



Healthcare-associated infections (HAIs) affect millions of patients worldwide annually and represent a major challenge to patient care within hospitals. Reference Pittet and Donaldson1 The World Health Organization (WHO) estimates that ∼1.7 million patients are affected by HAIs in the United States and 4 million in Europe every year. 2 HAIs affect patient outcomes by increasing mortality, promoting antimicrobial resistance and increasing healthcare-associated costs. Reference Pittet and Donaldson1,Reference Price, MacDonald and Melone3 The burden of HAI is even higher in low- and middle-income countries, representing a greater epidemiological problem than in high-income countries. Reference Allegranzi, Nejad and Combescure4 The pooled prevalence of HAI in resource-limited settings (∼15.5 per 100 patients) is 2–3 times higher than the rates observed in Europe and the United States. These infections also determine a marked economic impact at the societal level. Reference Price, MacDonald and Melone3,Reference Allegranzi, Nejad and Combescure4
Infection prevention and control (IPC) programs are a key strategy in preventing HAIs and containing antimicrobial resistance in hospitals. Reference Pittet and Donaldson1–Reference Price, MacDonald and Melone3 Adequate conditions for the development and implementation of IPC programs have been considered a key parameter of the quality of healthcare services. Reference Pittet and Donaldson1–Reference Price, MacDonald and Melone3,Reference Storr, Twyman and Zingg5 The insufficiency of these conditions has been a challenge for low- and middle-income countries, resulting in the aforementioned consequences of high HAI rates. Reference Price, MacDonald and Melone3,Reference Allegranzi, Nejad and Combescure4 Evidence-based guidance for national IPC programs is needed to support national and global capacity building for the reduction of HAI and antimicrobial resistance. Reference Pittet and Donaldson1,Reference Price, MacDonald and Melone3,Reference Storr, Twyman and Zingg5
In 2018, the WHO launched the IPC Assessment Framework (IPCAF) with 8 core components, with the main objective of providing an orientation to assess the situation of IPC at the individual healthcare facility level and to monitor the development and improvement of IPC activities over time. 6 The components are as follows: IPC program; IPC guidelines; IPC education and training; HAI surveillance; multimodal strategies for implementation of IPC interventions; monitoring and audit of IPC practices and feedback; workload, staffing, and bed occupancy; and built environment, materials, and equipment for IPC at the facility level. 6
In the last decade, several studies have evaluated IPC programs worldwide, and virtually all from high-income countries. Reference Price, MacDonald and Melone3,Reference Stone, Pogorzelska-Maziarz and Herzig7–Reference Jeong, Joo, Bahk, Koo, Lee and Kim17 The results of countrywide surveys of IPC programs are relevant nationally to drive public health policies and internationally to identify global inequalities in both quality and implementation processes of IPC programs among countries. Reference Tartari, Tomczyk and Pires18 These surveys are also important because they contribute to continued awareness of the importance of IPC and alert participants and policy makers to review gaps and priorities for action, allowing them to set targets to improve national IPC programs. Reference Tartari, Tomczyk and Pires18
Brazil is a country of continental dimensions with a population of >215 million. 19 IPC program content and implementation are an attribution of infection control committees (ICCs), whose existence in Brazil has been mandatory by law since 1997, 20 whereas the management of IPC programs at the federal level has been assigned to the Brazilian Health Regulatory Agency (ANVISA for short, in Portuguese). 21 Although some studies have evaluated IPC programs in Brazil, they have usually been restricted to a single city or state. Reference Padoveze, Fortaleza and Kiffer11,Reference Menegueti and Laus22–Reference Santos, Padoveze and Lacerda24 Owing to the high heterogeneity of the economic, social, and healthcare structure in Brazil, Padoveze et al Reference Padoveze and Fortaleza25 highlighted the fragility of IPC and ICC quality assessments in the country and the urgent need to overcome this limitation. Only 1 has study assessed the structures for prevention of HAI in Brazilian hospitals, and it was conducted between 2011 and 2013. Reference Padoveze, Fortaleza and Kiffer11 Since then, however, several global and national actions have been implemented to increase awareness of HAI and to promote improvements in IPC programs. In this study, we assessed IPC programs and ICCs from Brazil, including hospitals from all 5 regions of the country, after the implementation of national and international actions to increase awareness of HAI.
