



Introduction
An estimated 228 million cases of malaria occurred worldwide in 2018, with most of the cases (93%) in the African region. Six countries accounted for more than half of all malaria cases worldwide: Nigeria (25%), the Democratic Republic of the Congo (12%), Uganda (5%) and Cote d’Ivoire, Mozambique and Niger (4% each). In the same year, there were an estimated 405 000 deaths from malaria globally. Children under five are the most vulnerable group affected by malaria. In 2018, they accounted for 67% (272, 000) of all malaria deaths worldwide. The African region accounted for 94% of all malaria deaths in 2018, with Nigeria accounting for almost 24% of all global malaria deaths [World Health Organisation (WHO), 2019]. Also, in 2018 about 24 million children were estimated to be affected with P. falciparum in sub-Saharan Africa and an estimated 1.8 million of them were likely to have severe anaemia. It therefore becomes important to discuss malaria prevention especially in the on-going era of COVID-19 when there is little or no access to hospital care- for non-emergency cases- due, on the one hand, to re-allocation of health resources to combat the virus, and on the other hand to people’s fear of contracting the virus (Sarwari and Goode, Reference Sarwari and Goode2020).
In 2018 globally, 80% of ITNs were distributed through mass distribution campaigns, 10% in antenatal care facilities and 6% as part of immunization programmes. Again, in 2018, 50% of the population at risk of malaria in sub-Saharan Africa slept under ITN, an increase from 29% in 2010, while the percentage of the population with access to ITN increased from 33% in 2010 to 57% in 2018. However, coverage improved marginally since 2015 and has been at a standstill since 2016 (WHO, 2019).
According to Nigeria’s Demographic and Health Survey (NDHS) 61% of households own at least one insecticide treated net (ITN); while 65% of the de facto population in households, with at least one ITN slept under an ITN the night before the survey (National Population Commission [NPC] and Inner City Fund [ICF], 2019). The WHO recommends one ITN for every two people at risk of malaria and Nigeria has been involved in the distribution of ITNs to vulnerable and at-risk population (Olapeju et al., Reference Olapeju, Choiriyyah, Lynch, Acosta, Blaufuss, Filemyr and Koenker2018). In addition, one of the targets of Roll Back Malaria (RBM) programme in the first five years was to ensure that 60% of the vulnerable groups-such as children under the age of 5 five and pregnant women-have access to and sleep under ITN (Oresanya et al., Reference Oresanya, Hoshen and Sofola2008; Global Malaria Action Plan, 2008).
The 2015 Nigeria Malaria Indicator Survey (NMIS) shows that about two-thirds of households in the country own at least one ITN, but only 44% of children under five years used an ITN the night before the survey, which is below the 50% target (National Malaria Elimination Programme et al., 2016). This shows that one in five people who have ITNs do not use them even when evidence suggests that sleeping regularly under ITNs is the most effective way to prevent malaria among children (Orji et al., Reference Orji, Onyire, Chapp-Jumbo, Anyanwu and Eke2018). This suggests the need for attention and improved health seeking behaviour. Hence, this study investigates the influence of mother and child’s characteristics on the use of ITNs. Mother’s characteristics include mother’s age, place of residence, education, religion, wealth level, number of children and previous experience of child’s death, while child’s characteristics include sex of child and child’s age. In addition, this study is interested in how the influence of these factors varies between northern and southern Nigeria.
Evidence shows that consistent use of insecticide-treated bed nets can reduce the incidence of malaria by up to 90% and under-5 mortality by more than 40% (National Malaria Elimination Programme et al., 2016). The ownership of ITN in Nigeria has increased from 8% in 2008 to 61% in 2018 (NPC, 2019). ITN ownership in Nigeria vary by region, place of residence or other maternal demographic characteristics (Andrada et al., Reference Andrada, Herrera, Inyang, Mohammed, Uhomoibhi and Yé2019; Auta, Reference Auta2012). Andrada et al. (Reference Andrada, Herrera, Inyang, Mohammed, Uhomoibhi and Yé2019) found that household ownership of at least one ITN varied significantly by region, Northwest region had the highest ownership and the lowest ownership was noted in South West. Equally, found that household ownership varied significantly by place of residence and household size, with the highest ownership among the rural areas. Education level of the household, place of residence, household size were all predictors of ITN ownership.
Aside ownership of ITN as a predictor of net use, earlier studies have documented other associated factors. For instance, Ibegu et al. (Reference Ibegu, Hamza, Umeokonkwo, Numbere, Ndoreraho and Dahiru2020) attributed high usage of Long-lasting insecticidal nets (LLINs) among pregnant women to high level of education, being in employment and earning above the minimum wage. Iliyasu et al. (Reference Iliyasu, Gajida, Galadanci, Abubakar, Baba, Jibo and Aliyu2012) found that women who are exposed to educational programs on the effects of malaria in pregnancy were more likely to use insecticides nets. Ameyaw et al (Reference Ameyaw, Adde, Dare and Yaya2020) found that women who live in rural locations have higher odds of utilizing ITN compared with those in urban areas and that pregnant women aged 40-44 years are less likely to use ITN compared with those aged 15-19. Poorer women had higher odds of ITN utilization than their wealthy counterparts, and most of the former are in the rural areas (Nwagha et al., Reference Nwagha, Nwagha, Dim, Anyaehie, Egbugara and Onwasigwe2014).
