



Introduction
Delirium is a complex neuropsychiatric syndrome, which is more common in older hospitalised adults. The Diagnostic and Statistical Manual on Mental Disorders, Fifth Edition (DSM-5) defines delirium as an acute and/or fluctuating change in awareness, arousal and other cognitive deficits due to physical illness or drugs (American Psychiatric Association, 2013). Approximately, 50% of patients also experience hallucinations or delusions (Tieges et al. Reference Tieges, Evans, Neufeld and MacLullich2018). Clinically, delirium occurs in hyperactive, hypoactive or mixed forms, based on psychomotor behaviour (Grover et al. Reference Grover, Sharma, Aggarwal, Mattoo, Chakrabarti and Malhotra2014). Hypoactive subtype, featuring predominantly motor retardation, is the most common presentation among older adults with delirium in acute and rehabilitative wards (Bellelli et al. Reference Bellelli, Morandi, Di Santo, Mazzone, Cherubini and Mossello2016). In the majority of cases, the duration of an episode of delirium is short, and over in a number of days, but in approximately 20% of cases, it can persist for weeks or months (Cole, Reference Cole2010).
The reported prevalence of delirium in hospitalised older medical patients in general medical and geriatric wards varies from 18% to 35% depending on the population studied, study inclusion criteria and methods used for screening for delirium (Inouye et al. Reference Inouye, Westendorp and Saczynski2014). The first hospital-wide point-prevalence study of delirium in a large Irish general hospital setting in 2013 found approximately 19.6% of 280 adult inpatients screened had delirium (Ryan et al. Reference Ryan, O’Regan, Caoimh, Clare, O’Connor and Leonard2013). A more recent multicentre study in the UK including general medical inpatients aged over 65 (n = 1507) found that the point prevalence of delirium was lower at 14.7% (Geriatric Medicine Research Collaborative, 2019).
Other work has highlighted that older persons with dementia and frailty are a particularly high-risk group for delirium (Timmons et al. Reference Timmons, Manning, Barrett, Brady, Browne and O’Shea2015) with comorbid dementia found in approximately 50% of older delirious patients (Ryan et al. Reference Ryan, O’Regan, Caoimh, Clare, O’Connor and Leonard2013).
Delirium is associated with adverse outcomes including increased mortality, more prolonged admission duration and a higher risk of subsequently requiring long-term supported care (Pendlebury et al. Reference Pendlebury, Lovett, Smith, Dutta, Bendon and Lloyd-Lavery2015; Zhang et al. Reference Zhang, Pan and Ni2013; Gleason et al. Reference Gleason, Schmitt, Kosar, Tabloski, Saczynski and Robinson2015), particularly in those with delirium superimposed on dementia (Morandi et al. Reference Morandi, Davis, Fick, Turco, Boustani and Lucchi2014). Delirium is also associated with a doubling of the rate of progression of cognitive decline (Fong et al. Reference Fong, Jones, Shi, Marcantonio, Yap and Rudolph2009) and is associated with significant patient and carer distress (Partridge et al. Reference Partridge, Martin, Harari and Dhesi2013). Gonzalez et al. (Reference González, Martínez, Calderón, Villarroel, Yuri and Rojas2009) found an increase in mortality of 11% for every additional 48 hours of active delirium in older medical inpatients (González et al. Reference González, Martínez, Calderón, Villarroel, Yuri and Rojas2009).
Despite its frequency and negative impact upon healthcare outcomes, delirium is under-recognised clinically with between one-third and two-thirds of delirium cases going unrecognised (O’Hanlon et al. Reference O’Hanlon, O’Regan and Maclullich2014). This under-recognition has been associated with factors such as the fluctuating course of delirium, the less compelling nature of hypoactive presentations, its overlap with dementia and depression, lack of formal cognitive assessment in hospital settings and underappreciation of clinical consequences (Philpot, Reference Philpot2010; O’Hanlon et al. Reference O’Hanlon, O’Regan and Maclullich2014).