Methods
Study design and data collection
We conducted a cross-sectional study in Brazilian public and private hospitals from October 2019 to December 2020. The ICCs included in this study were those from hospitals participating in the Impact of Infections by Antimicrobial-Resistant Microorganisms in Patients Admitted to Adult Intensive Care Units in Brazil: Platform of Projects to Support the National Action Plan for the Prevention and Control of Antimicrobial Resistance (IMPACTO-MR) program. This multicenter, countrywide platform is supported by the Brazilian Ministry of Health and was created to develop studies related to HAIs and antimicrobial resistance. 26 The centers were selected by convenience sampling ensuring they encompass all 5 Brazilian federative regions.
The questionnaire used in this study, containing the IPC program elements and specific structural characteristics of the hospital, was developed and adapted from the ANVISA guidelines for completing the assessment of patient safety practices. 27 The questionnaire shares similarities with most of the variables in each WHO IPCAF core component (Supplementary Material), and for this reason, no scoring system was used.
The data collection process started with an online questionnaire sent to the professional in charge of the ICC in all institutions, to be answered using the REDCap platform. Once completed, a team of 2–3 investigators conducted an on-site visit to the participating institutions to check documents and validate the answers received online. The audit visit focused on the documents, processes, and structures that were reported on the questionnaire. In addition, we collected monthly epidemiological data through a standardized form sent to the ICC for information on adherence to the guidelines for HAI prevention.
Statistical analysis
In the study, we used descriptive analysis. Categorical variables (yes or available) were presented as proportions, and continuous variables have been presented as means (SD) or medians (IQR) according to their distribution. Comparisons between Brazilian federative regions were performed using frequency analysis, cross tabulation, and χ 2 test for categorical variables and the Kruskal-Wallis test for continuous variables, assuming the statistical significance of P < .05. The analyses were performed in R version 4.0.2 software (R Foundation for Statistical Computing, Vienna, Austria). 28
Ethics
The research was conducted in accordance with the ethical and legal principles contained in Resolution No. 466/2012 of the Brazilian National Health Council and was approved by the Research Ethics Committee of Hospital Moinhos de Vento (coordinating center) and the hospitals that participate in the IMPACTO-MR program (no. 3.385.438 and CAAE no. 02139418.3.2003.5330) (Supplementary Material).
Results
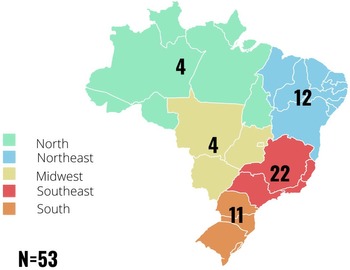
In total, 53 hospitals randomly distributed across the country were evaluated through their respective ICCs (Fig. 1). All included hospitals had the following features: an ICC, at least 6 intensive care unit (ICU) beds, and access to a microbiology laboratory that follows the guidelines and interpretative criteria for antimicrobial susceptibility testing of the European Committee on Antimicrobial Susceptibility Testing (EUCAST), 29 the Clinical and Laboratory Standards Institute (CLSI), 30 or the Brazilian Committee on Antimicrobial Susceptibility Testing (BrCAST, affiliated with EUCAST). Reference Cast31

Fig. 1. Distribution of the 53 hospitals located in the 5 federative regions of Brazil. Hospitals in each region were distributed as follows: North (Acre, Amapá, Amazonas, Pará, Rondônia, Roraima, and Tocantins); Northeast (Maranhão, Piauí, Ceará, Rio Grande do Norte, Paraíba, Pernambuco, Alagoas, Sergipe, and Bahia); Midwest (Goiás, Mato Grosso, and Mato Grosso do Sul; along with Distrito Federal, the Federal District), Southeast (Espírito Santo, Minas Gerais, Rio de Janeiro, and São Paulo), and South (Paraná, Santa Catarina, and Rio Grande do Sul).
All ICCs had as members doctors (100%), nurses (100%), nursing technicians (43.4%), pharmacists (32.1%), and administrators (43.4%) (Table 1). Among other health professional categories involved in IPC practices, there were differences in the compositions of IPC departments among the analyzed regions (Table 2).
Table 1. Indicators to Evaluate Infection Prevention and Control programs in Brazilian Hospitalsa

Note. IPC, infection prevention and control; ICC, infection control committee.
a This table shows the number of Brazilian hospitals that meet some indicators in the ICC assessment. The indicators are grouped by components. Data were available from 53 hospitals.