Babalola et al. (Reference Babalola, Adedokun, McCartney-Melstad, Okoh, Asa, Tweedie and Tompsett2018) found ideational characteristics that were positively and significantly associated with consistent net use to include willingness to pay for nets, awareness of a place to obtain bed nets, perceived response efficacy of bed nets with others, positive attitudes towards bed nets, perceived self-efficacy to use nets, and descriptive norms about bed net use. Adedokun and Uthman (Reference Adedokun and Uthman2020) found that individual and contextual factors influenced the use of mosquito nets among women of reproductive age in Nigeria. Such factors include knowledge of the causes of malaria, perception that the chances of getting malaria are the same whether mosquito nets are used or not, knowledge on the efficacy of malaria prevention drugs. The study equally found that the socioeconomic status of communities and states influence ITN use as women who live in the most socioeconomically disadvantaged communities and states utilized mosquito nets more compared to those in the least disadvantaged position. Regarding obstacles to ITN use, Israel et al. (Reference Israel, Fawole, Adebowale, Ajayi, Yusuf, Oladimeji and Ajumobi2018) found common barriers to utilization of nets among under-five children to include excessive heat, reactions to chemicals, unpleasant odour and cost and found that daily utilization was poor as only two-fifth sleep under the net.
However, earlier studies have emphasised mothers’ characteristics and little is known about the influence of factors related to children. Secondly, earlier studies have treated region (i.e the six geo-political zones) as an independent variable. This study takes a step further by analysing data for each region separately. In other words, after looking at the influence of difference factors on ITN use in Nigeria, attempt was also made to treat each broad region (i.e north and south) as an entity. The importance of understanding north-south differences is discussed in the next section. To reiterate, this study investigates mother and child-related factors associated with the use of ITN, and how the factors vary across northern and southern Nigeria.
Why North-South differences?
There are important conceptual/theoretical and empirical reasons to be curious about differences in health seeking behaviour between northern and southern Nigeria. One, a recent study by Rose et al. (Reference Rose, Sylla, Badolo, Lutomiah, Ayala, Aribodor and McBride2020) found that population density and dry weather drive mosquito bite. According to the population census figures published by the National Population Commission in 2009, ten states with the least population density are from the north, while five states with the highest population density are from the south. The figure ranges from 51 persons per km2 in Yobe (north) to 2695 persons per km2 in Lagos (South). Also, some variations exist in the weather conditions (Abaje and Oladipo, Reference Abaje and Oladipo2019). This shows that attitude towards mosquito bite and the need to use ITN may be different across the two regions. Secondly, Alabi et al. (Reference Alabi, Atinge, Ejim and Adejoh2020) call the attention of researchers and policymakers to the importance of understanding how historical and socio-cultural differences shape different reactions to health seeking behaviours between the northern and the southern parts of Nigeria, and advise that uniform intervention policies may not yield the same results due to different worldviews. The two regions have different perennial socio-cultural characteristics that date back to the pre-colonial era. For example, using the 2018 NDHS, a study reported 62.8% of mothers within the reproductive age in the north had no education compared to 6.6% in the south. More than half (59.6%) of the respondents in the south had secondary education compared to 18.6% in the north. Approximately a quarter of northern mothers live in the rural areas compared to 56.6% in the south. While 81.2% of the mothers in the north are Muslims, 84.9% of those in the south are Christians. The rate of joint decision making on healthcare between spouses in the south stands at 51.5% compared to 19.4% in the north (Alabi et al., Reference Alabi, Atinge, Ejim and Adejoh2020). All these characteristics may influence uptake, use and perception of ITNs, and since the distributions of these characteristics vary across the regions, one may expect that factors influencing the use of ITNs may also vary. These suggest that the two regions may need to be considered separately where necessary.
Earlier studies (see Kunnuji et al., Reference Kunnuji, Robinson, Shawar and Shiffman2017 and Alabi et al., Reference Alabi, Atinge, Ejim and Adejoh2020) have used the Cosmopolitan-Success and Conservative-Failure hypothesis to explain regional differences between northern and southern Nigeria. However, authors of this study are aware of the criticisms being rendered by decolonization scholars against the use of such terms as “cosmopolitanism” and “conservatism” as the concepts tend to portray entities who share western ideals as being open, positive and cosmopolitan, and those who hold tenaciously to the African traditional ways as rigid, close, negative and conservative (Alabi and Badru, Reference Alabi and Badru2021). Hence, such terms are avoided- except where necessary- in this exercise. The point is to show that there are important reasons to consider regional differences for the overall development of the country. Beyond the scope of this study, the antagonism between the northern and southern governors regarding anti-grazing laws, and the differential reactions to the protests SARS (Special Anti-Robbery Squad) in 2020 by northern governors’ forum and southern governors’ forum are political indicators that, even though the country operates federalism- at least constitutionally-, differences in the socio-cultural worldviews of the people should be considered for adequate policy interventions.