Given that delirium can be prevented in about one-third of patients at risk it is important to identify those most at risk in the hospital setting with proactive screening for possible precipitating factors for delirium early in admission (Marcantonio Reference Marcantonio2017). National Institute for Health and Care Excellence guidelines (2019) recommend that all patients aged 65 and over are screened for delirium upon hospital admission. The National Institute for Health and Care Excellence guidelines also recommend daily monitoring for changes in behaviour possibly indicative of delirium for those at risk with pre-existing cognitive impairment, current hip fracture and severe illness considered additional risk factors to age. Risk Reduction and Management of Delirium guidelines from the Scottish Intercollegiate Guideline Network (2019) also emphasise the importance of serial delirium screening given the fluctuating nature of the condition.
This is the first delirium prevalence study in an older hospitalised population in the north-west of Ireland focussing on delirium occurrence through the use of serial delirium screening. This prospective cohort study intended to identify the occurrence of delirium among older adults admitted to general medical wards in a hospital setting in the north-west of Ireland by measuring delirium prevalence and incidence rates. By using delirium screening on admission and serial screening during hospital stay, we examined the burden of delirium in an older population admitted to general medical wards. We also aimed to capture patient and hospital factors predictive of delirium that may influence patient groups targeted for early intervention.
Aims
The primary aims of this study were: (i) to assess delirium prevalence on admission and incidence during admission in a cohort of older medical inpatients and (ii) to compare delirious with non-delirious groups according to underlying risk factors including age, gender, pre-existing dementia, score on cognitive testing, functional disability and severity of physical illness at baseline.
Methods
Study design and setting
This prospective cohort study was conducted in Sligo University Hospital, a regional specialist referral centre and acute general hospital, with approximately 300 acute inpatient beds, over a 4-month period (from March to June 2015).
Inclusion/exclusion criteria
All patients aged 70 years and over, admitted to medical wards and still hospitalised when approached to take part in the study within 72 hours of their admission, were eligible to be included in the study. Exclusion criteria were patients admitted with severe aphasia, who were intubated, who had severe sensory problems, who were in a terminal phase of illness or were unable to speak English. Patients admitted to wards other than general medical wards, including intensive care units (ICU), were also excluded.
Patients who were admitted twice within the study period were included only in respect of their first admission.
Screening and assessment
All eligible and consenting patients had an assessment at the first recruitment day undertaken at baseline by a specialist mental health nurse which included the following measures.
Delirium assessment
The Revised Delirium Rating Scale (DRS-R-98) (Trzepacz et al. Reference Trzepacz, Mittal, Torres, Kanary, Norton and Jimerson2001) was used to document delirium presence and severity. DRS-R-98 incorporates 16 clinician-rated items (13 for severity and 3 for diagnosis) for the preceding 24 hours. It differentiates delirium from dementia, depression and schizophrenia (Adamis et al. Reference Adamis, Sharma, Whelan and Macdonald2010) with sensitivity ranging from 91% and 100% (depending on the cut-off score chosen) and it has both good interrater reliability and internal consistency (Adamis et al. Reference Adamis, Sharma, Whelan and Macdonald2010). The severity scale score ranges from 0 to 39 with higher scores indicating more severe delirium and a score of 16 or more is compatible with the diagnosis of delirium (Trzepacz et al. Reference Trzepacz, Mittal, Torres, Kanary, Norton and Jimerson2001). Administration typically takes 15–20 minutes. In this study, a participant was defined as having delirium if they were rated as 16 and above using the DRS-R-98.
Cognition
Montreal Cognitive Assessment (MoCA) (Nasreddine et al. Reference Nasreddine, Phillips, Bédirian, Charbonneau, Whitehead and Collin2005) was used to assess general cognition. The MoCA assesses multiple cognitive domains including attention, concentration, executive functions, memory, language, visuospatial skills, abstraction, calculation and orientation. MoCA is scored on a 30-point scale and higher scores indicate better cognitive performance. Administration typically takes about 12–15 minutes. In this study, if patients could not complete sections (e.g. due to visual impairment) MoCA was standardized to give a maximum score of 30.
