Introduction
Infectious mononucleosis is a relatively common presentation to the ENT department, with patients being admitted because of difficulty in eating and drinking, for dehydration and for pain management. The symptoms tend to last for two to four weeks, and most patients have no further issues once these have resolved.1
The Epstein–Barr virus (EBV), or human herpesvirus 4, is the most common cause of infectious mononucleosis, also known as glandular fever. It accounts for 80–90 per cent of infectious mononucleosis cases, with the remainder caused by other viruses such as cytomegalovirus (CMV).1–Reference Womack and Jimenez5 Over 95 per cent of the world's adult population has been infected with EBV, but only 26–74 per cent of those infected with EBV as young adults will develop infectious mononucleosis.Reference Lennon, Crotty and Fenton3,Reference Womack and Jimenez5
Liver enzymes are elevated in the majority of patients, and time to resolution is variable and not well characterised.Reference Lennon, Crotty and Fenton3 The derangement in liver function is thought to affect 75 per cent of patients and is generally subclinical and self-limiting.Reference Fugl and Andersen4
At discharge, practice varies with regard to follow up of abnormal liver enzymes, and there is no clear guidance for UK practice. General practitioners may be asked to repeat liver function tests at varying intervals, and patients may be subjected to serial liver function testing with no added benefit. Anecdotally, some centres may perform abdominal ultrasound to evaluate the derangement in liver function; the utility of this practice is unclear.
This study aimed to evaluate the utility of liver function tests and abdominal ultrasound in further management of patients presenting with infectious mononucleosis to our ENT department.
Methods
This was a retrospective study of all patients admitted to our ENT department with infectious mononucleosis over a five-year period (1 January 2015 to 31 December 2019). Patients were identified using clinical codes. Infectious mononucleosis was defined as a positive monospot test result and/or positive Epstein–Barr virus serology and/or a clinical presentation in keeping with infectious mononucleosis.1
There was no local guideline on the management of patients with acute infectious mononucleosis in our trust. Patients with suspected infectious mononucleosis generally have a monospot test to confirm diagnosis. In addition, they routinely have standard liver function blood tests, assessing levels of alkaline phosphatase, alanine transaminase and bilirubin. There was no standard practice regarding the use of abdominal ultrasound or follow up of abnormal liver function test results in patients with infectious mononucleosis.
Data were collected via a standardised data collection proforma using the hospital's electronic database. We extracted data on the following variables: age, gender, past medical history of liver disease or immunosuppression, monospot test results, liver function test results, abdominal ultrasound findings, and clinical features of acute or chronic liver failure. Our laboratory's reference ranges for the liver function test parameters were as follows: total bilirubin, 0.0–21 μmol/l; alkaline phosphatase, 30–130 IU/l; aspartate transaminase, 0.0–41 IU/l; and gamma-glutamyl transferase, 0.0–60 IU/l. Results higher than the upper limit were considered deranged. Missing data were excluded from analysis.
Categorical data were presented as count and percentage. Continuous data were summarised as mean and standard deviation (SD), or median and interquartile range if non-parametric. No inferential statistical test was performed. Data were analysed using Microsoft™ Excel® spreadsheet software.
The main outcome measure was the presence of abnormal liver function test results and time to resolution. In addition, we checked the patients’ clinical records for any complications of acute or chronic liver failure during the follow-up period.
Approval for this study was obtained from the hospital clinical effectiveness unit (approval number: 10703). Ethical approval was not required for this project, as the method was retrospective and the methodology did not involve altering patients’ treatment or the services provided.
Results
A total of 153 patients were included (84 (54.9 per cent) males and 69 (45.1 per cent) females), with a mean age (SD) at presentation of 20.9 (5.38) years.
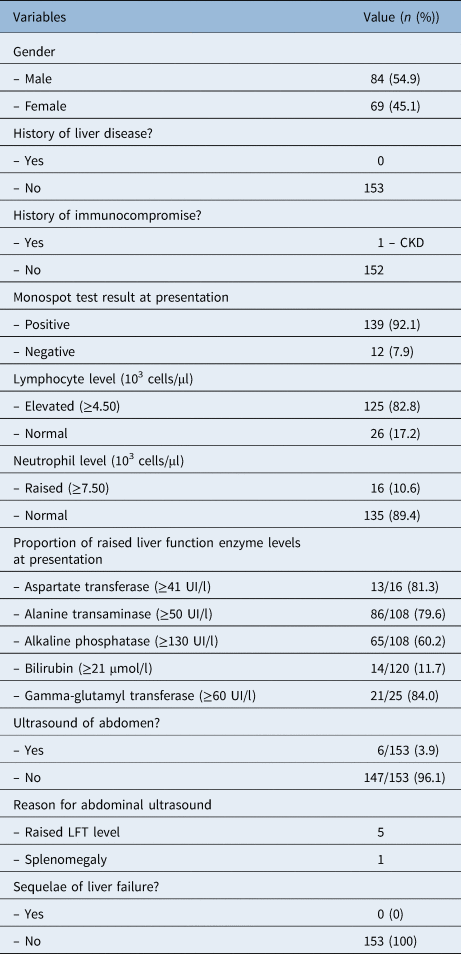
Table 1 summarises the study variables assessed. A positive monospot test result was found in 139 of 151 patients (92.1 per cent) at initial presentation. Two patients (1.3 per cent) did not have a monospot test performed at presentation. The total number of positive cases for infectious mononucleosis increased to 146 of 153 (95.4 per cent) following a repeat monospot test or detection of the presence of immunoglobulin M (IgM) to the Epstein–Barr virus viral capsid antigen in initially negative cases.