Methods
Data and population
The study utilised the latest Malaria Indication Survey (MIS) data collected between October and November 2015. The survey, conducted every 5 years, could not hold in 2020 due to the COVID-19 pandemic but will hold in 2021, ceteris paribus. The decision to use the 2015 MIS, instead of the 2018 NDHS, was motivated by the fact that the former exclusively focuses on malaria and has much more details in this regard than the latter. The MIS used the National Population and Housing Census of 2006 as the sampling frame and adopted a two-stage sampling technique to select respondents. In the first stage, eight enumeration areas were selected from each of the 36 states and the Federal Capital Territory (FCT) Abuja, which resulted in a total of 333 enumeration areas. In the second stage, 25 households were selected from each enumeration area. Eligible respondents were women within the reproductive age of 15-49. Women who were either permanent residents of the household or were present in the households the night before the survey were eligible to participate in the survey. The children recode data set was comprised of 6524 women, but only 6160 respondents who provided responses to the outcome variable were included in this study. The 6160 respondents were composed of 4009 from the north and 2151 from the southern part of Nigeria.
Nigeria is comprised of 36 states and the FCT which are grouped into six geo-political zones, namely: southeast, southwest, southsouth, northcentral, northeast and northwest. The six geopolitical zones are categorised into two broad regions (north and south) in this study for ease of analysis. Figure 1 shows the 36 states and the FCT, and the region (whether north or south) in which they are situated.
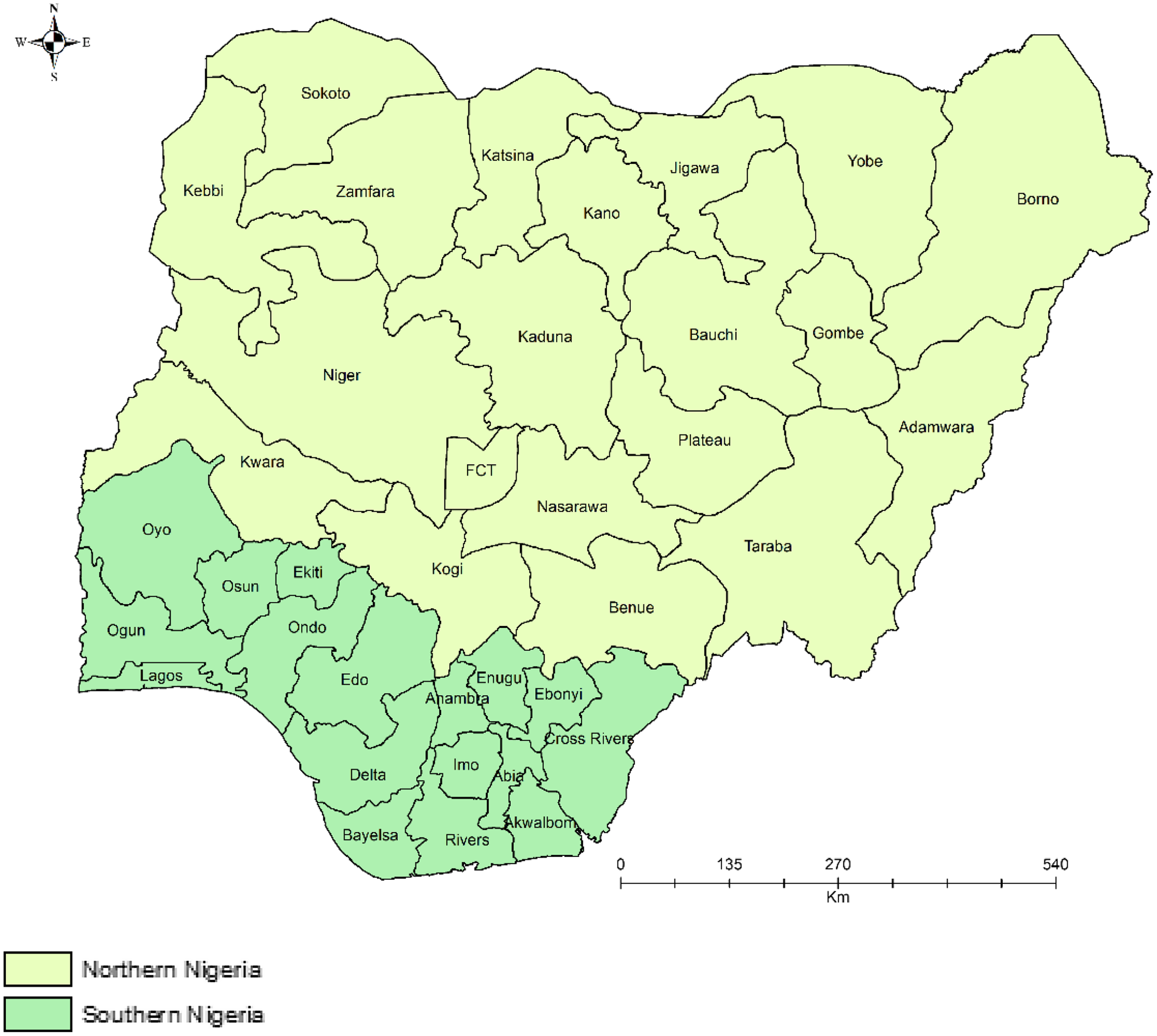
Figure 1. The 36 states and the FCT, and the region.