Severity of physical illness
The Acute Physiology and Chronic Health Evaluation II (APACHE II) (Knaus et al. Reference Knaus, Draper, Wagner and Zimmerman1985) was used to measure the severity of physical illness.
APACHE II is a popular means of measuring the severity of illness in delirium research and takes into account age, chronic illness and acute physiological disturbance (APS). Scores range from 0 to 71, with higher scores closely correlated with subsequent risk of hospital death (Minne et al. Reference Minne, Abu-Hanna and de Jonge2008). The APS subscale has 11 items and each one can be scored from 0 to 4 (4 is the worst).
Physical function (activities of daily living)
Barthel Index (Collin et al. Reference Collin, Wade, Davies and Horne1988) was used to measure activities of daily living (ADL) representing functional disability. The Barthel Index has 10 items, with total scores ranging from 0 to 20. A score of 0 indicates total disability and dependency, while 20 suggests normal ADL.
Diagnosis of previous history of dementia
Short Informant Questionnaire on Cognitive Decline (IQCODE) (Jorm, Reference Jorm1994) was used to diagnose pre-existing dementia. IQCODE uses collateral information through a structured interview with an informant who knows the patient well, to assess changes in cognition and everyday functions over the previous 10-year period. Evaluation is not affected by the patient’s pre-morbid intelligence or education (Park, Reference Park2017). A cut-off point of ≥3.5 was used to diagnosis pre-morbid dementia (Jorm, Reference Jorm1994).
Delirium presence and severity, general cognition and the severity of physical illness were serially assessed by the same assessor across the entire hospital stay at intervals of every 3 (±1) days if patients remained in the hospital. A final assessment was completed on the day prior to discharge if the discharge date known. For those with a hospital stay longer than 16 days, a final assessment was undertaken on the 28th day. The maximum possible number of assessments was eight per participant. At initial and final assessments, the Barthel Index (Collin et al. Reference Collin, Wade, Davies and Horne1988) was administered to determine physical functioning status.
Cases with pre-existing dementia were identified if a clear history of a documented DSM-V diagnosis of dementia was recorded in the medical notes. If this was absent, pre-morbid dementia was assessed by telephone interview using the IQCODE (Jorm, Reference Jorm1994).
Demographic information gathered from the participant’s medical case notes and the hospital computerised database included gender, age and medical diagnoses. The methodology has been described in more detail in a previous report (Williams et al. Reference Williams, Finn, Melvin, Meagher, McCarthy and Adamis2017).
Statistical analysis
All data were coded and entered into IBM Statistical Package for Social Science v24 (IBM Corp, 2016) software package for windows. Nominal variables were presented as counts and percentages and continuous variables were reported using the mean, median and standard deviation (s.d.). The differences between groups (delirium, no delirium) were assessed using χ 2 tests for categorical variables and the Mann–Whitney U test for continuous variables. In this study, a participant was defined as having delirium if they scored 16 and above using the DRS-R-98 severity scale and presence of delirium yes or no was recorded as a categorical variable. The association of demographic and clinical factors with delirium while controlling for confounder variables was evaluated using a regression model conducted by the Backward Stepwise (Wald) method. In this model, the dependent variable was the binary variable delirium (presence of delirium yes or no) including prevalent and incident cases and predictor variables were age, gender, presence of pre-existing dementia, scores of MoCA, APACHE-II, APS and Barthel Index at initial assessment.
Ethical approval
Informed consent was obtained using a previously published method (Adamis et al. Reference Adamis, Martin, Treloar and Macdonald2005). If a patient lacked capacity or had fluctuating capacity and a relative was not available for assent but the patient was willing to take part in the study, he/she was enrolled in the study and when they regained capacity he/she was asked again for informed consent, or a relative was asked to assent on the patient’s behalf. The study was approved by the Sligo University Hospital Research Ethics Committee. Data were anonymised prior to entry and analysis.
Results
Descriptive statistics
Over a 4-month recruitment period, 235 inpatients were invited to participate. After excluding patients who declined to partake (n = 24), or those who did not meet inclusion criteria (n = 13), 198 inpatients were included (see Fig. 1).