Table 1. Characteristics of clinical variables

CKD = chronic kidney disease; LFT = liver function test
A total of 121 patients had standard liver function tests performed on admission. Aspartate transferase and gamma-glutamyl transferase were also measured in 16 and 25 patients, respectively. At least one parameter of the liver function tests was deranged in 99 of 123 patients (80 per cent) at initial presentation. The derangements in liver function in individual test parameters were as follows: aspartate transferase, 13 of 16 (81.3 per cent); alanine transaminase, 86 of 108 (79.6 per cent); alkaline phosphatase, 65 of 108 (60.2 per cent); bilirubin, 14 of 120 (11.7 per cent); and gamma-glutamyl transferase, 21 of 25 (84.0 per cent).
A total of 81 of 153 patients (52.9 per cent) had least one liver function test assessment following discharge. Third, fourth and fifth liver function test measurements were performed in 17 (11.1 per cent), 4 (2.6 per cent) and 4 of 153 patients (2.6 per cent), respectively.
A total of 63 patients (41.2 per cent) who had a least one liver function test parameter raised on admission had follow-up liver function tests conducted in the community. Of these, 33 patients had normal liver function test results at a median (interquartile range) of 32 days (20–50 days) post discharge. Two patients had abnormal liver enzymes more than six months after presentation. The maximum time to recovery in this group was 286 days. The other 30 patients still had abnormal liver function test results at a follow-up period ranging from 1 to 46 days after presentation. None of our patients developed any sequelae of acute or chronic hepatitis.
Six patients (3.9 per cent) underwent abdominal ultrasound as in-patients at the initial presentation. The reasons stated for this were deranged or worsening liver function in five patients and clinical splenomegaly in one patient. The following findings were recorded: splenomegaly in five of six patients and a normal liver in all patients. One patient underwent a computed tomography scan as alternative imaging, which showed splenomegaly. Two of these patients underwent repeat ultrasound scanning at follow up in the community because of left upper quadrant abdominal pain and worsening liver function test results; the scan findings were normal.
Discussion
This study evaluated the utility of performing liver function tests in adult patients with a diagnosis of infectious mononucleosis. Our patient population represented relatively young immunocompetent adults; this is the typical population of patients admitted to ENT with infectious mononucleosis. The main reason for hospital admission to ENT in infectious mononucleosis cases is for supportive care (analgesia and intravenous hydration) for pharyngitis and tonsillitis.
The monospot test is generally performed in suspected infectious mononucleosis cases; it has an accuracy of 71–90 per cent.Reference Womack and Jimenez5 The ‘gold standard’ test for acute infection is for antibodies to the Epstein–Barr virus (EBV) viral capsid antigen; however, this is not routinely performed in the UK in typical cases. A positive monospot test result and/or a typical clinical presentation were considered to be diagnostic. In our population, 144 of 153 patients (94.1 per cent) had a positive monospot test result or presence of IgM to the EBV viral capsid antigen on presentation or on a later repeat test. In the case of negative antibodies to the EBV viral capsid antigen, other viruses such as CMV may be the cause.Reference Womack and Jimenez5 Infectious mononucleosis was diagnosed in a small proportion of patients (7 of 153, 4.6 per cent) based on typical clinical features and/or full blood count results.