Ethical consideration
All ethical issues had been considered by the Demographic and Health Survey (DHS) office before and during the study. There was no ethical consideration on the part of the researchers. The researchers requested for the dataset from the DHS office after registering on its website (https://dhsprogram.com/data/new-user-registration.cfm) and indicating the rationale and brief description of the study. The DHS office granted the permission to use the data and provided the researchers with a link to the data set.
Measures
Outcome variable
The dependent variable was the use of ITNs, which was derived from the question that asked about the type of mosquito net the child slept under the night before the survey, with four options (‘0’ = ‘no nets’; ‘1’ = ‘only treated nets’; ‘2’ = ‘both treated and untreated nets’, and ‘3’ = ‘only untreated nets’). No respondent responded, “both treated and untreated nets”. At the inferential level of analysis, the first and last options were merged and coded as ‘0’ = no net/untreated net, while those who chose the second option (‘1’) were regarded as having used treated nets.
Independent variables
There were nine independent variables. The first was mother’s age captured at ratio level but was categorized -using the WHO standards of age categorization-only at the descriptive level of analysis into 7 groups beginning with 15-19 and ending with 45-49. Place of residence was measured by whether a respondent was living in a rural or urban area as of the time of the study. Education was captured at four levels in line with the educational system in Nigeria, namely, ‘no education’, ‘primary education’, ‘secondary education’ and ‘tertiary education’. The question on religion had five values, namely, ‘Christianity’, ‘Islam’, ‘Traditional Religion’, ‘no religion’ and ‘other’. Only the first two categories were included in the bivariate and multivariate analyses as the three other categories had small values. Wealth index was measured at five levels from poorest to richest by the DHS using the ownership of basic household items. Number of children aged 5 or less was captured at ratio level but was categorised at the descriptive level into ‘two children or less’ and ‘more than two children’. Sex of child was determined by whether the child whom the mother was asked about in the outcome variable was male or female. Child’s age was captured in months in the data sets and was categorised into ‘24 months or less’ (i.e., infants) and ‘more than 24 months’ (i.e., children) in line with the WHO standards. Regarding previous experience of child mortality, mothers were asked of the male and female child who had died in two different questions. Any respondent who responded in the affirmative to at least one of them was treated as having had a previous experience of child mortality.
Data analysis
The descriptive analysis was done using simple frequencies, percentages, mean and standard deviation separately for each region and results presented in Table 1. The study used simple bar chart to show the rate of ITN use in the FCT and all the 36 states in Nigeria as shown in Figure 1. To show the pattern graphically, a map is presented in Figure 3, showing the rates of ITN use in three categories (less than 20%, 20%-49% and 50% or above) across the states in the country-see Figure 2. At the bivariate level, binary logistic regression was used to investigate the influence of each of the independent variables on use of ITN. Side-by-side with the bivariate regression, a multivariate logistic regression model was fitted to see how the variables interact with one another and the results presented in Table 2. Later, the data set was separated into north and south, and a logistic regression model fitted for each one, to see regional differences in the predicting power of covariates. The results are shown in Table 3. The regression models were fitted at 95% level of significance. All the covariates are categorical except for factors such as mother’s age, number of children in household, and child’s age in months.
Table 1. Socio-demographic characteristics and other variables

* No value recorded for 4 children in the north.

Figure 2. The rate of ITN use in the FCT and all the 36 states in Nigeria.

Figure 3. Rate of use of ITN across the 36 States.
Table 2. Logistic regression model showing the influence of individual variables and their joint effects

Reference category: North; Urban; No education; Poorest; Christianity; Male; No previous child’s death.
Table 3. Logistic regression showing regional variations in the predictors of use of ITN

Reference category: North; Urban; No education; Poorest; Christianity; Male; No previous child’s death.