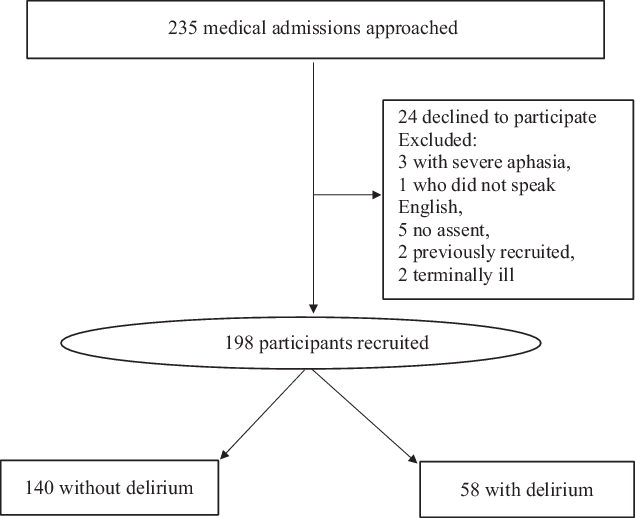
Figure 1. Participant recruitment and delirium detection.
The number of participants at each assessment was as follows: 1st assessment, n = 198; 2nd assessment, n = 152; 3rd assessment, n = 101; 4th assessment, n = 66; 5th assessment, n = 52; 6th assessment, n = 32; 7th assessment, n = 23; 8th assessment, n = 12. A total of 636 assessments were undertaken with 198 participants.
Of 198 recruited, 92 (46.5%) were women. Mean age was 80.6 years (s.d. 6.81; range 70–97). Clinical variables of the study population and descriptive statistics at initial assessment are outlined in Table 1.
Table 1. Clinical variables of the study population and descriptive statistics: initial assessment

s.d., Standard Deviation; APACHE II, Acute Physiology and Chronic Health Evaluation II; MoCA, Montreal Cognitive Assessment.
a Chi-Square Test.
b Mann–Whitney U Test.
Delirium occurrence
Using the DRS-R98 with a severity cut-off of ≥16, 35 participants (17.7%) were identified as prevalent (present on admission) delirium cases and a further 23 (11.6%) as incident (new-onset) delirium cases. The overall delirium occurrence rate was 29.3% (n = 58).
Delirium and medical diagnoses
In those with delirium the most frequent diagnoses documented in inpatient discharge summaries were respiratory infection (n = 17, 29.3%), urinary tract infection (UTI) (n = 13, 22.4%), chronic obstructive airways disease (COPD) (n = 6, 10.3%), stroke (n = 4, 6.9%) and constipation (n = 2, 3.4%).
Pre-existing dementia
The IQCODE (Jorm, Reference Jorm1994) was performed by telephone interview with relatives of 140 participants as a clear history of a documented DSM-V diagnosis of dementia was not recorded in the medical notes of these participants.
Combining the results of the review of participant’s clinical notes and IQCODE, 86 (43.4%) participants had pre-existing dementia. Of those identified as delirious with the DRS-R98, 39 (67.2%) had pre-existing dementia.
Demographic and clinical factors associated with delirium
Bivariate statistics
We compared those with delirium (prevalent or incident) with those who did not have delirium during hospitalisation in terms of demographic variables (age, gender) and clinical variables (pre-existing dementia, and initial scores of MoCA, APACHE-II, APS subscore of APACHE-II and Barthel Index) using Chi-Square Test for the categorical variables and Mann–Whitney for continuous variables.
There were no differences in terms of gender between those with delirium and those without delirium (x 2 = 0.001, df: p = 0.987). Participants with pre-existing dementia were significantly more likely to develop delirium during the hospitalisation (x 2 = 18.592, df: 1, p < 0.0001).
Table 2 shows a comparison of initial scores on MoCA, APACHE-II, APS and Barthel Index in the group who developed delirium (n = 58) versus those who did not (n = 140) during hospitalisation. Those with delirium had significantly worse scores in cognition, functional ability, APS and were older compared to those without delirium. No differences were found in the total APACHE-II scores between the two groups.