There is no clear guidance on the utility of liver function tests in infectious mononucleosis. The literature on this topic consists mainly of older studies, and, to our knowledge, no study has evaluated the utility of performing sequential liver function tests in patients with infectious mononucleosis. The National Institute for Health and Care Excellence clinical knowledge summary mentions that clinicians should consider checking liver function test results at initial presentation. The recommendations for this clinical knowledge summary were based on expert opinions.1
We found that up to 80 per cent of patients had an elevated liver enzyme(s) at initial presentation, and a smaller proportion (11.7 per cent) of patients had slightly raised total serum bilirubin at presentation. This is in keeping with other reports evaluating liver function test results in patients hospitalised with infectious mononucleosis. One Chinese study evaluated 287 patients admitted with a diagnosis of infectious mononucleosis; they reported elevated transaminases and total bilirubin in 74 per cent and 12.6 per cent of patients, respectively.Reference Wang, Li, Ren and Zhao6 It is generally accepted that the time of resolution of abnormal liver function in patients with infectious mononucleosis is around three to four weeks.Reference Kofteridis, Koulentaki, Valachis, Christofaki, Mazokopakis and Papazoglou7,Reference Rea, Russo, Katon, Ashley and Buchwald8 This is in keeping with our population; we found a median time to resolution of 4.5 weeks. However, this is variable, with a third quartile of seven weeks, and a minority of patients with persistent elevation for over six months. Others have also found that abnormal liver function test results can persist for over six months from initial presentation.Reference Rea, Russo, Katon, Ashley and Buchwald8
Epstein–Barr virus as a cause of acute liver failure in infectious mononucleosis is rare. One US study evaluated the role of EBV in acute liver failure. In a sample of 1887 adults with acute liver failure, 4 cases (0.21 per cent) were considered to be EBV related, and in only 1 case was EBV considered to be the definitive cause. In addition, half of these cases did not present with typical clinical features of infectious mononucleosis.Reference Mellinger, Rossaro and Naugler9 Chronic hepatitis in infectious mononucleosis is rare.Reference Schechter and Lamps10 There are a lack of data predicting the occurrence of this in patients with infectious mononucleosis. Patients who show clinical signs of acute liver failure, including jaundice, would need specialist evaluation.
Anecdotally, and in our experience, some ENT units will perform an abdominal ultrasound in the presence of elevated liver enzymes. We found that six patients in our unit underwent abdominal ultrasound to further evaluate abnormal liver enzymes and splenomegaly. As expected, most cases showed splenomegaly. In addition, all patients had a normal biliary tree and liver. One study performed serial abdominal ultrasound to examine the spleen and liver in 29 patients admitted to ENT with infectious mononucleosis.Reference Dommerby, Stangerup, Stangerup and Hancke11 They found that all patients had an enlarged spleen and 50 per cent had an enlarged liver.
Although only a small proportion of our patients underwent abdominal ultrasound, our experience suggests that routine abdominal ultrasound is not required to evaluate abnormal liver enzymes in the context of infectious mononucleosis.
We also evaluated time to resolution of deranged liver enzymes, as patients are often subjected to multiple blood tests at varying intervals post discharge. The analysis of time to resolution was limited, as there was no routine follow-up assessment in patients with abnormal liver function test results at presentation, and measurements were performed at varying intervals. We found that liver enzymes returned to normal at a median (interquartile range) time of 32 days (20–50 days). However, this was highly variable, and enzymes can take months to return to normal.
No patient had any sequelae of acute or chronic hepatitis. These findings suggest that serial evaluation of deranged liver enzymes following a diagnosis of infectious mononucleosis, in the absence of clinical concern and in the immunocompetent adult, is not required. This would avoid the need for multiple consultations and blood tests following discharge. Our findings also question the need for routine assessment of liver function tests in the acute presentation of infectious mononucleosis in immunocompetent adults with no clinical features of liver disease. However, clinicians may still consider sequential testing in patients who are deemed ‘high risk’ for developing acute hepatic failure (immunosuppressed, previous liver transplant or human immunodeficiency virus positive patients) or in those who show clinical signs (including jaundice, abdominal pain or ascites).Reference Wang, Li, Ren and Zhao6
• Infectious mononucleosis is a relatively common self-limiting condition typically affecting young adults
• Derangement of liver enzymes is an expected feature and usually subclinical
• Time to resolution of deranged liver enzymes varies widely
• No complication of acute or chronic hepatitis was found in our population
• Findings suggest serial assessment of liver enzymes in the community is not required
There are limitations to this study. A small proportion of our population was diagnosed on the basis of typical clinical features only. The retrospective nature of this study limited standardised assessment of liver function on admission and follow up in patients with elevated enzymes. We estimated the time to resolution of elevated liver enzymes; however, this assessment was limited by incomplete assessment of liver function in patients with abnormal test results and the varying intervals of assessment. There is scope for a well-designed prospective study to further characterise the derangement of liver enzymes and time to resolution.
Conclusion
Derangement of liver enzymes is an expected self-limiting feature of infectious mononucleosis. Our findings suggest that serial assessment of liver function is not required in immunocompetent adults with subclinical derangement in liver enzymes.
Competing interests
None declared