Results
Socio-demographic characteristics and other variables
Table 1 shows that there were considerable regional differences in the socio-demographic characteristics and other variables. The rate of adolescent motherhood (aged 15 to 19) was 7% in the north compared to 2.6% in the south. More than a quarter (27.7%) of mothers in the north were within the ages of 25 and 29 while 31.8% of mothers in the south were within the same age category. The mean age in the north was 27.6 compared to 29.8 in the south. About three-quarters (75.9%) of mothers from the northern region resided in rural areas, while more than half (53.3%) of those from the south resided in an urban area. The majority (62%) of mothers from the north did not have any formal education, while more than half (56.5%) of those from the south had secondary education. More than three-quarters (77.7%) of mothers from the north were Muslims while an overwhelming majority (86.8%) of those from the south were Christians. More than half (58%) of mothers from the north were in the poor categories while 73.3% of those from the south were in the rich groups, showing that southern women can be said to be wealthier than their counterparts in the north.
Regarding the number of children (aged 5 or less), it was found that more than half (57.6%) of households in the north had at most two children compared to 72.8% in the south. This reinforced the fact that average fertility size was higher in the north than in the south. Approximately half of the children from the north were males compared to 51.8% from the south. In both regions, the children were more than 2 years of age (59.5% in the north and 55.4% in the south). About 1 in 3 women in the north had experienced child mortality, compared to less than a quarter (19.1%) in the south. Regarding types of mosquito nets used for children aged 5 or less, it was found that less than half (47.9%) of mothers from the north reported that they had no net at all compared to 70.8% in the south. More than half (51.4%) of northern women reported the use of only treated nets while less than one-third (27.1%) of those from the south reported same. The use of untreated nets was more common in the south (2.2%) than in the north (0.7%).
Figure 2 further shows the use of treated nets across the 36 states and the FCT in Nigeria. It was found that the use of ITNs ranged from 79.8% in the northern state of Jigawa to 6.9% in the southern state of Imo. The 10 states with the highest rate of ITN use are from the north including all the 6 states in the north-west (Jigawa, Kaduna, Zamfara, Kano, Katsina and Sokoto) where policy intervention programmes supported by international donor partners have been concentrated. Of the 13 states with the least rate of ITN use, 11 are southern states while the remaining two (Kwara and the FCT, Abuja) are from the north central. Figure 3 shows the pattern of ITN use across states and regions. It was found that only one southern state (Ebonyi in the south-east) had ITN use rate of more than 50%, while the remaining 16 states from the south had less than 47% rate of ITN use. Contrarily, of the 13 states in the north-west and north-east, 9 states had more than 50% rate of ITN usage.
Results of bivariate and multivariate logistic regression
In Table 2, the authors present the results of the logistic regression models showing the unadjusted effects of each of the independent variables (labelled “bivariate” in the table), and their adjusted effects (labelled “multivariate” in the table) after controlling for other variables included in the model. It was found that when tested alone and together with other covariates, region had a significant influence on the use of ITN as mothers from the south reported less use of ITN for their children compared to respondents from the north. But the influence was more pronounced when the variable was tested separately (B: −1.046; OR: 0.351 vs B: −0.419; AOR: 0.657; p was less than 0.001 in both cases). Mother’s age was also a significant factor, and the direct effect was that the likelihood of using ITN reduces as mother’s age increases (OR: 0.974; AOR: 0.985). When place of residence was tested separately, it was found that mothers in rural areas had 1.6 times more likelihood than their counterparts in the urban areas to use ITN for their children (B: 0.436, p<0.001). But the reverse was observed when the variable was in the same model with other covariates (B: −0.214; AOR: 0.808; p<0.01). Similarly, the finding on education when tested alone showed that mothers who had some educations were less likely to use ITN for the children compared to those with no formal education. In fact, the likelihood of ITN use decreased with increase in the level of education (OR of 0.7 for primary education; OR of 0.49 for secondary education, and OR of 0.44 for tertiary education, p<0.001 in all cases). But when education was included together with other covariates, the result indicated that those who had education were more likely to use ITN for their children compared to those with no formal education (p<0.001).
The influence of mother’s wealth is somewhat consistent and showed that the likelihood of ITN use reduces as wealth increases (p<0.001). Regarding the influence of religion, it was found that Muslim mothers were likely to use ITN for the children compared to Christian mothers (p<0.001). But the influence was more pronounced when tested alone (B: 0.914; OR: 2.5), than when tested with other covariates (B: 0.549; AOR: 1.7). The number of children aged 5 or less in the household was a significant predictor as the likelihood of ITN use decreases with increase in the number of children in the household. Whether tested separately or together with covariates, age and sex of child did not have significant influence on the use of ITN. Previous experience of child’s death had significant influence on ITN use as mothers who had experienced the death of at least one child were more likely to use ITN for their children.
Regional variations in the predictors of the use of ITN
Having established that mothers in the north and south differ in their use of ITNs for children, two logistic regression models (one for each region) are presented in Table 3, to see how the influence of the variables differ across the two regions. Evidence is found of the existence of variation in the influence of age. In the north, the likelihood of ITN use reduced significantly as mother’s age increases (AOR: 0.982, p<0.001) but the association was not significant in the south. In the north, mothers who had secondary education were 1.5 more likely to use ITN than those who had no education (p<0.001), but the association was not statistically significant in the south. Although mothers who had tertiary education also had higher likelihood of ITN use than the reference category, the significance was only at 93% level (AOR: 1.5; p: 0.073). But in the south, mothers who had education (at any level) were significantly more likely to use ITN than those who had no education. Mothers who had tertiary education were most likely to use ITN in the south (AOR: 2.2; p: 0.001).