Table 2. Comparison of the continuous variables at initial assessment between those who developed delirium during hospitalisation and those who did not

APACHE II, Acute Physiology and Chronic Health Evaluation II; MoCA, Montreal Cognitive Assessment; APS, Acute Physiological Disturbance Subscore of APACHE-II; IQR, InterQuartile Range; s.d., Standard Deviation.
Regression analysis
Finally, to control for confounding variables, we conducted a binary logistic analysis with the dependent variable as delirium or not, and independent variables gender, age, pre-existing dementia and the initial scores on the following measures; MoCA, APACHE-II, APS and Barthel Index. The final parsimonious model is shown in Table 3.
Table 3. Significant predictors for delirium during hospitalisation after controlling for confounding factors

As outlined in Table 3 older age, impaired cognition and lower functional ability at admission are associated with a significant likelihood of delirium. Neither pre-existing dementia nor severity of physical illness was associated with a significant likelihood of delirium.
Discussion
This study assessed the occurrence of delirium among older adults admitted to acute medical wards in an Irish hospital by combining the prevalence and incidence rates of delirium. Our results indicate a high burden of delirium in this population with an overall occurrence rate in almost one-third of older medical inpatients.
Our delirium occurrence rate (29.3%) is comparable to that found in a 2014 review of international studies estimating the overall occurrence rates of delirium in older populations on general medical and geriatric wards to range from 29% and 64% (Inouye et al. Reference Inouye, Westendorp and Saczynski2014). The prevalence rate of delirium in our study, 17.7% is marginally lower than the prevalence range of 18% and35% found in this 2014 review but our incidence rate 11.6% falls within the incidence range reported by authors (11% and 14%) (Inouye et al. Reference Inouye, Westendorp and Saczynski2014).
Variation in delirium occurrence in the literature may be influenced by individual admission thresholds of the hospital where the study is conducted, as well as due to varying methodology in included studies, including differing delirium criteria and scales used (Laurila et al. Reference Laurila, Pitkala, Strandberg and Tilvis2003; Davis et al. Reference Davis, Kreisel, Muniz Terrera, Hall, Morandi and Boustani2013, Reference Dyer, Briggs, Nabeel, O’Neill and Kennelly2016a). Comparing these results to previous Irish studies, our delirium prevalence rate is lower than the prevalence rate of 20.7% found in a study among Irish adult inpatients screened using DRS-R98 (Ryan et al. Reference Ryan, O’Regan, Caoimh, Clare, O’Connor and Leonard2013). The higher delirium prevalence found in this 2010 study may be partly explained by the different cut-off score for the diagnosis of delirium of ≥12 on DRS-R98 used in that study, compared to the more stringent cut-off of score of ≥16 used in our study. Despite the variation in the literature, our findings emphasise the importance of delirium detection and implementation of delirium care pathways to improve clinical outcomes in older hospitalised patients.
This prospective cohort study also identified associations of delirium, by comparing personal and clinical characteristics, between the group with delirium and the group without.
Independent risk factors for delirium found in regression analysis in our study included older age, impaired cognition and lower functional ability at admission and findings are supported in the delirium literature (Ahmed et al. Reference Ahmed, Leurent and Sampson2014).
Among our total study group, two-fifths had pre-existing dementia and in those with delirium, almost two-thirds had pre-existing dementia. These findings indicate a high prevalence of pre-existing dementia in our cohort of older adults admitted to the acute hospital setting, which is higher again in those with delirium. Our results are supported by a clear association between dementia and delirium in the literature. A multihospital study in Ireland found over half of admitted older patients with dementia had superimposed delirium (Timmons et al. Reference Timmons, Manning, Barrett, Brady, Browne and O’Shea2015). However, a 2017 dementia prevalence study found that approximately one-third of 190 older hospitalised Irish adults had dementia (Briggs et al. Reference Briggs, Dyer, Nabeel, Collins, Doherty, Coughlan, O’Neill and Kennelly2017). Establishing dementia prevalence was not a primary aim of our study and as such our methodology, including cognitive impairment assessment measure, differed from those used by Briggs et al. (Briggs et al. Reference Briggs, Dyer, Nabeel, Collins, Doherty, Coughlan, O’Neill and Kennelly2017) and contributed to discrepancies in dementia prevalence figures between studies.