Table 2. Characteristics of Hospital Infection Prevention and Control Programs in Brazilian Hospitals, for Federative Regions

Note. IPC, infection prevention and control. Data available from 53 hospitals.
The analysis of data collected via electronic form and on-site visit to the centers revealed that 52 (98%) hospitals had an IPC program (Table 1), 50 (96%) of which had a clearly defined objective for the program. The mean time of existence of ICC was 21.6 years (±11.9). We detected a statistically significant difference in the time of existence of the ICCs between the South and North regions (P = .012), with no significant differences between the other regions in the adjusted analysis (Table 2). Only 9 hospitals had a budget allocated to the IPC program, mostly localization in the Southeast region. Only 2 of the 25 public hospitals with the IPC program had a budget allocated annually to the program (8%), whereas 7 (25%) of the 28 private hospitals had this budget.
The guidelines available from the IPC programs are described in Table 1. Among them, the guidelines for HAI prevention and hand hygiene were evaluated in more detail regarding their recommendations. All centers (100%) had either protocols or guidelines for the prevention and control of ventilator-associated pneumonia, bloodstream infection, surgical site infection, and catheter-associated urinary tract infection. Also, most centers had guidelines for medical waste management and hand hygiene (98.1% and 100%, respectively).
The surveillance indicators are also described in Table 1. All hospitals (100%) reported conducting nosocomial infection surveillance and epidemiological surveillance to detect outbreaks in a timely manner. Within the HAI surveillance component, only 7.5% of hospitals reported occupational infections in healthcare workers. All hospitals had access to a microbiology laboratory to support HAI surveillance, and 38% of laboratory services were outsourced. Within the IPC education and training component, 88.7% of centers provided specific, systematic, and periodic IPC training for hospital staff. Adherence to specific training provided by the ICC was lower among the laundry staff (34.0%) than among other professionals (Table 1).
Within the monitoring and audit of IPC practices and feedback component, nearly all ICCs reported performing routine data collection on nosocomial infections, usually monthly, and using these indicators to evaluate services and plan future actions (100%). Antimicrobial use per patient day was the least-monitored indicator (22.6%) (Table 1).
Nearly all centers had an adequate structure and policy for cleaning, with regular assessment of the policies and structures that guide routine hand hygiene practices in the hospital environment. All hospitals (100%) had personal protective equipment for all professionals and specific containers for disposal of hospital waste, and 98.1% had routine bacteriological control of water (Table 1). There was no statistically significant difference between the Brazilian regions in most of the characteristics described.
Discussion
To support countries in their efforts to strengthen IPC, the WHO released evidence-based guidelines addressing the key components of IPC programs. 2,32 These guidelines cover 8 core components of IPC and include recommendations and best practice statements. Some publications provide an evaluation of ICCs using these core components. In Georgia, for example, 41 hospitals underperformed in the implementation of WHO recommendations, especially those for IPC practices. Reference Deryabina, Lyman and Yee15
In view of the various problems that occurred during the COVID-19 pandemic and the health-system collapse in Brazil and worldwide, the existence of an ICC proved to be indispensable. ICCs were particularly useful in rebuilding care pathways and protocols for IPC, enabling immediate and appropriate decisions to control the spread of the pathogen and to protect health professionals. 33
A well-structured IPC program can reduce infection rates, and some recommendations result from the economic and social burden generated by these events. HAI is preventable and can be reduced by up to 70% through effective IPC measures. Reference Umscheid, Mitchell, Doshi, Agarwal, Williams and Brennan34 Although the implementation of the ICC was not supported in all assessed hospitals, Reference Santos, Padoveze and Lacerda24 most hospitals evaluated in this study had an IPC program. Our data show that all types of infections occurring in Brazilian hospitals are generally reported by the ICC. This reporting practice has a major impact on public health by contributing significantly to infection control. Therefore, simple IPC measures and policies frequently implemented by the ICC, such as hand hygiene, are initial steps for the future success of the IPC program and the effective implementation of IPC practices to prevent the transmission of pathogens. Reference Alhumaid, Al Mutair and Al Alawi35
