5.6% of participants reported having social support, specifically to run errands, to prepared foods, do laundry, and avoid crowded places. Despite that NYC has approximately 9 million residents, 17 persons from Districts 3 and 4 struggled to find support to mitigate the spread of COVID-19 infection. Lack of social support may make it difficult for them to quarantine for 14 d, which may be due to other competing priorities such as tending to needs of children and families. Nonetheless, social support aides in preventing depression and anxiety. Reference Hlebec and Kogovšek18 Social support is also integral during pandemics where limitation or with restrictions may be placed on individuals, Reference Song, Son and Lin19 whereby a spouse, friend, or relative, can run errands during the pandemic.
The advanced level represented only 7%, indicating the large majority of participants were unable to reach this level, highlighting that space is a critical challenge for many in urban communities. In fact, according to the study by Ahmad et al., Reference Ahmad, Erqou and Shah20 persons living in poor overcrowded dwelling conditions are at higher risk for COVID-19 infection and/or mortality. To address this issue of overcrowding and increased risk of infection, NYC health and hospital corporation developed a hospital program to provide isolation for COVID-19 infected persons who live in crowded settings. Reference Jordan-Martin, Madad and Alves21
Another interesting finding in our study was that over 60% of participants reported that they learned something new by completing the survey, highlighting that information is still not reaching communities that may need it most. COVID-19 pandemic health communication tailored to diverse racial and ethnic communities is important in communicating public health information and guidelines to prevent the spread of the pandemic and to help communities make more informed decisions. According to Alsan et al., Reference Alsan, Stantcheva and Yang22 patients in the United States with poor health literacy, mainly communities of color, experienced poorer health outcomes. Health literacy presents a significant challenge for public health authorities in Districts 3 and 4 as well, particularly if they wish to promote behaviors that prevent COVID-19 infection among residents living in crowded housing environments.
Another startling discovery made by this study was that most employed residents in Districts 3 and 4 were less prepared for the pandemic compared with those who were unemployed. There may be confounding factors or social determinant issues inhibiting their ability to be more prepared. Some of this includes education, income, type of employment, time, and resources. As noted earlier, residents who are essential workers may not have adequate income, time, resources, support, or knowledge to become more prepared.
Conclusions
Our study found that a substantial proportion of communities in urban areas were not fully prepared for the pandemic even a year into the crisis. However, preparedness disparities were more profound among racial and ethnic communities. Latinx and Blacks lacked basic preparedness needs such a food and water for a 2-wk period. Moreover, Latinx were considerably behind with basic COVID-19 preventative supplies such as having hand sanitizer and cleaning supplies. Our study also found certain social determinant factors influence different levels of readiness. Participants with no college experience were slightly more ready than those with college experience. Similarly, more participants who were not working were more ready than those employed. Last, participants who were employed had statistically significant lower odds of beginner readiness when compared with those who were not employed.