Our figure of over two-thirds with delirium superimposed on dementia is higher than in an earlier delirium point prevalence study in an acute Irish hospital setting where approximately half the study group with delirium had pre-existing cognitive impairment (Ryan et al. Reference Ryan, O’Regan, Caoimh, Clare, O’Connor and Leonard2013). Again, methodological differences between studies may contribute to discrepancies in findings.
However, an association between cognitive impairment and a higher risk of delirium (Timmons et al. Reference Timmons, Manning, Barrett, Brady, Browne and O’Shea2015) highlights the importance of including a baseline formal cognitive screening test in the assessment of older hospitalised adults with suspected cognitive dysfunction in order to identify individuals at higher risk for delirium.
The initial severity of physical illness measured using APACHE-II did not have a significant association with delirium in our study, although those with delirium had significantly worse scores in the APS section of APACHE-II compared to those without delirium. In addition to the APS subcomponent, the APACHE-II measure used in our study includes age and chronic illness burden. It has been used widely in delirium studies although it is mainly designed to predict mortality in ICU.
Patient groups in intensive care, palliative or cancer care settings were not included in our study, or were those in the terminal phase of illness or those with severe symptoms of stroke. Perhaps if these patient groups, often with a higher chronic illness burden and more severe clinical parameters, were included in our study results may have shown an association between severity of physical illness and delirium occurrence.
However, our study findings correspond to findings of previous research conducted by this research group (Williams et al. Reference Williams, Finn, Melvin, Meagher, McCarthy and Adamis2017) supporting the notion that low brain reserve, characterised by a higher level of neuropathology, is more likely to be involved in delirium rather than the severity of the physical illness (Jones et al. Reference Jones, Fong, Metzger, Tulebaev, Yang and Alsop2010).
Functional impairment, identified in our study as an independent delirium risk factor, is also recognised in the literature and has been estimated to increase the risk of delirium four-fold among patients on general medical wards (Inouye et al. Reference Inouye, Westendorp and Saczynski2014).
Overall, our findings suggest those older hospitalised patients with worse functional status and dementia on admission are target groups for an enhanced delirium prevention focus. This group is in need of more stringent monitoring for changes in behaviour possibly indicative of delirium during hospital admission.
Additionally, our study found the most frequent diagnoses documented in inpatient discharge summaries of those with delirium were respiratory infection, followed by UTI. This result is supported by other study findings that UTI or pneumonia may be present in up to two-thirds of hospitalised patients with delirium (Vasilevskis et al. Reference Vasilevskis, Han, Hughes and Ely2012). Our findings suggest the need for a lower threshold of suspicion among clinical staff for delirium in these patient groups who require enhanced delirium prevention and screening strategies within the acute hospital setting.
Implications of the study
This study highlights the considerable burden of delirium in older medical inpatients. This is especially relevant in the context of an ageing population as delirium rates are anticipated to rise in parallel with the predicted increased prevalence of pre-existing dementia. This makes delirium, associated with serious morbidity and mortality in older adults, an important focus for the development and implementation of formal screening and preventative care pathways. Given that delirium is under-recognised, healthcare staff who regularly encounter older medical patients with complex co-morbidities require delirium focussed education to promote awareness and accurate diagnosis of delirium (El Hussein et al. Reference El Hussein, Hirst and Salyers2015). Improving awareness of delirium among healthcare professionals is important. Promotion of delirium prevention is also key to effectively improving prevention, screening and management of delirium as part of formal delirium clinical pathways in acute hospital settings (Tauro, Reference Tauro2014). This has been helped in Ireland by the recent inclusion of guidance for healthcare staff on the identification and management of delirium in the Emergency Department/Acute Medical Assessment Unit as part of the National Clinical Programme for Older People in Ireland (Delirium ED/AMAU algorithm, HSE, 2017).