Mother’s wealth was a significant predictor of ITN use in both regions, and the direction was that the likelihood of ITN use decreases as wealth increases, but significant difference was only observed among mothers in the richer (AOR: 0.458, p<0.001 in the north; AOR: 0.334; p: 0.016 in the south) and richest categories (AOR: 0.333, p<0.001 in the north; AOR: 0.255; p: 0.003 in the south). Muslims had significantly higher odds of using ITN than Christians in both regions, but the influence was more in the north (B: 0.607, p<0.001) than in the south (B: 0.397; p: 0.007). The age and sex of the child remained insignificant in both regions. Regional differences were observed in the influence of previous experiences of child deaths. Mothers who had experienced the death of at least one child were 1.4 times more likely to use ITNs (p<0.001) in the North, but the influence was not significant in the south.
Discussion
This study investigated the influence of mother’s and child’s factors associated with the use of ITNs, and the factors that vary across the northern and southern regions. Contrary to earlier findings and theory by Alabi et al. (Reference Alabi, Atinge, Ejim and Adejoh2020) that the south will likely embrace health seeking behaviour more than the north due to higher levels of education in the former, this study found that the respondents from the north had access to and use ITNs more than their counterparts from the south. However, the finding of this study supports the research by Alabi and Badru (Reference Alabi and Badru2021) who found that the risks of overweight/obesity is lower in northern Nigeria compared to the southern region.
There are some plausible reasons why the finding of this study runs contrary to the logic of CSCFH. One, mosquitoes’ “preference for humans is associated with intense dry seasons and urbanization” (Rose et al., Reference Rose, Sylla, Badolo, Lutomiah, Ayala, Aribodor and McBride2020, p.1). Since the hotter and dryer states are in the north, one will expect that residents in northern Nigeria will experience mosquito bites than those in the south. Perhaps, this could explain why there is a geographically disproportionate coverage of donor-funded public health malaria intervention programmes- they are mainly focused on the northern region of the country. Universal access to free malaria commodities and services are available in all the states in the north with the support of the Global Fund to fight AIDS, Tuberculosis and Malaria, the United States President’s Malaria Initiative and the United Kingdom Department for International Development Programme. However, in the south, only Ogun and Osun (south-west), Delta and Cross River (south-south) and Ebonyi (south- east) States benefit from these programmes. The National Malaria Strategic Plan 2014–2020 aims to achieve universal access to ITNs and their use across the country. The north has been known to lack access to adequate health facilities compared to the south, and this may explain why donor agencies have focused attention on the former.
Second plausible reasons, which are related to the first, include urbanization and population density. The rate of urbanization and population density are higher in the South than in the North. For example, population density ranges from 51/km2 in the north-eastern state of Yobe to 2695/per km2 in the south-western state of Lagos. Hence, one will expect that those in the south will experience more mosquito bites, but why do they have a low rate of ITN use? High population density and lack of physical space can cause heat, and earlier studies have documented that heat is a barrier to use of ITNs (Pulford et al., Reference Pulford, Hetzel, Bryant, Siba and Mueller2011; Desmon, Reference Desmon2019). Participants in the study of Desmon (Reference Desmon2019) reported that they use mosquito nets during the rainy season when there is little or no heat but “when the heat starts to come, then we reject it (ITN) because … when you sleep in it, you will sweat.” (Our emphasis in bold text). Increasing heat due to urbanisation, high population density and implication for lack of ventilation due to erection of structures may serve as barrier for use of ITNs in the south. Contrarily, low population density in the north may allow cross ventilation such that heat will not serve as barrier to ITN usage. A third plausible reason is the fact there is wealth inequality between the northerners and southerners with the former being more disadvantaged. Consequently, residents in the south can afford insecticide sprays which they use in their houses in the night before going to bed compared to their counterparts in the north whose only way of preventing malaria may be the use of ITN.