The ICCs evaluated in our study reported low infection rates in employees. Underreporting of infection rates among health professionals may not only contribute to the failure of IPC actions but also present a threat to the functioning of hospitals due to the lack of preparedness of professionals. Reference Atnafie, Anteneh, Yimenu and Kifle36 This assessment proved to be very important during the COVID-19 pandemic, and several studies have highlighted, among other indicators, the infection rate in health professionals as a critical factor for facility level improvement. Reference Bandyopadhyay, Baticulon and Kadhum37,Reference Montarroyos38
Based on the results of our survey, the major obstacle seems to be the allocation of a dedicated budget for IPC implementation. Only 17% of hospitals had a budget specifically allocated to the IPC program. A dedicated budget for implementing IPC strategies and plans is a minimum requirement according to the WHO. 32 This gap was more pronounced in public hospitals; most of the hospitals that had a dedicated IPC budget were private. The ICC needs economic and administrative support to implement the IPC program, otherwise it might be inefficient and yield unsatisfactory results. The simultaneous availability of qualified personnel, infection control policies, and adequate structures (equipment and materials) is crucial for the implementation of optimal IPC measures. Data from the WHO global report on IPC, with surveys conducted in 62 countries (including Brazil), show a significant increase in the proportion of countries having a dedicated budget for IPC programs between 2017–2018 (25.8%) and 2021–2022 (48.4%; P = .02). 39 However, consistent with the present data, there is still considerable potential for improvement. An Australian study showed that implementing a budget for a cleaning bundle (audit, communication, technique, training, and product) returned a positive net monetary benefit and incremental cost-effectiveness ratio. Reference White, Barnett and Hall40
Regarding IPC education and training of staff, most ICCs offered IPC training to employees and staff members, but not all human resources had the same level of training in the different areas of the facility. Despite the good connection with the cleaning staff, which reported appropriate training, adherence to specific training provided by the ICC was low (34%) among the laundry staff in most hospitals. Specific training for all health professionals is crucial for the success of the IPC program. Therefore, training should not be limited to frontline health workers or IPC specialists but rather encompass all staff regardless of position or function, as providing technical and specific training for the entire hospital personnel is essential to prevent and reduce HAI. Reference Jeong, Joo, Bahk, Koo, Lee and Kim17
Previous studies conducted in Brazil have pointed out deficiencies in HAI prevention and control practices in outsourced services, such as laundry and laboratory. Reference Alves and Lacerda23,Reference Menegueti41 Outsourcing microbiology services, as reported by many centers in the present study, may create obstacles to the actions of the ICC, which depends on the turnover of microbiological results for timely IPC actions. Reference Padoveze, Fortaleza and Kiffer11,Reference Costa, Cardoso and Ferreira42
A strength of our study is the analysis of IPC programs from all 5 Brazilian regions, which provided a broad view of the country’s reality that had not been possible in most previous publications. Limitations of the study include the eligibility criteria for inclusion of hospitals in the IMPACTO-MR program, based on which a sample of hospitals with better conditions was selected, which may have led to improved indicators in our survey. In addition, we modified the assessment form designed by the WHO and other national forms used in Brazilian studies to measure adherence to recommendations for ICC and IPC programs. For this reason, no scoring system was used to evaluate the hospitals or to measure and compare their respective ICCs.
The results of our analysis of IPC programs and ICCs in Brazilian hospitals showed great adherence to IPC guidelines and recommendations, particularly those on hand hygiene, sterilization, and catheter use. The profile of the ICCs of Brazilian hospitals described in the present study indicates the implementation of a range of strategies and policies to combat antimicrobial resistance and prevent HAI. These data are crucial for the establishment of new goals aiming to improve the evaluation of IPC indicators and, consequently, to reduce the rate of infections due to multidrug-resistant organisms in the country. We were able to identify relevant aspects of IPC that may help guide public policies aiming to improve the quality of healthcare services in low- and middle-income countries.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/ash.2023.136
Acknowledgments
Financial support
This research was funded by the Brazilian Ministry of Health through the Institutional Development Support Program of the Brazilian Unified Health System (PROADI-SUS). The funding body has no role in coordinating the study.
Conflict of interest
A.P.Z. is a research fellow of the National Council for Scientific and Technological Development, Ministry of Science and Technology, Brazil. A.P.Z. received a research grant from Pfizer and was a member of the advisory board for Spero Therapeutics and Eurofarma. All other authors have no competing interests to declare.





 Open access
Open access