Strengths and limitations
There are several notable strengths and limitations of this study.
Over 24 delirium instruments have been used in published studies (Inouye et al. Reference Inouye, Westendorp and Saczynski2014) and it is acknowledged that too inclusive or restrictive criteria can cause marked differences in reported prevalence rates of delirium (Kean & Ryan, Reference Kean and Ryan2008). Furthermore, delirium characteristically fluctuates in its course, which makes it difficult to identify using a single assessment. Repeating assessments, as we did in this study increases the opportunity for detection of deficits, as well as eliciting fluctuation and is important given the associated increased risk of mortality and adverse outcomes (Davis et al. Reference Davis, Kreisel, Muniz Terrera, Hall, Morandi and Boustani2013). The DRS-R-98 measure used in this study is a comprehensive instrument useful for delirium diagnosis and severity rating and is sensitive to change and hence can be used for monitoring patients over a period, making it suited to detecting incidence of delirium during admission (Grover & Kate, Reference Grover and Kate2012). However, our methodology excluded the possibility of examining delirium duration because of the time frame of the assessments.
We acknowledge the possibility that we may have underestimated the prevalence of delirium through the use of our exclusion criteria. However, it is unlikely given the population of non-English speaking individuals aged over 70 in the catchment area of Sligo University Hospital (SUH) is not large. Also, those with pre-existing severe aphasia are more likely to be on specialist wards under the care of neurologists rather than in acute medical wards. Exclusion criteria may have also impacted on the associations found between severity of physical illness and delirium prevalence.
There are also recognised challenges associated with assessing capacity to consent to partake in delirium research. Strict assessment of capacity leads to exclusion of people with more severe delirium and produces biased and unethical results (Adamis et al. Reference Adamis, Sharma, Whelan and Macdonald2010). We followed guidance provided by the World Medical Association Declaration of Helsinki, 2001 for this study: ‘Research on individuals from whom it is not possible to obtain consent, including proxy or advance consent, should be done only if the physical/mental condition that prevents obtaining informed consent is a necessary characteristic of the research population’ (World Medical Association Declaration of Helsinki, 2001). In accordance, modifications to the informed consent process are required in research with delirious patients to decrease the likelihood of ultimately obtaining invalid and thus unethical results through the exclusion of patients who lack capacity or a proxy (Sweet et al. Reference Sweet, Adamis, Meagher, Davis, Currow, Bush, Barnes, Hartwick, Agar, Simon, Breitbart, MacDonald and Lawlor2014).
Challenges also exist with delayed verification dementia research (Christie, Reference Christie2018). However, the utility of the informant history, an integral part of the IQCODE, is well recognised. In this study, we used telephone interviews to address inherent difficulties with this method, which include the availability of an informant to provide a history (Dyer et al. Reference Dyer, Nabeel, Briggs, O’Neill and Kennelly2016b) (Briggs & O’Neill, Reference Briggs and O’Neill2016).
Given our study population was drawn from a single hospital in the north-west of Ireland, caution should be used in generalising these results to other populations. However, the rates of delirium reported here are in line with previously published studies of delirium. Further longitudinal research across multi-site hospital and community settings may address the above study limitation.
Conclusion
Delirium is a common problem in hospitalised populations as demonstrated robustly in this study and as a medical emergency, warrants screening in high-risk groups on admission. Our findings support the use of formal delirium clinical pathways in the acute hospital setting. Such pathways should include delirium assessment in older adults on admission and consideration of serial screening during admission in high-risk populations, including those with cognitive impairment, dementia and poor functional status. Staff training in delirium screening, prevention and multifactorial interventions with a focus on at-risk groups may contribute to timely and optimal management of individuals with delirium and a decrease in delirium occurrence during admission. Our study did not explore the use of delirium management strategies and outcomes. Given the high burden of delirium found in our study population, future studies may add to the delirium literature by including a focus on delirium treatment in older adult inpatients.
Conflict of interest
The authors have no conflict of interest to disclose.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committee on human experimentation with the Helsinki Declaration of 1975, as revised in 2008.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.