The findings from this study show that as mother’s age increases, ITN use reduces. This could be as result of the perception by mothers that they have enough experience on how to control mosquitoes and hence may not be really interested in ITN use or that the children have grown past the under-five age category, recognised as one of the vulnerable groups in malaria control programmes. This study’s finding on age as a factor in the use of ITN is consistent with similar studies by Dye et al. (Reference Dye, Apondi, Lugada, Kahn, Smith and Othoro2010), Graves et al. (Reference Graves, Ngondi, Hwang, Getachew, Gebre, Mosher and Richards2011), Rehman, et al. (Reference Rehman, Coleman, Schwabe, Baltazar, Matias, Roncon Gomes and Kleinschmidt2011) and Ye et al. (Reference Ye, Patton, Kilian, Dovey and Eckert2012). However, this study’s finding is inconsistent with studies by Atieli, et al. (Reference Atieli, Zhou, Afrane, Lee, Mwanzo, Githeko and Yan2011) and Berie et al. (Reference Berie, Alemu, Belay and Gizaw2013) as they did not find any relationship between age and the use of ITNs. This research’s finding that the association is significant in the north but not in the south may reflect large household sizes in the north. It makes sense to say that a woman’s fertility will increase with her age, and since family size is higher in the north than in the south, it makes sense to say that the reason for non-use of ITNs among older mothers in the north may be due to the high number of children in the household relative to the number of available ITNs.
On place of residence and the use of ITNs, the finding shows that mothers in rural areas utilize ITN more than mothers in urban settings, when examined without other variables. Although ownership and usage are two different things, NPC and ICF (2019) reported that household ownership was higher in rural (68%) than urban areas (53%). This may be explained by the fact that the rural areas may be more exposed to mosquitoes because of the type of houses built in the rural areas, which may not have window nets nor ceilings to give additional protection from mosquitoes, hence they may be more interested in the use of ITNs. However, when examined with other variables of interest, mothers in urban areas are more likely to use ITNs than those in the rural areas. Mothers in urban areas may have access to more information, to health facilities and intervention programmes. This finding is consistent with other studies that attributed the low use of ITNs in rural areas to poor access to health-related information and other resources (Garcia-Basteiro et al., Reference García-Basteiro, Schwabe, Aragon, Baltazar, Rehman, Matias and Kleinschmidt2011; Gobena et al., Reference Gobena, Berhane and Worku2012; Sena et al., Reference Sena, Deressa and Ali2013).
The finding demonstrates that mother’s education is a significant factor in the use of ITNs, this implies that the educational attainment of mothers is a positive factor in the utilization of ITNs by mothers either for themselves or for their under five children. This finding is in line with similar findings by Oresanaya et al. (Reference Oresanya, Hoshen and Sofola2008), Chukwuocha et al. (Reference Chukwuocha, Dozie, Onwuliri, Ukaga, Nwoke, Nwankwo and Adindu2010), Arogundade et al. (Reference Arogundade, Adebayo, Anyanti, Nwokolo, Ladipo, Ankomah and Meremikwu2011), Ankomah et al. (Reference Ankomah, Adebayo, Arogundade, Anyanti, Nwokolo, Ladipo and Meremikwu2012), Auta, (Reference Auta2012), Ye et al. (Reference Ye, Patton, Kilian, Dovey and Eckert2012), Adeneye et al. (Reference Adeneye, Jegede, Nwokocha and Mafe2014), Eteng et al. (Reference Eteng, Mitchell, Garba, Ana, Liman, Cockcroft and Andersson2014), Ezeama et al. (Reference Ezeama, Ezeamah and Akor2014), Ezire et al. (Reference Ezire, Adebayo, Idogho, Bamgboye and Nwokolo2015), Fokam et al. (Reference Fokam, Kindzeka, Ngimuh, Dzi and Wanji2017), Tariku et al. (Reference Tariku, Alemu, Gizaw, Muchie, Derso, Abebe and Biks2017) and Nkoka et al. (Reference Nkoka, Chipeta, Chuang, Fergus and Chuang2019) that mother’s level of education is associated with her perception of who was most vulnerable to malaria and may require ITNs in the household. However, some other studies did not find any relationship between educational level and ITN use (Sangaré et al., Reference Sangaré, Weiss, Brentlinger, Richardson, Staedke, Kiwuwa and Stergachis2012), Loha et al. (Reference Loha, Tefera and Lindtjørn2013) and Berkessa et al. (Reference Berkessa, Oljira and Tesfa2015). This may be due to the fact that education alone may not account for why a mother may or may not use ITN but other factors such as how comfortable it is to sleep under the net, perceived side effects and space in the room to hang the net. Little or no variation exists between the north and the south as it relates to the influence of education on the use of ITNs among mothers. For example, mothers in the north with secondary school education were more likely to use ITN than those without education, while mothers in the south with any form of education were more likely to use ITN than those without any form of education.
On mother’s wealth and use of ITNs, the finding demonstrates that as mother’s wealth increases, the use of ITN reduces. This may be due to wealthy mother’s ability to afford alternative vector control measures such as indoor insecticide sprays and other means of controlling mosquitoes. Hence the need to use ITNs may be reduced. This finding is in line with 2018 NDHS report that household ownership of ITNs decreases with increasing wealth, from 73% in the lowest wealth quintile to 48% in the highest quintile (NPC and ICF, 2019). At the regional level, mother’s wealth is a significant predictor of the use of ITNs in both regions. This implies that irrespective of region, once a mother could afford alternatives to ITNs, she may do so without hesitation. And this might be attributed to issues raised about ITNs as being uncomfortable to use, cause heat, fear of side effects, and the poor quality of ITNs (Adebayo et al., Reference Adebayo, Akinyemi and Cadmus2014; Adeneye et al., Reference Adeneye, Jegede, Nwokocha and Mafe2014; Nyavor et al., Reference Nyavor, Kweku, Agbemafle, Takramah, Norman, Tarkang and Binka2017; Taremwa et al., Reference Taremwa, Ashaba, Adrama, Ayebazibwe, Omoding, Kemeza and Hilliard2017).
The finding of this study revealed that religion has an influence on Muslim mothers use of ITNs more than their Christian counterparts in both regions. This finding is consistent with other studies that found a relationship between belonging to religious groups and the use of ITN (Nkoka et al., Reference Nkoka, Chipeta, Chuang, Fergus and Chuang2019; Nketiah-Amponsah, Reference Nketiah-Amponsah2010). This study’s finding on religion somewhat contradicts the finding of Alabi et al. (Reference Alabi, Atinge, Ejim and Adejoh2020) who reported that Christians in the north embrace health seeking behaviour (such as institutional delivery) more than their Muslim counterparts in the same region, but the reverse is the case in the south where Muslims practise facility-based delivery more than their fellow Christians. Future investigations are however required to understand why and how Muslims use ITNs more than Christians. This is important considering that Muslims are believed to be more ‘conservative’ than Christians.
On the number of children in the household and the use of ITN, findings show that as the number of children increase, the likelihood of the children sleeping under ITNs decreases in the North. This may be attributed to the number of ITNs in a particular household and the number of children, if the number of children outstrips the number of ITNs; the decision has to be made about those who will sleep under the net. Neither age nor sex of the child had significant influence on the use of ITNs.
In the North, experience of child’s mortality is a significant factor in the use of ITN as those who experienced child mortality are more likely to use ITNs. This might be because if the cause of the death of a child was known to the mother, she might want to take measures to prevent a reoccurrence and one way to do so is to prevent malaria using ITNs. However, at the regional level, the experience of child death is a significant factor in the use of ITNs in the north but not in the south. This may be explained by the fact that child mortality is higher in the north than in the south, and in reaction, international organisation and donor agencies have focused on preventing the occurrence of child deaths in the north by encouraging and assisting mothers in the region on different health seeking behaviours including the provision of ITNs and educating mothers in the region on the importance of using same.
Limitations
This study has a few limitations. One, the study relied on secondary analysis of self-reported data from the mothers. The primary data is prone to under and over reporting, forgetfulness and difficulty in recall. However, the key dependent variable focused on immediate events which occurred around 24 hours prior to the study, which helps to minimise the problem of recall. Two, the study treated groups in each of the two broad regions as entirely homogenous, whereas each region is comprised of three geopolitical zones, and each zone has different social groups. However, groups in each of the two broad regions have some similarities in terms of geography and culture which makes the groupings into north and south worthy of analysis.
Conclusion
This study has shown that considerable regional differences exist in the use of ITNs between northern and southern Nigeria, and this reinforces the early study of Alabi et al. (Reference Alabi, Atinge, Ejim and Adejoh2020) that the north and south have considerable socio-cultural differences and this influences the way each region reacts to innovation, and factors that influence health seeking behaviour. Although the impact of most of the covariates is reasonably similar in the two regions, three variables stand out clearly (mother’s age, number of children in the household, and previous experience of child mortality). These three variables are statistically significant in the north, but not in the south.
Contrary to the notion that the north is less likely to embrace health seeking behaviour-such as child delivery at the hospital- compared to the south (Alabi et al., Reference Alabi, Atinge, Ejim and Adejoh2020), this study found that such assumption does not apply to the use of ITNs as the mothers from the north use ITNs for their children more than their counterparts from the south. This may be because of the fact that the government of Nigeria, partners from the United States and non-governmental organisations have focused more on the distribution of ITNs in the north where poverty and child mortality as a result of malaria is higher. Future studies should employ the qualitative method of research to fully capture the main reasons for some of these findings.
Funding
This research received no specific grant from any funding agency, commercial entity or not-for-profit organization.
Our sincere appreciation goes to Abiodun Ajijola of the Department of Geography, University of Lagos for assisting with the final version of the map.
Conflicts of Interest
The authors have no conflicts of interest to declare.
Ethical Approval
The latest 2018 NDHS was approved by the Institutional Review Board of ICF with number ICF IRB FWA00000845. The survey was also approved by Nigeria’s National Health Research Ethics Committee (NHREC) with approval number NHREC/01/01/2007. Permission to use the data was sought from the DHS programme office. The rationale for using the data and country of research interest was stated in the online request form (https://dhsprogram.com/data/newuser-registration.cfm). Access to the data was granted after consideration of the researchers’ request. The researchers did not consider any ethical issues as the data were anonymous. Furthermore, the DHS programme office followed all necessary ethical guidelines before and during data collection. The authors assert that this work complies with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.






